SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Comparative
study
on
three
surgical
techniques
for
intra-articular
calcaneal
fractures:
open
reduction
with
internal
fixation
using
a
plate,
external
fixation
and
minimally
invasive
surgery
夽
Missa
Takasaka,
Cintia
Kelly
Bittar,
Fernando
Saddi
Mennucci
∗,
Carlos
Augusto
de
Mattos,
José
Luís
Amim
Zabeu
HospitaleMaternidadeCelsoPierro,PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received27April2015 Accepted10July2015 Availableonline9April2016
Keywords:
Calcaneus/injuries Calcaneus/surgery Comparativestudy
a
b
s
t
r
a
c
t
Objective:Toevaluate,compareandidentifythesurgicaltechniquewithbestresultsfor treatingintra-articularcalcanealfractures, takingintoaccountpostoperativeoutcomes, complicationsandscoringintheAofasquestionnaire.
Methods:This wasa retrospectivestudy on54 patientswith fracturesofthecalcaneus whounderwentsurgerybetween2002and2012bymeansofthefollowingtechniques:(1) openreductionwithextendedL-shapedlateralincisionandfixationwithdouble-Hplateof 3.5mm;(2)openreductionwithminimalincisionlateralapproachandpercutaneous fixa-tionwithwiresandscrews;and(3)openreductionwithminimalincisionlateralapproach andfixationwithadjustablemonoplanarexternalfixator.
Results:Patientstreatedusingalateralapproach,withfixationusingaplatehadamean Aofasscoreof76points;thosetreatedthroughaminimalincisionlateralapproachwith screwandwirefixationhadameanscoreof71points;andthosetreatedthrougha mini-malincisionlateralapproachwithanexternalfixatorhadameanscoreof75points.The threesurgicaltechniqueswereshowntobeeffectivefortreatingintra-articularcalcaneal fractures,withoutanyevidencethatanyofthetechniquesbeingsuperior.
Conclusion:Intra-articularcalcanealfracturesarecomplexandtheirtreatmentshouldbe individualizedbasedonpatientcharacteristics,typeoffractureandthesurgeon’s experi-encewiththesurgicaltechniquechosen.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheServiceofOrthopedyandTraumatology,HospitaleMaternidadeCelsoPierro,PontifíciaUniversidadeCatólica deCampinas(PUC-Campinas),Campinas,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.S.Mennucci). http://dx.doi.org/10.1016/j.rboe.2016.04.002
rev bras ortop.2016;51(3):254–260
255
Estudo
comparativo
entre
três
técnicas
cirúrgicas
para
fraturas
intra-articulares
de
calcâneo:
reduc¸ão
aberta
e
fixac¸ão
interna
com
placa,
fixac¸ão
externa
e
minimamente
invasiva
Palavras-chave: Calcâneo/lesões Calcâneo/cirurgia Estudocomparativo
r
e
s
u
m
o
Objetivo: Avaliar,comparareidentificaratécnicacirúrgicacommelhorresultadoparao tratamentodefraturasintra-articularesdocalcâneo,levandoemconsiderac¸ãoevoluc¸ão pós-operatória,complicac¸õesepontuac¸ãonoquestionárioAofas.
Métodos: Estudoretrospectivode54pacientescomfraturasdecalcâneooperadosentree 2002e2012comastécnicas1)reduc¸ãoabertacomincisãolateralalargadaem“L”efixac¸ão complacaduplo“H”de3,5mm,2)reduc¸ãoabertaporincisãolateraleconômicaefixac¸ão percutâneacomfioseparafusose3)reduc¸ãoabertaporincisãolateraleconômicaefixac¸ão comfixadorexternomonoplanarregulável.
Resultados: Pacientestratadospelaviadeacessolateralefixac¸ãocomplacativerammédia de76pontosnaescalaAofas,empacientestratadospelaviadeacessolateraleconômica efixac¸ãocomfioseparafusoamédiafoide71enospacientestratadoscomviadeacesso lateralefixadorexternofoide75pontos.Astrêstécnicascirúrgicasdemostraram-seefetivas notratamentodafraturaintra-articulardocalcâneo,semevidênciadesuperioridadedeuma técnicasobreasdemais.
