REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Incidence
of
community-acquired
infections
of
lower
airways
among
infants
Ana
Luisa
Oenning
Martins
a,
Deisy
da
Silva
Fernandes
Nascimento
a,
Ione
Jayce
Ceola
Schneider
b,
Fabiana
Schuelter-Trevisol
a,c,∗aUniversidadedoSuldeSantaCatarina(Unisul),Tubarão,SC,Brazil
bUniversidadeFederaldeSantaCatarina(UFSC),Florianópolis,SC,Brazil
cCentrodePesquisasClínicasdoHospitaNossaSenhoradaConceic¸ão,Tubarão,SC,Brazil
Received18June2015;accepted3September2015 Availableonline26October2015
KEYWORDS
Pneumonia; Bronchiolitis; Child; Epidemiology; Riskfactors
Abstract
Objective: Toestimatetheincidenceofcommunity-acquiredinfectionsofthelowerrespiratory tractandtheriskfactorsassociatedwithitsoccurrenceininfants,intheirfirstyearoflife. Methods: Aprospectivecohortstudyofinfantswhowerefollowedupduringthefirst12months oflife.Interviewswereconductedwiththeirmothers,andchildrenwereclinicallymonitored bimonthlytoinvestigatetheoccurrenceoftheincidencedensityofcommunity-acquired infec-tionsofthelowerrespiratorytract.Coxregressionanalysiswasusedtoestimatethecrudeand adjustedrelativeriskofthevariablesassociatedwiththeoutcome.
Results: Themeanageofthemotherswas26years,62%ofthemhadmorethan11yearsof schooling,and23.5wereatriskofsocialexclusionregardingeconomicincome.Theincidence density ofpneumonia and bronchiolitiswere, respectively, 0.51and3.10 episodesper 100 children-months.Childrenwho hadlow birthweight (<2500g)were5.96(95%CI1.75---20.40) timesmorelikelytohavepneumoniathaninfantsweighing2500gorover.
Conclusions: Theincidenceofacutelowerrespiratorytractinfectioninchildren wassimilar tothatfoundinotherstudies.Onlylowbirthweightwasanindependent riskfactorforthe occurrenceofpneumonia.
©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Pneumonia; Bronquiolite; Crianc¸a;
Incidênciadeinfecc¸õescomunitáriasdeviasaéreasinferioresemcrianc¸as
Resumo
Objetivo: Estimaraincidênciadeinfecc¸õescomunitáriasdeviasaéreasinferioreseosfatores deriscoassociadosàsuaocorrênciaemlactentesemseuprimeiroanodevida.
∗Correspondingauthor.
E-mail:[email protected](F.Schuelter-Trevisol).
http://dx.doi.org/10.1016/j.rppede.2015.10.005
2359-3482/©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY
Epidemiologia; Fatoresderisco
Métodos: Estudoprospectivode coortecomlactentesqueforamacompanhadosduranteos primeiros12mesesdevida.Foramrealizadasentrevistascomasmãeseascrianc¸asforam clini-camentemonitoradasbimestralmenteparainvestigaraocorrênciadadensidadedeincidência deinfecc¸õescomunitáriasdasviasaéreasinferiores.AanálisederegressãodeCoxfoiutilizada paraestimaroriscorelativobrutoeajustadodasvariáveisassociadascomodesfecho. Resultados: Aidademédiadasmãesfoide26anos,62%tinhammaisde11anosdeescolaridade, e23,5estavamemriscodeexclusãosocialemrelac¸ãoàrenda.Adensidadedeincidênciade pneumoniaebronquioliteforam,respectivamente,0,51e3,10episódiospor100crianc¸as-mês. Crianc¸ascombaixopesoaonascer(2.500gramas)foram5,96vezes(IC95%1,75---20,40)mais propensosaterpneumoniadoquecrianc¸ascompesode2.500gramasoumais.
Conclusões: Aincidênciadainfecc¸ãoagudadasviasaéreasinferioresemcrianc¸asfoi semel-hante àencontrada em outrosestudos. Apenas baixopesoao nascerfoi um fator de risco independenteparaaocorrênciadepneumonia.
