Universidade de Lisboa
Faculdade de Motricidade Humana
Effects of roller massager on muscle performance, morphology,
and oxygenation after exercise-induced muscle damage
Dissertação elaborada com vista à obtenção do Grau de Mestre em Exercício e Saúde
Orientador
Pedro Pezarat Correia
Co-orientador
Sandro Remo Martins Neves Ramos Freitas
Presidente
Doutor Augusto Gil Brites de Andrade Pascoal
Professor Auxiliar da Faculdade de Motricidade Humana da Universidade de Lisboa
Vogais
Doutor Sandro Remo Martins Neves Ramos Freitas
Professor Auxiliar da Faculdade de Motricidade Humana da Universidade de Lisboa
Doutor Duane Calvin Button
Assistant Professor da Memorial University of Newfoundland, Canada.
Nuno Filipe Casanova Martins
iii
Dedicatória
A vocês…
A vocês que me amam
A vocês que me apoiam
A vocês que me lançam ao desconhecido
A vocês que lançam ao desafio
A vocês que me tornam melhor
A vocês…
v
Agradecimentos
“Gratitude is not only the greatest of virtues, but the parent of all the others.” Marcus Tullius Cicero
Após um percurso de ano e meio, um capítulo brevemente se encerra. Um longo caminho de desafios e experiências. Desesperos e vitórias. Desilusões e conquistas. Sorrisos e lágrimas. Dezenas de páginas escritas, centenas de artigos revistos, e uma dificuldade astronómica em colocar por palavras o que se viveu durante meses.
Em primeiro lugar, quero agradecer à Faculdade de Motricidade Humana da Universidade de Lisboa, assim como aos laboratórios de fisiologia e bioquímica do exercício e de comportamento motor, que permitiram o desenvolvimento de todo este trabalho, providenciando-me todas as condições necessárias para que este florescesse naturalmente.
Pedro Pezarat Correia, o meu orientador, que prontamente aceitou o meu desafio de avançar para uma temática pouco desenvolvida, afastando-me milhas e quilómetros da minha zona de conforto, e resolveu qualquer problema logístico que tentasse sabotar o desenvolvimento de ciência.
Sandro Freitas, um mestre, um mentor, uma inspiração. Ao início foi uma relação que custou a arrancar. Sentia-me desamparado, desiludido, perdido. Decidi responder à sua ausência com o dobro da dedicação e procurar as respostas por mim próprio. A quantidade de trabalhos solicitados era inversamente proporcional ao número de congratulações. O desespero acompanhava de forma exponencial.
“Eu sempre disse que o Nuno está aqui desde o início a trabalhar para uma liga dos campeões e não para uma segunda divisão, e o trabalho que ele demonstra diariamente
vai se refletir no seu sucesso”.
A maré mudou. Como que se a Lua se lançasse fora de órbita. O que parecia uma relação de patrão-empregado, provavelmente por uma visão infantil da minha pessoa, tornou-se uma relação de companheiros, de colegas, de amigos. O apoio que eu sentia não ter, dispara para níveis inalcançáveis por qualquer escala. Horas a trabalhar, lado a lado, a colocar e resolver problemas, a rir, a tornarmo-nos músicos internacionais
vi
e até estrategas de marketing com aspirações de destronar empresas de rolos de cozinha multibilionários. A lista de bons momentos daria uma tese de doutoramento e como tal, os agradecimentos a este senhor nunca serão os suficientes.
To my dear foreign friends. Devin Philpott for such great moments and for bringing me the equipment that allowed me to complete my scientific journey. Duane Button, for all the patience during this process, helping with the paper, giving me life advices, and for making me laugh by asking the origins of my name Casanova. Jérôme Pasquette, the wind-surf man, for working patiently with me on my methodology, making sure that everything was working properly, especially my brain, by making me laugh every time when asking subjects to do a maximal voluntary contraction. “Allez allez”! Lastly but not least, Kieran Crook, my long distance longtime friend and brother, an inspiration and a true warrior, for all the support during the process, encouraging me when I was feeling down and in the end, helping with text revision, making sure that every single word was correct.
Querida Ritinha Machado, nem há palavras para descrever o apoio. Incansável do início ao fim. A aparecer com o pé torcido, sem aulas, apenas para me ajudar uns minutos. Pelos cafés que me pagaste. Pelas formações contínuas de excell. Por abrires e fechares o laboratório comigo ao longo de semanas. Pelo apoio durante todas as fases nestes duros meses. Dream Team!
Ana Lourenço, “nuty”, a minha parceira de desabafos, sempre na presença de um gelado, hambúrgueres do mês, ou uma bela poncha. Obrigado por todo o apoio. Obrigado pelos empurrões e por me levantares a cabeça sempre que me apetecia afundar. Obrigado não só nestes meses mas em todos estes anos que nos conhecemos. És sem dúvida uma pessoa especial e que terá sempre reservado para si um espaço muito cuidado no meu coração.
Os meus tropas, Ângelo Luís o cantor, José Dutschke a companhia de sauna. Um especial obrigado a estes senhores que me apoiam incondicionalmente, qualquer que seja a minha decisão, estando sempre disponíveis para me ouvir e me dar na cabeça quando necessário. Sem o apoio deles, muita coisa na minha vida estaria diferente neste momento.
Todos os colegas e amigos que passaram diariamente pelo laboratório e viveram cada momento comigo com destaque para algumas menções honrosas. Joana Reis, a mestre da mitocôndria, a mestre do NIRS, a mestre em cruxificar-me por ter deixado as coisas desarrumadas, a mestre da desilusão por não colocar sequer uma das suas cobaias
vii
a vomitar. João Vaz, o mestre do EMG, o mestre do MatLab, o traficante inigualável de elétrodos. Maria João Valamatos, a mestrinha do meu mestre, por socorrer em casos de SOS sempre que necessário, a resolver em tempo recorde qualquer problema técnico.
Team Casanova, a minha família especial que contacta diariamente comigo e me dá uma vontade enorme de viver e lutar pela minha paixão. Um carinho especial para algumas pessoas maravilhosas. O meu irmão das ilhas, Marco Silva, e toda a sua família, que sempre me apoiou nestes 2 anos de relação fazendo-me sentir como um autêntico açoriano de gema, como se o sangue que nos corre nas veias fosse o mesmo. As minhas meninas que estão sempre no meu coração, as minhas tropas e parceiras de guerra, a darem-me forças diariamente para continuar a lutar por mim, mesmo quando a luz ao fundo do túnel não passava de escuridão, Luísa Fonseca, Catarina Branco e Bárbara Alemão, que acabou por partilhar sem qualquer hesitação os seus gémeos com a ciência, embora o arrependimento fosse claro.
Aos meus boys, Rapazes do Sporting Clube de Portugal, por todo o apoio e gargalhadas nos treinos após dias desesperantes fechado num laboratório, a receberem-me com um grande abraço e a participarem ativareceberem-mente durante todo o processo. VA.
Os meus queridos amigos e cobaias que se prestaram de forma (in) voluntária a participarem neste estudo. Sem eles, a teoria nunca teria saído do papel. Um carinho especial a todos os que coxearam durante uns dias, pela ciência e por mim.
