RevBrasAnestesiol.2017;67(3):284---287
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Functional
residual
capacity
increase
during
laparoscopic
surgery
with
abdominal
wall
lift
夽
Hiroshi
Ueda
a,
Takuo
Hoshi
b,∗aIbarakiPrefecturalCentral,DepartmentofAnesthesiologyandCriticalCareMedicine,Ibaraki,Japan
bIbarakiClinicalandTrainingCenter,DepartmentofAnesthesiologyandCriticalCareMedicine,TsukubaUniversityHospital,
Ibaraki,Japan
Received16November2015;accepted4December2015 Availableonline20April2016
KEYWORDS
Abdominalwalllift; Functionalresidual capacity;
Laparoscopicsurgery
Abstract
Backgroundandobjectives: Thenumberoflaparoscopicsurgeriesperformedisincreasingevery yearandinmostcasesthepneumoperitoneummethodisused.Onealternativeistheabdominal wallliftingmethodandthisstudywasundertakentoevaluatechangesoffunctionalresidual capacityduringtheabdominalwallliftprocedure.
Methods:FromJanuarytoApril2013,20patientsunderwentlaparoscopiccholecystectomyata singleinstitution.Allpatientswereanesthetizedusingpropofol,remifentanilandrocuronium. FRCwasmeasuredautomaticallybyEngstromCarestationbeforetheabdominalwallliftand again15minutesafterthestartoftheprocedure.
Results:Afterabdominalwalllift,therewasasignificantincreaseinfunctionalresidual capac-ityvalues(beforeabdominalwalllift1.48×103mL,afterabdominalwalllift1.64
×103mL) (p<0.0001).Nocomplicationssuchasdesaturationwereobservedinanypatient duringthis study.
Conclusions:Laparoscopicsurgerywithabdominalwallliftmaybeappropriateforpatientswho haveriskfactorssuchasobesityandrespiratorydisease.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Elevadordaparede abdominal;
Capacidaderesidual funcional;
Cirurgia laparoscópica
Aumentodacapacidaderesidualfuncionaldurantecirurgialaparoscópica comelevac¸ãodaparedeabdominal
Resumo
Justificativaeobjetivos: Onúmero de cirurgiaslaparoscópicas realizadas estáaumentando a cada ano e, namaioria dos casos, o método com pneumoperitônio é o escolhido. Uma opc¸ãoé o método deelevac¸ãoda paredeabdominal. Esteestudo foi feito para avaliaras
夽
ThisstudywascarriedoutbytheIbarakiPrefecturalCentralHospital.
∗Correspondingauthor.
E-mail:[email protected](T.Hoshi). http://dx.doi.org/10.1016/j.bjane.2015.12.003
Functionalresidualcapacityincreaseduringlaparoscopicsurgery 285
alterac¸ões dacapacidade residualfuncionalduranteoprocedimentodeelevac¸ãodaparede abdominal.
Métodos: De janeiro a abril de 2013, 20 pacientes foram submetidos à colecistectomia laparoscópicaemumaúnicainstituic¸ão.Todosospacientesforamanestesiadoscompropofol, remifentanilerocurônio.A CRFfoimedidaautomaticamenteusandooEngströmCarestation antesdaelevac¸ãodaparedeabdominale,novamente,15minutosapósoiníciodo procedi-mento.
Resultados: Apóselevaraparedeabdominal,umaumentosignificativofoiobservadonosvalores dacapacidaderesidualfuncional(antesdaelevac¸ãodaparedeabdominal:1,48×103mL:após aelevac¸ãodaparedeabdominal:1,64×103mL)(p<0,0001).Nãohouvecomplicac¸ões,como dessaturac¸ão,emnenhumpacienteduranteesteestudo.
