Case Report
Relato de Caso
CoDAS 2013;25(3):297-300 Nair Kátia Nemr1
Marcia Simões-Zenari1 Tainá Soares Ferreira1 Heloisa Regina Fernandes1 Letícia Lessa Mansur1
Descritores
Miastenia gravis Disfonia Voz Qualidade de vida Diagnóstico
Keywords
Keywords Myasthenia gravis Dysphonia Voice Quality of life Diagnosis
Correspondence address:
Marcia Simões-Zenari
Curso de Fonoaudiologia, Faculdade de Medicina, Universidade de São Paulo R. Cipotânea, 51, Cidade Universitária, São Paulo (SP), Brasil, CEP: 05360-160. E-mail: [email protected]
Received: 12/21/2011
Accepted: 02/19/2013
Study carried out at the Laboratory of Speech-Language Pathology Investigation in Voice, Department of Physiotherapy, Speech-Language Pathology and Audiology and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
(1) Department of Physiotherapy, Speech-Language Pathology and Audiology and Occupational Therapy, School of Medicine, Universidade de São Paulo – USP – São Paulo (SP), Brazil.
Conlict of interest:nothing to declare.
Dysphonia as the primary complaint in a case of
myasthenia gravis: diagnosis and speech therapy
Disfonia como principal queixa num quadro de miastenia
grave: diagnóstico e fonoterapia
ABSTRACT
Myasthenia gravis is an autoimmune disease, manifested by progressive muscular weakness and fatigue. There are frequent ocular and bulbar symptoms, among them, dysphonia. This article reports a case of dysphonia that contributed to the diagnosis of myasthenia gravis through a speech evaluation. The patient sought speech therapy with the ENT diagnosis of presbyphonia. The perceptual voice assessment and acoustic analysis pointed out respiration, glottal voice source and resonance affections. Considering that some of the data obtained from anamnesis and vocal assessments were not directly related to presbyphonia, the speech therapist discussed the case with the physician and they both concluded it was necessary to refer the patient to a neurological evaluation. The neurologist then raised the diagnostic hypotheses of myasthenia gravis and requested further examinations. The patient underwent speech therapy and drug treatment. A vocal reassessment, which occurred two months after the initial treatment, showed improvement in voice quality, with great impact on quality of life. This article shows the importance of detailed clinical speech evaluation and participation of a speech therapist in an interdisciplinary team.
RESUMO
298 Nemr NK, Simões-Zenari M, Ferreira TS, Fernandes HR, Mansur LL
CoDAS 2013;25(3):297-300 INTRODUCTION
Myasthenia gravis is an autoimmune disease caused by a decrease of acetylcholine receptor and loss of postsynaptic re-ceptors(1,2). It is manifested by progressive weakness and fatigue
of skeletal muscles(3) and affects between 5 and 15 individuals
per 100,000, mostly being 30% elderly(2). The prevalence is
higher in women, with a ratio of approximately 2:1(4,5). There
are few clinical and epidemiological data on the occurrence of this disease in Brazil(5).
Myasthenia gravis can affect one or more muscle groups, and the involvement of the levator of upper eye-lid and extraocular muscles is quite common; therefore, symptoms such as ptosis and diplopia may be frequent(3,6).
Bulbar symptoms such as dysphonia, dysphagia, weak mastication, dysarthria, and weakness in facial muscles(1)
are also common, especially when the disease is manifested after the age of 65(2).
The dificulties with speech and swallowing appear as initial symptoms in more than 27% of cases(4). A study of 40 patients
with myasthenia gravis found dysphonia as the irst symptom in 6% of patients and dysphonia appeared with the progression of the disease in 60% of cases(3). The vocal affections
com-monly found in these patients are hypernasality, dificulty in sustaining pitch, vocal fatigue, intermittent aphonia, stridor, roughness, glottal incompetence, and changes in vocal qual-ity(2,3,6). Articulatory imprecision and verbal luency alterations
can also be observed together with dysphonia(2).
In a recent Brazilian study(5), dificulties in swallowing
were observed and voice disorders were more common in the age group between 12 and 50 years; in the group of individu-als with more than 50 years, the presence of dysphonia was as frequent as diplopia.
The diagnosis of myasthenia gravis is determined from the clinical signs and can be conirmed by electromyography in 95% of cases(3). The report of the patient is considered essential
for the diagnosis. Dysphonia is often not associated with the disease during the ear, nose, and throat (ENT) diagnosis(6).