©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Acuterespiratorytractinfections(ARIs)arealeadingcause ofmorbidityandmortalityamongchildren.In2010, infec-tiousdiseasescaused58%ofdeathsgloballyamongchildren younger than 5 years. Pneumonia, diarrhea and malaria accountedforone-thirdofdeathsinthisagegroup.1InLatin
America, respiratory infections were responsible for over
80,000deathsofchildren peryear,40%ofwhichoccurred
inBrazil.2The WorldHealthOrganization (WHO)considers
that bronchiolitis and pneumonia arethe most important
epidemiologicalcomponentsofARIsinearlychildhood.3
Bronchiolitis is an acute infection of the small
air-waysthatprimarilyaffectsyounginfants,oftenthoseaged
between2 and24months.The diseasefollowsa seasonal
pattern, with peaks during the winter in temperate
cli-mates, and during the rainy season in tropicalclimates.4
Pneumonia is a leading cause of morbidity and mortality
amongchildrenyoungerthanfiveyears,with95%ofcases
occurring in developing countries.3 Previous studies have
listed therisk factors for acquiringrespiratoryinfections,
among which are socioeconomic factors (low household
income,poorparentaleducation,andhighnumberof
per-sonsper household),earlycessationofbreastfeeding,low
birth weight, malnutrition, passive smoking, and daycare
attendance.5,6
Inthiscontext,theaimofthisstudywastoestimatethe
incidence of community-acquired lower respiratory tract
infections, and the risk factors associated withits
occur-rence in infants up to one year old in Tubarão, southern
Brazil.
Method
ThisstudywasapprovedbytheResearchEthicsCommittee oftheUniversityofSouthernSantaCatarina(codenumber 12.035.4.01III)onApril27,2012.
This is aprospective cohort study.The municipality of Tubarão is home to 96,284 residents. According to the InformationTechnologyDepartmentoftheNationalHealth System(DATASUS),around2000childrenareborninTubarão yearly(averageforthelast10years),above80%peryear,
onaverage,inthematernityofHospitalNossaSenhora da Conceic¸ão (HNSC).The HNSCis referencecenter andit is theonly hospitalthat provides neonatalintensive care in theregion.Itisa‘‘Baby-friendlyhospital’’since2001.
Itisestimatedthatone-thirdofinfantshaveatleastone episodeoflowerrespiratorytractinfectionintheirfirstyear oflife.7Thesamplesizecalculationconsideredthe
follow-ing:exclusivebreastfeedingisthemainprotectivefactorfor
reducinglowerrespiratory tractinfections (LRTIs);
reduc-tionof LRTIprovided by exclusive breastfeeding in about
65%8;powerof80%;alphaerrorof5%;and95%significance
level.A20%additionwasmadetocoverpossiblelossesto
follow-up,totalingaminimumsamplesizeof106subjects.
Data were collected between June 2012 and
Septem-ber2013frommothersof newbornbabiesat theHospital
NossaSenhora daConceic¸ão.After gettinga written
con-sentform,theparticipantswereinterviewedtocollectdata
regardingprenatalcare,deliverydetails,anddemographic
and socioeconomic characteristics of the family. Mothers
whoagreedtoparticipateweregivenahealthdiarytomake
weeklynotes about their child’sclinical data. The health
diaries werecollected at each medical appointment,and
newoneswerehanded out.Childcarewasprovidedtoall
children included in the study,with bimonthly scheduled
medicalappointments fora one-yearperiod.Duringthese
visits,clinicalfollow-updatawerecollected,and
confirma-tionofdataprovidedbymothersinthehealthdiarieswas
made.Sixmedicalappointmentswereprovidedtoeachchild
overaone-yearperiod.Thechildrenwereseenbyphysicians
whowerepediatriciansandprofessorsatthemedicalschool
attwooutpatientclinicsrunbytheUniversityofSouthern
SantaCatarina.
Inthisstudy,pneumoniaandbronchiolitiswerediagnosed
byaphysicianwhenthebaby’smothersoughthealthcare.
Symptoms associated with pneumonia were cough, fever,
andradiographicchangestoconfirmthediagnosis,whereas
symptoms associated with bronchiolitis were tachypnea,
coughandwheezingwithpresenceorabsenceoffeverand
coryza.Thedatawerecollectedduringthepediatricvisits
andreportedbythemothers.
