www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Postoperative
otorhinolaryngologic
complications
in
transnasal
endoscopic
surgery
to
access
the
skull
base
夽
Ricardo
Landini
Lutaif
Dolci
a,b,∗,
Marcel
Menon
Miyake
a,b,
Daniela
Akemi
Tateno
a,b,
Natalia
Amaral
Canc
¸ado
a,b,
Carlos
Augusto
Correia
Campos
a,b,
Américo
Rubens
Leite
dos
Santos
b,c,
Paulo
Roberto
Lazarini
a,baIrmandadedaSantaCasadeMisericórdiadeSãoPaulo,DepartamentodeOtorrinolaringologia,SãoPaulo,SP,Brazil bFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSC-SP),SãoPaulo,SP,Brazil
cIrmandadedaSantaCasadeMisericórdiadeSãoPaulo,DepartamentodeCirurgia,DisciplinadeNeurocirurgia,
SãoPaulo,SP,Brazil
Received7February2016;accepted14April2016 Availableonline31May2016
KEYWORDS
Nasoseptalflap; Endonasal; Endoscopic; Skullbase; Complications; Otorhinolaryngologic
Abstract
Introduction:Thelargeincreaseinthenumberoftransnasalendoscopicskullbasesurgeries isaconsequenceofgreaterknowledgeoftheanatomicregion,thedevelopmentofspecific materialsandinstruments,andespeciallytheuseofthenasoseptalflapasabarrierbetween thesinustract(contaminatedcavity)andthesubarachnoidspace(sterilearea),reducingthe highriskofcontamination.
Objective: Toassesstheotorhinolaryngologiccomplicationsinpatientsundergoingendoscopic surgeryoftheskullbase,inwhichanasoseptalflapwasused.
Methods:This was aretrospective study thatincluded patients who underwentendoscopic skull basesurgerywithcreation ofanasoseptal flap,assessing for thepresenceofthe fol-lowingpost-surgicalcomplications:cerebrospinalfluidleak,meningitis,mucoceleformation, nasalsynechia,septalperforation(priortoposteriorseptectomy),internalnasalvalvefailure, epistaxis,andolfactoryalterations.
Results:Thestudyassessed41patientsundergoingsurgery.Ofthese,35hadpituitary adeno-mas (macro- ormicro-adenomas; sellar and suprasellarextension), three hadmeningiomas (two tuberculum sellae and one olfactory groove), two had craniopharyngiomas, and one hadanintracranialabscess.Thecomplicationswerecerebrospinalfluidleak(threepatients; 7.3%),meningitis(threepatients;7.3%),nasalfossasynechia(eightpatients;19.5%),internal nasal valvefailure(sixpatients;14.6%),andcomplaints ofworsening ofthesenseofsmell
夽 Pleasecitethisarticleas:DolciRL,MiyakeMM,TatenoDA,Canc¸adoNA,CamposCA,SantosAR,etal.Postoperativeotorhinolaryngologic
complicationsintransnasalendoscopicsurgerytoaccesstheskullbase.BrazJOtorhinolaryngol.2017;83:349---55. ∗Correspondingauthor.
E-mail:[email protected](R.L.Dolci).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.020
(16patients;39%).Theolfactorytestshowedanosmiaorhyposmiaintenpatients(24.3%).No patienthadmucocele,epistaxis,orseptalperforation.
Conclusion:Theuseofthenasoseptalflaphasrevolutionizedendoscopicskullbasesurgery, makingtheproceduresmoreeffectiveandwithlowermorbiditycomparedtothetraditional route. However, althoughmainly transientnasal morbidities wereobserved,insome cases, permanent hyposmia andanosmia resulted. An improvementinthis techniqueis therefore necessarytoprovideabetterqualityoflifeforthepatient,reducingpotentialcomplications. © 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Retalhonasoseptal; Endonasal;
Endoscópica; Basedocrânio; Complicac¸ões; Otorrinolaringológicas
Complicac¸õespós-operatóriasotorrinolaringológicasemcirurgiasendoscópicas transnasaisparaacessoabasedocrânio
Resumo
Introduc¸ão:Ograndecrescimentononúmerodecirurgiasendoscópicastransnasaisparaabase docrânioocorreuapartirdeummaiorconhecimentoanatômicodaregião;dodesenvolvimento demateriaiseinstrumentaisespecíficose,principalmente,apósautilizac¸ãodoretalho nasosep-talcomoumabarreiraentreotratosinusal(cavidadecontaminada)eoespac¸osubaracnóideo (áreaestéril),comreduc¸ãodegrandesriscosdecontaminac¸ão.