Por último, e os mais importantes durante todo o processo, família. Mãe, pai, mana. Uma presença diária e constante. Ouviram os meus desesperos. Ouviram as minhas tristezas. Ouviram as minhas conquistas e descobertas. Ouviram as minhas gargalhadas e limparam as minhas lágrimas. Permitiram que todos os caminhos na minha vida culminassem neste ponto, a concluir mais uma etapa da minha jornada académica. Por vezes não me expresso o suficiente. Por vezes não me expresso de todo. Mas eles sabem. Eles sabem que o amor e carinho que sinto por eles são incalculáveis. Se existem pessoas que posso realmente confiar a minha vida, são eles. Sempre foram. Como em qualquer relação, bons e maus momentos existem, mas o amor que nos une é inabalável. Gostava de ter palavras para descrever o impacto que estas pessoas tiveram na minha vida mas qualquer tentativa nunca faria justiça. Qualquer tentativa não passaria de uma simples amostra. Uma gota de água num oceano de paixão que me rodeou desde nascido.
ix
Effects of roller massager on muscle performance,
morphology, and oxygenation after exercise-induced
muscle damage
Efeitos do roller massager no desempenho, morfologia,
e oxigenação muscular após dano muscular induzido
xi
Abstract
This study determined roller massager (RM) effectiveness on ankle plantar flexors’ recovery after exercise-induced muscle damage (EIMD) stimulus. Two experiments were conducted. The first experiment (n=10) examined functional [i.e., ankle plantar flexion maximal voluntary isometric contraction (MVIC) and submaximal (30% of MVIC) sustained force; ankle dorsiflexion maximal range of motion and resistance to stretch; and pain pressure threshold] and morphological [medial gastrocnemius (MG) cross sectional area, thickness, fascicle length, and fascicle angle] variables, before and immediately, 1h, 24h, 48h, and 72 after EIMD. In the second experiment (n=10), changes in MG deoxyhemoglobin concentration kinetics (velocity and amplitude) during a submaximal sustained force test were observed before and 48h after EIMD. Participants performed both experiments twice, with and without (NRM) the application of a RM (6 × 45 seconds with 20 seconds rest between sets). RM intervention did not alter plantar flexors’ strength and flexibility impairment after EIMD, as well the MG morphology and oxygenation kinetics (p>0.05). On the other hand, a strong tendency for an acute (within 1 hour) change of ipsilateral (post-effects: RM=+19%, NRM=-5%, p=0.032) and contralateral (p=0.095) MG pain pressure threshold was observed. In conclusion, the present results suggest that a roller massager has no effect on muscular performance, morphology, and oxygenation recovery after EIMD, except for muscle pain pressure threshold (i.e., a soreness). Thus, RM may have potential application in recovery for people with increased muscle soreness, if performed immediately before a physical task.
Key-words: Exercise induced muscle damage, roller massager, recovery, performance,
xiii
Sumário
Este estudo avaliou a eficácia do roller massager (RM) na recuperação dos flexores plantares após dano muscular induzido pelo exercício (DMIE). Duas experiências foram conduzidas. A primeira (n=10) examinou variáveis funcionais [i.e., contração voluntária isométrica máxima dos flexores plantares (CVIM) e contração submáxima (30% da CVIM) contínua; amplitude articular máxima do tornozelo em dorsiflexão e resistência ao alongamento; e limiar da dor sob pressão] e morfológicas [área de secção transversa do gémeo medial (GM), espessura, comprimento e ângulo dos fascículos], antes e imediatamente, 1h, 24h, 48h e 72h após DMIE. Na segunda experiência (n=10), alterações na concentração de hemoglobina desoxigenada (velocidade e amplitude) do GM durante o teste de contração submáxima contínua foram observadas antes e 48h após DMIE. Os participantes realizaram ambas as experiências por duas vezes, com e sem (NRM) a aplicação do RM (6 x 45 segundos com 20 segundos entre séries). A intervenção com RM não alterou os danos na força e flexibilidade dos flexores plantares provocados pelo DMIE, nem a morfologia e cinética de oxigénio do GM (p>0.05). Por outro lado, foi observada uma forte tendência para uma alteração aguda no limiar da dor sob pressão (durante 1 hora) no GM ipsilateral (efeitos imediatamente após: RM=+19%, NRM=-5%, p=0.032) e contralateral (p=0.095). Concluindo, estes resultados sugerem que o roller massager não induz efeitos na recuperação do desempenho muscular, morfologia, e oxigenação após DMIE, com excepção do limiar da dor sob pressão (i.e., dor). Assim, a utilização do RM pode ter potencial em pessoas com dores musculares, se aplicado imediatamente antes da atividade.
Palavras-chave: Dano muscular induzido exercício, roller massager, recuperação,
1
INDEX OF CONTENTS
List of figures ... 3
List of acronyms ... 5
Introduction ... 7
Objectives and hypothesis ... 11
Review of literature ... 13
1 - Exercise induced muscle damage ... 13
1.1 Stimulus characterization ... 13
1.2 Signs and symptoms responses ... 14
1.2.1 Muscle function ... 14
1.2.1.1 Maximal voluntary isometric contraction ... 14
1.2.1.2 Rate of force development ... 15
1.2.1.3 Maximal range of motion... 16
1.2.2 Perception of pain and soreness... 16
1.2.3 Muscle morphology ... 17
1.2.4 Local muscle deoxygenation kinetics ... 17
1.2.5 Intramuscular blood proteins ... 18
1.3 Prevention methods ... 19
1.3.1 Stretching ... 19
1.3.2 Cryotherapy ... 19
1.3.3 Exercise ... 20
1.3.4 Repeated bout effect ... 21
1.3.5 Massage ... 21
2 - Foam roller and roller massager ... 22
2.1 Definitions and types ... 22
2.2 Variables... 23 2.2.1 Intensity ... 23 2.2.2 Duration ... 23 2.2.3 Density ... 24 2.3 Effects... 24 2.3.1 Range of motion ... 24 2.3.1.1 Foam roller ... 24 2.3.1.2 Roller massager ... 27
2
2.3.2 Recovery ... 30
2.3.3 Pain pressure threshold ... 31
2.3.3 Warm-up ... 31 2.3.4 Crossover effects ... 32 2.3.5 Muscle activation ... 33 2.3.6 Arterial function ... 34 Methods ... 35 Participants ... 35
Experimental design and procedures ... 35
Equipment and variables ... 38
Dynamometry ... 38
Algometry... 39
Ultrasonography ... 39
Near-infrared reflectance spectroscopy ... 40
Electromyography ... 40
Data processing ... 41
Statistics ... 43
Reliability and sample size ... 43
Results ... 45 Experiment 1 ... 45 Experiment 2 ... 49 Discussion ... 51 Conclusions ... 55 References ... 57
3
List of figures
Figure 1. Study design.
Legend: CSA – Cross-sectional area; EIMD – Exercise-induced muscle damage; MVIC – Maximal voluntary isometric contraction; NIRS – Near infrared reflectance
spectroscopy; NRM – No-roller massager; PPT – Pain pressure threshold; RM – Roller massager; ROM – Range of motion; SSF – Submaximal sustained force………..36
Figure 2. Roller massager intervention setup. ... 38
Figure 3. (A) Maximal isometric voluntary force, (B) submaximal (30%) sustained
force, (C) maximal ankle dorsiflexion range of motion, and (D) plantar flexors
resistance to stretch responses after exercise-induced muscle damage stimulus in both roller massager (RM) and no-roller massager (NRM) conditions. Values are normalized to baseline values.
* – Statistically different from baseline (p<0.05). ... 46
Figure 4. (A) Cross-sectional area, (B) muscle thickness, (C) fascicle angle and (D)
fascicle length of the medial gastrocnemius after exercise-induced muscle damage stimulus in both roller massager (RM) and no-roller massager (NRM) conditions (n=9). Values are normalized to baseline values.
* – Statistically different from baseline (p<0.05).