The Open Source Epidemiologic Statistics for Public
Health (OpenEpi), version 2.3.1 was used to calculate
First level
• Chid’s gender • Per capita income • Maternal age and education
• Low birth weight • Breastfeeding
• Crowding • Daycare attendance • Passive smoking Second level
Third level
Figure1 Descriptionofhierarchicalanalysisforacute respi-ratorytractinfections.
EpiDataprogramversion3.1(EpiDataAssociation,Odense, Denmark),andstatisticalanalysiswasperformedusingthe StatisticalProductandServiceSolutionssoftware(SPSS)for Windows,version20(IBMSPSSStatistics,Chicago,IL,USA). Theoutcomeincidencewascalculatedasincidencedensity rate,expressedasthenumber ofeventsper person-time. Coxregressionanalysiswasusedtocalculatethecrudeand adjusted relative risk for outcome variables. The signifi-cancelevelwassetat5%.Multivariateanalysiswasusedfor adjustmentofconfoundingfactors,accordingtothe hierar-chicalmodelproposedbyVictoraetal.,9asshowninFig.1.
Results
Between June 2012 and September 2013, 210 interviews were conducted with nursing mothers. Fig. 2 shows a
flowchartdemonstratingtheselectionofstudyparticipants.
The sample with complete data consisted of 187 infants
(89.0%),ofwhom87(46.5%)weremale.The mean
mater-nal agewas26 years(range, 14---45years). Regardingthe
socioeconomic status, the median household income was
BRL 1866.00, whereas calculating 60% of the median per
capita income, which is a parameter used by the
Brazil-ianInstituteofGeographyandStatistics(IBGE)toindicate
relativepoverty,resultedinBRL248.80.Withregardto
edu-cation,62.0%(95%CI:54.5---69.0)ofthenursingmothershad
morethan11yearsofschoolattendance,and65.8%(95%CI:
59.1---72.6)ofthe respondentslivedwithmorethan three
people in the same home. Only 27 (14.4%) infants were
exclusivelybreastfeduntilsixmonthsofage.
Duringthe study period,therewere 11cases of
pneu-monia (6.5%, corresponding to 0.51 episodes per 100
children-month) and71cases of bronchiolitis(42.3%,
cor-respondingto3.10episodesper100children-month).Only
1infanthadpneumoniaontwooccasions,ateightandten
monthsofage.Regardingbronchiolitis,14childrenhadone
recurrentepisode,4children hadtworecurrentepisodes,
and1childhadfourepisodesofbronchiolitisduringthefirst
yearoflife. OfallchildrenwhowerediagnosedwithARI,
only1washospitalizedforpneumoniainthefirstmonthof
life.Table1presentsthedataregardingtheexposuretoARIs
andperinatalriskfactors(Fig.1).
UsingCoxregressionanalysis,lowbirthweightwas
asso-ciated with the occurrence of pneumonia. Children who
Excluded
15 admitted to the ICU 220 non-residents at the study site
140 decline to participate
Baseline clinical assessment: 210
22 Lost to follow-up 1 Dead
Clinical follow-up: 187 children 585 newborns between June and
September 2012
Lost to follow-up: 3 with 6 months 6 with 8 months 4 with 12 months
Analyzed: 187 children (person-time)
Figure2 Flowchartofstudyparticipants.
werebornweighinglessthan2500gwere5.83timesmore likely to develop pneumonia than normal birth weight infants.Nosignificantassociationwasfoundbetween pneu-monia and breastfeeding, daycare attendance, passive smoking, and other studied variables. No significant asso-ciationsbetweenbronchiolitisandthestudyvariableswere found.Table2showstherelativeriskofthevariable
adjust-mentsusingahierarchicalmodel.
None of the maternal risk factors (household income,
age,educationlevel,andnumberofpersonsperhousehold)
wereassociatedwithARIsinthepresentstudy.