Objetivo:Avaliarascomplicac¸õesotorrinolaringológicasnospacientessubmetidosàcirurgia endoscópicadabasedocrânio,naqualfoiutilizadooretalhonasoseptal.
Método: Estudoretrospectivo,noqualforamavaliadosospacientessubmetidosàcirurgiada basedocrânioporviaendoscópicacomrealizac¸ãodoretalhonasoseptal,quantoàpresenc¸ano pósoperatóriodasseguintescomplicac¸ões:fístulaliquórica,meningite,formac¸ãodemucocele, sinéquianasal,perfurac¸ãoseptal(anterioràseptectomiaposterior),insuficiênciadeválvula nasalinterna,epistaxeealterac¸ãoolfatória.
Resultados: Foramavaliados41pacientessubmetidosàcirurgia.Destes,35eramportadoresde adenomashipofisários(macrooumicroadenomas;selareseextensãosupraselar),três menin-giomas(doisdetubérculoselareumdagoteiraolfatória),doiscraniofaringiomaseumabscesso intracraniano. Ascomplicac¸ões observadasforam: fístulaliquórica (trêspacientes ---7,3%), meningite(trêspacientes---7,3%),sinéquiaemfossanasal(oitopacientes---19,5%), insuficiên-ciadeválvulanasalinterna(seispacientes---14,6%),equeixadepioradoolfato(16pacientes ---39%).Otesteolfatórioevidenciouanosmia ouhiposmia em10pacientes(24,3%).Nenhum pacienteapresentoumucocele,epistaxeouperfurac¸ãoseptal.
Conclusão:Ousodoretalho nasoseptalproporcionouuma revoluc¸ãonacirurgia dabasedo crânioporviaendoscópicatornandoosprocedimentosmaiseficazesecombaixamorbidade, comparandocomaviatradicional.Porém,passouaocasionarmorbidadesnasaisprincipalmente transitórias, mas em algunscasos permanentes,como hiposmia e anosmia. Assim,torna-se necessárioumaperfeic¸oamentodestatécnicaparaproporcionarumamelhorianaqualidadede vidadopacienteediminuirpossíveiscomplicac¸ões.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Thestudies by JhoandCarrau inthe1990sdemonstrated
that the endoscopic sinonasal route allowed for direct
access to various skull base disorders, including tumors
of the pituitary gland. This was a very significant step
in the development of endoscopic skull base surgery. In
this new field, several studies have shown the
numer-ous possibilities of treatment of diseases in that region;
together with recent advances in anatomical knowledge
and surgical techniques, they have fostered the
expan-sion of transnasal endoscopic skull base surgery. As a
result of improved optics, hemostatic equipment,
spe-cificclamps,microdebriders,diagnostictests,andtheuse
of neuronavigation, therewas an improvement in
techni-cal efficiency, reducing morbidity, mortality and surgical
time.1---6
Intheearlystagesoftheendonasalendoscopicapproach
totheskullbase,themain criticismwasthehighrates of
mortalitycomparedtothetraditionalroute.Thevalidation
of this technique occurred after the development of the
nasoseptal flap,which helped create an effective barrier
between the sinonasal tractand the subarachnoid space,
avoidingthecontactofaninfectedcavitywithasterilearea
atgreatriskofinfection.7,8
Thereareseveralstudiesintheliteratureontheclosure
ofskullbasedefectsusingnasoseptalflapinawidevariety
of diseases and skullbase locations7---10; few studies have
demonstrated thepotential morbidities and howtoavoid
them.Thus,thisstudyaimedtoevaluatepossiblesinonasal
complicationsin patientsundergoingskullbasesurgeryby
transnasalendoscopy.
Methods
Datacollected frommedicalrecordsofpatients operated
by the skull base team of this institution, composed of
otorhinolaryngologistsandneurosurgeons,were
retrospec-tivelyassessed.Allpatientsincludedinthestudyunderwent
endonasalendoscopicsurgicalprocedures,with
transsphe-noidal, transplanum, or transcribriform approach to the
baseof theskullanduseofnasoseptalflap,from
Novem-ber 2012 to December2014, and with a minimumof 100
daysoffollow-upaftersurgery.Patientswhodidnotundergo
theendonasalaccessexclusivelytotheskullbase,aswell
asthosein which thenasoseptal flapwasnot used,were
excluded. Patients were evaluated for demographic data
andforthepresenceofCSFleak,meningitis,mucocele
for-mation,olfactorychanges,nasalsynechiae,epistaxis, and
septal perforation in the postoperative period. The data
collectedreferredtothelastpatientvisitandwerebased
onreportsofcomplaintsfrompatients,otorhinolaryngology
physical examination, nasal endoscopy, and imaging tests
(computedtomography[CT]andmagneticresonance
imag-ing [MRI]) for the diagnosis of mucoceles. Patients with
olfactoryalterationscomplaintsweresubmittedtothesmell
test (Connecticut Chemosensory Clinical Research Center
Test[CCCRC]).ThestudywasapprovedbytheEthics
Com-mittee(CAAE---34487814.8.0000.5479).