Conclusões: Acirurgialaparoscópicacomelevadordaparedeabdominalpodeserapropriada parapacientescomfatoresderiscocomoobesidadeedoenc¸asrespiratórias.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND(
http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theuseoflaparoscopictechniquesinsurgeryisincreasing year byyear. There aretwomajor techniques for laparo-scopicsurgery, pneumoperitoneummethodandabdominal wall lift method. Establishing a pneumoperitoneum is a majortechniqueforlaparoscopicsurgery,whilelifting pro-cedureisaminortechnique.Apatient’spulmonaryfunctions areaffectedbyvariousfactorsduringlaparoscopicsurgery. Functionalresidualcapacity(FRC)isdecreasedbythesupine positionandtheinduction ofanesthesia1---3 duringsurgery. ThedecreaseinFRCmaycausehypoxemiaduetoincreases inbloodflowwheregasexchangeisnottakingplace. Fur-thermore,pulmonarycomplianceisdecreasedbythe pneu-moperitoneummethod,4butnotbytheabdominalwalllift.5 NopreviousstudyhasevaluatedFRCduringlaparoscopic surgerywithabdominalwalllift.Inthecurrentstudywetest our hypothesis that abdominalwall lift method increases FRC.
Methods
Ourstudyplanwasapprovedfromtheinstitutionalreview board. We retrospectively studied 20 adult patients who underwent elective laparoscopic cholecystectomy with abdominalwallliftfromJanuarytoApril2013atIbaraki Pre-fecturalCentralHospital.Wedidnotexcludeanyonefrom thisstudy.Duringtheprocedure,therightcostalarchand thenavelareawereliftedwithasubcutaneous wireusing theabdominalwall-liftsystem(MizuhoIka,Tokyo,Japan). FRCwasmeasuredrepeatedlybyEngstromCarestation(GE HealthCare,UKLtd.,Buckinghamshire,UK).Ittakesseveral minutesinthemeasurementofFRC.Weuseaverageoftwo tothreemeasurementsbeforetheabdominalwallliftand 15---30minafterthestartoftheprocedure.
Theanesthesiaandmonitoring
The patients were not given any sedative drugs before surgery.Generalanesthesiawasinducedwithremifentanil
0.2g·kg−1·min−1andtargetcontrolledinfusionofpropofol
(targetconcentrationofplasmawas3g·mL−1).
Rocuroniumwasusedforneuromuscularblock.Tracheal intubation wasperformed with tracheal tubes of internal diametersof7and8mmusedforfemaleandmalepatients, respectively.Anesthesiawasmaintainedwithpropofoland remifentaniltomaintain thebispectral indexbetween 40 and60andthesystolicpressureat±30%ofpre-anesthetic values.Tomaintain neuromuscularblock, rocuroniumwas givenintermittentlyandtheirtrain-of-fourratioof0%was confirmed. The lungs were ventilated mechanically with 30---40%oxygeninair,tidalvolume8mL·kg−1,atarespiratory
rateof10min−1.
Duringanesthesiaallpatients weremonitoredby elec-trocardiogram,non-invasivebloodpressure,pulseoximetry, bispectralindex,andtrain-of-four.
Statisticalanalysis
BasedonapreviousJapanesestudyonFRCchangesin anes-thetizedandintubatedpatients,6 power analysisrevealed thataminimumsamplesizeof17wasrequiredinorderto detectadifferenceof15%inFRCincreasingafter abdomi-nalwalllift(ˇ=0.80,˛=0.05).Dataarepresentedasmean (±SD).ComparisonsaremadebetweentheFRCbeforeand afterabdominal wall lift by paired t-test (Stat View 5.0, SASInstitute, NC,USA)and p<0.05 is considered tobea significantdifference.
Results
Patient characteristics are summarized in Table 1. There were 3 obese patients with a Body Mass Index (BMI) of >30kg·m−2. All patients were included in the statistical
analysis. After abdominal wall lift, there was a signifi-cantincreaseoffunctionalresidualcapacityvalues(before abdominalwalllift1.48×103mL,afterabdominalwalllift
1.64×103mL)(p<0.0001).