If untreated, myasthenia gravis can impair the individual due to the damage that can occur in motor endings(7). The
treat-ment is usually done through medications(3) or, in some cases,
through surgery with signiicant improvement in symptoms(6)
and even complete remission in a few patients(7). Few data are
available regarding the referral to associated treatments such as physiotherapy and speech therapy. In a literature review, physiotherapy proved to be indispensable(7) with improvement
in motor performance, fatigue reduction, and prevention of generalized respiratory complications. Speech therapy is in-dicated due to swallowing/mastication alterations, dysphonia, and speech dificulties, the improvement of which contributes to raising the quality of life of patients(8,9).
The purpose of this paper was to report a case and discuss the treatment results of an elderly individual whose speech evaluation was critical to the referral for neurological assess-ment and, thereafter, to establish the diagnosis of myasthenia gravis and appropriate conducts.
CLINICAL CASE
This study was approved by the Ethics Committee of the institution (236/10). The patient agreed with the realization and dissemination of this research and its results and signed the consent form.
The 84-year-old patient was referred by an ENT doctor for clinical assessment because the diagnosis was not possible via laryngoscopy.
During anamnesis held in our school clinic, the patient mentioned that her voice felt “horrible and nasty” and that she could not speak loudly and had dificulty being understood by others. The main vocal aspects indicated by the patient were vocal fatigue, hoarseness, voice failure, vocal tremor, and the need to make an effort to speak. She also complained of con-stant coughing and gagging. The patient reported daily use of medications prescribed by the physician due to hypothyroidism, gastroesophageal relux episodes, diabetes, hypertension, and peripheral vestibular dysfunction.
Upon completion of anamnesis, perceptual voice assess-ment and acoustic analysis, qualitative analysis of the spectrum, quality of life related to voice, orofacial motricity, speech, and oral functions of mastication and swallowing were carried out. Alterations on the three vocal production systems were observed: breathing, glottal source, and ilter — resonance and articulation of speech sounds. During the assessment tasks, the patient had great dificulty coordinating breathing and speech, her pitch was lower, she presented aspirated vo-cal attack and loudness, and her fundamental frequency (f0) were decreased. The vocal range was reduced, as well as the maximum phonation duration and vocal resistance. With the implementation of the CAPE-V protocol(10,11), dysphonia was
considered moderate and intense, with asthenia and roughness as the most affected aspects, followed by instability and breathi-ness. The patient presented gagging and vocal fatigue with rapid vocal deterioration in spontaneous speech leading to aphonia. Important articulatory imprecision was observed mainly in isolated phonemes, and dificulty coordinating speech organs and sustaining fricatives were observed. The mean fundamental frequency was 107.52 Hz (Table 1).
The acoustic spectrographic analysis was performed us-ing the Spectrogram software and the fundamental frequency was measured with the Praat software. The tracing showed partially visible harmonics, presence of noise between har-monics, substitution of harmonics by noise, interruptions, bifurcations, graphical irregularity, and reduced series of harmonics (Figure 1).
It was observed that vocal alterations produced signiicant negative impact on the quality of life of the patient, limiting her participation in social and family events. Her score on the Vocal Health Quality questionnaire (VHQ)(12) was 25 on a scale of 0
to 100, where the maximum value represents better quality of life related to voice.
299
Speech therapy for dysphonia
CoDAS 2013;25(3):297-300
presbyphonia. However, as speech assessment had raised issues that were not compatible only with this diagnosis — such as important vocal fatigue, dysarthria, and dysphagia — the mul-tidisciplinary team discussed the case and decided to refer the patient for neurological evaluation at the same hospital. The neurologist who evaluated the patient considered the clinical signs suficiently suggestive for the diagnosis hypothesis of myasthenia gravis and, therefore, initiated drug treatment in parallel to further examination. Such diagnosis was subse-quently conirmed.
The patient underwent weekly speech therapy pro-gram with an emphasis on techniques for glottal closure, articulation of speech sounds, and improvement of vocal intensity and resistance. To prevent the patient to have vocal fatigue, the selected exercises were distributed at each session so that they would interim glottal source tech-niques with others that would not involve vocal production, such as respiration and articulation of voiceless sounds. Exercises were interrupted at the slightest sign of loss of
vocal quality/vocal fatigue. The glottal source exercises were not suitable for domestic practice at the beginning of treatment. As vocal fatigue was one of the symptoms that rapidly improved due to the medication, this control gradually became less necessary.
After 2 months of speech therapy and drug use, a new clinical evaluation of voice and speech was carried out when the improvement on the initially identiied affections became apparent. Roughness passed to moderate and asthenia and instability passed to mild and moderate, respectively. Only the presence of breathiness became more apparent, which is com-patible with increased vocal intensity presented by the patient in the presence of incomplete glottal closure. Furthermore, maximum phonation time and vocal resistance improved and vocal fatigue decreased; also, the fundamental frequency was higher (Table 1).
