Case Report
Case Report
A 62-year-old female patient was admitted presenting with typical precordial pain initiated after intense emotional stress (witnessing her husband’s murder), significant dyspnea and signs of low cardiac output (pallor and hypotension).
On physical examination the patient was lethargic and markedly pale. Heart auscultation: rhythmic heart sounds and tachycardia; lung auscultation: crackles in up to 2/3 of lower pulmonary fields. BP: 77 x 30 mmHg; HR: 80 bpm; RR: 32 irm; Temp: 37°C, no pertinent antecedents.
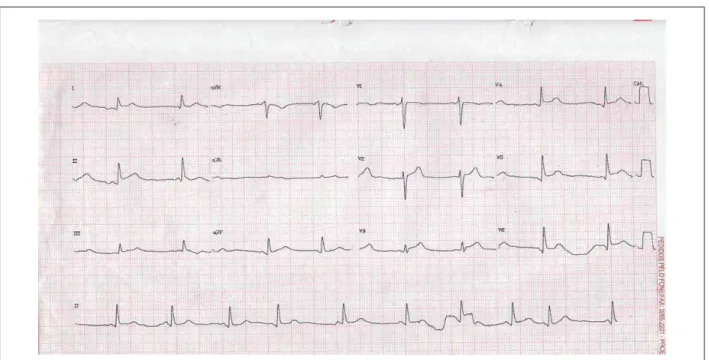
Admitting electrocardiogram showed ST segment elevation in the inferolateral wall (Figure 1).
Laboratory tests revealed elevated cardiac enzymes (Table 1). Chest X-ray disclosed pulmonary congestion and normal cardiac shadow.
The patient progressed to cardiogenic shock and respiratory failure, and the use of vasoactive amines and ventilatory support was initiated.
She was referred to the hemodynamics laboratory where a study of the coronary arteries showed no significant obstructions and the left ventriculography showed an aneurism of the anterior wall in a shape similar to that of a takotsubo or barbells (Figure 2).
After 48 hours, the patient showed significant clinical improvement and use of amines was progressively discontinued along with weaning from mechanical ventilation.
An echocardiogram 72 hours after onset showed akinesis and dilation of the left ventricular apex with preserved systolic function and weak diastolic dysfunction due to relaxation deficit.
The patient was discharged on the ninth day of hospitalization in stable clinical condition using aspirin, statin, and an ACE inhibitor. She returned for out-patient evaluation 15 days later, and a new echocardiogram showed preserved global and segment kinetic function.
Discussion
Takotsubo cardiomyopathy is a new cardiac syndrome characterized by transient dysfunction of the left ventricle with chest pain, electrocardiographic changes and a minor release of enzymes mimicking an acute myocardial infarct1. Left
ventriculography shows apical ballooning with hyperkinesis of the basilar segment resembling a barbell or a “takotsubo” (a fishing pot used in Japan for trapping octopus).
One peculiarity of the syndrome is that it is triggered by very diverse factors, one of them being stress. All stress situations cause an elevation of catecholamines which may also be the cause of ventricular dysfunction, such as in pheochromocytoma2.
Despite having an unknown cause, sympathetic stimulation has been proposed as a central factor in the pathophysiology of this syndrome. Patients with Takotsubo syndrome have higher catecholamine levels than infarct patients of the same Killip class. Regional differences in adrenergic sensitivity or innervation may explain the different clinical presentations and segment alterations. Finally, some investigations have suggested that the septal thickening is a primordial factor in the pathophysiology of the syndrome by dividing the left ventricle into two chambers resulting in apical ballooning provided a secondary triggering factor dehydration or increased catecholamine levels is present3.
Precipitated by intense emotional stress, the syndrome is more common in women between 60 and 75 years of age, as is the case in question4. The most frequent symptom is
retrosternal pain, although some patients present with dyspnea, shock, or merely electrocardiographic abnormalities5.
On the electrocardiogram, the ratio between the ST segment elevation in V4-5 and ST segment elevation in V1-3 is significantly high, and the QTc interval is longer. The absence of reciprocal alterations, absence of abnormalities in Q, and the ST V4-6 / V1-3 > 1 ratio show high sensitivity and specificity for the diagnosis6.
Laboratory tests show elevated troponin T and less frequently, CK-MB.
Key words
Stress, psychological / complications; heart diseases; Takotsubo syndrome.
Stress-induced cardiomyopathy, also know as reversible left ventricular apical ballooning, “Broken-Heart” syndrome, and in Japan, Takotsubo, is characterized by the presence of a transient left ventricular dyskinetic movement of the anterior wall of with hypercontraction of the ventricular basilar segments precipitated by emotional stress.
