SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Amputation
risk
after
the
revascularization
procedures
in
sarcoma
resections
夽
Luiz
Eduardo
Moreira
Teixeira
a,b,∗,
Thiago
Marques
Leão
c,
Daniel
Barbosa
Regazzi
c,
Cláudio
Beling
Gonc¸alves
Soares
baUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,BeloHorizonte,MG,Brazil
bHospitalMadreTeresa,Servic¸odeOrtopediaeTraumatologia,BeloHorizonte,MG,Brazil
cUniversidadeFederaldeMinasGerais(UFMG),HospitaldasClínicas,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received2May2016 Accepted30August2016 Availableonline21October2017
Keywords:
Softtissuesarcoma Osteosarcoma Limbsalvage Amputation
Reconstructivesurgicalprocedures
a
b
s
t
r
a
c
t
Objective:Theobjectiveofthisstudyistoevaluatetheefficacyofvascularreconstructive surgeryafterresectionofboneandsofttissuetumorsinextremitiesandtheriskof progres-siontoamputation.
Methods:This is a retrospective, observationaldata collection frommedical recordsof patientswhounderwentresectionofboneandsofttissuetumorsintheperiodof2002–2015. Thirteenpatientsmettheinclusioncriteria,whichevaluatedthecorrelationsbetween cer-tainfactors(gender,tumortype,location,reconstruction,revascularizationandpatency, infection)withamputationinthepostoperativeperiod.
Results:Inthisstudy,ofthe13patientsundergoingreconstruction,five(38.46%)evolved toamputation.Allpatientswhoprogressedtoamputationhadthefollowingincommon: presenceofbonesarcoma(p=0.005),havingundergonereconstructionwithanorthopedic prosthesis(p=0.005),lackofvascularpatencyintherevascularizationsiteinthe postopera-tiveperiod(p=0.032),andsurgicalsiteinfection(p=0.001).Noneofthepatientswithsoft tissuesarcomaunderwentamputation,andtheonlypatientwithbonesarcomawhodid notundergoamputationhadnoinfectionandmaintainedvascularpatencyofthegraft. Conclusion:Theoccurrenceofinfectionappearstobeoneofthemainriskfactorsforfailure ofrevascularization,especiallyincasesofbonesarcomainwhichvascularreconstruction isperformedwithplacementofanon-conventionaljointprosthesis.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalMadreTeresa,Servic¸odeOrtopediaOncológica;andUniversidadeFederaldeMinasGerais,Hospitaldas Clínicas,BeloHorizonte,MG,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.E.Teixeira). http://dx.doi.org/10.1016/j.rboe.2017.10.005
Risco
de
amputac¸ão
após
procedimento
de
revascularizac¸ão
nas
ressecc¸ões
de
sarcoma
Palavras-chave:
Sarcomadetecidosmoles Osteossarcoma
Salvamentodemembro Amputac¸ão
Procedimentoscirúrgicos reconstrutivos
r
e
s
u
m
o
Objetivo: Oobjetivodesteestudoéavaliaraeficáciadacirurgiadereconstruc¸ãovascular apósressecc¸ãodetumoresósseosetecidosmolesemextremidadeseoriscodeevoluc¸ão paraamputac¸ão.
Métodos: Estudoretrospectivo,observacional,decoletadedadosemprontuáriomédicode pacientessubmetidosaressecc¸ãodetumoresósseosedetecidosmolesde2002a2015;13 pacientespreencheramocritériodeinclusão,foramavaliadasascorrelac¸õesde determina-dosfatores(gênero,tipodetumor,localizac¸ão,reconstruc¸ão,revascularizac¸ãoepatência, infecc¸ão)comamputac¸ãonopós-operatório.