In the spectrogram, the bifurcations and interruptions ini-tially observed were no longer present, and better deinition and greater regularity of harmonics were also observed. Only the
Figure 1. Illustrative spectrogram image of the pretreatment emission of vowel /a/, Spectrogram software
Signal
5 kHz
4 kHz
3 kHz
2 kHz
1 kHz
4 sec 6 sec 8 sec 10 sec 12 sec 7 sec 8 sec 9 sec 10 sec 11 sec 12 sec Signal
5 kHz
4 kHz
3 kHz
2 kHz
1 kHz
Figure 2. Illustrative spectrogram image of the posttreatment emission of vowel / a/, Spectrogram software
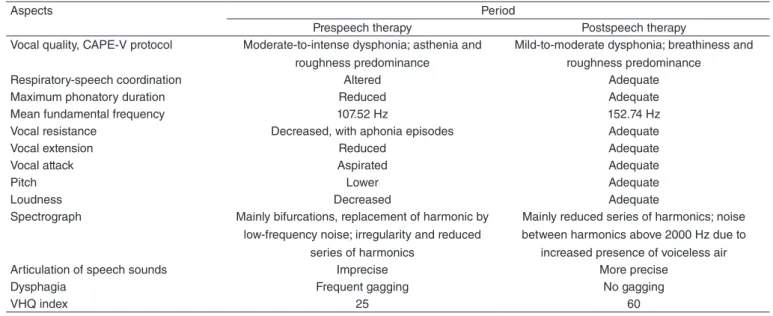
Table 1. Speech assessment aspects pre- and postspeech therapy
Aspects Period
Prespeech therapy Postspeech therapy Vocal quality, CAPE-V protocol Moderate-to-intense dysphonia; asthenia and
roughness predominance
Mild-to-moderate dysphonia; breathiness and roughness predominance
Respiratory-speech coordination Altered Adequate
Maximum phonatory duration Reduced Adequate
Mean fundamental frequency 107.52 Hz 152.74 Hz
Vocal resistance Decreased, with aphonia episodes Adequate
Vocal extension Reduced Adequate
Vocal attack Aspirated Adequate
Pitch Lower Adequate
Loudness Decreased Adequate
Spectrograph Mainly bifurcations, replacement of harmonic by low-frequency noise; irregularity and reduced
series of harmonics
Mainly reduced series of harmonics; noise between harmonics above 2000 Hz due to
increased presence of voiceless air Articulation of speech sounds Imprecise More precise
Dysphagia Frequent gagging No gagging
VHQ index 25 60
300 Nemr NK, Simões-Zenari M, Ferreira TS, Fernandes HR, Mansur LL
CoDAS 2013;25(3):297-300
presence of noise between the harmonics and replacement of harmonics by noise at frequencies above 2,000 Hz increased, which is consistent with the increased presence of breathiness previously reported (Figure 2).
However, the most signiicant improvement was regarding quality of life related to voice, expressed through the reports of the patient and also through the VHQ index, which increased from 25 to 60.
It is important to indicate that, during speech therapy, audi-tory evaluation was performed and the patient was diagnosed with presbycusis. This fact may explain her dificulty in per-ceiving some aspects of vocal production.
DISCUSSION
The presentation of this case evidences how speech assess-ment was important for the multidisciplinary team to correctly diagnose and quickly start treatment, which would not be pos-sible with the ENT diagnosis alone.
Vocal aspects resulting from myasthenia gravis are related to fatigue and weakness of adductor muscles and tension of the vocal folds. Dysphagia may be associated with disorders of pharynx and esophagus muscles, and dysarthria and articulatory imprecision can be justiied by the weakness of the muscles of the tongue and palate(2,3). Valuing both clinical aspects and
patient report was critical to deine the appropriate treatment for this case. Speech therapy combined with drug treatment enabled many affected aspects to quickly improve.
There was a significant gain in the quality of life of the patient, which was very meaningful to her because gains in intelligibility and motivation for social interactions were possible.
The data found in the initial analysis of the spectrogram are consistent with the literature on dysarthria: spectrogram instability with no harmonics at high frequencies due to weakness and slowness or lack of coordination of laryngeal muscles as well as uneven distribution of energy along the vocal tract(13).
Early diagnosis and early agile multidisciplinary treatment enable improvement of signs and symptoms of myasthenia gravis and, in many cases, even total remission. For patients who present dysphagia associated with this disease, these factors are essential to prevent aspiration, dehydration, and malnutrition(14).