286 H.Ueda,T.Hoshi
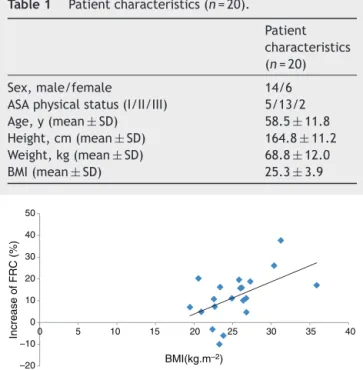
Table1 Patientcharacteristics(n=20).
Patient characteristics (n=20)
Sex,male/female 14/6 ASAphysicalstatus(I/II/III) 5/13/2 Age,y(mean±SD) 58.5±11.8 Height,cm(mean±SD) 164.8±11.2 Weight,kg(mean±SD) 68.8±12.0 BMI(mean±SD) 25.3±3.9
Increase of FRC (%)
–20 –10 0 10 20 30 40 50 40 35 30 25 20 15 10 5 0
BMI(kg.m–2)
Figure1 RelationshipbetweenBMIandincreaseofFRC.After abdominal wall lift, there was a significant increase of FRC values.Inaddition,therewasacorrelationbetweenBMIand increaseofFRC.
Thecoefficientofdetermination(R2)was0.278andp-value was0.017.Duringthisstudy,nocomplicationssuchas desat-urationwereobservedinanyofthepatients.
Discussion
Alongwithanimprovementinthedevicesandtechniquesof laparoscopicsurgeriestheinstancesofsuchproceduresfor patientswithrespiratorycomplicationsareincreasing annu-ally.Ameta-analysisrevealedthatthedurationofsurgery withabdominalwall lift is significantlylonger than pneu-moperitoneummethod.7 However,theresultsofourstudy suggestthat FRCduringlaparoscopic surgerywith abdom-inal wall lift increases significantly. This may be a great advantageforpatientswithrespiratorycomplications.
When compared with laparotomy, laparoscopic chole-cystectomyis associatedwithshorter meanpostoperative hospital stay, and reduced mean cost.8 Laparoscopic cholesystectomywithpneumoperitoneumcausessignificant decreasesinVitalCapacity(VC)andFRCatthe postopera-tiveperiod,althoughlesssignificantthanopenlaparotomy.9 Although we did not compare withpostoperative FRC, in ourstudyofthe abdominalwallliftmethod,FRCactually increaseswiththesurgeryandabigdifferenceisobserved betweenthe decreaseand increaseof FRC inthe respec-tivesurgicalmethods,especiallyinpatientswithrespiratory problems.
Becausethisisretrospectivestudy,wedonothaveexact data of airway pressure or I:E ratio,but we usually ven-tilate patients withI:E ratio 1:2 without using PEEP and recruitmentmaneuver.
Abdominal wall lift method involves lifting up the righthypochondriumandumbilicalregionthereforeitmay
increaseFRCbyoutwardmovementofthechestand abdom-inalwall.TheincreaseofFRCmaycontributetothelower levelsofPaCO2observedpostoperativelycomparedto
pneu-moperitoneumasreportedbyRenetal.,7whichisofgreat benefit for obese patients or those with respiratory dis-ease. However,we have notevaluatedpostoperativepain at eitherthelifting siteorthewound alongsidea postop-erativebloodgasanalysis;thereforeitisunknownwhether ourpatientsshowedlowerlevelofPaCO2withoutextensive
pain.