Results
Forty-fivepatients wereoperated fromNovember 2012to
December 2014, of whom 41 met the inclusion criteria,
undergoingendoscopicskullbase surgery:28 females and
13 males. The mean age was46 years (15---79 years) and
meanfollow-uptimewas12.2months(3.5---30months).Four
patients wereexcluded due tonon-use of nasoseptalflap
(reoperation)orlosstofollow-up.
Thirty-five patients had pituitary adenomas,three had
meningiomas (two tuberculum sellae and one olfactory
groove),twohadcraniopharyngiomas,andonehadabrain
abscess(Table1).
For educational purposes, complications were divided
according to their location (as previously described by
Soudry et al.11), the integrity of the nasoseptal flap, the
receivingarea(skullbase),andthedonorarea(septumand
nasalmucosa;Table2;Fig.1).
Table1 Casesofendonasalendoscopicsurgeryoftheskull base.
Pathology Number(%)
Adenomas 35(85.3)
Multi-producer 7(17)
Non-producer 10(24.4)
ACTH 11(26.8)
GH 6(14.6)
FSH 1(2.4)
Meningioma 3(7.3)
Tuberculumsellae 2(4.8)
Olfactorygroove 1(2.4)
Craniopharyngioma 2(4.8)
Brainabscess 1(2.4)
Forty-one cases ofendoscopic endonasalsurgery ofthe skull basewereperformedwithnasoseptalflapcreation.
Integrityoftheflap
Therewere nocomplications directly related tothe flap.
In all patients, the flap had good postoperative viability
Table2 Complicationsfromendonasalendoscopicsurgery oftheskullbase.
Number(%)
Complicationsofthedonorarea
Synechia 8(19.5)
Noclinicalrepercussion 4(9.7)
Withclinicalrepercussion 4(9.7)
Nasalvalveinsufficiency 7(17)
Associatedwithsynechia 4(9.7)
Associatedwithseptaldeviation 2(4.8) Nasalwingcollapsepriortosurgery 1(2.4) Complaintofolfactoryalteration 16(39)
Anosmia 4(9.7)
Severehyposmia 3(7.3)
Moderatehyposmia 2(4.8)
Mildhyposmia 1(2.4)
Normosmia 4(9.7)
Didnotperformthetest 2(4.8)
Mucocele 0(0)
SeptalPerforation 0(0)
Complicationsofthereceptorarea
Cerebrospinalfluidleaks 3(7.3)
Meningitis 3(7.3)
Flapintegrity NC
Nasal crusts
A
B
C
D
Nasal crusts Middle
turbinate
Inferior
turbinate turbinateInferior
Inferior turbinate
Middle turbinate
SE Rem. nasal
septum Inferior turbinate
Inferior turbinate
Nasoseptal flap Vomer
Vomer
Sinus floor
Nasal synechia
Nasal septum
Figure1 (A)and(B)Nasofibroscopyattwoweekspostoperativeinpatientswhounderwenttranssphenoidalsurgeryforpituitary adenoma,awidenumberofcrusts throughoutthenasalcavitycanbeobserved.Itisnotpossibletoobservethesphenoidsinus andsellarregions.Nomanipulationisperformedinthesurgicalareaduetotheriskofmanipulationofnasoseptalflap,whichcan resultinacerebrospinalfluidleak.(C)Therightnasalfossasynechiacanbeobservedbetweentheinferiorturbinateandthenasal septum,inthepostoperativeperiodofthreemonths;(D)sixmonthspostoperativeofpituitaryadenoma,inwhichvariousanatomical structurescanbeidentified,includingtherightmiddleturbinateasthenasoseptalflapwasmadetotheleft(thebeginningofflap withinthesphenoidsinusfloorcanbeobserved),withremovaloftheipsilateralmiddleturbinateasthepatienthadasignificant septaldeviationtotheright.Itisalsopossibletoobservethesphenoidregionwideopenandcompletelycoveredbytheflap;itis possibletoidentifytheupperportionofthenasalseptum,asthenasalseptumwasremoved(preservingtheareaK,Keystone,and 1cmfromthenasalseptumsuperiorly).
