SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Transtibial
technique
versus
two
incisions
in
anterior
cruciate
ligament
reconstruction:
tunnel
positioning,
isometricity
and
functional
evaluation
夽
Ricardo
Hideki
Yanasse,
Alisson
Amoroso
Lima,
Rodrigo
Silveira
Antoniassi
∗,
Danilo
Abu
Ezzedin,
Marcos
Henrique
Ferreira
Laraya,
Roberto
Ryuiti
Mizobuchi
ServiceofOrthopedyandTraumatology,FaculdadedeMedicinadeMarília(Famema),Marília,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10February2015 Accepted24April2015 Availableonline9April2016
Keywords:
Knee
Anteriorcruciateligament reconstruction
Radiography
a
b
s
t
r
a
c
t
Objective:Tocomparethetranstibialandtwo-incisiontechniquesforanteriorcruciate liga-ment(ACL)reconstructionusingasingleband.
Methods:Aprospectiveandrandomizedstudywasconductedinblocks.Patientsunderwent ACLreconstructionbymeansoftwotechniques:transtibial(group1:20patients)ortwo incisions(group2:20patients).Theradiographicpositioningofthetunnel,inclinationof thegraft,graftisometricityandfunctionalresults(IKDCandLysholm)wereevaluated.
Results:Thepositioningofthefemoraltunnelontheanteroposteriorradiograph,expressed asameanpercentagerelativetothemedialborderofthetibialplateau,was54.6%ingroup 1and60.8%ingroup2(p<0.05).Thepositioningofthefemoraltunnelonthelateral radio-graph,expressedasameanpercentagerelativetotheanteriorborderofBlumensaat’sline, was68.4%ingroup1and58%ingroup2(p<0.05).Themeaninclinationofthegraftwas19◦
ingroup1and27.2◦
ingroup2(p<0.05).Themeangraftisometricitywas0.96mmingroup 1and1.33mmingroup2(p>0.05).Group2hadbetterresultsfromthepivot-shiftmaneuver (p<0.05).
Conclusion:Thetechniqueoftwoincisionsallowedpositioningofthefemoraltunnelthat wasmorelateralizedandanteriorized,suchthatthegraftwasmoreinclinedandthere wasaclinicallybetterresultfromthepivot-shiftmaneuver.Therewasnodifferencein isometricityandnofinalfunctionalresultovertheshortfollow-uptimeevaluated.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheServiceofOrthopedyandTraumatology,FaculdadedeMedicinadeMarília(Famema),Marília,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.S.Antoniassi). http://dx.doi.org/10.1016/j.rboe.2016.04.001
Técnica
transtibial
versus
duas
incisões
na
reconstruc¸ão
do
ligamento
cruzado
anterior:
posicionamento
dos
túneis,
isometricidade
e
avaliac¸ão
funcional
Palavras-chave:
Joelho
Reconstruc¸ãodoligamento cruzadoanterior
Radiografia
r
e
s
u
m
o
Objetivo: Compararastécnicastranstibialededuasincisõesnareconstruc¸ãodoligamento cruzadoanterior(LCA)combandaúnica.
Métodos: Foifeitoumestudoprospectivoerandomizadoembloco.Ospacientesforam sub-metidosareconstruc¸ãodoLCApormeiodeduastécnicas:transtibial(grupo1:20pacientes) oudeduasincisões(grupo2:20pacientes).Foramavaliadosoposicionamentoradiográfico dostúneis,ainclinac¸ãodoenxerto,aisometricidadedoenxertoeosresultadosfuncionais (IKDCeLysholm).
Resultados: OposicionamentodotúnelfemoralnaradiografiaemAPexpressoem porcent-agememrelac¸ãoàbordamedialdoplanaltotibialnogrupo1foiemmédiade54,6%e nogrupo2foide60,8%(p<0,05).OposicionamentodotúnelfemoralnaradiografiaemP expressoemporcentagememrelac¸ãoàbordaanteriordalinhadeBlumensaatnogrupo1 foiemmédiade68,4%enogrupo2foide58%(p<0,05).Ainclinac¸ãodoenxertonogrupo 1foiemmédiade19grausenogrupo2foide27,2graus(p<0,05).Aisometricidadedo enxertonogrupo1foiemmédiade0,96mmenogrupo2foide1,33mm(p>0,05).Ogrupo 2apresentoumelhoresresultadospelamanobradePivot-Shift(p<0,05).