Conclusão: :Afraturaintra-articulardocalcâneoéumafraturacomplexaeseutratamento deveserindividualizado,baseadonascaracterísticasdopaciente,notipodefraturaena experiênciadocirurgiãocomatécnicaoperatóriaescolhida.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Calcanealfracturescorrespondtoapproximately1%to2%of allthefracturesofthehumanbodyandconstitutenearly60% oftarsalbonesfractures.Theygenerallyfollowhigh-energy axialtraumas,suchasfallfromheightormotoraccidents.
Accordingtothe currentliterature,60% to75% ofthese fracturesareconsideredtobedisplacedandintra-articular,1–3 which evidences the difficulty of the treatment. They can causegreatdisabilityduetopainandchronicstiffness,in addi-tiontohindfootdeformities.Thesefracturesarecharacterized clinicallybypoorfunctionalresultsduetotheircomplexity.
Approximately80%to90%ofthecalcanealfractures hap-peninmalesbetween21and40years,mostlyinindustrial workers.Severalauthors4–7havereportedthatthe rehabilita-tionofthesefracturescantakefromninemonthstoseveral years,whichimplicatesgreateconomicburdenonsociety.
Sincetheearly1980s,thetreatmentofchoicefordisplaced and intra-articular calcaneal fractures was open reduction with internal fixation; however, soft tissue complications, suchassurgicaldehiscenceandinfection,canoccurinupto 30%ofthepatients.8–10
Inanattempttoreducecomplicationrates,newsurgical techniquesemerged,suchasminimallyinvasiveincisionand percutaneousfixation,whichcauselessinjurytothetissues andreducetheincidenceofsofttissuecomplications.10,11
Despite the modern surgical techniques and the con-siderablenumberofstudies intheliterature,11–13 calcaneal fracturesandtheirbesttreatmentmethodremainanenigma fororthopedicsurgeons.
Thisstudyaimedtoassess,compare,andidentifythe sur-gicaltechniquewiththebestclinicalfunctionalresultinthe treatment ofdisplaced and intra-articular calcaneous frac-ture, including (1) open reduction withextended L-shaped lateralincisionandfixationwith3.5-mmdouble-Hplate;(2) open reductionwithminimalincisionlateral approachand percutaneous fixationwithwires and screws;and (3) open reductionwithminimalincisionlateralapproachandfixation withadjustablemonoplanarexternalfixator.
Material
and
methods
ThestudyprotocolwasapprovedbytheResearchEthics Com-mitteeunderNo.064/11.
Thiswasaretrospectivestudythatanalyzedthemedical chartsof54patientswith60calcanealfractures,operatedon between2002and2012,inanuniversityhospitalin Campi-nas,SP,Brazil,byasingleorthopedicsurgeon(foot-and-ankle specialist).Theinclusioncriteriacomprisedskeletallymature individuals withdeviatedintra-articularcalcaneal fractures classified asSanderstypeIIand III,who were operatedon withoneofthefollowingsurgicaltechniques:
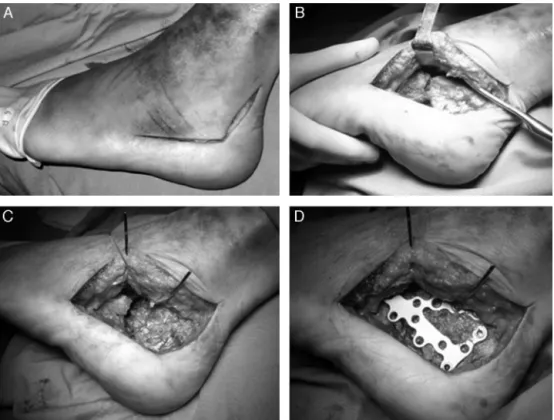
Fig.1–WidelateralapproachasdescribedbySeligson(A);reductionofthefracturebydirectvisualizationwithperiosteum elevator(B);temporaryfixationofthereductionwithKirschner1.6wire(C);internalfixationwith3.5-mmcalcaneusplate (D).