# – Statistically different between groups (p<0.05). ... 47
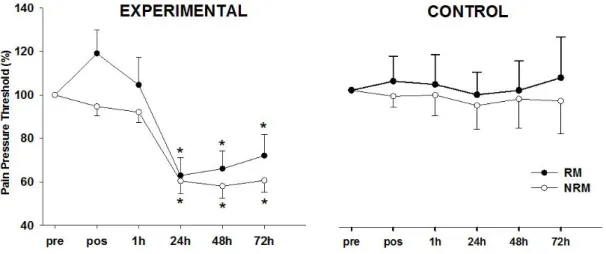
Figure 5. Pain pressure threshold of the medial gastrocnemius in the experimental and
control limbs after exercise-induced muscle damage stimulus in both roller massager (RM) and no-roller massager (NRM) conditions. Values are normalized to baseline values.
* – Statistically different from baseline (p<0.05). ... 48
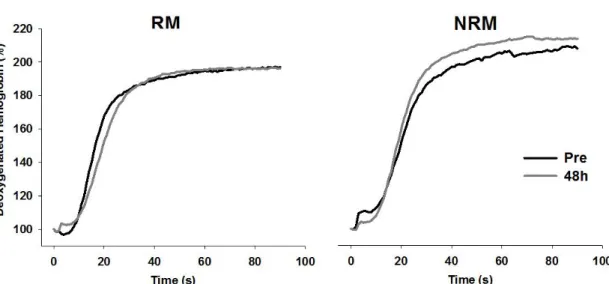
Figure 6. Deoxygenated hemoglobin response during the submaximal sustained force
test after exercise-induced muscle damage stimulus in both roller massager (RM) and no-roller massager (NRM) conditions. Values are normalized to baseline values. ... 49
5
List of acronyms
A1 – Amplitude SS – Static stretching
CK – Creatine kinase SSF – Submaximal sustained force
CRPNF - Contract-relax proprioceptive 𝝉 – Time constant
neuromuscular facilitation 𝝉’ – Effective time constant
CSA – Cross-sectional area TA – Tibialis anterior DOMS – Delayed-onset muscle soreness TD – Time delay EIMD – Exercise-induced muscle damage VL – Vastus Lateralis EMG – Electromyography
FA – Fascicle angle FL – Fascicle length FR – Foam roller
HHb – Deoxyhemoglobin
ICC – Intraclass correlation coefficient LG – Lateral gastrocnemius
Mb – Myoglobin
MDC – Minimal detectable change MG – Medial gastrocnemius MT – Muscle thickness
MVIC – Maximal voluntary isometric contraction NIRS – Near-infrared reflectance spectroscopy NRM – No-roller massager
PPT – Pain pressure threshold r – Pearson correlation coefficient RBE – Repeated bout effect RFD – Rate of force development RM – Roller massager
ROM – Range of motion SD – Standard deviation
SEM – Standard error of measurement SMT – Self-manual therapy
7
Introduction
The speed of physical recovery after exercise-induced muscle damage (EIMD) is a crucial aspect for physical performance optimization and training methodology (Howatson, Glyn, & van Someren, 2008). It has been reported that EIMD decreases muscle maximal force production, muscle rate of force development (RFD) (Clarkson et al., 2002), ability to sustain submaximal isometric contractions (Ye et al., 2015), and joint maximal range of motion (ROM) (Matsuo et al., 2014). In addition, among other physiological effects, it is reported that EIMD increases muscle tenderness and swelling (Cleak & Eston, 1992), joint resistance to stretch (i.e., due to tissues passive tension increase) (Whitehead, Weerakkody, Gregory, Morgan, & Proske, 2001), edema (Nosaka & Clarkson, 1996a) (Lacourpaille et al., 2014), blood creatine kinase (CK) (Nosaka & Clarkson, 1996b) and blood myoglobin (Mb) (Davies et al., 2008). These effects peak at 24-72 hours following EIMD (Cheung, Hume, & Maxwell, 2003), and are thought to be restored to baseline at a faster rate by different physical approaches like massage, cryotherapy, static stretching (SS), and low-intensity exercise (Torres et al., 2012). However, a recent systematic review has reported a lack of effectiveness for most of these methods, whereas massage proved to be slightly effective in the relief of EIMD symptoms (Torres et al., 2012).
Foam rolling has been recently proposed as a recovery strategy to reduce EIMD symptoms by using a foam roller (FR) or a roller massager (RM) (Cheatham et al., 2015; Schroeder and Best, 2015). It consists in a mechanical technique that mimics manual massage by using a dense FR to apply pressure on soft tissues. It has been demonstrated that RM does attenuate decrements in lower extremity muscle performance by improving both static-passive and static-dynamic hip flexion ROM, muscle activation, vertical jump height, and reducing perceived pain in the subsequent days after EIMD (MacDonald, Button, Drinkwater, & Behm, 2014; Pearcey et al., 2015; Jay et al., 2014). However, the underlying physiological mechanisms of the RM effects in reducing motor functional impairment after EIMD are still unclear.
It has been suggested that the RM prophylactic effect after EIMD is due to a blood flow increase in the damaged tissue, and thus enhancing blood lactate removal, reducing tissue edema, and promoting a higher and faster oxygen delivery to the muscle (Cheatham et al., 2015). However, this hypothesis has not been examined.
8
Near-infrared reflectance spectroscopy (NIRS) provides continuous, noninvasive monitoring of the relative concentration changes in oxy-, deoxy- (HHb), and total hemoglobin during exercise, representing an estimate of the fractional oxygen extraction within the microvascular level (Ferrari, Binzoni, & Quaresima, 1997). A previous study has demonstrated that EIMD affects muscle oxygenation kinetics, since it induces impairments in the blood flow to the microvascular level (Davies et al., 2008). The authors observed a ~30% slower HHb kinetics 48h after performing an EIMD stimulus. However, it is unknown if RM can positively change the muscle oxygenation kinetics after EIMD, and thus improving recovery.
Previous studies examining the RM effects on neuromuscular performance following EIMD have not considered two important neuromuscular mechanisms. The first relates to the joint mechanical response, since previous studies have only assessed the maximal joint ROM. However, the joint maximal ROM assessment only informs about the angle performed at the joint, and does not inform about its mechanical profile. By measuring the joint resistance to stretch (i.e., joint passive torque), it is possible to determine whether overall muscle-tendon complexes crossing the joint will have an overall stiffness change, following EIMD, and whether or not RM alters this change. Secondly, from a morphological point of view, although muscle swelling status is an important EIMD recovery marker, most of previous studies have not examined its recovery after RM intervention. Only MacDonald et al. (2014) assessed muscle swelling indirectly through limb girth measurement. However, a sonographic measurement of muscle cross sectional area (CSA) may be a more valid marker of muscle swelling (Chan, Newton, & Nosaka, 2012). In addition, changes in CSA following EIMD are expected to be due to variations in muscle architecture [i.e., fascicles angles (FA) increase without changes in length]. However, it is unknown if these effects are prevented by a RM intervention.
Recently, it has been reported that both EIMD and RM induce contralateral (i.e., crossover) effects. For instance, it is known that a bout of eccentric exercise attenuates the magnitude of EIMD symptoms. This is known as repeated bout effect (RBE). Starbuck et al (2012) demonstrated a contralateral RBE after observing a reduced strength loss in the contralateral elbow flexors 24 hours after EIMD, when the ipsilateral elbow flexors were previously target with an EIMD stimulus. In respect to RM contralateral effects, Aboodarda, Spence, & Button (2015) observed a pain pressure threshold (PPT) increase in both contralateral and ipsilateral limbs after rolling the
9
ipsilateral plantar flexors. Similarly, Jay et al. (2014) observed a tendency for a reduction in perceived soreness 10 minutes after a RM intervention. These studies suggest that recovery (e.g. perceived pain) processes may be mediated by the central nervous system. However, it is unknown if the RM contralateral effects occur following an EIMD stimulus.