Resultados: Nopresenteestudo,dos13pacientessubmetidosàreconstruc¸ão,cinco(38,46%) evoluíram comamputac¸ão.Todos ospacientesqueevoluíram comamputac¸ãotinham emcomumofatodeserportadoresdesarcomaósseo(p=0,005),tersidosubmetidosa reconstruc¸ãocompróteseortopédica(p=0,005)enãoapresentarpatênciavascularnolocal darevascularizac¸ãonoperíodopós-operatório(p=0,032),alémdeapresentarinfecc¸ãono localdacirurgia(p=0,001).Nenhumdospacientesportadoresdesarcomadepartesmoles foisubmetidoàamputac¸ãoeoúnicopacientedogrupocomsarcomaósseoquenãosofreu amputac¸ãonãoapresentavainfecc¸ãoemantinhapatênciavascularnoenxerto.
Conclusão:Aocorrênciadeinfecc¸ãopareceserumdosprincipaisfatoresderiscoparaa falên-ciadarevascularizac¸ão,especialmentenoscasosdesarcomaósseoemqueareconstruc¸ão vascularéfeitajuntamentecomcolocac¸ãodeprótesesarticularesnãoconvencionais.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Primarymalignanttumorsofthemusculoskeletalsystemare rare, accountingfor1%ofall typesofcancer1–9;surgery is
the primary method of treatment. Currently, limb preser-vation is possible in 80% of cases. A few decades ago, involvement of large vessels by tumors was an indica-tionforamputation.1,2,7,10,11However,withtheimprovement
of imaging techniques and adjuvant treatment, it has becomepossibletouse vascular reconstructiontechniques without harm regarding relapse or metastatic dissemina-tion ofthe disease,which increases the limbpreservation rate without compromising survival or recurrence of the disease.2,8–10
Vascularreconstructioninpatientsundergoingsurgeryfor resectionofsarcomashasproventobeaviablemethodinlimb salvageprocedures;autologousgraftsorvascularprostheses madeofsyntheticmaterials,suchaspolytetrafluoroethylene (PTFE),canbeused.1,3–9,11,12
Umezawaet al.1 assessed23 patientswithbone orsoft
tissuetumorsinthelowerlimbswhounderwentextensive resectionswithvascularstructureresection;totalamputation wasavoidedinallpatients.Emorietal.3 evaluatedpatients
withsofttissuesarcomaslocatedintheinguinalregionwho underwenttumorresectionandrequiredvascular reconstruc-tion;innineofthetenpatientsintheirstudy,preservation oftheaffectedlimbwaspossible.Otherauthorshaveshown good results of vascular reconstruction as a limb salvage technique.4,6,8
Basedonthesedata,thisstudy aimedtoassesstherisk ofamputationafterarterialreconstructioninboneandsoft tissuesarcomasattheextremities,andthefactorsassociated withfailureofthesalvageprocedure.
Material
and
methods
Thisisaretrospective,observationalstudyofdatacollection inmedicalrecordsofpatientswhounderwentboneandsoft tissuetumorresectionfrom2002to2015.
Thestudyincludedpatientswho,duringtumorresection, requiredinterventionbythevascularsurgeryteamfora vas-cularreconstructionprocedure;theprocedurewasindicated priortoorduringsurgery.Patientsinwhomthevascular pro-ceduredidnotrequirereconstruction(suchasarteriorrhaphy), thosewithincompletedatainthemedicalrecord,thosewith lessthansixmonthsoffollow-up,andthosewhodidnotagree toparticipatewereexcludedfromthestudy.
Thestudiedvariableswere:
1. Age 2. Gender
3. Reconstruction level (iliofemoral, femoropopliteal, poplitealtibial,brachial)
4. Typeoftumor(bone,softtissue) 5. Typeofreconstruction(prosthesis,graft) 6. Postoperativeinfection
Fig.1–(A)Vascularprosthesis;(B)invertedsaphenousveingraft.
The statistical analysis was performed initially by a descriptive study of frequencies, expressed as mean and standard deviation (SD). The comparative study was con-ductedinitiallybyunivariateanalysisusingthechi-squared testwithorwithoutcorrectionbyFischer’sexacttestfor qual-itativevariables.Continuous variableswere analyzedusing Student’s t-test. The multivariate analysis was performed using multiple logistic regression, including variables with p<0.25.ThestudywasperformedusingSPSS® software ver-sion21.0(Chicago,USA),consideringassignificantp-values ≤0.05.
