BrazJOtorhinolaryngol.2017;83(6):720---722
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
The
facial
palsy
as
first
symptom
of
the
temporal
bone
lung
cancer
metastasis
夽
A
paralisia
facial
como
primeiro
sintoma
de
metástase
de
câncer
pulmonar
no
osso
temporal
Dragoslava
Djeric
a,
Ivan
Boricic
b,
Nada
Tomanovic
b,
Ljiljana
Cvorovic
a,
Srbislav
Blazic
a,
Miljan
Folic
a,∗,
Igor
Djoric
caUniversityofBelgrade,FacultyofMedicine,ClinicalCenterofSerbia,ClinicforOtorhinolaryngologyandMaxillofacialSurgery,
Belgrade,Serbia
bUniversityofBelgrade,FacultyofMedicine,InstituteofPathology,Belgrade,Serbia cClinicalCenterofSerbia,DepartmentofRadiology,Belgrade,Serbia
Received19August2015;accepted17September2015 Availableonline19December2015
Introduction
Lungcancerusuallyspreadsbylymphaticorhematogenous route;aroundonefifth ofnewlydiagnosedlung adenocar-cinomaspresent withdistantmetastasesinorganssuchas brain,adrenalglands,liverandbones.1However,lung can-cer metastases in the temporal bone are quite rare,and assuch,present substantialdiagnostic challenge. Clinical manifestationsofmetastaticdiseaseinthetemporalbone areusuallyobscureandmayincludesymptomssuchas hear-ingloss,tinnitus,vertigo,facialpalsy,otalgia,otorrheaand headache.Theoccurrenceofanosteolyticlesioninthe tem-poralbone(evenintheabsenceofaknownprimarytumor) shouldalwaysbeconsideredasapossiblemetastasis,
espe-夽 Please citethis article as:Djeric D, Boricic I, Tomanovic N,
CvorovicL,BlazicS,FolicM,etal.Thefacialpalsyasfirstsymptom ofthetemporalbonelungcancermetastasis.BrazJ Otorhinolaryn-gol.2017;83:720---2.
∗Correspondingauthor.
E-mail:[email protected](M.Folic).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.
cially inelderlypatients. The authorspresent ararecase ofan otogenicfacialpalsyandmetastasis inthetemporal boneasan initialmanifestationoflung canceranddiscuss potential diagnostic pitfalls. This paper wasapproved by theEthicsCommitteeofClinicforOtorhinolaryngologyand MaxillofacialSurgery.
Case
report
A 73-year-old female patient presented with peripheral facial palsy and otalgia that were treated for about two months in a primary health care center. After an incom-pleteresolutionofsymptoms,thepatientwasadmittedinto ourfacilityforadditionaldiagnosticsandfollow-up. Otomi-croscopic examinationontheleftearrevealed hyperemic tympanicmembranewithprominent parsflaccida.Patient also had left periphery facial palsy (House-Brackmann scale, grade3),conductivelefthearing loss(airbone gap 30dB), B-typetympanometry, high rateofC-reactive pro-tein(60mg/L)andleukocytosis(14×106L−1). Patienthad normalbodytemperature,andwaswithoutnauseaor dizzi-ness.Accordingtomedicalrecord,patientwastreatedfor chronicobstructivebronchitisandosteoporosis,withregular controlsandfollow-up.
