BrazJOtorhinolaryngol.2016;82(3):285---288
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Electrochemotherapy
as
palliative
treatment
in
patients
with
thyroid
papillary
carcinoma
夽
Juan
José
Grau
a,
Miguel
Caballero
b,c,∗,
Cristobal
Langdon
c,
Manuel
Bernal-Sprekelsen
c,
Jose
Luis
Blanch
baDepartmentofMedicalOncology,HospitalClínicdeBarcelona,Institutd’InvestigacionsBiomèdiquesAugustPiiSunyer
(IDIBAPS),UniversidaddeBarcelona,Barcelona,Spain
bENTSurgicalOncologySection,DepartmentofMedicalOncology,HospitalClínicdeBarcelona,IDIBAPS,
UniversidaddeBarcelona,Barcelona,Spain
cDepartmentofOtorhinolaryngology,HospitalClínicdeBarcelona,IDIBAPS,UniversidadeBarcelona,Barcelona,Spain
Received4December2014;accepted7May2015 Availableonline21September2015
KEYWORDS
Bleomycin;
Electrochemotherapy; Headandneck cancer;
Palliativetherapy; Thyroid
Abstract
Introduction:Localprogressionofpapillarythyroidcarcinoma(PTC)afterfailureofstandard therapiesmaycausepain,ulceration,andbleeding.Aspatientsarefullyawareofthetumor growth,theymightsufferhighgradeanxiety.Electrochemotherapy(ECT)isanewlocal pallia-tivetreatmentforskinmetastasesofmalignantmelanomaorothertumors,includingsquamous headeneckcancerpatients.
Objective: ToevaluatetheimpactofECTinpatientswithlocalprogressionofPTC.
Methods:Four patients with local progression of PTC were treated with ECT based on Bleomycin,andevaluatedaccordingtotumorresponse,localpainandsideeffects.
Results:Inallcases,somegradeoftumorresponsewasobserved,lasting6,7,12and8months, respectively. Also,reductionoflocal painandanxietywas registeredinallpatients.Tumor infiltratedskinnecrosiswastheonlycollateraleffectofthetreatment.ECTinducedatumor responseinallPTCpatientswithimprovementofsymptoms.
Conclusions: ECTmaybeanoptionfor localpalliative treatmentinPTCpatients withlocal tumorprogression.
© 2015Associac¸˜aoBrasileira de Otorrinolaringologiae CirurgiaC´ervico-Facial.Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:GrauJJ,CaballeroM,LangdonC,Bernal-SprekelsenM,BlanchJL.Electrochemotherapyaspalliativetreatment
inpatientswiththyroidpapillarycarcinoma.BrazJOtorhinolaryngol.2016;82:285---8.
∗Correspondingauthor.
E-mail:mcaba@clinic.ub.es(M.Caballero). http://dx.doi.org/10.1016/j.bjorl.2015.05.008
286 GrauJJetal.
PALAVRAS-CHAVE
Bleomicina;
Eletroquimioterapia; Câncerdecabec¸ae pescoc¸o;
Terapiapaliativa; Tireoide
Eletroquimioterapiacomotratamentopaliativoempacientescomcarcinomapapilar datireoide
Resumo
Introduc¸ão:Aprogressãolocaldocarcinomapapilíferodetireoide(CPT)apósafalhadaterapia derotinapodecausardor,ulcerac¸ãoesangramento.Considerandoqueospacientesestão per-feitamente cientesdo crescimento tumoral, podem apresentarum alto grau deansiedade. A eletroquimioterapia (EQT) é um novo tratamento paliativo para metástases de pele de melanomamaligno oude outrostumores, inclusive em pacientescomcarcinoma escamoso decabec¸aepescoc¸o.
Objetivo:AvaliaroimpactodaEQTempacientescomprogressãolocaldeCPT.
Método: QuatropacientescomprogressãolocaldeCPTforamtratadoscomEQTcombaseem bleomicina,eavaliadosemrelac¸ãoaograuderespostatumoral,dorlocal,efeitoscolaterais.