The clinical course of Takotsubo cardiomyopathy is similar to that of an acute myocardial infarct with typical chest pain and electrocardiographic changes, and during the acute phase, coronary angiography is used to distinguish between the two conditions.
Broken-Heart Syndrome (Takotsubo Syndrome)
Alessandra Edna Teófilo Lemos, Antonio Luiz Junior Araújo, Michely Teófilo Lemos, Lucia de Souza Belém, Francisco Juarez C. Vasconcelos Filho, Raimundo Barbosa Barros
Hospital de Messejana, Fortaleza, CE - Brazil
Mailing address: Alessandra Edna Teófilo Lemos •
Rua Osvaldo Cruz, 1000 / 1703 - Meireles - 60125-150, Fortaleza, CE - Brazil E-mail: [email protected]; [email protected]
Manuscript received June 08, 2007; revised manuscript received August 14, 2007; accepted August 29, 2007.
Case Report
Lemos et al. Takotsubo Syndrome
Arq Bras Cardiol 2008; 90(1) : e1-e3 is that it may reflect a temporal variation of the resolution of the process, though this does not explain the hypercontractility of the apical segment.
The absence of significant obstructive coronary artery disease and the reversibility of the left ventricular dysfunction are important concepts for the diagnosis; on average, ventricular function is restored in up to 18 days after the onset of the symptoms8.
In the case in question, after an intense emotional trauma, a post-menopausal woman progressed with cardiogenic shock and respiratory failure due to acute pulmonary edema, and showed significant improvement within 48 hours. Hemodynamic coronary artery study Recently a variation of transient left ventricular ballooning
was described in which only the midventricle is affected, with hypercontractility of the basilar and apical segments, called reverse Takotsubo7. The explanation for this new variant seems
as uncertain as that of the standard disease. One speculation
Fig. 1 - Elevation of the ST segment in the inferolateral wall
Fig. 2 - Apical ballooning of the left ventricle
Table 1 - Dosage of cardiac enzymes
Test / Date 12.SEP.05 13.SEP.05
CK (U/L) 609 495
Mass CK-MB (ng/ml) 47.8 41.6
Troponin T ( ng/ml) 3.22 0.97
Case Report
Lemos et al. Takotsubo Syndrome
Arq Bras Cardiol 2008; 90(1) : e1-e3
References
1. Ishikawa K. “Takotsubo” cardiomyopathy: a syndrome characterized by transient left ventricular apical ballooning that mimics the shape of bottle used for trapping octopus in Japan. Intern Med. 2004; 43 (4): 275-6.
2. Sousa JM, Knobel M, Buchelle G, Sousa JA, Fisher CH, Born D, et al. Transient ventricular dysfunction (Takotsubo cardiomyopathy). Arq Bras Cardiol. 2005; 84 (4): 340-2.
3. Van de Walle SO, Gevaert SA, Gheeraert PJ, De Pauw M, Gillebert TC. Transient stress-induced cardiomyopathy with an “inverted Takotsubo” contractile pattern. Mayo Clin Proc. 2006; 81 (11): 1499-502.
4. Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, et al. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004; 141: 858-65.
5. Reeder GS. Stress-induced (Takotsubo) cardiomyopathy. [Acesso em 2005 Sept 7]. Disponível em: http://www.uptodate.com.
6. Ogura R, Hiasa Y, Takahashi T, Yamaguchi K, Fujiwara K, Ohara Y, et al. Specific findings of the standard 12-lead ECG in patients with “Takotsubo” cardiomyopathy: comparison with the findings of acute anterior myocardial infarction. Circ J. 2003; 67 (8): 687-90.
7. Hurst RT, Askew JW, Reuss CS, Lee RW, Sweney JP, Fortuin FD, et al. Transient midventricular ballooning syndrome: a new variant. J Am Coll Cardiol. 2006; 48: 579-83.
8. Vasconcelos JT, Martins S, Sousa JF, Portela A. Takotsubo cardiomyopathy: a rare cause of cardiogenic shock simulating acute myocardial infarction. Arq Bras Cardiol. 2005; 85 (2):128-30.
showed no significant lesions and left ventriculography displayed apical ballooning.
In the case described, the clinical and echocardiographic progress with resolution of the segment contraction confirmed
the diagnosis.
Despite the seriousness of the acute disease, the syndrome is transitory and treatment is essentially hemodynamic support measures.