w w w . r b o . o r g . b r
Original
article
Postoperative
infection
in
patients
undergoing
inspection
of
orthopedic
damage
due
to
external
fixation
夽
Noel
Oizerovici
Foni
∗,
Felipe
Augusto
Ribeiro
Batista,
Luís
Henrique
Camargo
Rossato,
José
Octavio
Soares
Hungria,
Marcelo
Tomanik
Mercadante,
Ralph
Walter
Christian
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22July2014 Accepted26September2014 Availableonline31October2015
Keywords:
Infection Externalfixators Internalfracturefixation
a
b
s
t
r
a
c
t
Objective:Toconductaretrospectiveanalysisoncasesundergoinginspectionof orthope-dicdamage,atanorthopedicemergencyserviceinateachinghospital,withtheaimof evaluatingpatientswithpostoperativeinfectionafterconversiontointernalosteosynthesis.
Methods:ThiswasaretrospectiveanalysiscoveringtheperiodfromJune2012toJune2013, onpatientswhounderwentinspectionoforthopedicdamageduetoexternalfixationand subsequentlywereconvertedtodefinitiveosteosynthesisusinganailorplate.
Results:Wefoundaninfectionrateof13.3%inoursampleand,furthermore,foundthat therehadbeentechnicalerrorsinsettingupthefixatorin60.4%ofthecases.
Conclusion: Wefoundaninfectionratethatweconsideredhigh,alongwithinadequaciesin constructingtheexternalfixator.Weemphasizethatthisprocedureisnotrisk-freeandthat trainingforphysicianswhoperformthisprocedureshouldbemandatory.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Infecc¸ão
pós-operatória
nos
pacientes
submetidos
ao
controle
de
danos
ortopédicos
pela
fixac¸ão
externa
Palavras-chave:
Infecc¸ão
Fixadoresexternos Fixac¸ãointernadefraturas
r
e
s
u
m
o
Objetivo:Fazer uma análise retrospectiva de casos submetidos ao controle de danos ortopédicos em um pronto socorrode ortopedia de hospital-escola com oobjetivo de avaliarospacientescominfecc¸ãopós-operatóriaapósseremconvertidosparaosteossíntese interna.
Métodos:Análiseretrospectivadepacientesdejunhode2012ajunhode2013submetidosao controlededanosortopédicoscomfixadorexternoqueposteriormenteforamconvertidos paraosteossíntesedefinitiva,comhasteouplaca.
夽
WorkperformedintheTraumaGroup,DepartmentofOrthopedicsandTraumatology,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](N.O.Foni). http://dx.doi.org/10.1016/j.rboe.2015.10.011
Resultados: Encontramosumataxadeinfecc¸ãode13,3%emnossacasuísticaeverificamos errostécnicosnaelaborac¸ãodofixadorem60,4%dasoportunidades.
Conclusão: Foiencontradaumataxadeinfecc¸ãoqueconsideramosalta,assimcomode inadequac¸õesnaconfecc¸ãodofixadorexterno.Salientamosqueesseprocedimentonãoé isentoderiscosetreinamentoparamédicosqueofazemdeveserobrigatório.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Damagecontrolistheorthopedicsurgicaltacticestablished intheliteraturethatisindicatedformultipletraumapatients orthosewithseveresoft-tissueinjuries.1However,this proce-dureisnotfreefromrisks.Localandsystemiccomplications associated with external fixation for damage control have beenreported2andoneoftheseisboneinfection.Studieshave showninfectionratesalongthepathsofthepinsrangingfrom 0.5to30%.2,3
Bacterialcontaminationandinfectionalongthepathofthe pinsofexternalfixatorsarerelativelycommon.Conversionto internalosteosynthesisundersuchconditions,whichcould involveuseofintramedullarynailsorplates,maygiveriseto severelocaland/orsystemiccomplications.4Thefrequencyof thisassociationofeventsisunclearintheliterature.3
Thecorrelationbetweeninfection along thepathofthe pinsofexternalfixatorsandpost-traumaticosteomyelitis sub-sequenttointernalosteosynthesis,thusconfiguringchronic infectionofthelocomotorsystem,iswellestablished.5,6
Infectionofthebone–pininterfaceofthefixatorhasbeen proventohaveadirectassociationwiththeinsertion tech-nique,withregardtothestabilityandpositioningofthelimb duringpinplacement,giventhatthismightgiverisetotension withinthesofttissues.Presenceofthesefactorscontributes towardinfectiouscomplicationssubsequenttoconversionto definitiveinternalosteosynthesis,irrespectiveofwhetherthis willinvolveanintramedullarynailoraplate.7,8
Theaimofourstudywastoidentifythequalityof reduc-tion andfixationand thefrequencyofboneinfection after definitivetreatment,amongpatientswhowereadmittedto anemergencyserviceoveraone-yearperiodandunderwent musculoskeletaldamagecontrol.