11
Objectives and hypothesis
The purpose of this study was threefold: 1) to determine the effectiveness of RM in changing the speed and magnitude of EIMD functional [i.e., maximal isometric force, submaximal sustained force (SSF), maximal ROM, resistance to stretch, PPT, and muscle activity)] and morphological [i.e., CSA and architecture (thickness, fascicle length (FL) and FA)] variables; 2) to examine the existence of RM contralateral effects; and 3) to examine if RM prophylactic effects are due to changes in muscular oxygenation kinetics.
Based on previous literature, we hypothesized that: 1) RM would decrease the negative functional and morphological effects induced by EIMD; 2) contralateral effects would occur in PPT; and 3) the prophylactic RM effect would relate to muscular oxygenation kinetics. For this purpose, two experiments were conducted. In both experiments, EIMD was induced unilaterally to the ankle plantar flexors in two interventions: using and without the using a RM. In experiment 1, functional and morphological variables were assessed before, immediately after, 1h post, 24h post, 48h post, and 72h after EIMD. In experiment 2, muscular oxygenation kinetics were assessed before and 48h after EIMD.
13
Review of literature
1 - Exercise induced muscle damage
1.1 Stimulus characterization
EIMD is a phenomenon that occurs after a bout of unaccustomed exercise, especially when an eccentric component is present (P. Clarkson, 1997). EIMD can last several days, usually peaking at 48-72h after the stimulus (Cheung, Hume, & Maxwell, 2003), manifesting itself as a decrease in muscle function (i.e., maximal force and RFD), an increase in pain perception, and an increase in local swelling and intramuscular blood proteins (Warren, Lowe, & Armstrong, 1999).
Howatson et al. (2008) simplifies the damage model in two stages: 1) the initial damage that occurs during exercise (primary damage); and, 2) the propagation through processes associated with the inflammatory response (secondary damage). When a bout of exercise is performed, damage can come from two different pathways: 1) metabolic and, 2) mechanical (Ebbeling & Clarkson, 1989). The metabolic pathway has been suggested to be a result from ischemia [i.e., possibly causing metabolic waste accumulation, changes in ion concentration and adenosine triphosphate deficiency resulting in damage (Byrnes & Clarkson, 1986)] or hypoxia during prolonged exercise (Armstrong, 1984). Marathon running is an example where damage is possibly caused by a lower metabolite removal (Ebbeling & Clarkson, 1989). However, the presence of an eccentric component induces mechanical stress in the tissues, possibly being the main cause of damage, with metabolic waste accumulation exacerbating this occurrence (Schwane & Armstrong, 1983). Studies performing downhill running as an EIMD protocol support this theory (Armstrong, Ogilvie, & Schwane, 1983).
The mechanical component responsible for muscle damage is related to the mechanical load on the muscle fibers. Since eccentric contractions are capable of producing more force than concentric and isometric (Talbot & Morgan, 1996), and due to the fact that sarcomeres lengthen in an non-uniform manner during the eccentric component (Proske & Morgan, 2001; Talbot & Morgan, 1996), passive structures create more tension resulting in Z-band streaming when the filaments are stretched beyond the point of overlap (Fridén, Sjöström, & Ekblom, 1983). Thus, possibly resulting in a
14
reduction of muscle force production and an increase in passive forces, inducing damage to the tissue (Proske & Morgan, 2001).
After the initial damage phase, there is a manifestation of processes that appear to be initiated by an increase in the intracellular [Ca2+], disrupting its homeostasis, leading to extra myofibrillar damage in skeletal muscle (Duncan, 1987). There is evidence that, in humans, a disruption in calcium homeostasis occurs after lengthening contractions, leading to changes in the sarcoplasmic reticulum (Nielsen, Madsen, Jørgensen, & Sahlin, 2005) causing an influx of Ca2+ into the cytosol and, consequently, producing further damage due to alterations in the cytoskeleton, mitochondria, sarcoplasmic reticulum and myofilaments (Byrd, 1992; Nielsen et al., 2005).
There is enough data to suggest that both primary and secondary phases are associated to the exercise-damage-repair process (Fridén & Lieber, 2001). However, the magnitude for which each are responsible remains unclear. In addition, even though muscle damage occurs mostly in fast-twitch fibers, it is also present in slow-twitch fibers (Sorichter et al., 2001). Research shows that to elicit muscle damage, the eccentric contraction does not need to be maximal (Kazunori Nosaka, Kazunori, & Mike, 2002) even if, with maximal contractions and longer muscle lengths, it may happen at a greater magnitude (Kazunori Nosaka, Kazunori, & Kei, 2001).
1.2 Signs and symptoms responses
As mentioned before, EIMD is a phenomenon that affects different systems in the human body, as for example: muscle function, perception of pain and soreness, muscle architecture, oxygen kinetics and intramuscular blood proteins. The following topics will briefly describe each system.
1.2.1 Muscle function
1.2.1.1 Maximal voluntary isometric contraction
Maximal voluntary isometric contraction (MVIC) has been reported as a reliable way to measure the magnitude of EIMD symptoms (Warren et al., 1999). This assessment consists of the production of a maximal contraction at a fixed joint angle
15
and, therefore, against an immovable resistance. This muscle function becomes impaired immediately after EIMD protocols and its recovery is gradual and prolonged (Warren et al., 1999). Despite the fact that specific muscle group training history affects the magnitude and duration of the symptoms, it has been consistently observed that damage seems to last longer in inactive elbow flexors when compared to the locomotor muscles (i.e., lower limbs) (Byrne, Christopher, Craig, & Roger, 2004). Even though magnitude and duration of the symptoms varies a lot between individuals, Clarkson et al. (1992) reported a 50-60% decrease in strength of the elbow flexors immediately after eccentric exercise followed by a linear recovery to baseline that lasted up to 2 weeks. However, recovery in the elbow flexors can take up to 12 weeks (Sayers & Clarkson, 2001).
As mentioned before, lower limb muscles seem to get a lower impairment in muscle strength when compared to the elbow flexors, possibly due to involvement in everyday activities. 30-40% is an expected decrease in muscle function after an EIMD protocol where approximately 95% of muscle recovery occurs after 7 days (Byrne, Christopher, & Roger, 2002).
1.2.1.2 Rate of force development
RFD is defined as the slope of the force-time curve obtained under isometric contractions. Peñailillo et al. (2015) suggests that measuring RFD might be a better indirect way to assess muscle damage when compared to MVIC. However, MVIC can be a reliable variable to evaluate muscle damage in the subsequent days. Peñailillo et al. (2015) proposes that RFD100-200 is a sensitive and specific marker that may more clearly differentiate between muscle damage and fatigue following eccentric exercise.
Jenkins et al. (2014) also observed that RFD can be a reliable marker of muscle damage. However, instead of following Peñailillo et al. (2015) recommendation of measuring RFD100-200, Jenkins et al. (2014) suggests to evaluate the first 100ms, which provides unique information in addition to peak torque. These authors also found a similar response between peak torque and late phase RFD (i.e., 200ms). In this study, RFD reached the lowest immediately after EIMD, consisting of 6 sets of 10 maximal eccentric isokinetic muscle actions, with a 45-60% decrease. Interestingly, RFD measurements (except RFD200) returned to baseline faster (72h after EIMD) than peak torque and late phase RFD.
16
1.2.1.3 Maximal range of motion
Joint maximal ROM assessment is often performed to evaluate a muscle’s ability to lengthen. When an EIMD protocol is performed, it is common to observe a significant reduction in joint ROM in the following days (Cheung et al., 2003). For instance, after 10 sets of 40 repetitions of plantar flexion, Yanagisawa et al. (2015) noticed an average reduction in ankle ROM at 48h (-40%) and 72h (-50%), returning to baseline only on the 7th day after the damage. Zainuddin et al. (2005) also noticed an average reduction in ROM (-19º) in the elbow joint after 60 maximum voluntary eccentric contractions, peaking on the 4th day.