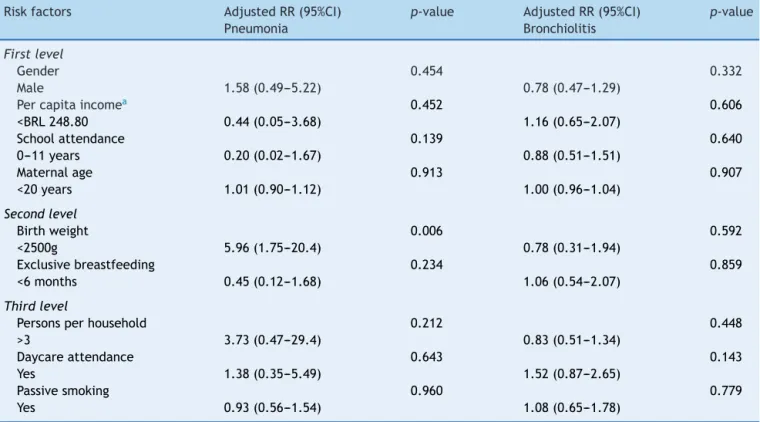
After relative risk adjustments according to the
hier-archical model, lowbirth weight wasassociated withthe
occurrenceof pneumonia.Childrenwhowereborn
weigh-inglessthan2500gwere5.96(95%CI1.75---20.4)timesmore
likelytodeveloppneumoniacomparedwiththoseweighing
2500gormore.
Table1 Perinatalriskfactorsandexposuretoacute respi-ratorytractinfections(n=187).
n % 95%CIa
Birthweight<2500g 17 9.1 5.4---13.4
GenderMale 87 46.5 39.6---53.5
Passivesmoking 53 28.3 21.9---34.8 Daycareattendance 28 15.0 10.2---20.9 Exclusivebreastfeeding
<6months
89 47.6 40.6---54.5
Table2 Relativerisk ofvariablesregardingpneumonia andbronchiolitisadjustedaccordingtothehierarchicalmodel for estimatingincidencedensity.
Riskfactors AdjustedRR(95%CI) p-value AdjustedRR(95%CI) p-value
Pneumonia Bronchiolitis
Firstlevel
Gender 0.454 0.332
Male 1.58(0.49---5.22) 0.78(0.47---1.29)
Percapitaincomea 0.452 0.606
<BRL248.80 0.44(0.05---3.68) 1.16(0.65---2.07)
Schoolattendance 0.139 0.640
0---11years 0.20(0.02---1.67) 0.88(0.51---1.51)
Maternalage 0.913 0.907
<20years 1.01(0.90---1.12) 1.00(0.96---1.04)
Secondlevel
Birthweight 0.006 0.592
<2500g 5.96(1.75---20.4) 0.78(0.31---1.94)
Exclusivebreastfeeding 0.234 0.859
<6months 0.45(0.12---1.68) 1.06(0.54---2.07)
Thirdlevel
Personsperhousehold 0.212 0.448
>3 3.73(0.47---29.4) 0.83(0.51---1.34)
Daycareattendance 0.643 0.143
Yes 1.38(0.35---5.49) 1.52(0.87---2.65)
Passivesmoking 0.960 0.779
Yes 0.93(0.56---1.54) 1.08(0.65---1.78)
a Cut-offpoint:60%ofmedianincome.
Discussion
Inthepresentstudy,therewasahighcumulativeincidence ofbronchiolitis(42.3%)andpneumonia(6.5%),which high-lightstherelevanceoftheserespiratorymorbiditiesamong children. These findings areconsistent withseveral other studiesthatconsiderARIsascommoneventsduringinfancy and childhood.However,publishedstudies show variation inthe incidenceofpneumonia andbronchiolitis,probably duetodifferentcriteriafordefiningtheincidenceofthese occurrences.Inastudyconductedon936children,Aldous
etal.10 reportedthat32%ofthestudyparticipantshadat
leastoneepisodeofARIinthefirstyearoflife.Flaherman
etal.11carriedoutaretrospectivecohortstudyon123,264
children inCalifornia andreportedthat 16.7% ofchildren
developed bronchiolitis before the second year of life. A
recentstudyconductedinSouthAfricafoundthat87.4%of
children under5yearsof agehadat least oneepisodeof
bronchiolitisorpneumoniainan18-monthperiod.Ofthese
children,10.5% hadtwoARIepisodes,and1.7%hadthree
episodes.12 Bates et al.13 reported that 49.5% of infants
whoparticipated in their studyin Nepal had bronchiolitis
orpneumonia.