Resultados: Emtodososcasos,foiobservadoalgumgrauderespostatumoral,queperdurou por6,7,12e8meses,respectivamente.Damesmaforma,foiregistradadiminuic¸ãodador localedaansiedadeemtodosospacientes.Necrosecutâneanainfiltrac¸ãotumoralfoioúnico efeitocolateraldotratamento.EQTinduziurespostatumoralemtodosospacientescomCPT, commelhoradossintomas.
Conclusões:EQTpodeserumaopc¸ãoparaotratamentopaliativotópicoempacientescomCPT comprogressãotumorallocal.
©2015Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaC´ervico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Localrelapseor regional neck metastasesafter failureof standardtherapiesofpapillarythyroidcarcinoma(PTC)are rare.However,patientsdevelopinglocalor regionaltumor progressionmaysufferfromanxiety,localpain,exudation, orbleeding.
Electrochemotherapy(ECT)isanewexperimental tech-nologybasedonincreasingcellmembranepermeabilityof the tumor cells (electroporation) to molecules. ECT con-sistsofthe administrationof electric pulses inthe tumor duringperfusionof chemotherapytofacilitate drug deliv-ery into malignant cells.1,2 ECT is now being used as a
palliativetherapy for cutaneousmetastases andheadand
neckcancer.3---7 A recentlypublished meta-analysisof 915
patientsstudiedtheresultsofskin-directedtherapyforlocal
cutaneousmetastases,includingelectrochemotherapy,
pho-todynamictherapy,radiotherapy,intralesionaltherapy,and
topicaltherapy.8Thehistologyofprimarytumorswasmainly
melanoma andbreast carcinoma,and none of themwere
thyroid carcinoma. ECT was more active than the other
skin-directed therapies, as a 59% complete response rate
wasreported,andtransientlocalpainoccurringin 49%of
patientsthatresolvedwithinamonthwasthemorecommon
sideeffect.
The authors present the preliminary results of a pilot
study ofthyroid cancer patients withprogressionof local
recurrenceorneckmetastasestreatedwithECT.
Methods
Inclusioncriteria
Patientsresistant to radioiodine and to anti-targetagent
Sorafenib with local tumor progression of PTC after
primary therapy (thyroidectomy, cervical neck dissection,
and adjuvant radioiodine), and after treatment of the
relapse (salvage cervical surgery and radiotherapy) were
included. Sorafenibresistancewasconsidered whena20%
increase inthe sumof diametersof thetarget lesionwas
observed.
Additionalinclusioncriteria:EasternCooperative
Oncol-ogyGroupperformancestatusof2orless,lifeexpectancyof
atleastthreemonths,noactiverespiratorydiseaseor
seri-ouschronicpulmonarydisease,absolutewhitebloodcount
above 4000cells/L, hemoglobin greater than 10g/dL,
platelet count above100,000L, and noprevious clinical
historyofallergytobleomycin.
The study was approved by the Institutional Review
Board.Informedconsentwasobtainedfromallpatients.
Treatment
Under total anesthesia, with an inspired oxygen fraction
(FiO2) of 36%or less, bleomycin,20mg/m2 IVwas
admin-isteredinabolus.Betweeneightand28minlater,electric
pulsesof100sand1000Vwereadministeredtothetarget
tumorbyanelectrode(modelN-30-HG;IGEAS.r.l.---Carpi,
Italy),poweredbyacommercial pulsegeneratorfor
elec-troporationtreatments(CLINIPORATOR;IGEAS.r.l.---Carpi,
Italy). Tumor tissue wastreated homogeneously, covering
theentiretargetvolume.