Conclusão: A técnica de duas incisões permitiu um posicionamento dotúnel femoral maislateralizadoeanteriorizadoequeoenxertoficassemaisinclinadoe demonstrou clinicamenteummelhorresultadopelamanobradePivot-Shift.Nãohouvediferenc¸ana isometricidadeenoresultadofuncionalfinalnocurtotempodeseguimentoavaliado.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Historically,theparametersoftunnelpositioningin single-bandreconstructionoftheanteriorcruciateligament (ACL) havebeenadjustedandmodifiedinsearchofanideal clini-calresult.Theisometricpositioninginthesagittalplanehas beenthemainconcernininitialintra-articularACL recons-tructions.Itwasdeterminedthattheisometriczoneonthe femurwouldbesmallerthanthatofthetibia,whichremains thesame forapointlocatedbothinthe anteriorand pos-terior edgeofACL insertion.1–3 Aneccentric positioning in
thetibia,i.e.,inthemostanteromedialportionofACL inser-tion,aswellasthepositioninginthecenterofACLinsertion, wasrecommendedforACLreconstructionbysomeauthors.4,5
Howelletal.,1 withthetranstibialtechnique,associatedthe
positioninginthecenterofACL insertiononthe tibiawith intercondylarroofimpingement.Therefore,foralongtime,it wasrecommendedthatthegraftwaspositionedinthe pos-teromedialinsertion areaon the tibiaand in theposterior insertionareaonthefemur.6–8
The concern with residual rotational instability in ACL reconstruction is more modern. Loh et al.9 demonstrated
thatfemoralpositioningat10o’clockpresentsamore effec-tiveresistancetorotationalloadsthanthepositioningat11 o’clock.Pinczewskiet al.6 correlatedthe radiographic
posi-tioningofthetunnelsandtheangleofthegraftwithclinical resultsandestablishedtheidealradiographicparametersfor abetterlong-termresult.Theyalsodemonstratedarelation
between verticalization ofthe graft and an increased inci-denceofpositivepivot-shiftandradiographicabnormalities.6
There are controversies regardingwhether the transtib-ialtechniquewouldallowforamorehorizontalpositioning ofthe femoraltunnel; many authors recommendthe two-incisiontechnique10 orcreatingthefemoraltunnelthrough
theanteromedialportal.Althoughseveralstudieshave corre-latedthepositioningofthefemoraltunnelwithclinicaland biomechanicresults,nostudiescorrelatingpositioningwith the isometricity obtainedintheintraoperativeperiodwere retrievedintheliterature.
This study aimed to compare the radiographic tunnel positioning,graftinclination,graftisometricityinthe intraop-erativeperiod,andthefinalfunctionalresultofsingle-band ACLreconstructionusingthetranstibialorthetwo-incision techniques.
Methods
Fig.1–(A,B)MeasurementofthefemoralandtibialtunnelinlateralX-rayinthetranstibialandtwo-incisiontechniques, respectively.
Patientsfromgroup1underwentsurgeryfromDecember 2009toDecember2010,andthosefromgroup2,from Decem-ber2010toOctober2011.
Theinclusioncriteriawere:patientswithnootherligament injuries; no mechanical axis alignment abnormalities; age 18–45yearsold;nocomplicationsduringthepost-operative period, such as arthrofibrosis and deep infection; no his-toryofpriorkneesurgeries,inaccordancewiththefreeand informedconsentform;andTegneractivitylevel≥4priorto theinjury.11–13
Theexclusioncriteriawere:patientswhoreported preg-nancy,leftthestudy,oraskedtobeexcluded;thosewhodid notreturn forthe X-raysand IKDCassessment;and those whodidnotfollowphysiotherapyrehabilitationinaccordance withtherehabilitationprotocol.Accordingtothesecriteria, eightpatientswereexcluded,sixfromgroup1andtwofrom group2.
All patients were assessedbetween eightto 22 months (meanof13)afterthesurgery.Twoorthopedicsurgeons(knee specialists)whohad notparticipatedinthesurgical proce-durewereaskedtoassess thepatients;thesurgicalwound wascoveredwithcrepebandagesduringexamination,sothat thesurgeonscouldnotidentifytheincisions.