Sample
and
methods
This study was duly submitted to and approved by our institution’sethicscommitteeandwasregisteredunderthe committee’sprotocolnumber624.307.
Retrospectiveevaluationsweremadeon120patientswho underwentexternalfixationtocontrolmusculoskeletal dam-agebetweenJune2012andJune2013,attendedasemergencies attheemergencyserviceofourinstitution’sDepartmentof OrthopedicsandTraumatology.
In this retrospective study, we included patients who underwent damage control surgery consisting of external
fixationandwho,afterconversiontodefinitive osteosynthe-sis,evolvedwithinfection.
Patients who presented infectious complications in the presenceoflocalandsystemicalterationssuchas vasculopa-thy, diabetesmellitusorconsumptivedisease,andpatients withpsychiatricdisordersthatmighthaveimpairedthe evo-lutionoftheconditionorcareprovidedforthefixatorinsome manner,wereexcluded.
Alltheradiographsweregeneratedindigitalformandwere analyzed through the Impax software. Thedistances from theorificeand Schanzpinstothedefinitivesynthesiswere analyzedwithinthissoftware.Wesoughttoidentifyany pres-enceoftechnicalerrorsduringthedrilling(characterizedby multipledrilling),withsubjectiveanalysisconductedbythree differentgroupsoftwoevaluators.Onegroupwasformedby attendingphysicianswithatleastfiveyearsofexperiencein orthopedictrauma;anothergroupwasformedbytwo third-yearresidentsandathirdgroupwasformedbytworesidents inthesecondyearoforthopedics.Theevaluatorswerenamed asfollows(Table1):
- Evaluator1:attendingphysicianwithmorethanfiveyears ofexperience
- Evaluator2:attendingphysicianwithmorethanfiveyears ofexperience
- Evaluator3:third-yearresident - Evaluator4:third-yearresident - Evaluator5:second-yearresident - Evaluator6:second-yearresident
Postoperativeinfection wascharacterizedbymeans ofa clinicalexaminationconductedduringhospitalizationoratan outpatientinvestigation,fromthedatanotedinthemedical files.Theclinicalcriteriaforinfectionweretakentobethe following:erythema,hyperemiaorfistulaalongthepathsof thepinsorinthesurgicalincision(Fig.1).
During theexternalfixation, theholesdrilledpreviously usingabitwerealwaysrespectedandthepinswereinserted manually.Noneofthepinswereinthezoneofexposureofthe fracture.
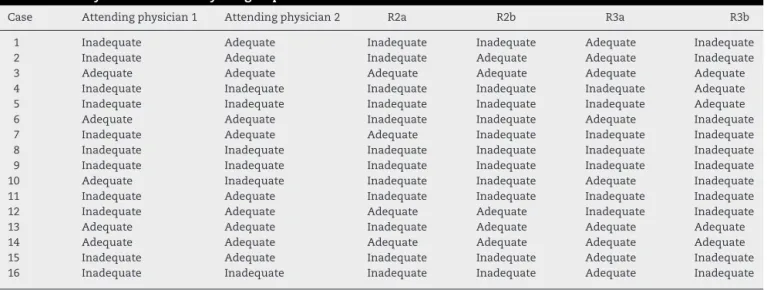
Table1–Analysisonthecasesbythegroupofevaluators.