Responsecriteria
Radiological evaluation was performed at 0, 6, and 12
weeksafterECT,accordingtoResponseEvaluationCriteria
in Solid Tumor (RECIST) criteria (version 1.1).9 Symptom
Electrochemotherapyandthyroidcancer 287
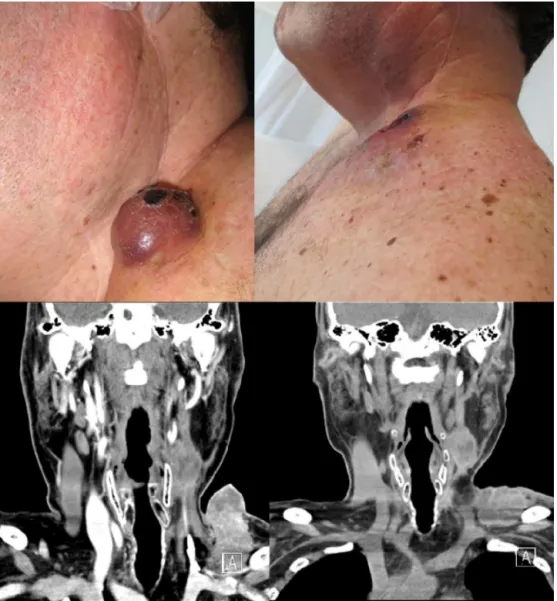
Figure1 Case1:ExternalaspectandCT-scanofalowerleftcervicalmassprior(leftimages)andafterfourweeks(rightimages) oftheelectrochemotherapy.
Edmonton Symptom Assessment System before treatment
and 12weeks after ECT.The patients subjectivelyscored
theintensityofthesesymptomsonavisualanalogicalscale
(VAS) between 0 (absence) and 10 (maximum intensity).
Toxicity and adverse events related to ECT were also
evaluatedat6,12,and24haftertheprocedure.
Duringthefollow-upperiod,thepatientswereevaluated
atleasteverythreemonthsorwhendiseaseprogressionwas
observed.
Results
Four consecutive patients, one male and three females,
wereenrolledinthestudy.Theagerangedbetween51and
60years.Thetargettumorwasalargecervicalmassinthree
patientsandskinmetastases(lessthan2cm)inone.
A clinical response was observed in all four patients
within the first three weeks after ECT (Fig. 1). These
findings were consistent with the radiological evaluation,
showingpartialresponse(PR)intwopatientsandtwocases
ofdisease stabilization withlowertumor burden, butnot
reachingthePRcriteriaasdefinedbyRECIST.
Thetargetedlesions’sizedecreasedoverthenextthree
monthsandremainedwithout progressionduringsixto12
months after the procedure. Three of the patients died
becauseofvisceral metastases, andtherewasnodisease
progressioninthetargetedlesionstreatedwithECT.Inone
case,thepatientdied18monthsafterECTduetolocaland
metastaticdiseaseprogression.
Thesymptomevaluationshowedamoderatedecreasein
thereportedmediannumericalscaleforanxiety(10---7)and
mildreductioninpain(7---6).Nosevereadverseeventswere
observedinthenext24h afterECT,apartfrommildlocal
paincontrolledwithnon-opioidanalgesia. The changesin
thetargetedlesionincludedpainlessskinnecrosis.
Discussion
ThisisthefirstreporttoassesstheclinicalefficacyofECTas
288 GrauJJetal.
using RECIST version 1.1.9 There were some difficulties
in the interpretation of the RECIST criteria. Firstly, some
increaseinthesizeofthelesioncouldbefound,especially
inthefirstfewweeks,attributedtothelocalinflammatory
reaction after ECT. In the two cases reported as ‘‘stable
disease’’, tumor response was observed in the central
partof thetumor, butthisis notevaluatedin theRECIST
criteria.
Patientsreported amoderate improvement in the two
most frequent tumor-derived symptoms: local pain and
anxiety. The treatment was well tolerated, and as the
administereddose of bleomycinwas below the maximum
tolerateddose, the procedure couldhave been repeated.
Noneofthepatientshadthetoxicitiesfrequentlyassociated
totreatmentswithbleomycin.10
PTC is commonly considered resistant to bleomycin
becauseitsunavailabilitytodiffusethroughthecell
mem-brane.ECTinduceselectroporationofthecellmembrane,
facilitatingtheentranceofbleomycinintothecellfromthe
plasma.2,11,12Oncethere,bleomycinappearstoactstrongly
against cell growth, inducing cell apoptosis that can be
observeduptoseveralweeksaftertheprocedure.13
The present results showed that ECT may be a valid
option as palliative local treatment in PTC patients with
local relapseor skin metastases. The number of patients
initiallyrecruited wassmall, but thatcould be explained
sincepapillarythyroid cancer is a highly curabledisease,
andbecausepatientswithprogressivediseasearerareand
allthecaseswerefromauniqueinstitution.Moreover,other
systemicchemotherapyagentsarecurrentlyunder
investi-gationforsuchpatients.