Thestatisticaltestswere conductedusingasignificance levelof5%(p<0.05).
This study was approved by the institution’s Research EthicsCommitteeunderNo.1440/11.
Radiographicassessment
Theradiographicassessmentwasconductedwithunmarked X-rays,whichwereindependentlyexaminedbytwotrained authors/investigators; the measurements were compared
and,incaseofdisagreement,athirdtrainedinvestigatorwas consulted,toensurereliabilityintheradiographicanalyses.
X-raysweretakenbetweensixmonthsandtwoyearsafter thesurgery.Thefollowingradiographicviewswereusedfor the evaluation: anteroposterior (AP), lateral (L), and tunnel view with30◦ flexion.The positioningofthe center ofthe
femoraltunnelinthelateralX-raywasperformedby mea-suringthelengthoftheBlumensaat’sline;theanteriorand posterioredgesofthetunnelwereidentifiedandthecenter ofthefemoraltunnelwasdetermined.Next,thepositionof thecenterofthetunnelwasexpressedasapercentageofthe lengthoftheBlumensaat’slinefromitsanteriorlimit(Fig.1A andB).14,15
Thefemoraltunnelpositioningwasassessedatthe tunnel-viewX-rayasapercentageofthewidthofthetibialplateau from the medial edge, as described by Khalfayan et al.16
(Fig.2AandB).
Thepositioningofthetibialtunnelwasmeasuredatthe lat-eralX-ray;thelengthofthetibialplateauandtheanteriorand posterialedgesofthetunnelrelativetothetibialplateauwere determined.Thecenterofthetibialtunnelwasexpressedas apercentageofthelengthofthetibialplateau(Fig.1Aand B).17AttheAPX-ray,thetotallengthofthetibialplateauwas
measuredandthemedialandlateraledgesofthetunnelwere determined.Thepositionofthecenterofthetibialtunnelwas expressedasapercentagerelativetothetotallengthofthe tibialplateau(Fig.2AandB).
Theinclinationofthegraftwasmeasuredinaccordance withthemethodusedbyPinczewskiinAPtunnel-viewX-ray with30◦offlexion.6Theangleformedbythelinethatconnects
Fig.2–(A,B)Measurementofthefemoralandtibialtunnelpositioninginthetranstibialandtwo-incisiontechniques, respectively.
Surgicaltechnique
Thereconstructionusingthetranstibialtechniquewas per-formed through a small incision in the flexor tendons (semitendinosusandgracilis)insertionregion,withtheir har-vestingandpreparationofthequadruplegraft.Then,thetibial
tunnelwasmadewithhelpofaguide(Fig.4A).Theentryofthe tunnelwasadjacenttothemedialcollateralligament. Subse-quently,thefemoraltranstibialguidewaspositioned(Fig.4B) and thesurgeonsoughtthemostanatomicalpointfor cre-atingthefemoraltunnel.Aftermakingthetunnels,thegraft waspassedthroughtheminaretrogradefashion;itwasfirstly
Fig.4–(A,B)Tibialandfemoralguidesforthetranstibial technique.
fixedinthefemurwithaninterferencescrewthroughasmall lateral approach,and thenfixedinthe tibiawith theknee in30◦offlexion,discreetvalgusstress,anddiscreetexternal
rotationofthetibiawithanotherinterferencescrew. Subse-quently, the ligament tests(Lachman and anterior drawer) wereperformedtoassessstability.
The reconstruction through the two-incision technique (Chambat) was done in the same way as the previous technique; the only difference was in making the femoral tunnel,whichwasdrilledusingaoutside-inguide(Chambat) (Fig.5).10,18
Graftisometricityassessmentintheintraoperativeperiod
After the femoral fixation of the graft, repeated flexion-extensionofthekneewasperformedforitsaccommodation. Subsequently,isometricitywasassessedusingan intraopera-tivemaneuverstartingbyapplyingtractiononthedistalend ofthegraftonmaximumflexion.Athinmarkatthelevelofthe
Fig.5–Femoralguideusedinthetwo-incisiontechnique.
anterioredgeofthetibialtunnelwasmadeonthegraftwith methyleneblue.Thekneewasbroughttocompleteextension, whenwhichanewmarkwasmade.Withthehelpofaruler, theauthorsmeasuredwhetherornotthegraftmoved.The procedurewasconductedasquicklyaspossibletoavoid diffu-sionofthepigmentthroughthegrafttissue,inordertoensure betterprecisionofthemarking.