Interestingly, it seems that there is a different response to muscle damage between upper and lower limbs. For instance, Chen et al. (2011) noticed a ~3 times higher decrement in the elbow flexors and extensors ROM (i.e., 9º reduction 1-2 days after EIMD), when compared to the knee flexors and extensors (i.e., 3º reduction 1-2 days after EIMD). The authors suggest that this difference could be related to the constant exposure of the lower limbs to eccentric actions in daily activities.
1.2.2 Perception of pain and soreness
It is common to every exercise practitioner to feel an increase in pain perception after performing a novel exercise, especially with the presence of an eccentric component, peaking between 48h-72h (Cheung, Hume, & Maxwell, 2003). This pain perception increase resulted from a bout of exercise is called delayed-onset muscle soreness (DOMS), and tends to be lower in the next sessions due to the RBE (K. Nosaka, Sakamoto, Newton, & Sacco, 2001). Since this is an effect that happens every time as a result of EIMD, it became a reliable marker to measure the magnitude of muscle damage, as well as the time course changes. It usually is measured in two different ways: 1) PPT (i.e., using an algometer, applying pressure against the muscle until the subjects reports a pain sensation); and 2) a visual scale to determine muscle soreness.
After an EIMD protocol consisting of 10 sets of 10 of back squats, Pearcey et al. (2015) noticed a significant lower PPT in the quadriceps, peaking at 48h with a 30% decrease. However, tolerance to pain was only 13% lower at 72h. Chen et al. (2011), using a visual analog scale, noticed an increase of ~50% muscle soreness in the elbow
17
flexors and extensors, against 10% and 20% for the knee extensors and flexors respectively, peaking 48h after EIMD, hypothesizing that the lower soreness perception in the lower limbs is due to the constant stimulus in daily living activities with an eccentric component.
1.2.3 Muscle morphology
It is common to observe an increase in muscle swelling after EIMD protocols, especially due to the accumulation of metabolic waste in the muscles (Warren et al., 1999). In order to assess changes in muscle swelling, a measurement of circumference of that body part is usually the used tool. For instance, Zainuddin et al. (2005) observed that, after 60 maximum voluntary eccentric contractions, there was a significant increase in upper arm circumference, peaking between the 4th and 7th day, with an average increase of 10.4mm and 10.9mm, respectively, followed by a reduction to 6.5mm in the 10th day. Ej et al. (2004) measured leg girth after 12 sets of 20 repetitions of a step test. Values peaked on the 3rd day with a ~6mm increase, reaching close to baseline levels on the 8th day. Chen et al. (2011) compared the changes in both upper and lower limbs and observed an increase in both muscle groups. However, lower limb muscles peaked at 48h with ~4mm for knee extensors and ~5mm for knee flexors, while upper limb muscles peaked at 96h with increases of ~10mm for the elbow flexors and ~9mm for the elbow extensors. These values go hand in hand with Zainuddin et al. (2005) and Ej et al. (2004). The authors suggest that a lower increment in the lower limbs is due to the constant stimulus in daily living activities when compared to the upper limbs.
1.2.4 Local muscle deoxygenation kinetics
The equipment commonly used to assess muscle deoxygenation kinetics variables is the NIRS, a non-invasive method to estimate the fractional oxygen extraction within the microvascular level (Ferrari, Binzoni, & Quaresima, 1997) being able to examine the change in oxygenated hemoglobin, HHb, tissue oxygen index and total hemoglobin before, during, and after the exercise.
18
Muscle damage has been demonstrated to alter microcirculation, and consequently to affect oxygen delivery to the working muscle (Kano et al., 2005). Moreover, previous studies found a marked increase in conduit artery blood flow during exercise (Laaksonen et al., 2006) and rest (Sbriccoli et al., 2001), and an increase in capillary diameter in resting muscle, and in the proportion of capillaries that did not support red blood cell flux following eccentric exercise (Kano et al., 2005).
Dysfunctions of this nature could lead to impaired oxygen delivery and distribution within the capillary bed. In addition, oxygen delivery and utilization during exercise might be affected, compromising blood-muscle oxygen flux. Other studies have demonstrated that EIMD affects muscle deoxygenation kinetics. For instance, Davies et al. (2008) observed a ~30% slower HHb kinetics in cycling exercise, 48h after performing 10 sets of 10 squats with 70% of bodyweight. The authors suggested that structural and functional changes of the microvasculature possibly lead to an impairment in the muscle oxygen extraction.
In another study, Ahmadi et al. (2007) reported, after 40 minutes of downhill walking with 5% of subjects’ bodyweight, changes in resting and exercising muscle oxygenation. It was observed a prolonged increment in resting muscle oxygen consumption and an increase of oxygen desaturation and resaturation kinetics during isometric contractions. The authors suggested that several mechanisms could explain the results such as impairment in microcirculatory flow, increases in slow-twitch fiber recruitment, and a higher requirement of energy-demanding repair processes due to the presence of muscle damage leading to increments in resting muscle oxygen utilization.
1.2.5 Intramuscular blood proteins
Lastly, CK and Mb are commonly measured to assess the presence and magnitude of muscle damage. As mentioned before, there seems to be differences in muscle damage magnitude between upper and lower limbs. For instance, Chen et al. (2011) observed a higher increase of CK and Mb in the upper limbs. CK increased to ~2000 IU/L and 2500 IU/L in the elbow extensors and flexors respectively, while the lower limbs only showed an increase of ~200 IU/L and 1000 IU/L (peaking on the 4th day) for the knee extensors and flexors respectively. Mb showed the same relative response with increases up to ~400 ug/L in the upper limb and only ~20 ug/L and 200
19
ug/L for the knee extensors and flexors respectively, peaking at the same time as CK measurements.
Zainuddin et al. (2005) observed similar results in the elbow flexors with CK levels peaking at ~3000 IU/L on the 4th day, reaching close to baseline levels on the 10th day. Margaritelis et al. (2015) also assessed CK after different EIMD protocols reaching levels of ~2000 IU/L on the 3rd day.
1.3 Prevention methods
Since EIMD affects several components of human performance, it is important to define strategies to reduce either the magnitude or the duration of the symptoms. Therefore, different methods have been suggested over the years to enhance recovery such as stretching, light exercise, cryotherapy, previous damaging exercise (i.e., RBE), and massage (Rui Torres, Ribeiro, Alberto Duarte, & Cabri, 2012).
1.3.1 Stretching
SS is a common practice, especially after training, with the objective of reducing muscle soreness and aid recovery. However, even though some studies report a
reduction in muscle stiffness (R. Torres, Appell, & Duarte, 2007; Rui Torres, Pinho, Duarte, & Cabri, 2013), most of the literature show little to no benefits after using this method as a strategy to prevent and recover from EIMD symptoms (Howatson et al., 2008; Rui Torres et al., 2012). Even when measuring perceived pain as a marker of EIMD, SS showed no benefits at attenuating the muscle soreness increase (Herbert & Gabriel, 2002).
1.3.2 Cryotherapy
In order to minimize DOMS, cryotherapy is one of the strategies used after exercise, especially in sport environments. The application of cold results in changes in skin, subcutaneous, intramuscular and joint temperature, diminishing edema and
20
inflammatory processes by stimulating cutaneous receptors leading to vasoconstriction (Sellwood, Brukner, Williams, Nicol, & Hinman, 2007). A review by Banfi, Lombardi, Colombini, & Melegati (2010) found that whole body cryotherapy modifies physiological and biochemical parameters, with a decrease in proinflammatory cytokines, changes in antioxidant status, and positive effects on muscular enzymes such as CK and lactate dehydrogenase, closely related to muscle damage.