(nonecrosis).Therewerenopedicletransectionsduringits constructioninsurgery.
Receivingarea
Three cases (7.3%) of CSF leaks were observed, two
in patients undergoing surgery for adrenocorticotropic
hormone (ACTH)-producing pituitary adenomas (Cushing’s
syndrome)andonefortreatmentofolfactorygroove menin-gioma.AcraniotomywasperformedforthetreatmentofCSF leakinbothpatientswithpituitaryadenoma.Inthepatient
witholfactory groove meningioma, a pericranial flap was
made.Afterthese procedures,the threepatientsshowed
improvementof CSFleak.These samethreepatients also
hadmeningitis,andweretreatedwithintravenous
antibi-otics.Allshowedsatisfactoryprogressaftertreatmentwith antibiotics,withoutsequelae.
Donorarea
Alterationsin thenasalfossa (synechiae,valvefailure,or both)wereobservedin11(26.8%)patients,whowereasked abouttheperceptionofnasalobstructionincomparisonwith
thepreoperativeperiod:fivereportedworseningin breath-ing,fivereportednodifference,andonereportedimproved breathing.Thispatienthadhadaseverenasalseptum
devi-ationprior tosurgery andunderwentaseptoplastyat the
sameoperationperiod.Regardingthechangesofthenasal
cavity, eight(19.5%)patientshadsynechiaandsix(14.6%) patientsdevelopedchangesintheinternalnasalvalve;three
patients had both. Thus, amongthe 41 patients studied,
five reportedworsening in breathing(12.1%). No patients
presentedseptalperforation,epistaxis,ormucocele. Regardingolfactoryfunction,16patients(39%)reported
post-operative complaints(after over 100 daysof
follow-up) and were subjected to the CCCRC (Tables 3 and 4).
Of these, ten (24.3%) had some degree of hyposmia or
anosmia (two also showed deviation of the septum or
synechia),four(9.7%)had normosmia,andtwo(4.8%)did
notundergothetest(onepatientdue tolosstofollow-up
andtheotherduetocognitiveimpairmentthatprevented
theapplicationoftheCCCRC).Aboutthetenpatientsthat
hadolfactionalteration,theaccessroutewere:
transsphe-noidal in eight patients (four multi-producer adenomas,
one GH,oneACTH,and onenon-producer,aswell asone
craniopharyngioma),andthetranscribriformapproachwas
Table3 Complicationsfromendonasalendoscopicsurgeryoftheskullbase,perdisease.
Olfactory alterations
Cerebrospinal fluidleak
Meningitis Nasal synechia
INVF P/M/E
Adenoma 7 2 2 7 5
Craniopharyngioma 1
Tuberculumsellaemeningioma
Olfactorygroovemeningioma 1 1 1
Intracranialabscess 1 1 1
Total 10 3 3 8 6 0
Whencomplicationsweredividedbysurgicalaccess,thefollowingwereobserved:inthreecases(7.3%),cerebrospinalfluidleakand meningitis;inthetwoabovementionedcomplications,twopatientsunderwentsurgeryforadrenocorticotropichormone(ACTH)-producer pituitaryadenomas(Cushing’ssyndrome)andonefortreatmentofolfactorygroovemeningioma.Amongthechangesofthenasalcavity: ineight(19.5%)patients,synechiawasobserved,seveninpatientsundergoingsurgeryforpituitaryadenoma,andoneforintracranial abscess.Six(14.6%)patientsdevelopedchangesintheinternalnasalvalve,fivepatientsundergoingsurgeryforpituitaryadenoma,and oneforintracranialabscess(threepatientsshowedsynechiaandalterationoftheinternalnasalvalve).Themostcommoncomplication inthisstudywasa changeinolfaction,observedintenpatients,anddocumented bytheolfactorytestConnecticut Chemosensory Clinical ResearchCenterTest[CCCRC].Of these tenpatients,seven patientsunderwentsurgeryfor pituitary adenoma,one for a craniopharyngioma,onebecauseofanintracranialabscess,andoneforanolfactorygroovemeningioma.Fourpatientswhoraisedthe complaintpostoperativelywereexaminedandwerefoundnormosmic.Twopatientswiththecomplaintdidnotundergotheexamination; onewaslosttofollow-upandanotherduetocognitiveimpairment.Nopatientsdevelopedseptalperforation,epistaxis,ormucocele. INVF,internalnasalvalvefailure;P/M/E,septalperforation/mucocele/epistaxis.