rev bras ortop.2016;51(3):254–260
257
Fig.3–Exampleofcalcanealfracturetreatedwithminimalincisionlateralapproachandfixationwithpinsandscrews.(A) Minimalincisionlateralapproach;(BandC)post-operativeresult.
fibularistendons,itispushedoutanteriorlytoexhibitthe lateralaspectofthecalcaneusandthecalcaneocuboidand subtalarjoints.Thefractureisthenreducedandfixedwith a3.5-mmcalcaneusimplant(Figs.1and2).
2. Mini-incisionandfixationwiththreadsandscrews:lateral 3-to5-cmincisiondirectlyabovethetarsalsinus.Divulsion ofthesofttissues,payingcarefulattentiontothefibularis tendons.Thejointfractureisreducedusingdelicate fine-tipchisels.Atemporaryfixationisperformedusing1.6-mm Kirschnerwiresinthefragments,formaintenanceofthe reduction,anddefinitefixationisachievedwithcannulated 3.5-or4.5-mmscrews(Fig.3).
3. Mini-incisionandmonoplanarexternalfixator:lateral 3–5-cm incision directly abovethe tarsalsinus. Divulsionof the soft tissues,payingcarefulattention tothe fibularis tendonsandthesuralnerve.Thejointfractureisreduced usingdelicatefine-tipchisels.Atemporaryfixationis per-formed using1.6-mm Kirschnerwiresin thefragments, for maintenanceof the reduction.Two Schanz pins are insertedinthecalcaneusbelowthejointsurfaceofthe sub-talarregion,twopinsareinsertedintheposteriorregionof thecalcaneusand,finally,twopinsareinsertedinthe ante-riorregion.Theexternalfixatorisblocked.Thenthemain and verticalrails aredistracteduntilproperreductionis visualizedunderfluoroscopy(Fig.4).
Post-operatively,earlymobilizationoftheankleand sub-talarjointsisstimulatedinthefirstpost-operativeweek.The suturesareremovedtwoweeksafterthesurgery.Forpatients operatedwiththeexternalfixationtechnique,partialloadis initiatedafterfour weeks; totalload starts ateightweeks,
Table1–Patientsoperatedwitheachsurgicaltechnique.
Surgicaltechnique Numberof patients
Numberof fractures
L-shapedincisionandplate fixation
20 23
Lateralmini-incisionandfixation withthreadsandscrews
27 27
Adjustablemonoplanarfixator 7 10
togetherwiththeremovalofthefixator.Inothertechniques, partialloadisinitiatedintheeighthpost-operativeweek.All patients undergopost-operativeoutpatientfollow-up forat leasttwoyears.
Skeletally immaturepatients, those withcalcaneal frac-turesclassifiedasSanderstypesI andIV,andthosewhohad undergonepriorfootsurgerywerenotincluded.
Procedures
Fig.4–Exampleoffracturetreatedwithminimalincisionlateralapproachandfixationwithmonoplanarexternalfixator.
BilateralX-raysinlateralandaxialviewsweretaken preop-eratively,aswellasintheimmediateandlatepost-operative. TheBöhlerandGissaneanglesweremeasured.Thepatients respondedtotheAmericanOrthopedicFootandAnkleSociety (AOFAS)14andJohnson15 questionnaires,andearlyand late surgicalcomplicationswerealsorecorded.TheAOFAS ques-tionnairemeasuresthesubjectivescaleofpain,footfunction, andthealignmentofthefootandankle,withthefollowing variables:levelofactivity(basicorrecreational),walked dis-tance,abilitytowalkindifferentsurfaces,gaitabnormality, footand hindfootmotion(flexion-extensionand inversion-eversion),andanklehindfootstability.