Ourstudy alsohassuggested that therewasa univari-ate correlation between BMI and increase of FRC during laparoscopicsurgerywithabdominalwalllift.Eichenberger et al. reported that atelectasis formation would be par-ticularly significant in morbidly obese patients (with a BodyMass Index(BMI)of>35kg·m−2).10 Furthermore,they showed that atelectasis remained unchangedfor at least 24hours.Althoughwehaveonly threeobesepatientsand the number of subjects are not enough to discuss the relationship between BMIand FRC, these findingssuggest that for obese patients in particular abdominal wall lift-ing may be more advantageous than pneumoperitoneum. ThereareseveralmethodsofmeasuringFRC:closed-circuit helium dilution method,11 oxygen (O
2) wash-in method,12
nitrogen (N2) washout method (Fowler’s method),13 body
plethysmography, and computed tomography as the gold standard. Engstrom Carestation measures FRC via the nitrogen washoutmethod. This method can measure FRC repeatedlyinananesthetizedpatientwithoutinterrupting mechanicalventilation.
Chiumelloetal. demonstratedthat theEnd Expiratory Lung Volume (EELV) measurement by Engstrom Caresta-tionwithmodifiednitrogenwashout/washintechnique(at all lung volumes) correlates well with CT scanning14 and is therefore a reliable measurement tool. In the cur-rent studywe repeatedly measured theFRC forthe same patient to verify the data. Therefore, we posit that our data of the numerical increase and decrease of FRC is reliable.
Summary
Laparoscopic surgery via abdominal wall lift may be an appropriatesurgicaloptionforpatientswhohaverisk fac-torssuchasobesityandrespiratorydisease.
Funding
Funding was provided solely from institutional and/or departmentalsources.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
Functionalresidualcapacityincreaseduringlaparoscopicsurgery 287
References
1.CraigDB,WahbaWM,DonHF,etal.‘‘Closingvolume’’andits relationshiptogasexchangeinseatedandsupineposition.J ApplPhysiol.1971;31:717---21.
2.WestbrookPR,StubbsSE,SesslerAD,etal.Effectsofanesthesia andmuscleparalysisonrespiratorymechanicsinnormalman. JApplPhysiol.1973;34:81---6.
3.DonHF,WahbaWM,CuadradoL,etal.Theeffectsofanesthesia and100percentoxygenonthefunctionalresidualcapacityof thelungs.Anesthesiology.1970;32:521---9.
4.Rauh R, Hemmerling TM, Rist M, et al. Influence of pneu-moperitoneumand patient positioning on respiratorysystem compliance.JClinAnesth.2001;13:361---5.
5.MatsumotoK.Changesinthorax-lungcomplianceduringgeneral anesthesiawithmechanicalventilationinresponsetovarious intraoperativemaneuvers.Masui.2006;55:704---7.
6.KanayaA,SatohD,KurosawaS.Higherfractionofinspired oxy-genin anesthesia inductiondoes notaffect functional study residual capacity reduction after intubation: a comparative study of higher and lower oxygen concentration. J Anesth. 2013;27:385---9.
7.RenH,TongY,DingXB,etal.Abdominalwall-liftingversusCO2 pneumoperitoneuminlaparoscopy:areviewandmet-analysis. IntJClinExpMed.2014;7:1558---68.
8.GracePA,QuereshiA,ColemanJ,etal.Reducedpostoperative hospitalizationafterlaparoscopiccholecystectomy.BrJSurg. 1991;78:160---2.
9.JohnsonD,LitwinD,OsachoffJ,etal.Postoperative respira-toryfunctionafterlaparoscopiccholecystectomy.SurgLaparosc Endosc.1992;2:221---6.
10.EichenbergerA,ProiettiS,WickyS,etal.Morbidobesityand postoperativepulmonaryatelectasis:anunderestimated prob-lem.AnesthAnalg.2002;95:1788---92.
11.Brown R, Leith DE, Enright PL. Multiple breath helium dilu-tion measurement of lung volumes in adults. Eur Respir J. 1998;11:246---55.
12.Mitchell RR, Wilson RM, Holzapfel L, et al. Oxygen wash-in methodformonitoringfunctionalresidualcapacity.CritCare Med.1982;10:529---33.
13.Newth CJL, Enright P, Johnson RL. Multiple-breath nitrogen washouttechniques:includingmeasurementswithpatientson ventilators.EurRespirJ.1997;10:2174---85.