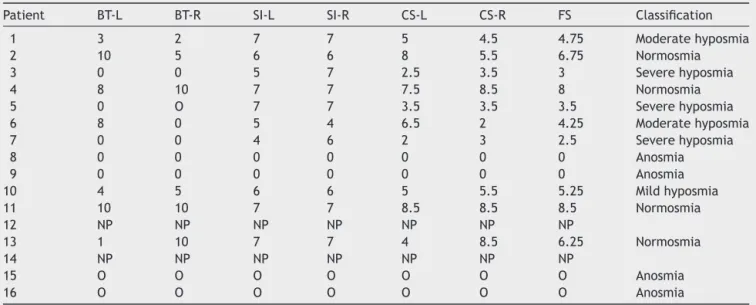
Table4 ResultoftheConnecticutChemosensoryClinicalResearchCenterolfactorytestaftersurgicalapproach.
Patient BT-L BT-R SI-L SI-R CS-L CS-R FS Classification
1 3 2 7 7 5 4.5 4.75 Moderatehyposmia
2 10 5 6 6 8 5.5 6.75 Normosmia
3 0 0 5 7 2.5 3.5 3 Severehyposmia
4 8 10 7 7 7.5 8.5 8 Normosmia
5 0 O 7 7 3.5 3.5 3.5 Severehyposmia
6 8 0 5 4 6.5 2 4.25 Moderatehyposmia
7 0 0 4 6 2 3 2.5 Severehyposmia
8 0 0 0 0 0 0 0 Anosmia
9 0 0 0 0 0 0 0 Anosmia
10 4 5 6 6 5 5.5 5.25 Mildhyposmia
11 10 10 7 7 8.5 8.5 8.5 Normosmia
12 NP NP NP NP NP NP NP
13 1 10 7 7 4 8.5 6.25 Normosmia
14 NP NP NP NP NP NP NP
15 O O O O O O O Anosmia
16 O O O O O O O Anosmia
Thistestconsistsoftwoparts,consistingoftheolfactorythresholdofresearchandsmellidentification;theolfactoryclassificationis performedbyanalyzing:(1)thecombinedscorebetweenthethresholdtest(butanol)andsmellidentification,whichcorrespondsto thearithmeticmeanofbothscores.Thereafter,acombinedscorewasobtainedforeachnasalcavityseparately.(2)TheCombined ScoreIndex,whichisthearithmeticmeanofthecombinedscoresofeachnasalcavity.Thus,accordingtothecombinedscoreofthe indexesobtained,thefollowingvalueswereconsideredfortheclassificationoftheolfactorystatusofeachpatient:6.0---8.5:normosmia; 5.0---5.75:mildhyposmia;4.0---4.75:moderatehyposmia;2.0---3.75:severehyposmia;and0---1.75:anosmia.R,right;L,left;CS,combined score;FS,finalscore;SI,smellidentification;BT,butanolthreshold;NP,notperformed.
groove meningioma). The patientwho underwent surgery
for brainabscessshowed moderatehyposmia; thepatient
who underwentthe procedure for treatment of olfactory
groovemeningiomapresentedanosmia.
Discussion
The surgical approachtotheskullbase via theendonasal
endoscopicaccessisalreadyconsideredtherouteofchoice
forthetreatmentofvariousdisorders,particularlypituitary
adenomas.However,theneedtomanipulatethenasal
cav-ityandtheparanasalsinuses,aswellasthepreparationof theflapnasoseptal,mayresultinsinonasalcomplications.
The establishment of a multidisciplinary team including
neurosurgeonsandotorhinolaryngologistshasproventobe
essentialinthesurgicalandpostoperativemanagementof
thesepatients, andhasbeenadopted inthemain centers
worldwide.12 This study is one of first in Brazil toreport
endoscopicapproachtotheskullbase andtheexperience
ofatertiarypublichospital.
In the present study, no complications related to flap
integrity were observed, as flap construction was
stan-dardizedtotheright,withvariationwhenanasalseptum
deviationhindereditsconstructiontotheright;thisreduced
thechances of complications in makingthe flap. Another
factor that helped flap viability was the maintenance of
apedicleby performinga lowerandupperincisioninthe
choanalarch, witha distanceof atleast1---1.5cm,asthe
lowerincisionismadeinthelowerarchofthechoanaand
thetopincisionjustbelowthesphenoidostium.