http://dx.doi.org/10.1016/j.bjorl.2015.09.007
Thefacialpalsyasfirstsymptomofthetemporalbonelungcancermetastasis 721
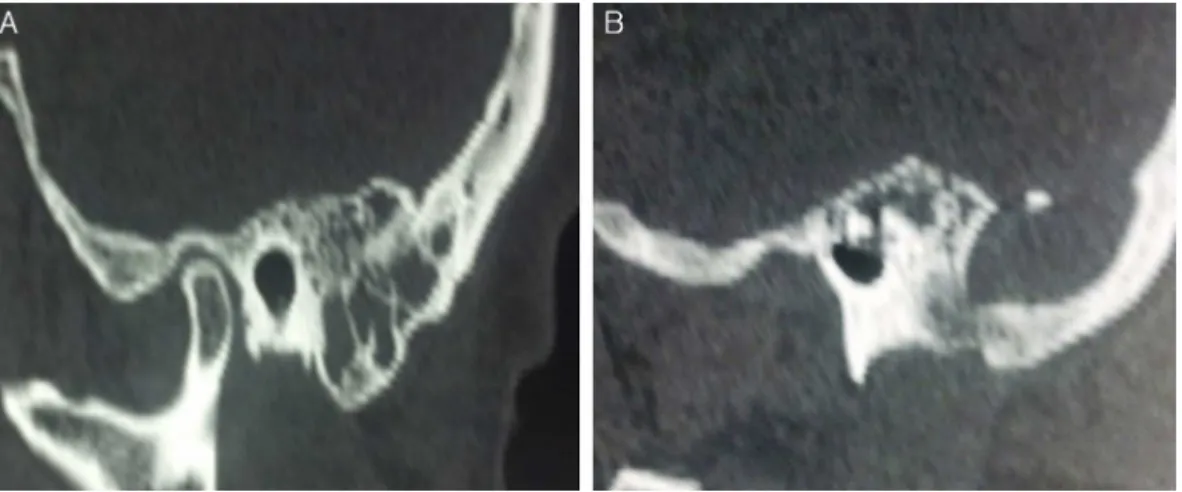
Figure1 (A)TemporalboneCTscan:thickenedmucosawithinthemastoidaircells.(B)Presenceofanexpansiveosteolytic temporalbonelesion;notethedestructionofmastoidapex.
Figure2 Immunohistochemicalanalysis:atypicaltumorcells thatshowstronganddiffusenuclearpositivityforTTF-1 anti-body.Streptavidin-biotin,originalmagnification400×.
Temporal bone computed tomography (CT) revealed mucosalthickeningwithinthemastoidaircells, osteolytic lesionin theleftmastoidandoccipitalbone andthe het-erogeneous mass in the middle ear structures (Fig. 1). Treatment with intravenous antibiotics ensued (Ceftria-xone2g/perday),withoutanyimprovementofsymptoms. Patienthadnosignsorsymptomsofthemalignantdisease; chestradiographyshowednosignsoflungcancer.
During surgery, the mastoidectomy, paracenthesis and ventilation tube implantation were performed. We noted presenceof soft,friable,granulation tissueintheantrum andinthemastoid;fragmentsweresentfor histopatholog-icalanalysis.
Histopathological and immunohistochemical analysis revealed presence of rare atypical cells that were cytokeratin-andTTF-1positive(Fig.2).Therefore,thecase wasdiagnosedasthemetastasisoflungcarcinoma.ChestCT scan, bronchoscopy and histopathological analysis of lung samples ensued; these additional analyses confirmed the diagnosis of a lung adenocarcinoma that waslocalized in theapicalsegmentoftheleftlung. Inaveryshortperiod of time, our patient---who at the time also had bilateral
mediastinallymphnode enlargement---diedsuddenly, prior toanyspecificoncologicaltreatment.
Discussion
Metastases in the temporal bone are relatively rare; the most common primary sites usually are breast, lung, kidney and stomach cancers.2---5 The pattern of metastaticspreadtoward the temporal bone mayinvolve lymphatic/hematogenous route, diffuse metastatic lep-tomeningealcarcinomatosisor directextensionoftumor.2 Lung cancer usually spreads via hematogenous route, in headandneckregionusuallytowardbrain.1,2,5Inourcase, metastatic spread was due to lymphatic/hematogenous spread of tumor cells that also caused mediastinal lym-phadenopathy. Due to hematogenous spread, tumor cell embolimayfavorthepetrous apexof thetemporalbone, whichhasbonemarrowthatisirrigatedbyaslow-flow cap-illarynetwork.