Clinical/functionalevaluation
IKDC, LysholmKneeScale,andTegner scorewereusedfor functionalandclinicalevaluation.11,12,19–22
Examinationwasperformedindependentlybytwo ortho-pedicsurgeons(kneespecialists).Theresultswerecompared; incaseofdisagreementathirdtrainedinvestigatorwas con-sultedtoensurereliabilityintheclinicalanalyses.
Statisticalanalysis
The Mann–Whitney U test was used for the comparisons betweengroups1and2regardingage,timebetweeninjury and surgery,tunnel positioning,graft thickness, graft incli-nationinthecoronalplane,isometricity,IKDC,Lachmanand pivot-shiftmaneuvers,andLysholmandTegnerscores.
The relation between the variables was analyzed with Spearman’scorrelationcoefficient.
StatisticalanalyseswereperformedwithStatisticaversion 8.0.
Thesignificancelevelwassetat5%(p<0.05).
Results
Therewasnodifferencebetweenbothgroupsregardingage (p=0.8),time betweeninjury and surgery(p=0.78), levelof activity (Tegner) before injury (p=0.62), and Lysholm score beforesurgery(p=0.61).
Onepatientfromgroup2presentedgraftruptureandwas excludedfromtheanalysesoffunctionalresults(IKDC, pivot-shiftandLachman exams,and post-operativeLysholm and Tegnerscores),andeightpatients(sixfromgroup1andtwo fromgroup2)didnotreturnforclinicalandradiographic eval-uations.
PositioningofthefemoraltunnelandtibialtunnelinAP andLX-rays
ThemeanpositioningofthefemoraltunnelintheAPX-ray ingroup1was54.6%(SD4.1)andingroup2,60.8%(SD4.5;
p=0.0004;Table1).
ThemeanpositioningofthefemoraltunnelintheLX-ray ingroup1was68.4%(SD10.9)andingroup2,58%(SD9.9;
p=0.0005;Table1).
Regarding the tibial tunnel, there was no difference betweenbothgroups.
Graftinclination
Ingroup1,meangraftinclinationwas19◦(SD3.7)andingroup
Table1–Meanvaluesoftunnelpositioning,expressed aspercentageandstandarddeviation(SD),ingroups1 and2.
Mean(SD) p-Value
(Mann–Whitney) Group1–
transtibial
Group2– two-incision
APfemoraltunnel(%) 54.6(4.1) 60.8(4.5) 0.0004 Lfemoraltunnel(%) 68.4(10.9) 58.0(9.9) 0.005 APtibialtunnel(%) 45.4(6.4) 45.2(4.9) 0.11 Ltibialtunnel(%) 43.5(9.3) 38.1(9.8) 0.12
AP,measurementperformedinanteroposteriorX-ray;L, measure-mentperformedinlateralX-ray.
Table2–Meanvaluesandstandarddeviation(SD)of graftinclinationandisometricityingroups1and2.
Mean(SD) p-Value
(Mann–Whitney) Group1–
transtibial
Group2– two-incision
Graftinclination(◦) 19.0(3.7) 27.2(5.7) 0.0005 Isometricity(mm) 0.96(0.8) 1.33(1.6) 0.69
Isometricityofthegraft
Therewasnodifferencebetweenbothgroups(Table2).
Functionalresults–IKDCandLysholm
TherewasnodifferencebetweenbothgroupsregardingIKDC (Table3),aswellaspost-operativeLysholmandTegnerscores (Table4).