Case Attendingphysician1 Attendingphysician2 R2a R2b R3a R3b
1 Inadequate Adequate Inadequate Inadequate Adequate Inadequate 2 Inadequate Adequate Inadequate Adequate Adequate Inadequate 3 Adequate Adequate Adequate Adequate Adequate Adequate 4 Inadequate Inadequate Inadequate Inadequate Inadequate Adequate 5 Inadequate Inadequate Inadequate Inadequate Inadequate Adequate 6 Adequate Adequate Inadequate Inadequate Adequate Inadequate 7 Inadequate Adequate Adequate Inadequate Inadequate Inadequate 8 Inadequate Inadequate Inadequate Inadequate Inadequate Inadequate 9 Inadequate Inadequate Inadequate Inadequate Inadequate Inadequate 10 Adequate Inadequate Inadequate Inadequate Adequate Inadequate 11 Inadequate Adequate Inadequate Inadequate Inadequate Inadequate 12 Inadequate Adequate Adequate Adequate Inadequate Inadequate 13 Adequate Adequate Inadequate Adequate Adequate Adequate 14 Adequate Adequate Adequate Adequate Adequate Adequate 15 Inadequate Adequate Inadequate Inadequate Adequate Inadequate 16 Inadequate Inadequate Inadequate Inadequate Adequate Inadequate
problems for the definitive internal fixation. Amongthese
problems,wenotedanycasesofsurgerypostponedbecause
ofinfectionalongthepathofthepin,changestothesurgical incisionfordefinitiveosteosynthesisandunplannedsurgical proceduresforreassemblingthefixatorbecauseofanunstable assembly.
Themeantimetakenforconversionoftheexternalfixators todefinitiveosteosynthesiswasevaluatedthrough retrospec-tiveanalysisonthemedicalfiles.
Results
Outofthe 120patientswho underwentdamagecontrol,16
(13.3%)sufferedpost-traumaticosteomyelitisafterthe defini-tivesynthesis.Amongthese16patients,theirconditioncould bedirectlycorrelated withthedefinitiveinternal osteosyn-thesisbecausetherewerenosignsoflocalinfectionafterthe externalfixationattheemergencyservice.
Themean ageofthese16 patientswas43.4 years,with
arangefrom19to81.Wenotedthatmalepatients predomi-nated,comprising13patients(81.2%),andtheremainingthree (18.8%)werefemale.
Regardingthetimetakenforconversionoftheexternal fix-atortodefinitiveosteosynthesis,theshortestperiodwasfive
daysandthelongestwas30days.Themeantimetakenfor
thedefinitiveconversionwas15days.
Infectionoccurredineightcasesoflower-legfracturealone (50%),whiletwopatientshadfracturesofthefemurand ipsi-lateraltibia(floatingknee)(12.5%),twohadfracturesofthe
Fig.1–InfectionalongthepathofaSchanzpin.
ankle(12.5%),twohadfracturesofthetibialplateau(12.5%), onehadafractureofthefemuralone(6.2%)andonehada fractureofthehumerus(6.2%).
Among these16 patients with post-traumaticinfection,
37.5%ofthecases(sixpatients)occurredafterclosedfractures and62.5%(10patients)afterexposedfracturesofGustilograde 3A(Table2).
In10patients(62.5%),thefixatorwasassembledacrossthe joint,whileitwasmonostoticwithmonolateralconfiguration intheother6patients(37.5%),withtube-to-tubeconnection. Regardingtheetiologicalagent,itwasadequatelyidentified in10(62.5%)ofthe16infectedpatients.Inone-thirdofthese, multiplebacteriawereobservedandsurgerywasrequiredfor cleaning, debridement and curettage ofthe path from the pinorifice.Thepolymicrobialfindingsfromtheintraoperative cultureswerethefollowing:Staphylococcusaureus, coagulase-negativeStaphylococcus, Klebsiellasp,Acinetobacterbaumannii
andPseudomonasaeruginosa.
Table2–Distributionofthepatientsstudied.
Name Sex Age Fracturelocation Gustilo Externalfixator Pin number
Distancefrompinto definitivesynthesis
Presenceof multiple drilledholes
Timetaken until conversion
1 M 19 Lowerleg 3A Transarticularoverankle 4 6cm 30days 2 M 73 Lowerleg 3A Transarticularoverknee 4 5cm 14days 3 M 43 Lowerleg 3A Linearonlowerleg 4 3.2cm(lockingscrew) x 14days 4 M 19 Lowerleg 3A Linearonlowerleg 4 1.5cm(lockingscrew) x 6days 5 M 36 Lowerleg 3A Linearonlowerleg 4 4.3cm(lockingscrew) x 9days 6 M 24 Femur 3A Tube-to-tubeonfemur 4 1cm x 21days 7 M 33 Humerus 3A Transarticularoverelbow 4 0 x 10days 8 M 24 Femur+lowerleg 3A Transarticularoverknee 8 0 5days 9 M 56 Lowerleg 3A Linearonlowerleg 6 0 x 21days 10 M 37 Plateau 0 Transarticularoverknee 4 0 x 13days 11 M 31 Femur+knee 3A Transarticularoverknee 8 0 x 15days 12 F 81 Ankle 0 Transarticularoverankle 4 0 15days 13 F 71 Ankle 0 Transarticularoverankle 4 5cm 6days 14 M 25 Lowerleg 0 Linearonlowerleg 4 5cm(lockingscrew) 10days 15 F 74 Tibialdiaphysis+fibula 0 Transarticularoverankle 4 3.5cm 21days 16 M 49 Plateau 0 Transarticularoverknee 4 0 10days
Fig.2–Multipledrillinginatube-to-tubefixatorassembly.