Even though some studies show benefits after cryotherapy interventions, it is not possible to make a solid recommendation of this method as a recovery strategy, due to the inconsistency of the results (Torres et al., 2012). Costello et al. (2015) concluded that there is insufficient evidence to support whole body cryotherapy as a strategy to reduce soreness and subjective fatigue. Interestingly, when it does, it fails to translate into enhanced functional recovery (Bleakley, Bieuzen, Davison, & Costello, 2014). In addition, there’s evidence that cold-water immersion after resistance exercise may suppress ribosome biogenesis, which could impair the hypertrophic response (Figueiredo et al., 2016).
1.3.3 Exercise
Low-intensity exercise is another commonly used method to improve recovery after EIMD, increasing blood circulation, facilitating the removal of toxic products and release of endorphins, leading to a reduction in pain perception (Hough, 1902). This analgesic effect might also be caused by an increased stimulation of sensitive fibers type Ia, Ib and II, possibly leading to an interference in pain perception carried by type III and IV (Weerakkody, Whitehead, Canny, Gregory, & Proske, 2001).
Torres et al. (2012) did not find sufficient evidence to support the idea of low-intensity exercise as an effective recovery strategy from EIMD, especially in reducing muscle soreness. However, other authors (Hasson, Scott, William, Marque, & Jay, 1989; Saxton & Donnelly, 1995; Zainuddin, Sacco, Newton, & Nosaka, 2006) showed temporary analgesic effects from this recovery modality.
21 1.3.4 Repeated bout effect
As mentioned before, EIMD symptoms occur after a bout of unaccustomed exercise, especially with an eccentric component. However, after a second bout of exercise, the magnitude of the symptoms reduces significantly. This protective effect is called RBE and its duration might last several weeks up to 6 months (K. Nosaka, Sakamoto, Newton, & Sacco, 2001). To explain this phenomenon, three main theories were hypothesized. The neural theory refers that there is an increase in motor unit activity, slow-twitch fiber recruitment, and motor unit synchronization. Connective tissue theory mentions that there is an increased intramuscular connective tissue and an intermediated filament remodeling. Cellular theory indicates that there is a strengthening of cell membranes, removal of weak fibers and a longitudinal addition of sarcomeres (McHugh, Connolly, Eston, & Gleim, 1999). Other mechanisms that might be responsible for the RBE are the strengthening of the sarcoplasmic reticulum (P. M. Clarkson & Tremblay, 1988) and a blunted inflammatory response due to a decrease in neutrophil and monocyte activation (Pizza et al., 1996).
Even though RBE protects the ipsilateral limb for several weeks from a second bout of exercise, there seems to be an effect in the contralateral limb as well. For instance, Starbuck & Eston (2012) observed a protective effect in the contralateral limb for 2 weeks, while Xin et al. (2013) found a reduced performance loss after 4 weeks, but no benefits in muscle soreness and serum CK.
1.3.5 Massage
Massage is probably the recovery modality with the most robust benefits, increasing blood circulation, decreasing edema and contributing to muscle repair (Rui Torres et al., 2012). It has been suggested by Rapaport, Schettler, & Breese (2010) and by Crane et al. (2012) that massage reduces the inflammatory response by decreasing cytokine levels. Rui Torres et al. (2012) confirms that massage has benefits regarding EIMD, especially when administered for 20-30 minutes immediately or up to 2 hours after exercise, relieving muscle soreness at 24h. The authors hypothesize that massage may stimulate afferent fibers Ia, Ib and II leading to a reduction in pain transmission,
22
possibly in the same way as low-intensity exercise. However, this phenomenon is only temporary.
Massage seems to have a statistically significant but clinically small effect on strength loss recovery from an EIMD protocol at 1h, even though other variables show conflicting and contradictory results (Torres et al., 2012). While some studies found benefits from massage on limb girth (McDermott, Char, Goya, Whliehurst, & Lightfoot, 1992) and neutrophil count (Smith et al., 1994), others found no changes in the same variables (Zainuddin, Newton, Sacco, & Nosaka, 2005; Hilbert, Sforzo, & Swensen, 2003).
While manual massage is commonly associated with recovery, recent research is finding that equipment like FR and RM might offer similar benefits (Cheatham, Kolber, Cain, & Lee, 2015).
2 - Foam roller and roller massager
2.1 Definitions and types
FR and RM are popular self-manual therapy (SMT) tools, commonly used by fitness and rehabilitation professionals to improve joint passive ROM, increase PPT, and aid recovery by decreasing EIMD symptoms (Cheatham et al., 2015). Using his own bodyweight, the user applies a self-adjusted pressure onto the FR while performing rolling motions, usually at a constant rate for a designed time period. In the case of a RM, the user selects a constant pressure that might be chosen based on a percentage of total bodyweight (Sullivan et al., 2013) or on perceived pain during the rolling protocol (Aboodarda et al., 2015).
There are different SMT equipment including FR, RM, and even a tennis ball can be used for a specific tender spot. FR and RM have different sizes, shapes and densities, being the latter an important factor regarding soft tissue massage, if the goal is to target a deeper layer.
23
2.2 Variables
2.2.1 Intensity
Intensity during rolling protocols is not a well-established variable. Despite a variety of interventions, we can observe the occurrence of some common instructions to control rolling intensity, such as:
Amount of bodyweight over the FR (Pearcey et al., 2015);
Perceived pain during the protocol (Macdonald, Button, Drinkwater, & Behm, 2014);
Combination of both (Junker & Stöggl, 2015).
Interestingly, during a pilot test in a study designed by Sullivan, Silvey, Button, & Behm (2013), the RM was rolled over a force plate by experienced professionals to determine the typical amount of force individuals would exert. The intensity used during the intervention itself was determined by the average of the collected values (13kg). Even though there are no studies comparing different intensities during rolling protocols, the most common instructions are to apply as much bodyweight as possible on the equipment or to reach a perceived pain of 7 in a scale of 0 to 10.
2.2.2 Duration
During rolling protocols, total duration is another variable that has not yet been established. However, there seems to be a duration-dependent effect. Sullivan et al. (2013) compared 1 or 2 sets of 5 or 10 seconds, while Bradbury-Squires et al. (2015) compared 5 sets of 20 or 60 seconds, showing a tendency for major effects seen with higher protocol durations.
In FR and RM interventions, total duration ranges from 2 to 5 sets of 30 to 60 seconds (Cheatham et al., 2015). Further research is needed to find out the necessary time to produce benefits, if there is a diminishing returns response, and if too much can elicit any harm.
24 2.2.3 Density
Density is a variable than can affect the tissue layers in which the equipment specifically targets. When the main goal is to target deep tissue layers of a specific muscle, a rigid roller might be the best option since a greater mean pressure and a lower mean contact area are present with this type of equipment (Curran, Fiore, & Crisco, 2008).
2.3 Effects
2.3.1 Range of motion
SS is one of the best methods to improve ROM but the potential power and force production decrements may become a limitation, even though these impairments can be reduced when stretching is performed at lower durations and intensities (Behm, Blazevich, Kay, & McHugh, 2016). However, research shows that FR and RM may offer acute increases in ROM without subsequent performance impairments (Cheatham et al., 2015).
Below is a brief description of different research methodologies as well the results found regarding ROM changes in FR and RM. Overall, studies show an acute effect for different muscle groups, with only one showing long term results when applied for a longer period of time (Junker & Stöggl, 2015).