Johnson’squestionnaireassessescomplicationsand sub-jective satisfaction of the patient: completely satisfied, satisfiedwithminimalrestrictions,satisfiedwithhigh restric-tions,anddissatisfied.
Thegoalwastoassesswhichofthefollowingsurgical tech-niquespresentedthebestresultinthetreatmentofdisplaced andintra-articularcalcaneousfracture:L-shapedlateral inci-sionandfixationwithplate;mini-lateralincisionandfixation withwiresand screws; and adjustablemonoplanarfixator. TheStudent’st-testforcomparisonofmeans,withunknown anddifferentvariances,wasusedforeachpairofmethods.
Thus, the following were compared: (1) if the L-shaped lateralincisionandfixationwithplatewasequaltothe mini-lateralincisionandfixationwithwiresandscrews;(2)ifthe L-shapedlateralincisionandfixationwithplatewasequalto theadjustablemonoplanarfixator;and(3)ifthemini-lateral incisionandfixationwithwiresandscrewswasequaltothe adjustable monoplanar fixator. The answes for the AOFAS questionnairefromeachpatientcomprisedthecollecteddata.
Results
Of20patientstreatedbylateralaccessroutewithplate fixa-tion,16walkedwithoutrestrictions(80%),twolimped(10%), andtwoneededcrutches(10%).Themeanscoreof76(range: 62 to94)wasobtainedintheAOFASscale,inwhich excel-lentresultsrangefrom90to100points.Goodresultsrange from80to89;regular,from70to79;andbad,below69.The meanpost-operativeBöhleranglewas22◦ (range:12to32◦) andthemeanGissaneanglewas129◦(range:100to132◦); nor-malvaluesrangefrom20◦and40◦forthefirstangle,andare approximately100◦forthesecond.16
Ofthe 27 patientstreated withminimal incision lateral approach and minimal fixation, 24 walked without limita-tions, two limped, and one needed crutches. All patients presented difficulty to walk in uneven terrain. The mean AOFASscorewas71points(range:60to90).Themean post-operativeBöhlerangleinthesepatientswas18◦(range:6to 40◦)andthemeanGissaneanglewas88◦(range:76to102◦).
Ofthesevenpatientswhoweretreatedwithminimal inci-sionlateralapproachandexternalfixation,sixwalkedwithout limitationsandonepresentedlimping.ThemeanAOFASscore was75points(range:63to87).Themeanpost-operative Böh-leranglewas17.8◦(range:0to32◦)andthemeanGissaneangle was103◦(range:100to126◦).
rev bras ortop.2016;51(3):254–260
259
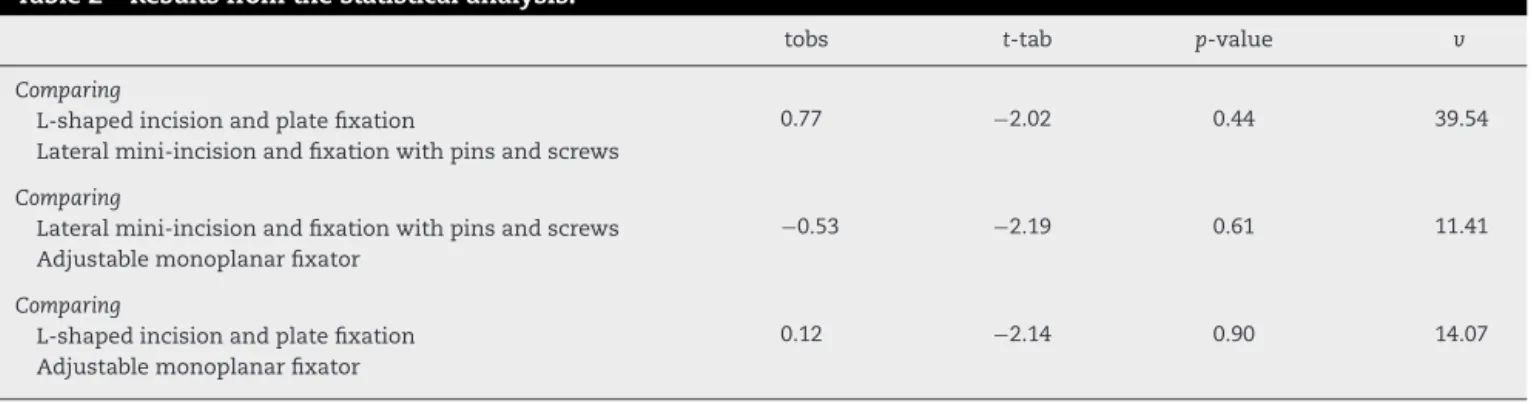
Table2–Resultsfromthestatisticalanalysis.