AnalysisofLachmanandpivot-shiftmaneuvers
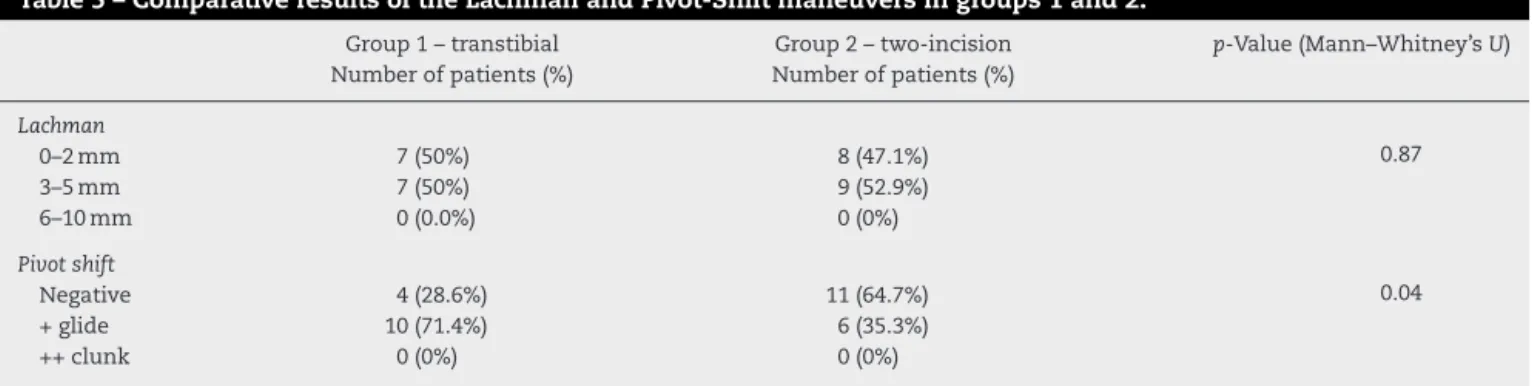
TherewasnodifferencebetweenbothgroupsforLachman maneuvers(p=0.87).
Group2presentedbetterresultsforpivot-shiftmaneuver whencomparedwithgroup1(p=0.04;Table5)
Correlationoftunnelpositioningwithfunctionalresults
Inbothgroups,theindividualparametersoftunnel position-ing (AP femoraltunnel, Lfemoral tunnel,AP tibialtunnel, L tibial tunnel) were not correlated (p>0.05) with func-tionalresults(IKDC,pivot-shiftandLachmanmaneuvers,and LysholmandTegnerscore).
Table3–ResultsoftheInternationalKnee
DocumentationComittee(IKDC)scoreingroups1and2.
Group1– transtibial
Group2– two-incision
p-Value (Mann–WhitneyU) Numberof
patients(%)
Numberof patients(%)
SubjectiveIKDC
A 12(85.7%) 11(64.7%) 0.16
B 2(14.3%) 4(23.5%)
C 0(0.0%) 2(11.8%)
IKDCrangeofmovement
A 10(71.4%) 6(35.3%) 0.09
B 3(21.4%) 11(64.7%)
C 1(7.2%%) 0(0.0%)
IKDCligamentexam
A 2(14.3%) 6(35.3%) 0.19
B 12(85.7%) 11(64.7%)
C 0(0.0%) 0(0%)
IKDCfinal
A 2(14.3%) 3(17.6%) 0.96
B 11(78.6%) 12(70.6%)
C 1(7.1%) 2(11.8%)
Obs:The“D”scorewasnotobservedinanyofthegroups.
Correlationofgraftinclinationinthecoronalplanewith functionalresults
Withingroup1,highergraftinclinationwassignificantly cor-relatedwithLysholmscore(r=0.62,p=0.02).
Within group 2, higher graft inclination was associated withbetterIKDCresultsandwassignificantlycorrelatedwith IKDCfunctionaltest(r=0.56,p=0.02).
Whenanalyzingbothgroupstogether,graftinclinationwas significantly correlated with pivot-shift maneuver (r=0.38,
p=0.04).
Correlationofisometricitywithtunnelpositioning, inclination,andfunctionalresults
Withingroup1,highergraftisometricitywasassociatedwith betterIKDCresultsandwassignificantlycorrelatedwith pivot-shift maneuver (r=0.59, p=0.03), functional test (hop test;
r=0.64,p=0.01),andfinalIKDC(r=0.67,p=0.009).
Withingroup2,highergraftisometricitywasonly signifi-cantlycorrelatedwithsubjectiveIKDC(r=0.58,p=0.01).