Results
Atotalof279patientsunderwentresectionofboneandsoft tissuesarcomasduringthestudyperiod.Ofthese,13required vascularreconstruction(12withinvertedsaphenousveingraft andonewithsyntheticgraft);allwereincludedinthestudy. Fig.1AandBpresentsimagesofvascularreconstructions.
Thepatient’s age variedfrom 12 to 68 years;the mean agewas36.46yearsandthemedian,35years.Nine(69.23%) patients were male and four (30.77%), female. Six (46.15%) patientshadbonesarcoma(onefibrosarcoma,one pleomor-phicsarcoma,onechondrosarcoma,andthreeosteosarcomas) and seven (53.85%) had soft tissue sarcomas (four malig-nantfibroushistiocytomas,onesofttissueEwing’ssarcoma, onesynovialsarcoma,andonehemangiopericytoma).Seven (53.85%)patientsunderwentradiationtherapy(oneinthe pre-operative periodand six in the postoperative period), and seven(53.85%)chemotherapy(threeinthesofttissuesarcoma groupandfourinthebonesarcomagroup).Epidemiological dataaresummarizedinTable1.
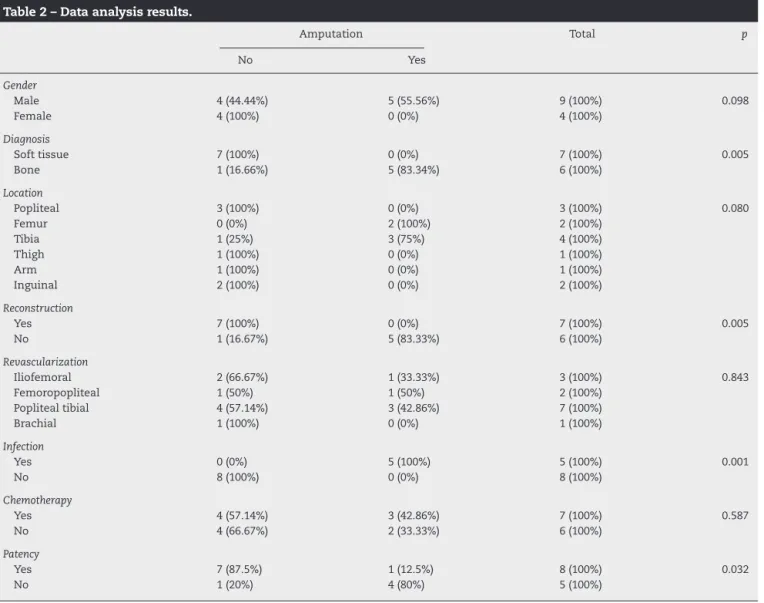
Amputation was required in five (38.46%) of the 13 patientsthathadrevascularizationproceduresaftersarcoma resection.Sevenpatients(53.85%) hadsoft tissuesarcomas andsix(46.15%)hadbonesarcomas.Allpatientswhoevolved toamputationhadbonesarcoma(p=0.005).Regardinggender, althoughthefivepatientswhounderwentamputationwere male,theresultwasnotstatisticallysignificant(p=0.98).
Reconstructionwithosteoarticularprosthesisofthe oper-atedsegmentwasperformedinsix(46.15%)patients,allwith bonesarcoma;ofthese,five(83.33%)evolvedwithexigencyfor amputation,astatisticallysignificantresult(p=0.005).
Regardingthelevelofrevascularization,inthree(23.08%) patients, it was performed at the iliofemoral level, in two (15.38%) at the femoropopliteal, in seven (53.85%) at the popliteal tibial, and in one (7.69%) at the brachial level. Five casesrequired amputation, one(20%) casewith revascularization at the iliofemoral level, one (20%) at the femoropopliteal,andthree(60%)atthepoplitealtibiallevel (p=0.843).
Five (38.46%) ofthe 13(100%) casesoperated,developed postoperative infection and eight (61.54%) had no infec-tion. A statistically significant association (p=0.001) was observedbetweentheoccurrenceofpostoperativeinfection andexigencyforamputation;ofthefiveinfectedpatients,all underwentamputation,whereasinthegroupwithout infec-tion,noneofthepatientsrequiredamputation.