In this case, drug treatment led to the rapid decrease of vocal symptoms and fatigue during speech and provided full participation of the patient in therapy. Furthermore, vocal fatigue was considered in treatment planning, especially with regard to the distribution of exercises during the session and therapeutic attention for the least sign of its presence.
The results exceeded the expectations of the patient and professionals involved, mainly because of the presence of other associated diseases such as gastroesophageal relux, presbycusis, and hypothyroidism, the latter being very com-mon in cases of myasthenia gravis(15). Practitioners should give
special attention to the described aspects in the analysis for differential diagnosis.
FINAL COMMENTS
This case study reiterates the importance of clinical as-sessment for the diagnosis of patients with voice and speech alterations. The combination of laryngoscopy, clinical signs, aspects reported by the patient, and interdisciplinary dialogue allowed the complete understanding of the framework and helped deine the diagnosis with appropriate referral and deter-mination of appropriate care. The results obtained in relation to both medical treatment and speech therapy were highly positive and reinforced the relevance of the latter not only to prevent complications but to provide better quality of life.
* NKN and LLM were in charge of the project and study design, as well as the general orientation as to the stages of execution and elaboration of the manuscript; MSZ supervised data collection and collaborated with data analysis and with the writing of the manuscript; TSF and HRF were responsible for data collection and formatting.
REFERENCES
1. Kanemaru SI, Fukushima H, Kojima H, Kaneko KI, Yamashita M, Ito J. A case report of myasthenia gravis localized to the larynx. Auris Nasus Larynx. 2007;34(3):401-3.
2. Montero-Odasso M. Dysphonia as irst symptom of late-onset myasthenia gravis. J General Internal Medicine. 2006;21(6):C4-C6.
3. Mao VH, Abaza, M, Spiegel JR, Mandel S, Hawshaw M, Heuer RJ, et al. Laryngeal myasthenia gravis: report of 40 cases. J Voice. 2001;15(1):122-30.
4. Jacobson DL, Gange SJ, Rose NR, Graham NM. Epidemiology and estimated population burden of selected autoimmune diseases in the United States. Clin Immunol Immunopathol. 1997;84(3):223-43. 5. Aguiar AAX, Carvalho AF, Costa CMC, Fernandes JMA, D’Almeida
JAC, Furtado LETA, et al. Myasthenia gravis in Ceará, Brazil. Arq Neuropsiquiatr. 2010;68(6):843-8.
6. Liu WB, Xia Q, Men LN, Wu ZK, Huang RX. Dysphonia as a primary manifestation in myasthenia gravis (MG): a retrospective review of 7 cases among 1520 MG patients. J Neurol Sci. 2007;260(1-2):16-22. 7. Santos FRM, Tiago APPP, Fonseca AL, Christofoletti G. Revisão da
isioterapia na miastenia grave. Revista Movimenta 2008;1(1):16-22. 8. Penatti CT, Silva IA, Domenis DR, Okubo PCMI. Atuação
fonoaudiológica na miastenia grave auto-imune adquirida: descrição de um caso. Rev Soc Bras Fonoaudiol. 2008;(Suppl):217.
9. Bassi AKZ, Melo TT, Pedraça LS, Cortêz ASS, Silva VB, Rodrigues LB, et al. Características fonoaudiológicas e audiológicas de uma paciente com miastenia grave: relato de caso. Rev Soc Bras Fonoaudiol. 2009;(Suppl):1929. 10. Kempster GB, Gerratt BR, Verdolini Abbott K, Barkmeier-Kraemer
J, Hillman RE. Consensus Auditory-Perceptual Evaluation of Voice: development of a standardized clinical protocol. Am J Speech Lang Pathol. 2009;18(2):124-32.
11. Behlau M. Consensus Auditory – Perceptual Evaluation of Voice (CAPE-V). ASHA 2003 [Refletindo sobre o novo]. Rev Soc Bras Fonoaudiol. 2004;9(3):187-9.
12. Gasparini G, Behlau M. Quality of Life: Validation of the Brazilian Version of the Voice-Related Quality of Life (V-RQOL) Measure. J Voice. 2009;23(1):76-81.
13. Ortiz KZ, Carrillo L. Comparação entre as análises auditiva e acústica nas disartrias. Rev Soc Bras Fonoaudiol. 2008;13(4):325-31.
14. Oda AL, Chiappetta ALML, Annes M, Marchesan IQ, Oliveira ASB. Avaliação clínica, endoscópica e manométrica da deglutição em pacientes com miastenia grave autoimune adquirida. Arq Neuropsiquiatr. 2002;60(4):986-95. 15. Bichuetti DB, Barros TM, Oliveira EML, Annes M, Gabbai AA.