Beforetheadventofthenasoseptalflap,complications
arising from the receiving area were a limiting factor
due to a high CSF leak rate, which ranged from 40% to
50% in the endoscopic approach. These rates were
con-sideredunacceptableduetohighmorbidityandmortality,
and the main criticism was that there was a
tradi-tionalandrenownedaccessroute withlowercomplication
rates.8,11,13,14Currently,thepercentageofpostoperativeCSF
leak is approximately 5%.7,15 In the present study, a rate
of 7.3% was observed; however, this rate included cases
ofexpandedendoscopicapproach(threemeningiomas[two
tuberculumsellae andone olfactorygroove meningioma],
two craniopharyngiomas, and one brain abscess), and a
CSFleakwasobservedintheolfactorygroovemeningioma.
Ifonly the pituitary surgeries are considered, a CSF leak
rateof5.7%wasobserved.Whentheexpandedendoscopic
approachtotheskullbaseisperformed,CSFleakratesare
higher,asthereishighCSFflow,leadingtoagreater
propen-sityofleaks.Ratesvaryfrom10%to16.1%.9,16,17Inthisstudy,
analyzingonlytheexpandedaccess,theCSFleakratewas
16.6%.
Thehighestratesofcomplicationsarisefromthedonor
area. Olfactory complications have been previously
stud-ied;somestudieshaveshownadirectrelationshipbetween
the construction of nasoseptal flap and possible
worsen-ing of symptoms, withrates ranging from 8% to46%.18---23
The present study diagnosed anosmia or some degree of
hyposmia(mild tosevere) inten patients(24.4%) through
CCCRC.Ifbothpatientswitholfactorycomplaintwhowere
nottested were diagnosed, thisratio would reach29.2%.
Unlikesomestudies thatincluded onlypatients whowere
operatedonusingthetranssphenoidalaccess,thepresent
sampleincludedtwopatientsinwhomthetranscribriform
accesswasused,whichhasaworseolfactoryprognosis.
Severalfactorsarerelatedtoolfactoryalterations.Inthe
firstmonth,thepresenceofcrustsinthenasalcavity
result-ingfromsurgicalproceduresplayanimportantroleandcan
persistfor30---100days.20,24,25However,thesecrustsoccur
transiently;withthe correct cleaning ofthe nasal cavity,
therecanbeasignificantimprovementinthesenseofsmell.
Inaddition,otherfactorsthatcanminimizeolfactory
com-plaintsarethepreservationof2cmfromtheupperregion
ofthenasalseptummucosaduringthemakingoftheflap,
asthisregionisrichinolfactoryneuroepithelium,andthe
preservationofthemiddleandupperturbinates,structures
withthepresenceofolfactoryfimbriae.
Anothercomplication arisingfromthedonorarea,and
oneof themost common,is nasalsynechia,which occurs
between the septum and structures of the lateral nasal
wall,thatcancauseworseningofnasalflow.Inthepresent
study,eightcasesofpostoperativesynechiae(19.5%)were
identified,a percentagesimilartoprevious reportsin the
literature,whichrangedfrom9%to20%.21,24Inthepresent
authors’experience,themaincausesofsynechiaearethe
lackofpropernasallavagewithsalineinthepostoperative
periodandfailuretoplacethenasalsplint,exposingareas
ofbloodyseptalmucosa.
Internalnasalvalvefailureisalsoacommon
complica-tion,whichwasobservedinsix(14%)ofthecasesstudied,
fourduetoadhesionsandtwoduetoresidualseptal
devia-tions.Anotherpossiblecauseofinternalnasalvalvefailure
is called ‘alar sill burn’ due to synechia of the lower
lateral cartilage and the nasal septum. This is reported
in 5% of patients following creation of the upper
inci-sionof nasoseptalflapwithelectrocauteryintheanterior
portion of the nasal septum, and can be avoided by
pla-cingthenasalsplint.24 Inthepresentstudy,nocaseswere
observed.