Seven (53.85%) of the 13 patients had undergone prior chemotherapy and six (46.15%) had not. Ofthe cases that receivedchemotherapy,three(42.86%)evolvedwithexigency for amputation, whereas among the cases that did not receivechemotherapy,two(33.33%)progressedwithexigency for amputation. Nostatistically significant correlation was observedbetweenneedforamputationandprior chemother-apy(p=0.587).
Similarly, no statistically significant correlation was observedbetweentheneedforamputationandtumor loca-tion(p=0.80).Inthepresentstudy,three(23.08%)tumorswere locatedinthepoplitealregion,two(15.38%)inthefemur,four (30.78%)inthetibia,one(7.69%)inthethigh,one(7.69%)in thearm,andtwo(15.38%)intheinguinalregion.Ofthefive amputations,two(40%)weretumorslocatedinthefemurand three(60%)tumorslocatedinthetibia.Table2summarizes theseresults.
Discussion
Vascularreconstructionassociatedwithresectionofsarcomas thataffectlargevesselsofalimbhasbeenshowntobeaviable methodforaffectedlimbpreservation.1,3–9,11,12
Table1–Epidemiologicaldata.
Name Age/gender Diagnosis Location RTX QTX
1 26/F Malignantfibroushistiocytoma Popliteal Postop No
2 38/M Fibrosarcoma Femur No No
3 27/M Ewing’ssarcoma(softtissue) Thigh Postop Yes
4 47/F Synovialsarcoma Inguinal Postop Yes
5 65/F Pleomorphicsarcoma Tibia Preop Yes
6 63/M Chondrosarcoma Proximalfemur No No
7 35/M Malignantfibroushistiocytoma Inguinal Postop No
8 12/M Osteosarcoma Tibia No Yes
9 24/M Hemangiopericytoma Popliteal No No
10 39/F Malignantfibroushistiocytoma Popliteal Postop No
11 14/M Osteosarcoma Proximaltibia No Yes
12 68/M Malignantfibroushistiocytoma Arm Postop Yes
13 16/M Osteosarcoma Tibia No Yes
Postop,postoperative;Preop,preoperative;QTX,chemotherapy;RTX,radiotherapy.
Table2–Dataanalysisresults.
Amputation Total p
No Yes
Gender
Male 4(44.44%) 5(55.56%) 9(100%) 0.098
Female 4(100%) 0(0%) 4(100%)
Diagnosis
Softtissue 7(100%) 0(0%) 7(100%) 0.005
Bone 1(16.66%) 5(83.34%) 6(100%)
Location
Popliteal 3(100%) 0(0%) 3(100%) 0.080
Femur 0(0%) 2(100%) 2(100%)
Tibia 1(25%) 3(75%) 4(100%)
Thigh 1(100%) 0(0%) 1(100%)
Arm 1(100%) 0(0%) 1(100%)
Inguinal 2(100%) 0(0%) 2(100%)
Reconstruction
Yes 7(100%) 0(0%) 7(100%) 0.005
No 1(16.67%) 5(83.33%) 6(100%)
Revascularization
Iliofemoral 2(66.67%) 1(33.33%) 3(100%) 0.843
Femoropopliteal 1(50%) 1(50%) 2(100%)
Poplitealtibial 4(57.14%) 3(42.86%) 7(100%)
Brachial 1(100%) 0(0%) 1(100%)
Infection
Yes 0(0%) 5(100%) 5(100%) 0.001
No 8(100%) 0(0%) 8(100%)
Chemotherapy
Yes 4(57.14%) 3(42.86%) 7(100%) 0.587
No 4(66.67%) 2(33.33%) 6(100%)
Patency
Yes 7(87.5%) 1(12.5%) 8(100%) 0.032
No 1(20%) 4(80%) 5(100%)
no vascular patency atthe postoperative revascularization site (p=0.032), and presentedinfection atthe surgical site (p=0.001).Noneofthesofttissuesarcomapatientsunderwent amputation;theonlypatientinthenon-amputatedbone sar-comagroupdidnotpresentinfectionandmaintainedvascular patencyinthegraft.