The incidencedensity ofbronchiolitis(3.1episodesper
100 children-months) and pneumonia (0.51 episodes per
100children-months)inthepresentstudycanbecompared
withfindingsfromdifferentauthors.Inarecentsystematic
review, Rudanetal.14 found a mean incidencedensity of
pneumonia(1.83 episodesper100children-month) among
childrenunderfiveyearsofageinlowandmiddleincome
countries. In another study conducted on children under
fiveyearsofage,anincidencedensityofpneumoniaof2.4
episodesper 100children-month wasfound in developing
countries.3Weberetal.15reportedthattheincidence
den-sity of bronchiolitis in Gambia was 7.3 episodes per 100
children-month among children aged 19---25 months. In a
cohortstudyconductedonchildrenfrombirthtothreeyears
old,Brooretal.16reportedthattheincidencedensityofARIs
was4.5episodesper 100 children-monthin infantsunder
oneyearofage,withoutdiscriminatingbetween
bronchioli-tisandpneumonia.
Inthe currentstudy,low birth weightwasan
indepen-dentriskfactorfortheoccurrenceofpneumonia.Children
whowereborn weighing less than2500g were5.96 times
more likelyto get pneumonia than those weighing 2500g
ormore.Prietschetal.2found thattheprevalenceof ARI
was10%higherinchildrenwithlowbirthweightcompared
withnormalbirthweightinfants.Lowbirthweighthasbeen
associated with severe pneumonia and increased risk of
mortalityinseveralstudies.17,18Usingacase-controlstudy,
Nascimentoetal.19 foundthat lowbirth weightincreased
twicetheriskof hospitalizationforpneumonia. Thesame
authorexplains that children with low birth weight have
decreasedimmuneresponseandimpairedpulmonary
func-tiondue tothe smallerdiameterofthelarge airwaysand
easier obstruction of peripheral airway than normal birth
weightinfants.20However,thecausalrelationshipbetween
lowbirthweightandtheoccurrenceofpneumoniais
com-plex, representing a cumulative effect of a number of
nutritionalandnon-nutritionalprenatalexposure.21
Severalstudies have shown that breastfeedingreduces
ameta-analysisconductedonupto2-year-oldchildrenin
developed countries, Bachrach et al.7 found that
breast-feedingwasaprotectivefactor:exclusivebreastfeedingfor
morethanfourmonthscanreduce by70%theriskof
hos-pitalizationfor respiratory diseases. In thecurrent study,
noassociation between breastfeedingand theoccurrence
ofARIswasobserved.InstudiesconductedbyNascimento
et al.19 and by Pavi´c et al.,24 breastfeeding also showed
no protective effect against these infections. A possible
explanationfortheseconflictingresultsisthat
breastfeed-ingreducesthediseaseseverityandriskofhospitalization
forARIs,butitdoesnoteliminatetheoccurrenceofthese
infections.
Only 15% of children who participated in this study
attendeddaycare centers,andtheyhadnogreaterriskof
ARIsthanthosewhodidnotattend,accordingtothe
anal-yses performed. In a case---control study, Macedo et al.22
found no significant association between daycare
atten-danceandincreasedhospitalizationfor ARI. Theseresults
areindisagreementwithmostofthestudiesthatassociate
daycareattendancewithasignificantincreasein the
inci-denceandprevalence of ARIs.25,26 Possibly, theyattended
daycare centers with adequate ventilation, hygiene, and
careconditions,whichprovidedsimilarconditionstothose
athome. Moreover,the resultsmay havebeen influenced
bythelow percentageof childrenattendingdaycare
cen-ters.Inaddition,thelengthofdaycareattendancewasnot
investigated,whichcouldalsoexplainthelackofassociation
betweenthesevariables.
Regarding passive smoking, 28.3% of children were
exposedtosecondhandsmokeforlivingwithsmokersinthis
study.However,thisvariablewasnotasignificantrisk
fac-torforARI,whichcontradictsmoststudiesthatlinksmoking
withtheoccurrenceof bronchiolitis.27---29 Welliveretal.,30
however,foundnoassociationbetweenpassivesmokingand
acutebronchiolitis,butwithsubsequentrecurrent
wheez-ing.Withregardtopneumonia,manystudieshavealsofound
noassociationbetweenpassivesmokingandtheoccurrence
of the disease.19,23,26 In addition, this study has neither
quantifiedthechildren’stobaccointakenormeasuredthe
frequencyof exposuretotobacco,which mayexplainthe
lackofassociation.Noneofthematernalriskfactors
(house-holdincome, age,educationlevel,andnumberofpersons
per household) were associated with ARIs in the present
study.The high percentageofmothers withmorethan11
years of school attendance (62%) may have favored the
absenceofassociationbetweenpooreducationand
occur-renceofoutcomesinthiscohort.