tobs t-tab p-value v
Comparing
L-shapedincisionandplatefixation 0.77 −2.02 0.44 39.54 Lateralmini-incisionandfixationwithpinsandscrews
Comparing
Lateralmini-incisionandfixationwithpinsandscrews −0.53 −2.19 0.61 11.41 Adjustablemonoplanarfixator
Comparing
L-shapedincisionandplatefixation 0.12 −2.14 0.90 14.07 Adjustablemonoplanarfixator
Discussion
Thecomplexcalcaneus anatomy,itsspongybonestructure with thin cortical, articular and displaced fractures, high-energytrauma,andlittlesofttissuecoveragecontributetothe difficultyinhandlingitsfractures.17–19
In developed countries, most of the displaced intra-articular calcaneal fractures are treated bymeans ofopen reductionvialateralapproachandfixationwithplateand 3.5-mmscrew. This techniqueoffers good visualization ofthe fracture, atthe cost ofgreater damagetothe soft tissues, whichincreasestheriskofnecrosis,surgicaldehiscence,and infection.Thus,severalsurgeonshavebeensearchingfor min-imallyinvasivesurgicaltechniqueswithlessdamagetothe softtissues.20,21
Inthegroupassessed,mostpatientsweremalesatworking age(meanof40years)andallcaseshadaxialtraumadueto fallfromheightasthetraumamechanism.
Inthe analysisoftheradiographic resultsoftheBohler andGissaneanglemeasurements,itwasobservedthatinthe openreductionwithplateandfixationwithplateandscrews andintheopenreduction(minimalincision)with percuta-neousfixationgroups,itwaspossibletorestoretheanglesin 100%ofthecases,whereas intheopenreduction(minimal incision)withadjustablemonoplanarexternalfixatorgroup itwasonlypossibletorestoretheBohleranglein40%ofthe cases.Meanwhile,allvaluesfortheGissaneanglewerearound thereferencevalue.Therecanbeasmallvariancein measur-ingtheseangles,assmallrotationsduringtheradiographic examinationmayinfluencetheobtainedvalues,andalsodue totheprecisionofthegoniometerused.Nevertheless,these measurementswerestandardizedandperformedbyan expe-riencedprofessional.
AccordingtotheJohnsonscore,nopatientwasshownto becompletelysatisfiednorcompletelydissatisfiedwithany oftheusedtechniques.Thiscanbeconsideredapositivefact, duetothetypicalclinicalevolutionofcalcanealfractures.
As for the AOFAS questionnaire, it was observed that regarding the minimally invasive technique with percuta-neous fixation, 7.4% of the patients presented excellent results;51.8%,good;29.6%,fair;andonly11.1%oftheresults wereconsideredpoor.Regardingtheminimallyinvasive tech-niquewithexternalfixation(monoplanaradjustablefixator), thequestionnaireresultsappointed20% goodresults; 60%, fair; and 20%, poor. In the literature, good and excellent resultscanvarybetween42%and62%withtheconventional
Table3–ResultsfromtheAOFASscale.