Itappearsthatthisproceduremayhaveanantitumoral
effect,particularlyin lesionssmaller than3cm.5 Another
meta-analysispublishedon413patientswithcutaneousand
subcutaneous tumors indicated that ECT had significantly
(p<0.001) higher effectiveness (by more than 50%) than
bleomycinorcisplatinaloneandthatECTwasmore
effec-tivein sarcoma thanin melanoma or carcinoma patients.
Nopatients withthyroid carcinoma werereported.14
Fur-therclinicaltrialswithmorepatientswillclarifytheroleof
thisprocedure.
Also,itshouldbedeterminedwhetheralargerelectrode
wouldenablereachingthetumormoreextensively,
poten-tiallyleadingtoimprovedresults.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
This study was supported by a research project grant
(PI09/90664)fromtheSpanishMinistryforScienceand
Inno-vationandbyaresearchprojectgrant(EC10-067)fromthe
Spanish Ministry of Health, Department of Pharmacy and
HealthProducts.
References
1.MiklavˇciˇcD,MaliB,KosB,HellerR,SerˇsaG. Electrochemother-apy:fromthedrawingboardintomedicalpractice.BiomedEng Online.2014;13:29.
2.LarkinJO,CollinsCG,AaronsS,TangneyM,WhelanM,O’ReilyS, etal.Electrochemotherapy:aspectsofpreclinicaldevelopment andearlyclinicalexperience.AnnSurg.2007;245:469---79. 3.GargiuloM,PapaA, Capasso P,MoioM,CubicciottiE,
Paras-candoloS.Electrochemotherapyfor non-melanomaheadand neck cancers: clinical outcomes in 25 patients. Ann Surg. 2012;255:1158---64.
4.LandstromFJ,NilssonCO,CrafoordS,ReizensteinJA,Adamsson GB,LofgrenLA.Electroporationtherapyofskincancerinthe headandneckarea.DermatolSurg.2010;36:1245---50. 5.MaliB,MiklavcicD,Campana LG,CemazarM, SersaG, Snoj
M,etal.Tumorsizeandeffectivenessofelectrochemotherapy. RadiolOncol.2013;47:32---41.
6.Mir LM, Orlowski S, Belehradek J Jr, Paoletti C. Elec-trochemotherapy potentiation of antitumour effect of bleomycinbylocalelectricpulses.EurJCancer.1991;27:68---72. 7.ReinholdU.Electrochemotherapyforprimaryskincancerand skinmetastasisrelatedtoothermalignancies.AnticancerDrugs. 2011;22:711---8.
8.SprattDE,GordonSprattEA,WuS,DeRosaA,LeeNY,Lacouture ME,etal.Efficacyofskin-directedtherapyforcutaneous metas-tases from advanced cancer: a meta-analysis. JClin Oncol. 2014;32:3144---55.
9.EisenhauerEA,Therasse P,Bogaerts J,Schwartz LH,Sargent D, Ford R, et al. New response evaluation criteria in solid tumours:revisedRECISTguideline(version1.1).EurJCancer. 2009;45:228---47.
10.AlbiolS, GrauJJ,Pereira A, Reguart N, Gascon P.Epidemic hemolytic-uremicsyndromerelatedtobleomycin. Haematolog-ica.2001;86:E10.
11.MirLM,OrlowskiS.Mechanismsofelectrochemotherapy.Adv DrugDelivRev.1999;35:107---18.
12.MMirLM,OrlowskiS.Thebasisofelectrochemotherapy. Meth-odsMolMed.2000;37:99---117.
13.MirLM, TounektiO, OrlowskiS.Bleomycin: revivalofanold drug.GenPharmacol.1996;27:745---8.