2.3.1.1 Foam roller
Mohr, et al. (2014) investigated the effects of FR and SS on hip-flexion ROM after six consecutive sessions. Four groups were assigned: 1) FR; 2) SS; 3) FR + SS; 4) Control. FR participants applied as much bodyweight as possible on the equipment and moved at a cadence of 1 second per roll, for three 1 minute repetitions with 30 seconds between sets. SS protocol consisted of three consecutive passive stretches to the point of discomfort without pain, for the same duration as FR treatment. The subjects in the combined condition performed both protocols one next to the other. ROM measurements were collected immediately post-intervention and regardless of
25
treatment, there was a significant change in passive ROM. However, the combination of FR and SS produced the greatest effect. Interestingly, there was no significant differences between FR and SS.
Škarabot et al. (2015) compared the acute effects of FR, SS and a combination of both on passive dorsiflexion ROM in resistance trained adolescent athletes, with at least six months of FR experience. All subjects went to the gym on 3 different occasions, the same time of the day, with at least 24h between sessions. In each session, they performed one of the three treatments in a randomized manner, always in the dominant leg. Ankle dorsiflexion ROM measurements were collected before each session (control measurements), immediately after, 10, 15, and 20 minutes post-intervention. SS consisted of three 30 second plantar flexor stretches to the point of discomfort but no pain, with 15 seconds between sets. FR protocol had the same duration, in order to have similar volumes, and subjects were instructed to apply as much pressure on the equipment as possible. The combination of FR and SS consisted of the FR intervention directly followed by the SS protocol. There was an acute increase in ROM for all interventions and FR + SS had an additive effect in comparison with FR alone, but not with SS. However, all interventions had time courses that lasted less than 10 minutes. Time course differences were present immediately after intervention and post-hoc testing revealed these were only for SS and FR+SS, with the number of subjects being a possible justification for the lack of significance for FR.
A main limitation of these studies is the different intervention volume (i.e., total treatment duration) between methods. When both treatments are combined, instead of adjusting the duration of each protocol to match total volume, subjects would perform one intervention next to the other, having double the duration of stimulus, which could affect the results since there seems to be a dose response relationship (Sullivan et al., 2013).
MacDonald et al. (2013) examined the effects of FR on knee joint ROM, and volitional and evoked quadriceps muscle force. A within-subject design was used, and each one performed the experimental conditions over four sessions, with 24-48h rest between, with measurements being taken before, 2 minutes and 10 minutes post-intervention. Subjects rolled the right quadriceps for 2 sets of 1 minute, with 1 minute rest between bouts, applying as much body mass as possible onto the FR. Results showed a significant increase in knee-flexion ROM of 10º at 2 minutes and 8º at 10 minutes post-FR intervention when compared to the control group.
26
Junker & Stöggl (2015) compared the effects of FR and contract-relax proprioceptive neuromuscular facilitation (CRPNF) on hamstring flexibility. All subjects performed a stand and reach flexibility test and were randomly assigned to one of two intervention groups: FR or CRPNF. A training protocol was handled to both groups to perform three times per week, for four weeks, and subjects were asked to document each training session. FR intervention consisted of 3 sets of 30-40 seconds performed in each leg with a pressure on their pain threshold. CRPNF group performed 3 stretches at approximately 25% of MVIC, increasing ROM until an uncomfortable stretching sensation was felt. After a 6 second contraction, subjects would increase the stretch within 10 seconds, repeating this process 3 times per set. 3 total sets were performed. Results from this investigation showed an improvement in ROM in both groups, with no statistically significant differences between protocols.
Markovic (2015) compared the acute effects of FR and a new form of instrument assisted soft-tissue mobilization on hip and knee ROM. The experiment consisted of two sessions separated by 24h. During the first one, warm-up was followed by an initial ROM measurement, intervention and a final ROM assessment. FR protocol consisted of two 1 minute bouts with 30 seconds rest between sets, repeating the process for the other muscle group. The condition using the new instrument had the same intervention duration. Results showed an increase in ROM in both groups post-intervention. However, even though FR increased hip and knee ROM post-intervention in 9% and 5% respectively, these measurements returned to baseline 24h post-intervention, while the new tool showed an increase of double the ROM and kept all of these changes 24h later.
Peacock et al. (2015) investigated the effects of FR along two different axes of the body in combination with a dynamic warm-up. This study had a counterbalanced, crossover, within-subjects design, comparing mediolateral (along the sagittal plane) and anteroposterior (along the frontal plane) rolling separated by seven days, with testing (i.e., flexibility and other performance tasks) being performed post-intervention. Both protocols consisted of 5 rolls per 30 seconds targeting several muscle groups. After the FR protocol, both groups performed a general full body warm-up routine. Results showed a statistically significant ROM improvement in the mediolateral group when compared to the anteroposterior condition (p<0.05) since it directly targeted the posterior part of the body, including the hamstrings.
27
Bushell, Dawson, & Webster (2015) investigated the effects of FR on hip extension ROM in a lunge position. The experimental group rolled the anterior portion of the thigh along the length of the muscle, for three 1 minute bouts with 30 seconds rest in between. Subjects participated in three testing sessions, one week apart, with measurements collected before and immediately post-intervention. Results showed a significant increase in hip extension ROM during the second session in the experimental group, even though these measurements returned to baseline after one week.
2.3.1.2 Roller massager
Halperin et al. (2014) compared the effects of SS and RM on ROM and performance. Subjects visited the laboratory in two different occasions, three to six days apart. After baseline measurements, participants performed one of the two interventions in a randomized order: SS or RM. Both interventions involved three repetitions of 30s with 10s rest between each bout. Prior to warm-up, subjects from RM intervention were informed about the protocol and were instructed on how to use the equipment. RM protocol took place while the participants were seated on a chair with their knees flexed at 90 degrees. Subjects were instructed to apply pressure equivalent to a pain level of 7 out of 10 at a pace of 1 second per roll. SS protocol consisted of subjects having one leg on the edge of an aerobic step while leaning against the wall with their hands. Their heel was pointing towards the ground, their knee was extended, and they were asked to stretch at the same perceived intensity as the RM group. At 1 and 10 minutes post-intervention, participants performed two other cycles of testing. The main findings of this study were that both SS and RM significantly improved ROM in the ankle joint up to 10 minutes after the interventions by approximately 4%. RM led to significantly greater force production relative to SS (8.2%). SS led to a small and statistically insignificant decrease in MVC (~4%), while RM led to small increase in MVC 10 minutes after the intervention of approximately 4%. Accordingly, both RM and SS led to similar improvements in ROM.
Sullivan et al. (2013) investigated the effects of RM on ROM and subsequent performance by comparing four different protocols, in order to determine the duration and volume necessary to produce any benefits. This intervention had four conditions: 1) 1 set of 5 seconds; 2) 2 sets of 5 seconds; 3) 1 set of 10 seconds; 4) 2 sets of 10 seconds.
28
These protocols were performed in two different days, two conditions per session (one in each leg). To avoid possible crossover effects, the second condition of the session was performed 30 minutes after the first one. Rolling intensity was kept constant for all subjects (13kg), determined previously in pilot testing representing the average of the typical force subjects would exert while rolling the muscle. Measurements were taken before and 3 minutes post-intervention. Results showed a significant main effect for time with an increase in ROM from pre to post-intervention of 4.3%. Moreover, there was a trend toward a group main effect with 10 seconds exceeding 5 seconds by 2.3%. Except from the control group, all subjects had an increase in ROM.