This study has some limitations thatshould bekept in
mindwhen interpreting the results. The follow-up period
wasrathershorttoexaminewhether theresults had
sta-tistical significance. The lack of environmental quality
assessmentof theairwasanotherlimitationof thestudy.
Itiswellknownthatairpollutionisanimportantriskfactor
forthedevelopmentofARIs,butchildrenwhoparticipated
inthisstudylivedincitieswhere therewasnosystematic
monitoringofairqualityandexposureassessment.Itshould
alsobementionedthatthereisanotherprivatematernity
hospitalinthemunicipalityforthosewhocanaffordtopay
foritorhaveahealthcareplan.Thus,thesampleincluded
inthisstudymayhavepresentedahomogeneous
socioeco-nomicstatus,which couldhave influencedtheabsenceof
association between familyincomeandtheoccurrence of
outcomes.
The incidence density of pneumonia and bronchiolitis
were 0.51 and 3.10 episodes per 100 children-months,
respectively. Therewasnosignificantcorrelation between
theoccurrenceofbronchiolitisandthevariablestested.
Basedontheresultsfromthisstudy,itcanbeconcluded
thatchildrenwhowerebornweighinglessthan2500ghave
higherriskofpneumoniathannormalbirthweightinfants,
whichhighlightstheneedforfurtherstudiestoidentify
fac-torsrelatedtolowbirthweightandpreventivemechanisms
topreventtheoccurrenceofthedisease.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.WorldHealthOrganization[homepageontheInternet].Causes ofchildmortalityfortheyear 2010. Availablefrom:http:// www.who.int/gho/childhealth/mortality/causes/en/index.
html[accessed07.11.12].
2.PrietschSO,FischerGB,CésarJA,LempekBS,BarbosaLV,Zogbi L,etal.Acutelowerrespiratoryillnessinunder-fivechildren inRioGrande,RioGrandedoSulstate,Brazil:prevalenceand riskfactors.CadSaudePublica.2008;24:1429---38.
3.RudanI,Boschi-PintoC,BiloglavZ,MulhollandK,CampbellH. Epidemiologyandetiologyofchildhoodpneumonia.BullWorld HealthOrgan.2008;86:408---15.
4.AmericanAcademyofPediatrics,SubcommitteeonDiagnosis, Management of Bronchiolitis. Diagnosis and management of bronchiolitis.Pediatrics.2006;118:1774---93.
5.Lopes CR, Berezin EN. Fatores de risco e protec¸ão à infecc¸ãorespiratóriaagudaemlactentes.RevSaudePublica. 2009;43:1030---4.
6.Rodríguez L, Cervantes E, Ortiz R. Malnutrition and gas-trointestinal and respiratory infectionsin children: a public health problem. Int J Environ Res Public Health. 2011;8: 1174---205.
7.BachrachVR,SchwarzE,BachrachLR.Breastfeedingandthe riskofhospitalizationforrespiratorydiseaseininfancy:a meta-analysis.ArchPediatrAdolescMed.2003;157:237---43.
8.DuijtsL,JaddoeVW,HofmanA,MollHA.Prolongedand exclu-sivebreastfeeding reducesthe risk ofinfectious diseases in infancy.Pediatrics.2010;126:18---25.
9.VictoraCG,HuttlySR,FuchsSC,OlintoMTA.Theroleof con-ceptualframeworksinepidemiologicalanalysis:ahierarchical approach.IntJEpidemiol.1997;26:224---7.
10.Aldous MB, Holberg CJ, Wright AL, Martinez FD, Taus-sig LM. Evaporative cooling and other home factors and lower respiratory tract illness during the first year of life. GroupHealth MedicalAssociates.Am JEpidemiol.1996;143: 423---30.
12.Sinha A,Kim S,Ginsberg G, FranklinH, Kohberger H, Strut-tonD,etal.Economicburdenofacutelowerrespiratorytract infectioninSouthAfricanchildren.PaediatrIntChildHealth. 2012;32:65---73.