Table4–Analysisoncasesaccordingtoevaluator.
Evaluator Numberofadequate cases(%)
Numberof inadequatecases(%)
1 5(31.3) 11(68.7) 2 10(62.5) 6(37.5) 3 9(56.2) 7(43.8) 4 5(31.3) 11(68.7) 5 4(25) 12(75) 6 5(31.3) 11(68.7) Total 38(39.6) 58(60.4)
In13 cases(81.2%)inwhichtherewassomeagreement
(adequate orinadequate), the fixationwasconsidered
ade-quate in four cases (30.8%) and inadequate in nine cases
(69.2%).
Inanalyzingtheevaluations,wehadatotalof96 evalu-ations.Thefixationwasconsideredadequatein38ofthese (39.6%)andinadequatein58(60.4%).Inanalyzingeach evalu-ator’sdecisions,wefoundthefollowing:forevaluatorone,five cases(31.3%)evaluatedasadequateand11(68.7%)as inade-quate;forevaluatortwo,10cases(62.5%)asadequateandsix (37.5%)asinadequate;forevaluatorthree,ninecases(56.2%)as adequateandseven(43.8%)asinadequate;forevaluatorfour, fivecases(31.3%)asadequateand11(68.7%)asinadequate; evaluatorfive,fourcases(25%)asadequateand12(75%)as inadequate;andevaluatorsix,fivecases(31.3%)asadequate and11(68.7%)asinadequate(Table4).
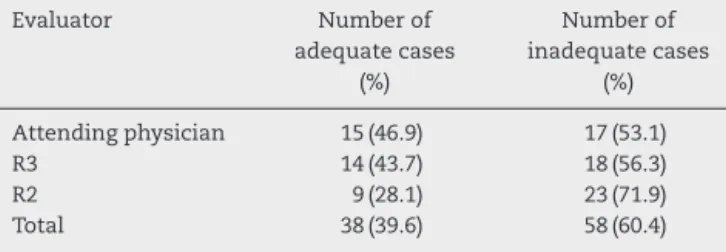
Inevaluatingtheorthopedistswithmorethanfiveyearsof experiencealone,therewere32evaluations,inwhichthe fix-ationwasconsideredadequatein15(46.9%)andinadequate
Table3–Evaluationofthecases.
Numberofevaluators Totalnumberofcases(%) Numberofadequatecases Numberofinadequatecases
6evaluators 4(25) 2 2
5evaluators 5(31.3) 2 3
4evaluators 4(25) 0 5
Table5–Evaluationaccordingtoexperience.
Evaluator Numberof adequatecases
(%)
Numberof inadequatecases
(%)
Attendingphysician 15(46.9) 17(53.1) R3 14(43.7) 18(56.3) R2 9(28.1) 23(71.9) Total 38(39.6) 58(60.4)
in17 (53.1%)(Table 4). In this group,there was agreement regardingthe qualityofthe fixation and reductioninnine cases (56.3%) and disagreement in the other seven cases (43.7%).Amongthenine caseswithagreement, thequality ofthereductionandfixationwasconsideredadequateinfour cases(44.4%)andinadequateinfive(55.6%).
Inevaluatingthethird-yearresidentsalone,therewere32 evaluations,inwhichthefixationwasconsideredadequate in14(43.7%)andinadequatein18 (56.3%)(Table4).Inthis group,therewasagreementregardingthequalityofthe fix-ationandreductioninninecases(56.3%)anddisagreement intheothersevencases(43.7%).Amongtheninecaseswith agreement,thequalityofthereductionandfixationwas con-sideredadequateinfourcases(44.4%)andinadequateinfive (55.6%).
