SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Reverse
shoulder
arthroplasty:
clinical
results
and
quality
of
life
evaluation
夽
Arnaldo
Amado
Ferreira
Neto
a,
Eduardo
Angeli
Malavolta
a,
Jorge
Henrique
Assunc¸ão
a,∗,
Evelinda
Marramon
Trindade
b,
Mauro
Emilio
Conforto
Gracitelli
aaUniversidadedeSãoPaulo,FaculdadedeMedicina,InstitutodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
bSecretariadaSaúdedoEstadodeSãoPaulo,RedePaulistadeAvaliac¸ãoemTecnologiadeSaúde,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14March2016 Accepted20June2016 Availableonline4May2017
Keywords:
Arthroplasty,replacement Jointdiseases
Osteoarthritis Rotatorcuff
a
b
s
t
r
a
c
t
Objective:Toevaluatetheclinicalandradiologicalresultsandtheimpactonqualityoflife ofthereverseshoulderarthroplasty.
Methods:Retrospective case series evaluating 13 patients undergoing reverse shoulder arthroplastywithatleasttwoyearsofclinicalfollow-up.Clinicalevaluationwasperformed beforeandaftersurgerywiththeASESandVASscalesandhand-mouth,hand-neck,and hand-headfunctionaltests.QualityoflifewasmeasuredwiththeSF-12questionnaire.The rateofcomplicationsandradiographicpostoperativefindingswererecorded.
Results:Thepatientsimprovedfrom23.1±15to82.7±15accordingtoASESscale(p<0.001). ThephysicalcomponentoftheSF-12increasedfrom31.7±6.9to47.1±8.6(p<0.001),while theemotionalincreasedfrom48±12.3to55.5±7.5(p=0.061).Thepainreducedfrom7.9 to1accordingtotheVAS(p=0.002).Theperformanceon thehand-mouth,hand-neck, andhand-headfunctionaltestsshowedsignificantimprovement(p=0.039,p<0.001and
p<0.001,respectively).Complicationsoccurredin15%ofpatientsandnotching,in31%.
Conclusion:Reverseshoulderarthroplastyledtoasignificantclinicalimprovementaccording totheASESandVASscales.Thequalityoflifehasimprovedaccordingtothephysicalaspect oftheSF-12,andshowedatrendofimprovementintheemotionalaspect.Thecomplication ratewas15%,andnotchingoccurredin31%.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheUniversidadedeSãoPaulo,FaculdadedeMedicina,InstitutodeOrtopediaeTraumatologia,GrupodeOmbro eCotovelo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.H.Assunc¸ão). http://dx.doi.org/10.1016/j.rboe.2017.04.007
Artroplastia
reversa
do
ombro:
avaliac¸ão
dos
resultados
clínicos
e
da
qualidade
de
vida
Palavras-chave:
Artroplastiadesubstituic¸ão Artropatias
Osteoartrose Manguitorotador
r
e
s
u
m
o
Objetivo: Avaliarosresultadosclínicoseradiológicoseoimpactonaqualidadedevidada artroplastiareversadoombro.
Métodos: Sériedecasosretrospectivaqueavaliou13pacientessubmetidosàartroplastia reversadoombrocomseguimentoclínicomínimodedoisanos.Foifeitaavaliac¸ãoclínica anteseapósacirurgiacomasescalasdaAmericanShoulderandElbowSurgeons(ASES)e escalavisualanalógica(EVA)easmanobrasfuncionaismão-boca,mão-nucaemão-cabec¸a. Aqualidadedevidafoiaferidacomoquestionário12-ItemShort-FormHealthSurvey(SF-12). Registramosoíndicedecomplicac¸õeseoaspectoradiográficopós-operatório.
Resultados: Ospacientesevoluíramde23,1±15para82,7±15pelaescaladaASES(p<0,001). OcomponentefísicodoSF-12passoude31,7±6,9para47,1±8,6(p<0,001)enquantoo emo-cionalde48±12,3para55,5±7,5(p=0,061).Adorregrediude7,9para1deacordocoma EVA(p=0,002).Asmanobrasfuncionaismão-boca,mão-nucaemão-cabec¸aapresentaram melhorias significativas (p=0,039, p<0,001 e p<0,001, respectivamente). Complicac¸ões ocorreramem15%dospacientesenotching,em31%.