Althoughrates of septalperforation ofup to14%have
been described,11 nopatientinthepresent studyhadthis
complication.Thecreationofthereverseflap,coveringthe
remainingcartilaginousseptumfromwherenasoseptalflap
wasremoved,isroutinelyperformedinthisservice,andthe
authorsbelieveittobeveryimportantforproperhealing.26
Inthepresentstudy,nocasesofmucocelewereobserved;
thishasbeenreportedinprevious studiesbetween0%and
50%,27---31 being more frequent in children due to
incom-plete formation of the frontal sinus in cases of accessto
theanteriorskullbase.31,32Theauthorsbelievethatthe
fol-lowing steps are critical tominimize the development of
mucocele,especiallyinthesphenoid:completeremovalof
the mucosa andall septae present in the sphenoidsinus,
making it easier for theflap toadhere; mucosal
denuda-tionintheareaaroundthedefectoftheskullbase;wide
sphenoidectomy,thus reducingtheriskofblockage of
air-flow;andavoidingoverlapbetweenflapsincasesofdouble
flap.29,33 In the present study,no cases of epistaxis were
observedthatrequiredmedicalorsurgicalintervention,as
all patientsweremaintainedpostoperativelywitha Foley
catheterandnasalsplintforthreetosevendays,resulting
inlesschanceofbleeding.
The study limitations relate to the fact that it was
performedretrospectively.Thereisaneedforfurther
stud-iesassociatingendoscopicskullbase surgerywithpossible
olfactory alterations. The smell test was performed only
postoperativelyandinpatientswithcomplaints.
Currently,thistechniqueiswellestablishedasthebest
waytoaccesstheskullbase.Studiessuchasthepresent
indi-cate theneed for furthertechnicalimprovement toavoid
anycomplicationsandthusprovidehealingandbetter
well-beingforpatients.
Conclusion
Thetransnasalendoscopictechniqueisnolongeranovelty
and has become a reality, especially after the advent of
nasoseptalflap.However,itsuseleadstonasalalterations
that are usually transitory, but sometimes permanent.
Among them are the olfactory alterations, which cause
a decrease in the patient’s quality of life. Based on the
surgicaltechniquesothatthepatientcanbebenefitedby
avoidingpostoperativecomplaintsandcomplications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ElangovanC,SinghSP,GardnerP,SnydermanC,Tyler-Kabara EC,HabeychM,etal.Intraoperativeneurophysiological moni-toringduringendoscopicendonasalsurgeryforpediatricskull basetumors.JNeurosurgPediatr.2015;30:1---9.
2.Kassam A, Snyderman CH, Carrau RL, Gardner P, Mintz A. Endoneurosurgicalhemostasistechniques:lessonslearnedfrom 400cases.NeurosurgFocus.2005;19:E7.
3.Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL. Expandedendonasalapproach:the rostrocaudalaxis. PartI. Cristagallitothesellaturcica.NeurosurgFocus.2005;19:E3. 4.Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL.
Expandedendonasalapproach:therostrocaudalaxis.PartII. Posteriorclinoidstotheforamenmagnum.NeurosurgFocus. 2005;19:E4.
5.PalmerJN,KennedyDW.Historicalperspectiveonimage-guided sinussurgery.OtolaryngolClin.2005;38:419---28.
6.SnydermanCH,PantH,CarrauRL,PrevedelloD,GardnerP, Kas-samAB.Whatarethelimitsofendoscopicsinussurgery?:the expandedendonasalapproachto theskullbase.KeioJMed. 2009;58:152---60.
7.HadadG, BassagasteguyL,CarrauRL, MatazaJC,KassamA, SnydermanCH, etal.Anovelreconstructive techniqueafter endoscopicexpandedendonasalapproaches:vascularpedicle nasoseptalflap.Laryngoscope.2006;116:1882---6.
8.KassamAB, CarrauRL,SnydermanCH, Thomas A,Vescan A, Prevedello D, et al. Endoscopic reconstruction of the cra-nial base using a pedicled nasoseptal flap. Neurosurgery. 2008;63:ONS44---53.
9.EloyJA,ShuklaPA,Choudhry OJ,SinghR,LiuJK.Challenges andsurgicalnuancesinreconstructionoflargeplanum sphe-noidaletuberculumsellaedefectsafterendoscopicendonasal resection of parasellar skull base tumors. Laryngoscope. 2013;123:1353---60.
10.HarveyRJ,ParmarP,SacksR,ZanationAM.Endoscopicskull basereconstructionoflargeduraldefects:asystematicreview ofpublishedevidence.Laryngoscope.2012;122:452---9. 11.SoudryE,PsaltisAJ,LeeKH,VaezafsharR,NayakJV,HwangPH.
Complicationsassociatedwiththepediclednasoseptalflapfor skullbasereconstruction.Laryngoscope.2015;125:80---5. 12.SnydermanC,CarrauR,KassamA.Whoistheskullbasesurgeon
ofthefuture?SkullBase.2007;17:353---5.