When analyzing bothgroups together, higher graft iso-metricity was significantlycorrelated withsubjective IKDC (r=0.53,p=0.02)andfunctionaltest(r=0.36,p=0.04).
Therewasnocorrelationofisometricitywithgraft inclina-tion(p>0.05).
Table4–Meanandstandarddeviation(SD)ofthepost-operativeLysholmandTegnerscoresingroups1and2.
Group1–transtibialmean(SD) Group2–two-incisionmean(SD) p-Value(Mann–Whitney’sU)
Post-operativeLysholmscore 96.6(4.5) 94.6(4) 0.09
Table5–ComparativeresultsoftheLachmanandPivot-Shiftmaneuversingroups1and2.
Group1–transtibial Group2–two-incision p-Value(Mann–Whitney’sU) Numberofpatients(%) Numberofpatients(%)
Lachman
0–2mm 7(50%) 8(47.1%) 0.87
3–5mm 7(50%) 9(52.9%)
6–10mm 0(0.0%) 0(0%)
Pivotshift
Negative 4(28.6%) 11(64.7%) 0.04
+glide 10(71.4%) 6(35.3%)
++clunk 0(0%) 0(0%)
Withingroups1and2andintheanalysisofbothgroups together, graft isometricity was not correlated with tunnel positioning(p>0.05).
Withingroups1and2andintheanalysisofbothgroups together,amongthepatientswithidealisometricity(<2mm), tunnel positioning was not statistically different from the otherpatients(p>0.05).
Discussion
The two-incision technique for ACL reconstructions was developed before the transtibial technique, which became moreusedduetotheconvenienceofasingleincision dur-ingthearthroscopicprocedure.18Currently,thetwo-incision
techniquehasregainedpopularity duetothepossibility of femoraltunnelpositioningregardlessoftheangleofthe tib-ialtunnel,aimingtopositionthegraft anatomically(atthe centeroftheproximalACLinsertion).10Thereare
controver-siesregardingwhetheritispossibletoanatomicallyposition thefemoraltunnelinthetranstibialtechnique,sinceinthe anatomicalpositioningofthetunnelthegraftistilted(more horizontal),hinderingitsachievementusingthistechnique.9
Inthepresentstudy,theauthorspreferredthetranstibial techniquetomakethefemoraltunnelduetoitsanatomical location.Thetibialguide waspositionedmoremedially,so thattheentryofthetunnelwasclosertothemedial collat-eralligament.23However,itwasobservedthatthepositioning
ofthefemoraltunnelwassignificantlydifferentcomparing bothtechniques,probably duetothedifficulties previously described.Inthetwo-incisiontechnique,thefemoraltunnel inAPX-rayswasmorelateral;inL,itwasmoreanterior;and intunnel-view,moreinclined.Theauthorsbelievethatthis positioningisindeedmoreanatomical.
The functional results did not demonstrate difference betweenbothtechniques.Nonetheless,intheisolated evalu-ationofthepivot-shiftmaneuver,thetwo-incisiontechnique presented significantly better results, possibly for better reproducingtheACLanatomy.Thebetterrotationalcontrol obtainedin the two-incision technique tookplace without compromisingthecontrolofanteroposteriorstability,which confirmswhathasbeenreportedintheliterature.24Tothebest
oftheauthors’knowledge,todate,onlybiomechanical25,26
andretrospective27studieshavedemonstratedthesuperiority
oftheanatomicalreconstructionregardingrotationalcontrol, andthishasnotyetbeenreportedinarandomizedclinical trial.
Foralongtime,inthetranstibialtechnique,isometricity wasconsideredfundamentaltoACLreconstruction;obtaining anisometricpointwasassociatedwithatunnelpositioningin theinsertionareaoftheposterolateralbandinthetibiaand anteromedialbandinthefemur.Withanatomical reconstruc-tion,thepositioninginthecenteroftheinsertionareagained importance.Regardinggraftisometricity,thepresentstudydid notobservestatisticallysignificantdifferencesbetweenboth techniques.Thisfindingisinagreementwithrecentstudies, inwhichtheglidingonmaximumextensionwassimilarin bothtechniques.28–30
Inbothgroups,graftinclinationwascorrelatedwith func-tional results;whenassessedtogether, thehigherthe graft inclination,thebetterthepivot-shiftresult.Thisconfirmsthe hypothesisthatanatomicalpositioningandhighergraft incli-nationleadstoahigherrotationalstability.