In their study, Emori et al.3 reported limb
Muramatsuetal.4reportedthatonlyonepatientrequired
amputationseven monthsaftersurgerydue toprogressive deteriorationwithischemiclimbpain;nonetheless,nopatient presentedvascular insufficiency inthe immediate postop-erative period. Furthermore, three cases of infection were identified;intwoofthem,asyntheticgrafthadbeenusedfor revascularization,whichledtheauthorstorecommendthe useofautologousveingraftasfirstchoice,inanattemptto reducetheriskofinfection.
Spark et al.6 reported a case of exigency for
amputa-tionten monthsaftersurgeryduetolocalocclusionofthe vascular graft,secondary to compression caused bytumor recurrence.Intheirstudy,theauthorsreportedtheuseofa distalfemoralprosthesisinonecaseandatotalfemoral pros-thesisinanothercase;intheformer,earlyreassessmentwas necessary,asthepatientevolvedwithtwoepisodesofgraft occlusioninthefirst24h(oneduetocompressionbetween theprosthesisandtheremnantsofmuscleandtheotherdue tothrombusformation).Inthatstudy,nocasesofprogression toamputationorinfectionwerereportedinpatientswithtotal anddistalfemoralprosthesis.
Nishinariet al.8 reportedthat, at18 months
postopera-tively, nine oftheir patients who had undergone resection with venous reconstruction in the lower limbswere alive; onepatientevolvedtoabove-the-kneeamputation,11months aftersurgery,due torelapse. Amongpostoperative compli-cations,thoseauthorsobservedonecaseofsurgicalwound infection,whichevolvedtovasculargraftruptureat21days aftersurgery,butdidnotrequireanamputation.
Adelanietal.9 assessedrevascularizationafterresection
ofsoft tissuesarcomas inthe lower limbs;onlyone of14 patientsunderwentamputationduetoanacutearterial occlu-sion.However,theauthorsreportedthepresenceofsurgical woundinfectioninfourcases(ofthese,twoofthemevolved withinfectionofthevasculargraft,bothmadefromsynthetic material)andthepresenceofthrombosisinfivecases.Two patientspresentedboththrombosisandinfection; nonethe-less,itwasnotpossibletoestimatethecause/effect relation-shipbetweenthetwo.Ithasbeen reportedthattheriskof infectionwithsyntheticvasculargraftsappearstobegreater. Nishinarietal.11evaluatedpatientswithmalignanttumors
involving large vessels of the lower limbs; only one case evolved with the exigency for amputation due to relapse. Nocasesofarterialreconstructionocclusionwereobserved. However,onecaseofruptureofanarterialreconstruction sec-ondary toinfection ina surgical woundwas reported; the graft wasligatedand satisfactorycollateral circulationwas observed.
Hohenbergeretal.12reportedacaseofamputationdueto
occlusionoftherevascularizationgraftonthe17th postopera-tiveday.Intheirstudy,aninfectionrateof21%wasobserved; inonecaseofinfection,occlusionofthesyntheticgraftthat replacedthefemoralveinwasreported.
Inturn,McKayetal.7reportedfourcasesofpatientswith
softtissue neoplasias inthe groinarea, who were submit-tedtoresectionandvascular reconstruction;theprocedure wassuccessfulinpreservingthelimbinallcases.No post-operativeamputationwasrequiredduringthatstudyandno arterialocclusionoranastomoticfailurewereobservedinthe reconstructions.
Intheassessedstudies,themainriskfactorsfor amputa-tionaftertumorresectionsurgeryandvascularreconstruction for limbpreservationappear tobelocal tumorrecurrence, occlusion,andlossofgraftpatency.
However, in the present study, it was observed that, in additiontolossofpatency,thereappearstobeastatistical significancebetweenlocalinfectionandamputation.Ofthe five casesthat evolved withexigencyfor amputation, four (80%)presentedinfectionandlossofpatency;onecase(20%) presentedinfectionwithpreservedpatency.Therefore,inthe presentstudy,infectionwasariskfactorfortheneedof ampu-tation. Inadequate vascularizationmayincrease theriskof infection;infectionmayalsocompromisegraftviability.