Bradbury-Squires et al. (2015) investigated the effects of different RM protocol durations on ROM, pain perception, and electromyography (EMG) of the quadriceps and hamstrings during a lunge. RM protocol consisted of 5 sets of 20 or 60 seconds per repetition with 60 seconds between bouts, with a constant pressure of 25% of bodyweight, at a continuous rate of 4 seconds per cycle. When compared to the control group (i.e., no treatment), both interventions produced an increase in ROM of 10% and 16%, for 20 seconds and 60 seconds respectively, with a trend for a greater increase in the 60 seconds group.
Even though most of the studies show an increase in ROM after a rolling protocol, there are exceptions. For instance, Jay et al. (2014) investigated the acute effects of RM on soreness, ROM and potential crossover effects. Subjects visited the laboratory in two sessions separated by 48h. In the first session, after collecting baseline measurements, an EIMD protocol was performed consisting of 10 sets of 10 repetitions of stiff-legged deadlifts with a kettlebell, with a 30 seconds rest between sets. In the second session, after measurements collection, subjects were assigned to one of three groups: 1) RM leg; 2) RM control leg; 3) Control. Measurements were collected 10, 30 and 60 minutes post-intervention. RM protocol consisted of 10 minutes of rolling in one leg, at a cadence of 1-2 seconds per stroke, with a moderate pressure. Results showed a ROM decrement in the beginning of the second session (i.e., 48h after EIMD protocol). However, RM group was the only one that showed an increase in ROM, but only at 10 minutes post-intervention.
Couture et al. (2015) investigated the effects of different FR protocol durations on hamstring ROM. This study consisted of three sessions. The first one was used for pre-treatment / baseline measurements and FR technique practice. In the second and third sessions, each subject was randomly assigned to one of two protocols: 1) 4 sets of
29
30 seconds; 2) 2 sets of 10 seconds. Both protocols had 30 seconds of rest between sets and subjects were asked to apply as much pressure as possible on the FR, at a cadence of 40 bpm. No significant differences were observed after intervention. However, the pressure per unit that was exerted by the roller onto the tissue could be a limitation that might explain the lack of benefits.
Vigotsky et al. (2015) investigated the effects of two 1 minute bouts of FR of the anterior thigh on acute hip extension ROM, knee flexion ROM and rectus femoris length. After a 10 minute dynamic warm-up, baseline measurements were collected. Immediately after, subjects performed a FR protocol consisting of two 60 second bouts with 30 seconds of rest between sets on the right anterior thigh, at a slow cadence, applying their bodyweight onto the roller. The authors found that even though a small change in hip extension ROM was observed, there were no changes in knee flexion ROM.
Mikesky et al. (2002) assessed the acute effects of the stick, similar to a RM, on hip ROM and muscle performance. Hamstrings were self-massaged by the subject for 2 minutes before the flexibility test. None of the performance measurements were acutely affected by the pre-treatment with the stick.
The authors suggest several explanations for the FR and RM effects on ROM. Firstly, rolling might lead to an elevation in intramuscular temperature, responsible for an increase in the viscoelastic properties of the muscle (Knight, Rutledge, Cox, Acosta, & Hall, 2001). Moreover, changes in thixotropic properties of muscle and fascia may be responsible for the results, decreasing tissue viscosity and creating a fluid extracellular environment, becoming less resistant when a stretch is applied. Possible increases in blood flow might be seen as an explanation since arterial distensibility is associated with flexibility. Case in point, Okamoto, Masuhara, & Ikuta (2014) observed an acute reduction in arterial stiffness and improved endothelial vascular function after a FR intervention. Lastly, since tolerance to stretch is one of the benefits reported in massage literature (Aquino et al., 2010), several authors suggest that the effects of FR on ROM might be due to neural mechanisms, by stimulating the Golgi receptors, inhibiting the muscle spindle activity and decreasing muscular tension, the autogenic inhibition.
30 2.3.2 Recovery
Using SMT equipment after exercise sessions, such as FR or RM, is a common practice with the objective of improving recovery rate and reduce the magnitude of the symptoms (i.e., muscle performance loss and increased muscle soreness). For instance, Macdonald et al. (2014) measured the effects of FR as a recovery tool after an EIMD protocol. In this study, variables were measured at baseline, post-EIMD protocol (10 x 10 squats with 60% of 1RM), 24h, 48h and 72h. FR intervention was performed in the end of each session, consisting of five different exercises targeting the major muscle groups for 2 sets of 60 seconds in each side, at a constant rate, by applying their bodyweight onto the FR. Results showed a benefit of FR in attenuating the decrements in lower extremity muscle performance, by improving both passive and static-dynamic hip flexion ROM, muscle activation, vertical jump height, and reducing perceived pain in the subsequent days after muscle damage.
Pearcey et al. (2015) investigated the effects of FR on DOMS and recovery of dynamic performance tasks. Variables were measured at baseline, 24h post-EIMD protocol (10 x 10 squats with 60% of 1RM), 48h and 72h. FR intervention was performed in the end of each session, consisting of rolling the quadriceps, adductors, hamstrings, iliotibial band, and gluteal muscles for 1 set of 45 seconds with 15 seconds rest for each muscle, repeating the protocol one time. Subjects were asked to apply as much bodyweight as possible onto the equipment. FR promoted an enhanced recovery from DOMS and reduced physical performance decrements after EIMD. There was an increase in PPT, power, speed sprint and strength-endurance at all-time points when compared to the control group.
Jay et al. (2014) found that with a RM intervention 48h after a DOMS inducing protocol, subjects showed a significantly higher PPT and lower muscle soreness at 0, 10 and 30 minutes post-intervention when compared to control. However, at 60 minutes, PPT was no longer statistically lower compared to control.
The authors suggest several mechanisms to explain the effects of FR on enhanced recovery. Firstly, an increase in blood flow and subsequently decreased inflammation reducing edema, enhancing tissue healing, and blood lactate removal (Smith et al., 1994). Furthermore, massage could also lead to systemic biochemical effects such as increased neutrophil levels and reduced plasma CK (Smith et al., 1994). Lastly, pain reduction might be related to this enhanced recovery.
31 2.3.3 Pain pressure threshold
Increases in PPT and reduction in muscle soreness are two common benefits reported after FR and RM interventions. As mentioned before, Aboodarda et al. (2015) investigated the immediate effects of RM on PPT, as well as the time course of acute changes following each type of intervention. The major findings of this study were that heavy rolling and massage led to an increased PPT when compared to light rolling and control, with the presence of a significant effect in the contralateral calf. However, these increases were transient and regardless of intervention, PPT values decreased over time, with results showing a statistically significant decrease at 15 minutes when compared to 30 seconds post massage.
The most plausible explanation suggested by the authors is the effect of heavy tissue massage in the central pain-modulatory systems. More specifically, the mechanical pressure created by massage can provide an analgesic effect via the ascending pain inhibitory system, by activating mechanoreceptors and proprioceptors, possibly altering the transmission of ascending nociceptive information and therefore, allowing a modulation of pain perception. Another central nervous system pain-modulatory mechanism proposed is the descending antinociceptive pathway, which is evoked by nociceptive stimulus like massage, that ascends from the spinal cord to the brain inhibiting pain transmission, leading to a lower pain perception not only locally but also at distant places. Furthermore, the removal of trigger points from muscle tissue, which usually lead to musculoskeletal pain (Borg-Stein & Simons, 2002), might be responsible for decrements in pain perception. Lastly, PPT decrease in the light massage group might be explained by the fact that the descending antinociceptive system has a greater influence on input from muscle nociceptors than skin nociceptors (Mense, 1998) and since light massage intervention was not a painful stimulus, the decrement in this variable could be associated with an increased sensitivity of superficial nociceptors.
2.3.3 Warm-up
Even though FR and RM are usually used as a recovery tool, they are also utilized before training sessions, paired with dynamic warm-up, as a means to increase ROM without subsequent muscle performance impairments and hopefully, promoting