The authors believe that absence of graft isometricity maycauseslackeningafterrepetitivemovementsof flexion-extension. In the transtibial group, it was observed that patientswithworseisometricitypresentedworsefunctional results,eveninthepivot-shiftmaneuver.Inthetwo-incision group, worse isometricity wasonlycorrelated with subjec-tiveIKDC;theauthorsbelievethatitisduetotheanatomical positioningofthegraftinthistechnique.
Thelimitationsofthestudyareassociatedwithitssmall sampleandshortfollow-uptimeforclinicalevaluations. KT-1000evaluationswerenotperformed.
Conclusions
The two-incisiontechnique allowedforamore lateral and anterior positioning of the femoral tunnel, and for higher graftinclination,presentingbetterclinicalresultinthe pivot-shiftmaneuver.Nodifferencesinisometricityandfunctional resultswereobservedintheshortfollow-upperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
r
e
f
e
r
e
n
c
e
s
1. HowellSM,ClarkJA,FarleyTE.Arationaleforpredicting anteriorcruciategraftimpingementbytheintercondylar roof.Amagneticresonanceimagingstudy.AmJSportsMed. 1991;19(3):276–82.
2. BradleyJ,FitzPatrickD,DanielD,ShercliffT,O’ConnorJ. Orientationofthecruciateligamentinthesagittalplane.A methodofpredictingitslength-changewithflexion.JBone JointSurgBr.1988;70(1):94–9.
3. SidlesJA,LarsonRV,GarbiniJL,DowneyDJ,MatsenFA3rd. Ligamentlengthrelationshipsinthemovingknee.JOrthop Res.1988;6(4):593–610.
4. GillquistJ,OdenstenM.Arthroscopicreconstructionofthe anteriorcruciateligament.Arthroscopy.1988;4(1):5–9. 5. GoodL,OdenstenM,GillquistJ.Precisioninreconstructionof
theanteriorcruciateligament.Anewpositioningdevice comparedwithhanddrilling.ActaOrthopScand. 1987;58(6):658–61.
6. PinczewskiLA,SalmonLJ,JacksonWF,vonBormannRB, HaslamPG,TashiroS.Radiologicallandmarksforplacement ofthetunnelsinsingle-bundlereconstructionoftheanterior cruciateligament.JBoneJointSurgBr.2008;90(2):172–9. 7. JacksonDW,GasserSI.TibialtunnelplacementinACL
reconstruction.Arthroscopy.1994;10(2):124–31.
8. MorganCD,KalmanVR,GrawlDM.Definitivelandmarksfor reproducibletibialtunnelplacementinanteriorcruciate ligamentreconstruction.Arthroscopy.1995;11(3):275–88. 9. LohJC,FukudaY,TsudaE,SteadmanRJ,FuFH,WooSL.Knee
stabilityandgraftfunctionfollowinganteriorcruciate ligamentreconstruction:comparisonbetween11o’clockand 10o’clockfemoraltunnelplacement.2002RichardO’Connor Awardpaper.Arthroscopy.2003;19(3):297–304.
10.GarofaloR,MouhsineE,ChambatP,SiegristO.Anatomic anteriorcruciateligamentreconstruction:thetwo-incision technique.KneeSurgSportsTraumatolArthrosc.
2006;14(6):510–6.
11.TegnerY,LysholmJ.Ratingsystemsintheevaluationofknee ligamentinjuries.ClinOrthopRelatRes.1985;(198):43–9. 12.MarxRG,JonesEC,AllenAA,AltchekDW,O’BrienSJ,Rodeo
SA,etal.Reliability,validity,andresponsivenessoffourknee outcomescalesforathleticpatients.JBoneJointSurgAm. 2001;83(10):1459–69.
13.LeeDY,KarimSA,ChangHC.Returntosportsafteranterior cruciateligamentreconstruction–areviewofpatientswith minimum5-yearfollow-up.AnnAcadMedSingapore. 2008;37(4):273–6.