Conclusão: Os pacientessubmetidosà artroplastiareversa doombrotiveram melhoria significativadeacordocomasescalasdaASESeEVA.Aqualidadedevidamelhorou signi-ficativamentedeacordocomoaspectofísicodoSF-12edemonstroutendênciademelhoria noaspectoemocional.Oíndicedecomplicac¸õesfoide15%enotchingocorreuem31%.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Reverse shoulderarthroplasty technique wasdeveloped by Paul Grammont in 1985 in France1; the first case series
was published in the following decade.2,3 Initially
devel-oped for the treatment of rotator cuff arthropathy,4–8 its
use extends to cases of primary anatomical arthroplasty revisions,9,10 complex fractures,11–13 sequelae of proximal
humeral fractures,14,15 and inflammatory arthroplasties.16
FromitsoriginalrestrictiontoEuropeanuse,itwasapproved bytheFoodandDrugAdministrationintheUnitedStatesin 2003andsincethenhasbeenwidelyusedinthatcountry.17
Reverse arthroplasty has biomechanical characteristics thatimprovefunctionofthedeltoidmuscleandcompensate adysfunctionalrotatorcuff.18Itsclinicalresultsaresuperior
tothoseofanatomictotalshoulderarthroplastiesinthe treat-mentofrotatorcuffarthropathy.4
Currently,reversearthroplastyhasbeenapprovedbythe BrazilianNationalSanitarySurveillance Agencyandispart ofthe therapeuticarsenaloftheSupplementalHealth Sys-tem.However,theBrazilianUnifiedHealthSystem(Sistema ÚnicodeSaúde[SUS])doesnotlisttheimplantwithinits pro-cedures,andmostpublichospitalsareunabletoadequately treatpatientswithindicationfortheuseofthisimplant.The nationalliteraturefeaturesonlytwostudiesonthesubject5,8;
bothevidencedclinicalimprovementwithtreatment. AftercontactingtheHealthSecretariatoftheStateofSão Pauloandanexplainingtheissue,theauthorswereinstructed toconduct furtherstudieson thesubject inanattempt to objectively expose the problem and, consequently, aid in
theprovisionofreversearthroplastyinspecializedshoulder surgerycenters.Thisisthefirstinaseriesofarticlestobe developedbythisgroup.Thegoalistoevaluatetheclinical and radiologicalresultsofreverse shoulderarthroplasty,as wellasitsimpactonqualityoflife.
Methods
Thiswasaretrospectivecaseseries.Patientswhounderwent reverseshoulderarthroplasty,withaminimumoftwoyears ofclinicalfollow-up,wereassessed.Thestudycomprised sur-geriesperformeduntilDecember2013.Patientssubmittedto other typesofarthroplastieswere notincluded. Thisstudy wasapprovedbytheInstitutionReviewBoardunderNo.1103.
Indicationsforreversearthroplastywere:
- Rotator cuff arthropathy; extensive and irreparable rup-tureoftherotatorcuff;primaryorsecondaryglenohumeral arthrosis,associatedwithirreparablerupture ofthe rota-torcuff;sequelaofproximalfractureofthehumeruswith pseudoarthrosisormajorand/orminortubercleresorption; sequelaeoftumorresection withirreparablerotator cuff lesion;andconventionalshoulderarthroplastywithupper subluxationofthehumeralcomponent,pseudoarthrosis,or reabsorptionofthetuberosities;
- Activeelevationbelow90◦;
Allprocedureswereconductedbyoneofthespecialistsin shoulderandelbowsurgeryatthisinstitution.
Thefollowingvariableswereanalyzed:
a) Demographicdata:gender,ageatsurgery,dateofsurgery, timeofsymptomspriortotheprocedure,timeof evalua-tion;
b) Diagnosis,categorized asrotatorcuffarthropathy, gleno-humeral arthrosis with irreversible rotator cuff lesion, sequela of proximal humerus fracture, inflammatory arthropathy,andtumorresectionsequela;
c) Typeofsurgery,categorizedasprimaryarthroplastyor revi-sion;
d) Functional maneuvers: hand-mouth, hand-head, and hand-neck,categorizedasableorunable,referringtothe pre-andpostoperativeperiod;
e) American Shoulder and Elbow Surgeons (ASES) score,19
regardingthepre-andpostoperativeperiod;
f) SF-1220qualityoflifescale,regardingthepre-and
postop-erativeperiod;
g) Visualanalogscale(VAS)forpre-andpostoperativepain; h) Complications: occurrence of postoperative infection,
periprostheticfracture,deepvenousthrombosis, pneumo-nia,urinarytractinfection,acutemyocardialinfarction,and death.
i) Magneticresonanceimaging,preoperative:
I) Degree of fatty degeneration of the supraspinal, infraspinatus,andsubscapularismuscles,accordingto Fuchsetal.21
II) Tendonsaffectedbytransfixingrupture.
j) Postoperative radiographic evaluation: occurrence of humeral stem loosening, glenosphere loosening, and notching.