Clinical examination of patients with temporal bone metastasismayshowvariousfindings,suchasretroauricular softtissueswellingorswellingofthetissuestructuresinthe externalauditorycanal,inflammation(suchasotitismedia witheffusion),perforationoftympanicmembrane,otalgia, facialparalysisandseveralothers;insomecases,metastasis inthetemporalbonemayevenbewithoutsymptoms.6,7
Facialnervepalsycanbecausedbyamyriadofcauses; in about two-thirds of the cases etiology is idiopathic or infective.8 Other causes include trauma, inflammatory and/or autoimmune diseases and primary or secondary tumors. Considering the sudden onset of facial paralysis andclinicalpresentation,ourpatientwasinitiallydiagnosed as an acute otitis with otogenic facial palsy. In absence of response to treatment (antibiotics, antiviral agents or steroids), CTscan is obligatory. Cases of prolonged facial paralysisareindicativeoffacialnerveexploration.9During surgeryof elderly patients withosteolytic temporal bone lesions,samples for histopathological analysis are obliga-tory;wefoundasoft,friabletissuepronetohemorrhagein themastoidthatwassentforhistopathologicalanalysis.
722 DjericDetal.
immunohistochemical analysis enabled accurate diagnosis withprimarysiteidentification.FurtherCT,bronchoscopic andhistopathologicalexamination confirmedthediagnosis of a primary lung adenocarcinoma. The whole diagnostic processlasted nearlythree months,and our patientdied withoutspecificcancertreatment.
Conclusion
Metastaticdiseaseshouldalwaysbeconsideredinpatients withfacialnerveparalysiswhoalsohadahistoryof malig-nantdisease.Ourcaseisquiteunique:otogenicfacialpalsy wasaninitialmanifestationoflungcancer;thefacialpalsy wastheresultoftemporalbonemetastasis.Therefore,one shouldalways excludea possible temporal bone metasta-sis in elderly patients with and even without the history ofmalignantdisease,especiallywhenthereisevidenceof temporalboneosteolysis.4---7
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
Thispaperwassupported,inpart,bytheSerbianMinistry ofScience(ProjectNo.175026).
References
1.Quint LE, Tummala S, Brisson LJ, Francis IR, Krupnick AS, Kazerooni EA, et al. Distribution of distant metastases from newly diagnosed non-small lung cancer. Ann Thorac Surg. 1996;62:246---50.
2.YodaS,CureogluS,PaparellaM.Pulmonary carcinoma metas-tasis to the internal auditory canal. Otol Neurotol. 2011;32: e48---9.
3.StreitmannMJ,SismanisA.Metastaticcarcinomaofthetemporal bone.AmJOtol.1996;17:780---3.
4.LanMY,ShiaoAS, LiWY.Facialparalysiscausedbymetastasis ofbreastcarcinomatothetemporalbone.JChinMedAssoc. 2004;67:587---90.
5.Bakhos D, ChenebauxM, Lescanne E, Lauvin MA, Cormier B, RobierA.Twocasesoftemporalbonemetastasesaspresenting signof lungcancer.EurAnn OtorhinolaryngolHead Neck Dis. 2012;129:54---7.
6.ChoiSH,ParkIS, KimYB,HongSM.Unusualpresentationofa metastatictumortothetemporalbone:severeotalgiaandfacial paralysis.KoreanJAudiol.2014;18:34---7.
7.YildizO,BuyuktasD,EkizE,SelcukbiricikF,PapilaI,PapilaC. Facialnervepalsy:anunusualpresentingfeatureofsmallcell lungcancer.CaseRepOncol.2011;4:35---8.
8.GvS,BsM,GoelS,SinghMP,AstekarM.Facialpainfollowedby unilateralfacialnervepalsy:acasereportwithliteraturereview. JClinDiagnRes.2014;8:34---5.