14.BernardM,HertelP,HornungH,CierpinskiT.Femoral insertionoftheACL.Radiographicquadrantmethod.AmJ KneeSurg.1997;10(1):14–21.
15.ZantopT,WellmannM,FuFH,PetersenW.Tunnelpositioning ofanteromedialandposterolateralbundlesinanatomic anteriorcruciateligamentreconstruction:anatomicand radiographicfindings.AmJSportsMed.2008;36(1):65–72. 16.KhalfayanEE,SharkeyPF,AlexanderAH,BrucknerJD,Bynum
EB.Therelationshipbetweentunnelplacementandclinical resultsafteranteriorcruciateligamentreconstruction.AmJ SportsMed.1996;24(3):335–41.
17.StäubliHU,RauschningW.Tibialattachmentareaofthe anteriorcruciateligamentintheextendedkneeposition. Anatomyandcryosectionsinvitrocomplementedby magneticresonancearthrographyinvivo.KneeSurgSports TraumatolArthrosc.1994;2(3):138–46.
18.HarnerCD,MarksPH,FuFH,IrrgangJJ,SilbyMB,MengatoR. Anteriorcruciateligamentreconstruction:endoscopy versustwo-incisiontechnique.Arthroscopy.1994;10(5): 502–12.
19.IrrgangJJ,HoH,HarnerCD,FuFH.UseoftheInternational KneeDocumentationCommitteeguidelinestoassess outcomefollowinganteriorcruciateligament reconstruction.KneeSurgSportsTraumatolArthrosc. 1998;6(2):107–14.
20.HeftiF,MüllerW,JakobRP,StäubliHU.Evaluationofknee ligamentinjurieswiththeIKDCform.KneeSurgSports TraumatolArthrosc.1993;1(3–4):226–34.
21.KocherMS,SteadmanJR,BriggsK,ZurakowskiD,SterettWI, HawkinsRJ.Determinantsofpatientsatisfactionwith outcomeafteranteriorcruciateligamentreconstruction.J BoneJointSurgAm.2002;84(9):1560–72.
22.PeccinMS,CiconelliR,CohenM.Questionárioespecíficopara sintomasdojoelhoLysholmKneeScoringScale:traduc¸ãoe validac¸ãoparaalínguaportuguesa.ActaOrtopBras. 2006;14(5):268–72.
23.RueJP,GhodadraN,BachBRJr.Femoraltunnelplacementin single-bundleanteriorcruciateligamentreconstruction:a cadavericstudyrelatingtranstibiallateralizedfemoraltunnel positiontotheanteromedialandposterolateralbundle femoraloriginsoftheanteriorcruciateligament.AmJSports Med.2008;36(1):73–9.
24.HarnerCD,PoehlingGG.Doublebundleordoubletrouble? Arthroscopy.2004;20(10):1013–4.
25.ScoppJM,JasperLE,BelkoffSM,MoormanCT3rd.Theeffect ofobliqúefemoraltunnelplacementonrotationalconstraint ofthekneereconstructedusingpatellartendonautografts. Arthroscopy.2004;20(3):294–9.
26.DriscollMD,IsabellGPJr,CondittMA,IsmailySK,JupiterDC, NoblePC,etal.Comparisonof2femoraltunnellocationsin anatomicsingle-bundleanteriorcruciateligament
reconstruction:abiomechanicalstudy.Arthroscopy. 2012;28(10):1481–9.
27.KimMK,LeeBC,ParkJH.Anatomicsinglebundleanterior cruciateligamentreconstructionbythetwoanteromedial portalmethod:thecomparisonoftransportalandtranstibial techniques.KneeSurgRelatRes.2011;23(4):213–9.
28.LeeJS,KimTH,KangSY,LeeSH,JungYB,KooS,etal.How isometricaretheanatomicfemoraltunnelandtheanterior tibialtunnelforanteriorcruciateligamentreconstruction? Arthroscopy.2012;28(10):1504–12.
29.YonetaniY,ToritsukaY,YamadaY,IwahashiT,YoshikawaH, ShinoK.Graftlengthchangesinthebi-socketanterior cruciateligamentreconstruction:comparisonbetween isometricandanatomicfemoraltunnelplacement. Arthroscopy.2005;21(11):1317–22.