Anotherriskfactorobservedinthepresentstudywasthe presenceofbonesarcoma,necessitatinganunconventional osteoarticularprosthesistoreplacetheresectedbone.Ofthe sixcasestreatedwithprosthesis,onlyone(16.67%) didnot undergoamputation;thispatientpresentedvascularpatency anddidnotevolvewithinfection.Moreover,allcases requir-ing amputationhad incommonthe useofunconventional osteoarticularprosthesisduetoresectionofbonesarcomaand infection.Inthegroupofpatientswithsofttissuesarcoma, noneevolvedwithamputationorinfection;theonlycase with-out graftpatency didnotrequire amputation,astherewas satisfactorycollateralcirculation.
Lossofpatencyandinfectionareriskfactorsfor amputa-tion,aswellastumorrecurrence,thatwereobservedincases ofamputationreportedinotherstudies.3,6,8,11 Thefactthat
theuseofunconventionalosteoarticularprosthesisincaseof bonesarcomasappearstobeariskfactor,maybeassociated withprolongedsurgerytimeandthepresenceofmoreinert biomaterials,withthepossibilityofinfectionassociatedwith theimplant.
Conclusion
Inthepresentstudy,theriskofamputationwas38.46%. Theoccurrenceofinfectionappearstobeoneofthemain riskfactorforrevascularizationfailure,especiallyincasesof bonesarcomainwhichvascularreconstructionisperformed togetherwiththeuseofunconventionaljointprostheses.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.UmezawaH,SakurabaM,MiyamotoS,NagamatsuS,Kayano S,TajiM.Analysisofimmediatevascularreconstructionfor lower-limbsalvageinpatientswithlower-limbboneand soft-tissuesarcoma.JPlastReconstrAesthetSurg. 2013;66(5):608–16.
2.SawaizumiM,ImaiT,MatsumotoS.Recentadvancesin reconstructivesurgeryforboneandsofttissuesarcomas.IntJ ClinOncol.2013;18(4):566–73.
sarcomasintheinguinalregion:oncologicandfunctional outcomes.AnnVascSurg.2012;26(5):693–9.
4. MuramatsuK,IharaK,MiyoshiT,YoshidaK,TaguchiT. Clinicaloutcomeoflimb-salvagesurgeryafterwideresection ofsarcomaandfemoralvesselreconstruction.AnnVascSurg. 2011;25(8):1070–7.
5. KarakousisCP,KarmpaliotisC,DriscollDL.Majorvessel resectionduringlimb-preservingsurgeryforsofttissue sarcomas.WorldJSurg.1996;20(3):345–9.
6. SparkJI,CharalabidisP,LawsP,SebenR,ClayerM.Vascular reconstructioninlowerlimbmusculoskeletaltumours.ANZJ Surg.2009;79(9):619–23.
7. McKayA,MotamediM,TempleW,MackL,MooreR.Vascular reconstructionwiththesuperficialfemoralveinfollowing majoroncologicresection.JSurgOncol.2007;96(2):151–9. 8. NishinariK,WoloskerN,YazbekG,ZeratiAE,NishimotoIN.
Venousreconstructionsinlowerlimbsassociatedwith
resectionofmalignancies.JVascSurg.2006;44(5): 1046–50.
9.AdelaniMA,HoltGE,DittusRS,PassmanMA,SchwartzHS. Revascularizationaftersegmentalresectionoflower extremitysofttissuesarcomas.JSurgOncol. 2007;95(6):455–60.
10.FergusonPC.Surgicalconsiderationsformanagementof distalextremitysofttissuesarcomas.CurrOpinOncol. 2005;17(4):366–9.
11.NishinariK,WoloskerN,YazbekG,ZeratiAE,NishimotoIN, PennaV,etal.Vascularreconstructioninlimbswith malignanttumors.VascEndovascSurg.2004;38(5): 423–9.