Intervention
Procedureswereperformedundergeneralanesthesia asso-ciatedwithinterscaleneblockade.Antimicrobialprophylaxis was conducted with second-generation cephalosporin for 24h.Thesurgicalapproachusedwasthedeltopectoral,with removaloftheremainingsubscapularistendonwhenitdid notpresent ruptureofitsentireextension.Inallcases,the jointcapsulewaswidelyreleased.TheprosthesesDeltaIIIor DeltaXTEND(DePuy,Warsaw,IN,UnitedStates)with cement-ing ofthe humeralshaft were used innine casesand the EquinoxeReverseSystem (Exactech, Gainesville,FL,United States) without cementing was used in four patients. The number ofscrewsusedforbaseplate fixationwas threeor four,dependingonpatient’sbonequalityandsurgeon’s prefer-ence.Avacuumdrainwasusedinallpatientsandmaintained for24–48h.Inthepostoperativeperiod,thepatientsuseda slingforsixweeks.Activemovementsoftheelbow,wrist,and fingerswereinitiatedintheimmediatepostoperativeperiod. Passiveandactiveshouldermovementswereinitiatedafter theuseofslingwasdiscontinued.
Statisticalanalysis
Continuousvariables wereassessedfornormalityusingthe Kolmogorov–Smirnov test, and for homogeneity using the
Table1–Demographicdata.
Sex
Male 6(46%)
Female 7(54%)
Diagnosis
Rotatorcuffarthropathy 9(69%)
Fracturesequela 3(23%)
Tumorlesion 1(8%)
Typeofarthroplasty
Primary 9(69%)
Revision 4(31%)
Age(years) 62.5±13.4
Timewithsymptoms(months) 63.7±44.7
Follow-up(months) 53±21.4
Levenetest.Continuousvariableswithparametricdata dis-tributionwerepresentedasmeansandstandarddeviations; thosewithnon-parametricdistribution,asmediansand per-centiles. Categorical variables were presented as absolute valuesandpercentages.
The comparison between the pre- and postoperative
periods, regarding the different categorical variables, was made usingthe chi-squaredorFisher’s exacttests. For the continuousvariables,Student’st-testwasusedfordatawith parametricdistribution,andtheWilcoxontestwasusedfor thosewithnon-parametricdistribution.
SPSS(version20.0)wasusedfordataanalysis;a5% signif-icancelevelwasadoptedforallcalculations.
Results
Seventeenpatientsunderwentsurgicaltreatment.Ofthese, fourwereexcludedforthefollowingreasons:deathunrelated tothesurgerybefore2-yearclinicalfollow-up(one),inability toanswerthequestionnaireduetodementia(two),andloss offollow-up(one).Thegeneraldataofthesampleisshownin
Table1.
Preoperativemagneticresonanceimagingwasperformed intheninepatientswhounderwentprimaryreverse arthro-plasty. Inall cases, this imagingstudy revealed transfixing rupturesofthesupraspinatusandinfraspinatustendons,with thetendinousstumpretractedattheglenoidlevel.Insixcases (66%),atransfixinglesionoftheuppertwothirdsofthe sub-scapularistendonwasobserved.Inallothercases,thetendon wasrupturedalong itsentireextension.Fattydegeneration wasclassifiedaccordingtoFuchsetal.21asgradeIIIin100%of thesupraspinatusandinfraspinatusmuscles.Subscapularis degenerationwasratedasgradeIIinfivecases(56%)andas gradeIIIinfourcases(44%).Inthefourcasesundergoing par-tialshoulderarthroplasty, magneticresonanceimagingwas notperformed.
Table2–Pre-andpostoperativeclinicalevaluation.
Preoperative period
Postoperative period
p
ASES 23.1±15 82.7±15 <0.001
SF-12physical 31.7±6.9 47.1±8.6 <0.001
SF-12emotional 48±12.3 55.5±7.5 0.06
VAS 7.9±2.9 1±1.7 0.002
Hand-mouth 8(62%) 13(100%) 0.39
Hand-neck 2(15%) 12(92%) <0.001
Hand-head 0(0%) 13(100%) <0.001
ASES,AmericanShoulderandElbowSurgeons;VAS,visualanalog scale;SF-12,12-ItemShort-FormHealthSurvey.