13.Bates MN, Chandyo RK, Valentiner-Branth P, Pokhrel AK, MathisenM,BasnetS,etal.Acutelowerrespiratoryinfectionin childhoodandhouseholdfueluseinBhaktapur,Nepal.Environ HealthPerspect.2013;121:637---42.
14.RudanI,O’BrianKL,NairH,LiuL,TheodoratouE,QaziS,etal. Epidemiologyandetiologyofchildhoodpneumoniain2010: esti-matesofincidence,severemorbidity,mortality,underlyingrisk factors and causative pathogens for 192 countries. JGlobal Health.2013;3:010401.
15.WeberMW,MilliganP,GiadomB,PateMA,KwaraA,SadiqAD, etal.Respiratoryillnessaftersevererespiratorysyncytialvirus diseaseininfancyinTheGambia.JPediatr.1999;135:683---8.
16.BroorS,ParveenS,BharajB,PrasadVS,SrinivasuluKN,Sumanth KM,etal.Aprospectivethree-yearcohortstudyofthe epidemi-ologyandvirologyofacuterespiratoryinfectionsofchildrenin ruralIndia.PLoSOne.2007;2:e491.
17.ColesCL,FraserD,Givon-LaviN,GreenbergD,GorodischerR, Bar-ZivJ,etal.Nutritionalstatusanddiarrhealillnessas inde-pendentriskfactorsforalveolarpneumonia.AmJEpidemiol. 2005;162:999---1007.
18.Suwanjutha S, Ruangkanchanasetr S, Chantarojanasini T, HotrakityaS.Riskfactorsassociatedwithmorbidityand mor-talityofpneumoniainThaichildrenunder5years.Southeast AsianJTropMedPublicHealth.1994;25:60---6.
19.NascimentoLF,MarcitelliR,AgostinhoFS,GimenesCS.Análise hierarquizadadosfatoresderiscoparapneumoniaemcrianc¸as. JBrasPneumol.2004;30:445---51.
20.WilcoxAJ. Ontheimportance ---and the unimportance--- of birthweight.IntJEpidemiol.2001;30:1233---41.
21.RothDE,CaulfieldLE,EzzatiM,BlackRE.Acutelower respi-ratoryinfectionsinchildhood:opportunitiesforreducingthe global burden through nutritional interventions. Bull World HealthOrgan.2008;86:356---64.
22.MacedoSE,MenezesAM,AlbernazE,PostP,KnorstM.Risk fac-tors for acute respiratorydisease hospitalization inchildren underoneyearofage.RevSaudePublica.2007;41:351---8.
23.VictoraCG,FuchsSC,FloresJA,FonsecaW,KirkwoodBR.Risk factorsforpneumoniaamongchildreninaBrazilian metropoli-tanarea.Pediatrics.1994;93:977---85.
24.Pavi´cI,Jurkovi´cM,PastarZ.Riskfactorsforacuterespiratory tractinfectionsinchildren.CollAntropol.2012;36:539---42.
25.FonsecaW,KirkwoodBR,BarrosAJD,MisagoC,CorreiaL,Flores JAM.Attendanceatdaycarecentersincreasestheriskof child-hoodpneumoniaamongtheurbanpoorinFortaleza,Brazil.Cad SaudePublica.1996;12:133---40.
26.FuchsSC,MaynartRC,CostaLF,CardozoA,SchierholtR.Tempo depermanêncianacrècheeinfecc¸ãorespiratóriaaguda.Cad SaudePublica.1996;12:291---6.
27.VonLinstowM-L,HolstK,LarsenK,KochA,AndersenPK,Høgh B.Acuterespiratorysymptomsand generalillnessduringthe firstyearoflife:apopulation-basedbirthcohortstudy.Pediatr Pulmonol.2008;43:584---93.
28.SempleMG,Taylor-RobinsonDC,LaneS,SmythRL.Household tobaccosmokeand admissionweightpredictsevere bronchi-olitisininfantsindependentofdeprivation:prospectivecohort study.PLoSOne.2011;6:e22425.
29.Simões EA, Maternal smoking. asthma, and bronchioli-tis: clear-cut association or equivocal evidence? Pediatrics. 2007;119:1210---2.