Inevaluatingthesecond-yearresidentsalone,therewere 32evaluations,inwhichthefixationwasconsideredadequate innine(28.1%)andinadequatein23(71.9%)(Table4).Inthis group,therewasagreementregardingthequalityofthe fix-ationandreductionin13cases(81.3%)anddisagreementin theotherthreecases(18.7%).Amongthe13caseswith agree-ment,thequalityofthereductionandfixationwasconsidered adequateinthreecases(23.1%)andinadequatein10(76.9%). Amongtheevaluationsinwhichthefixationwas consid-eredadequate,it could beseenthat therewas atendency toward similarity of evaluations between the attending physicians and the third-year residents, but fewer cases wereconsideredadequateamongthesecond-yearresidents (Table5).
Incomparingthecasesinwhichtherewasagreementin the evaluations betweenthe attendingphysicians and the third-yearresidents,weobservedthattherewasagreement infive(31.3%)ofthe16cases,amongwhichthereductionand fixationwasconsideredadequateinthreeandinadequatein two.Amongtheother11cases,althoughtheattending physi-ciansagreedintheirevaluationsinfourcases,theydidnot agreewiththethird-yearresidents:ofthese,thereductionand fixationwereconsideredadequatebytheattendingphysicians inonecaseandinadequateinthreecases.
Incomparingthecasesinwhichtherewasagreementin the evaluations betweenthe attendingphysicians and the second-year residents, we observed that this was seen in seven(77.8%)oftheninecases.Ofthese,thereductionand fix-ationwereconsideredadequateintwocasesandinadequate infivecases.Inonecaseinwhichtheattendingphysicians agreedthatthefixationwasadequate,thesecond-year resi-dentsconsideredthatitwasinadequate.
In evaluating the seven cases in which there was no agreementbetweentheattendingphysicianswithmorethan fiveyearsofexperience, weobservedthatinonecase,the
residents(boththirdandsecond-year)alsodidnotagree.In fourcases,thetwoevaluatorswhowerethird-yearresidents alsodidnotagree,whileinthreecases,thetwoevaluators who were third-year residents agreed, suchthat theyboth consideredthatthereductionandfixationwereinadequate. Amongthe seven casesinwhich the attendingphysicians didnotagree,theevaluatorswhoweresecond-yearresidents consideredthatthereductionandfixationwereadequatein onecaseandinadequateinfour.
Discussion
External fixators,whichare fixation devicesofgreater ver-satility that enable a variety of types of assembly and configuration,canbeputinplacequickly.Theyareapplied percutaneouslytotreatfracturesinemergencysituationsso astocontrolthedamagewithlessdamagetosofttissues.
Thisprocedure,appliedinbothaprovisionalanda defini-tivemanner,isstillusedroutinelyinmanyhospitalservices. Itwasfoundtobechosenby32to89%ofagroupof orthope-distsinapreviousstudy.9However,thisprocedureisnotfree fromrisks.
Inoursample,wefoundthatthefrequencyofinfection afterusinganexternalfixatorfordamagecontrolwas13.3%. Althoughthisrateiscompatiblewiththoseintheliterature, whichrangefrom0.5to30%,2,3weareconcernedaboutthis becausewejudgethatthisrateisveryhighamongthepossible complications.
Thefirstissuetobeborneinmindinseekingthe etiol-ogyoftheinfectionisalwaystheenvironmentinwhichthe treatmenttakesplace,whichinourcasewasateaching hos-pital.Thereseemstobeaweakcorrelationbetweencauseand effect,giventhatthisprocedureisconsideredtobeoneoflow complexity andtherewould beatleastonephysicianwith threeyearsoftraininginthesurgicalteam.
Anotherfactorthatisinvolvedincomplicationsfrom infec-tionafterinternalosteosynthesisisinfection ofthepathof the Schanz pins.Among our patients, presence of a clin-ical suspicion of infection was an indication for changing the pin installation to another location, or for continuing thetreatmentwithosteosynthesisbymeansofanexternal fixator.
Thereduction and fixationwere considered to be inad-equate in 60% of the evaluations. This proportion can be consideredtobeveryhigh:onaverage,theattending physi-cians and third-year residents found that the reduction and fixationwereadequate inonly50%oftheevaluations. This shows that there is a need for better teaching with regardtotreatmentsinemergencysituationsusingexternal fixators.
didnothaveany distancefrom the definitive osteosynthe-sis.
The correct pin insertion technique and care with the dressing and operative woundare essential forpreventing thesecomplications.9,10Predrilling,manualpininsertionand useofasafetycorridorarefactorsthatcannotbeforgotten duringthefixation.Systematizationofthisintraand postop-erativecareisafactorthatcanbecontrolledbythephysician in order toinfluence the infection rate ofthe path ofthe Schanzpins,fordamagecontrol.