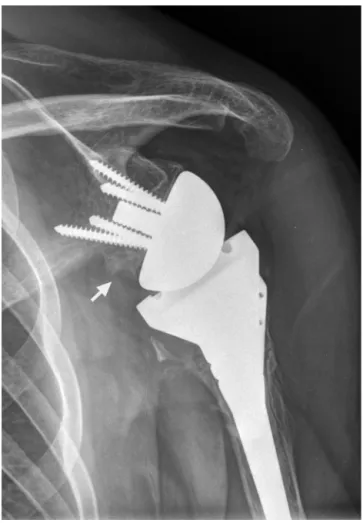
Fig.1–Post-operativeradiograph.Reverseshoulder arthroplastywithscapularnotching.
hand-neck, and hand-head tests alsoshowed a significant
improvement(p=0.039,p<0.001,andp<0.001,respectively). ClinicaldataareshowninTable2.
Clinicalcomplicationswereobservedintwopatients(15%); one case of post-operative infection, treated by surgical debridementandintravenousantibiotictherapy,andonecase ofdislocationonthe5thpostoperativeday,treatedwith reduc-tionunderanesthesiawithoutrevision.
Postoperativeradiographydidnotrevealhumeral,glenoid, or periprosthetic fractures.Notching was observed in four patients(31%;Fig.1).
Discussion
The present resultsshowed a significant clinical improve-mentofpatients.Aprogressionfrom23.1to82.7pointswas observedontheASESscale.Theresultsareconsistentwith otherstudiesthatusedthesameratingscale,showing clin-ical improvement and final results between 72 and 84.7,9
The improvementofsymptoms was alsodemonstrated by authorswho usedotherassessmenttools.5,6,8,10,16A
signifi-cantimprovementwasalsoobservedinpain,decreasingfrom 7.9to1intheVAS,afindingsimilartothatreportedbyother authors.7
AccordingtothephysicalcomponentofSF-12,therewasa significant improvementinquality oflife.Nonetheless, the mental component showed onlya trendforbetter results. Qualityoflifeanalysisisrarelyreportedinstudiesofreverse arthroplasty;thiswasthefirstBrazilianstudytoaddressthe issue.Woodrufetal.22assessedtheuseofreversearthroplasty
inrheumatoidpatientsandfoundpostoperativeresultsof38.2 forthephysicalcomponentand49.3forthemental,lowerthan thoseobservedinthepresentstudy.
Theoccurrenceofnotchinginthepresentserieswas31%. Thisresultiswithinthespectrumreportedbyotherauthors, whichrangesfrom13%to68%.5–8,10,16Likewise,15%of
com-plications found in the present study are similar to those reportedbyBrazilianandinternationalauthors.6,16
Compli-cations occurred in primary arthroplasty, eventhough the casesofrevisionpresenthighercomplicationrates.9,10Dueto
thesmallsamplesize,stratifiedanalysiswasnotperformed. Fávaroetal.8observedarateofcomplicationsofonly4%,a
lowerincidencethanthatreportedinthepresentstudyand by other authors.5,6,9,10,16 Thisis possiblyexplainedby the
factthattheirstudyonlyincludedcasesofprimary arthro-plasty,withashorterfollow-upperiodthanthatofthepresent study.
Themainlimitations ofthe present study are its retro-spective design and small samplesize. Another limitation wastheinclusionofdifferentdiagnosesandtheuseoftwo differentimplantmodels.Moreover,theminimumfollow-up time of24 months,although meeting the requirements of mostorthopedicjournals,doesnotaddresspossiblelong-term complications possible in arthroplasties procedures. How-ever, the authorsemphasizethat themean follow-up time of 53 months was superior to that of the other Brazilian studies.5,8
The present study contributes to the knowledge of the panorama of reverse arthroplasty in Brazil. The Brazilian expe rience is small; there are only two published stud-iesonthesubject.5,8 Thepresent study,albeitsmallerthan
Conclusion
Patientswho underwent reverse shoulderarthroplasty had significantimprovementinthe ASESandVASscales. Qual-ity oflife improvedsignificantly, according to the physical aspectofSF-12,andatrendforimprovementwasobserved intheemotionalaspect.Thecomplicationratewas15%,and notchingoccurredin31%ofthecases.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GrammontP,TrouilloudP,LaffayJ,DeriesX.Conceptstudy andrealizationofanewtotalshoulderprosthesis. Rhumatologie.1987;39:407–18.
2. GrammontPM,BaulotE.Deltashoulderprosthesisforrotator cuffrupture.Orthopedics.1993;16(1):65–8.
3. BaulotE,ChabernaudD,GrammontPM.Resultsof Grammont’sinvertedprosthesisinomarthritisassociated withmajorcuffdestruction.Aproposof16cases.ActaOrthop Belg.1995;61Suppl.1:112–9.