13.LiuJK, SchmidtRF, Choudhry OJ, ShuklaPA,Eloy JA. Surgi-calnuancesfor nasoseptalflapreconstructionofcranialbase defectswith high-flow cerebrospinal fluid leaks after endo-scopicskullbasesurgery.NeurosurgFocus.2012;32:E7. 14.Pinheiro-NetoCD,SnydermanCH.Nasoseptalflap.Adv
Otorhi-nolaryngol.2013;74:42---55.
15.Gardner PA,Kassam AB,Rothfus WE, SnydermanCH, Carrau RL. Preoperative and intraoperative imaging for endoscopic endonasal approaches to the skull base. Otolaryngol Clin. 2008;41:215---30,vii.
16.KoutourousiouM,Fernandez-MirandaJC,StefkoST,WangEW, SnydermanCH,GardnerPA.Endoscopicendonasalsurgeryfor suprasellarmeningiomas:experiencewith75patients.J Neu-rosurg.2014;120:1326---39.
17.Laufer I, Anand VK, Schwartz TH. Endoscopic endonasal extended transsphenoidal, transplanum transtuberculum approach for resection of suprasellar lesions. J Neurosurg. 2007;106:400---6.
18.AwadAJ,MohyeldinA,El-SayedIH,AghiMK.Sinonasalmorbidity followingendoscopicendonasalskullbasesurgery.ClinNeurol Neurosurg.2015;130:162---7.
19.deAlmeidaJR,SnydermanCH,GardnerPA,CarrauRL,Vescan AD.Nasalmorbidityfollowingendoscopicskullbasesurgery:a prospectivecohortstudy.HeadNeck.2011;33:547---51. 20.GallagherMJ,DurnfordAJ,WahabSS,NairS,RokadeA,Mathad
N. Patient-reported nasal morbidity following endoscopic endonasalskullbasesurgery.BrJNeurosurg.2014;28:622---5. 21.KorenI,HadarT,RappaportZH,YanivE.Endoscopictransnasal
transsphenoidalmicrosurgeryversusthesublabialapproachfor the treatmentofpituitary tumors: endonasalcomplications. Laryngoscope.1999;109:1838---40.
22.CavelO,AbergelA,MargalitN,FlissDM,GilZ.Qualityoflife followingendoscopicresectionofskullbasetumors. JNeurol SurgBSkullBase.2012;73:112---6.
23.Sowerby LJ, Gross M, Broad R, Wright ED. Olfactory and sinonasal outcomes in endoscopic transsphenoidal skull-base surgery.IntForumAllergyRhinol.2013;3:217---20.
24.PantH,BhatkiAM,SnydermanCH,VescanAD,CarrauRL, Gard-ner P, et al. Quality of life following endonasal skull base surgery.SkullBase.2010;20:35---40.
25.AlobidI,EnsenatJ,Marino-SanchezF,deNotarisM,CentellasS, MullolJ,etal.Impairmentofolfactionandmucociliary clear-ance after expanded endonasal approach using vascularized septalflapreconstructionforskullbasetumors.Neurosurgery. 2013;72:540---6.
26.Caicedo-Granados E,CarrauR,SnydermanCH, PrevedelloD, Fernandez-MirandaJ,GardnerP,etal.Reverserotationflapfor reconstructionofdonorsiteaftervascularpediclednasoseptal flapinskullbasesurgery.Laryngoscope.2010;120:1550---2. 27.BleierBS,WangEW,VandergriftWA3rd,SchlosserRJ.Mucocele
rateafterendoscopicskullbasereconstructionusing vascular-izedpedicledflaps.AmJRhinolAllergy.2011;25:186---7. 28.Di Rocco F, Couloigner V, Dastoli P, Sainte-Rose C, Zerah
M, Roger G. Treatment of anterior skull base defects by a transnasalendoscopicapproachinchildren.JNeurosurg Pedi-atr.2010;6:459---63.
29.HusainQ,SanghviS,KovalerchikO,ShuklaPA,ChoudhryOJ,Liu JK,etal.Assessmentofmucoceleformationafterendoscopic nasoseptalflapreconstructionofskullbasedefects.Allergy Rhi-nol.2013;4:e27---31.
30.NyquistGG,AnandVK,SinghA,SchwartzTH.Janusflap: bilat-eral nasoseptal flaps for anterior skull base reconstruction. OtolaryngolHeadNeckSurg.2010;142:327---31.
31.Verillaud B, Genty E, Leboulanger N, Zerah M, Garabedian EN, RogerG. Mucoceleaftertransnasal endoscopic repairof traumaticanteriorskull basefistulainchildren.IntJPediatr Otorhinolaryngol.2011;75:1137---42.