Inroutinepractice,the qualityofthefracture reduction isnot so importantin consideringpostoperative infection, giventhatthe useofexternalfixationistemporary.8 How-ever,insomesituationsinwhichthefixatorremainsinplace for a prolonged period, this factor needs to be taken into account.Inoursample,the longesttimethatelapseduntil conversionwas30days.Temporaryreductionisimportantfor stabilizingthecondition,andforlocalcareandthegeneral condition.
Inour cases, weobserved that all ofthem presented a safety corridorthat was seen tobe respectedinanalyzing theradiographs(inoursample,noneurovascularlesionswere observed).
Inordertoidentifythe importanceofthequality ofthe installationandspatialassemblyoftheexternalfixators,we askedphysicianswithdifferentlengthsoftrainingtojudge thequalityoftheassemblyandtodetermineratesoftechnical inadequacyfromradiographsinthefiles.Inourstudy,60%of thecaseswereconsideredtobetechnicallyinadequate,which wasaveryhighrate.
Regarding the frequency of bone infection after dam-age control, wefound that amongthe 13% with infection, occurrencesoferrorsortechnicalinadequaciesmayhave con-tributedtowardtheundesirableoutcomein50%.
Inconsideringtheassembliesoftheexternalfixators,we wereunabletocorrelatethefrequencyofinfectionwithany giventypeofassembly.Transarticularassemblies,whichare used for meta-epiphyseal fractures, fractures of ipsilateral bonesandextensivesoft-tissuelesions,inordertoavoid post-traumaticjointdeformities,werethemostprevalenttype,in 62.5%ofthecases.
Althoughit wasnot possibleto correlate internal post-osteosynthesisinfectionwiththeuseoffixatorsfordamage control,the presenceofinadequacyoftheassemblies that wereinstalledintheemergencyservicesuggestedthatthere isaneedfortrainingandforrulesforfixatorassemblyand use.
Conclusion
Bone infection occurred in 13.3% of the cases treated with musculoskeletal damage control followed by internal osteosynthesis.Inthesecases,thereductionandfixationwere consideredadequatein39.6%oftheevaluationsand inade-quatein60.4%.Weemphasizethatthisprocedureisnotfree fromriskandthattrainingforthephysicianswhoperformit shouldbeobligatory.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.ScaleaTM,BoswellSA,ScottJD,MitchellKA,KramerME, PollakAN.Externalfixationasabridgetointramedullary nailingforpatientswithmultipleinjuriesandwithfemur fractures:damagecontrolorthopedics.JTrauma. 2000;48(4):613–21.
2.ParameswaranAD,RobertsCS,SeligsonD,VoorM.Pintract infectionwithcontemporaryexternalfixation:howmuchofa problem?JOrthopTrauma.2003;17(7):503–7.
3.MahanJ,SeligsonD,HenrySL,HynesP,DobbinsJ.Factorsin pintractinfections.Orthopedics.1991;14(3):305–8.
4.HarwoodPJ,GiannoudisPV,ProbstC,KrettekC,PapeHC.The riskoflocalinfectivecomplicationsafterdamagecontrol proceduresforfemoralshaftfracture.JOrthopTrauma. 2006;20(3):181–9.
5.GreenSA,RipleyMJ.Chronicosteomyelitisinpintracks.J BoneJointSurgAm.1984;66(7):1092–8.
6.ClasperJC,CannonLB,StapleySA,TaylorVM,WatkinsPE. Fluidaccumulationandtherapidspreadofbacteriainthe pathogenesisofexternalfixatorpintrackinfection.Injury. 2001;32(5):377–81.
7.MoroniA,VanniniF,MoscaM,GianniniS.Stateoftheart review:techniquestoavoidpinlooseningandinfectionin externalfixation.JOrthopTrauma.2002;16(3):189–95. 8.CardozoRT,SilvaLG,BraganteLA,RochaMA.Tratamentodas
fraturasdiafisáriasdatíbiacomfixadorexternocomparado comahasteintramedularbloqueada.RevBrasOrtop. 2013;48(2):137–44.
9.BalbachevskyD,BellotiJC,MartinsCVE,FernandesHJA, FaloppaF,ReisFB.Comosãotratadasasfraturasexpostasda tíbianoBrasil?Estudotransversal.ActaOrtopBras.
2005;13(5):229–32.