4. YoungSW,ZhuM,WalkerCG,PoonPC.Comparisonof functionaloutcomesofreverseshoulderarthroplastywith thoseofhemiarthroplastyinthetreatmentofcuff-tear arthropathy:amatched-pairanalysis.JBoneJointSurgAm. 2013;95(10):910–5.
5. AmaralMVG,FariaJLR,SiqueiraG,CohenM,BrandãoB, MoraesR,etal.Artroplastiareversadoombronotratamento daartropatiadomanguitorotador.RevBrasOrtop.
2014;49(3):279–85.
6. Al-HadithyN,DomosP,SewellMD,PanditR.Reverseshoulder arthroplastyin41patientswithcuffteararthropathywitha meanfollow-upperiodof5years.JShoulderElbowSurg. 2014;23(11):1662–8.
7. WiaterJM,MoravekJEJr,BudgeMD,KoueiterDM,
MarcantonioD,WiaterBP.Clinicalandradiographicresultsof cementlessreversetotalshoulderarthroplasty:a
comparativestudywith2to5yearsoffollow-up.JShoulder ElbowSurg.2014;23(8):1208–14.
8. FávaroRC,AbdulahadM,FilhoSM,ValerioR,SupertiMJ. Artropatiademanguito:oqueesperardoresultadofuncional daartroplastiareversa?RevBrasOrtop.2015;50(5):523–9.
9.KellyJD2nd,ZhaoJX,HobgoodER,NorrisTR.Clinicalresults ofrevisionshoulderarthroplastyusingthereverse
prosthesis.JShoulderElbowSurg.2012;21(11):1516–25. 10.ValentiP,KilincAS,SauzièresP,KatzD.Resultsof30reverse
shoulderprosthesesforrevisionoffailedhemi-ortotal shoulderarthroplasty.EurJOrthopSurgTraumatol. 2014;24(8):1375–82.
11.FerrelJR,TrinhTQ,FischerRA.Reversetotalshoulder arthroplastyversushemiarthroplastyforproximalhumerus fractures:asystematicreview.JOrthopTrauma.
2015;29(1):60–8.
12.RossM,HopeB,StokesA,PetersSE,McLeodI,DukePF. Reverseshoulderarthroplastyforthetreatmentofthree-part andfour-partproximalhumeralfracturesintheelderly.J ShoulderElbowSurg.2015;24(2):215–22.
13.GuptaAK,HarrisJD,EricksonBJ,AbramsGD,BruceB, McCormickF,etal.Surgicalmanagementofcomplex proximalhumerusfractures–asystematicreviewof92 studiesincluding4500patients.JOrthopTrauma. 2015;29(1):54–9.
14.GwinnerC,GreinerS,GerhardtC,ScheibelM.Reverse shoulderarthroplastyforfracturesequelae.Orthopade. 2013;42(7):531–41.
15.MartinezAA,BejaranoC,CarbonelI,IglesiasD,Gil-AlbarovaJ, HerreraA.Thetreatmentofproximalhumerusnonunionsin olderpatientswithreverseshoulderarthroplasty.Injury. 2012;43Suppl.2:S3–6.
16.GeeECA,HansonEK,SaithnaA.Reverseshoulder arthroplastyinrheumatoidarthritis:asystematicreview. OpenOrthopJ.2015;9:237–45.
17.RockwoodCAJr.Thereversetotalshoulderprosthesis.The newkidontheblock.JBoneJointSurgAm.2007;89(2):233–5. 18.BoileauP,WatkinsonDJ,HatzidakisAM,BalgF.Grammont
reverseprosthesis:design,rationale,andbiomechanics.J ShoulderElbowSurg.2005;141Suppl.S:147S–61S.
19.RichardsRR,AnKN,BiglianiLU,FriedmanRJ,GartsmanGM, GristinaAG,etal.Astandardizedmethodfortheassessment ofshoulderfunction.JShoulderElbowSurg.1994;3(6): 347–52.
20.WareJJr,KosinskiM.KellerSD.A12-ItemShort-FormHealth Survey:constructionofscalesandpreliminarytestsof reliabilityandvalidity.MedCare.1996;34(3):220–33. 21.FuchsB,WeishauptD,ZanettiM,HodlerJ,GerberC.Fatty
degenerationofthemusclesoftherotatorcuff:assessment bycomputedtomographyversusmagneticresonance imaging.JShoulderElbowSurg.1999;8(6):599–605. 22.WoodruffMJ,CohenAP,BradleyJG.Arthroplastyofthe