Surgicaltechnique/AOFAS Mean Variation
L-shapedincisionandplate fixation
76 62–94
Minimalincisionlateral approachwithpinsand screws
71 60–90
Adjustablemonoplanar fixator
75 63–87
technique of open reduction and fixation using plate and screws. This demonstrates anadvantage ofthe mini-open reductionwithpercutaneousfixationcomparingtotheother techniques,asitpresented65.2%goodandexcellentresults, whichwasabovetheobservedmean(Table3).
Regardingthecomplications,atopicofhighrelevancefor thechoiceofthedefinitetreatment,thepresentstudy demon-stratedthatinthegrouptreatedwithmini-openreductionand percutaneousfixation,therewerenosofttissuecomplications suchasnecrosis,dehiscence,tendinitis,ornervousinjuries, whichcanreachfrom27%to33%ofthecasesintheliterature. Inthe externalfixationwithadjustablemonoplanar fixator group,onepatient(14.2%)presentedsofttissueinfection.In the grouptreatedwiththeconventional techniqueofopen reductionandfixationwithplate andscrews,four patients (20%)presentedthefollowingcomplications:infection(25%), skinnecrosis(50%),andsuralnerveneuroma(25%).
The literature indicates that approximately 80% of the patients who undergo the conventional surgical technique returntowork.22,23Thepresentstudydemonstratedthat,with theminimallyinvasivetechniqueandpercutaneousfixation, allpatientsreturnedtotheirworkactivities.Ofthepatients treated withthe conventional technique, 100%returned to theirworkactivities;however,50%ofthemresumeddifferent activities.
Thediscrepancyfoundintheliteraturebetweentheresults obtainedwiththeconventionaltechniqueofL-shapedaccess andtheminimallyinvasivetechniquesmaybeexplainedby thefactthatthelattercauseslessmorbidity,sincetheyare lessaggressivecausinglesssofttissuesdamage.
thephysicalandmentalstateofthepatient, andthe pres-enceofcomorbidities,suchassmokinganddiabetesmellitus, whichdirectlyinfluencethehealingprocessandcanincrease theriskofsurgicalcomplications.Theliteratureshowsthat the learning curve for the treatment with open reduction andfixationfordisplacedintra-articularcalcaneusfractures isaround35–50surgeries.24Therefore,thesurgeon’s experi-encemustalsobeconsideredwhendecidingthebestsurgical technique.
Conclusions
In the face ofaninternational discussion about the effec-tivenessofminimallyinvasivetechnique,thisstudyproved theefficiencyofsuchtechniquesanddemonstratedthat,in addition to that, they are correlated with lower morbidity andbetterqualityoflifeofthepatients,findings thathave alreadybeenobservedintheliterature.However,thepresent studydidnotdemonstrateastatisticalsuperiorityofthe min-imallyinvasivetechniquewithpercutaneousfixationoverthe othertechniques.Studieswithahighernumberofpatientsare needed,consideringthesmallnumberofrandomizedstudies comparingthesetechniques.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SandersR.Displacedintra-articularfracturesofthe calcaneus.JBoneJointSurgAm.2000;82(2):225–50. 2. BeschL,SchmidtI,MuellerM,Daniels-WredenhagenM,
HilgertRE,VarogaD,etal.Abiomechanicalevaluationto optimizetheconfigurationofahingedexternalfixatorforthe primarytreatmentofseverelydisplacedintraarticular calcaneusfractureswithsofttissuedamage.JFootAnkle Surg.2008;47(1):26–33.
3. GeelCW,FlemisterASJr.Standardizedtreatmentof intraarticularcalcanealfracturesusinganobliquelateral incisionandnobonegraft.JTrauma.2001;50(6):1083–9. 4. KinnerBJ,BestR,FalkK,ThonKP.Isthereareliableoutcome
measurementfordisplacedintra-articularcalcaneal fractures?JTrauma.2002;53(6):1094–101.
5. PhippE.Intra-articularfracturesofthecalcaneum:whysuch controversy?Injury.1997;28(4):247–59.
6. RoukisTS,WünschelM,LutzHP,KirschnerP,ZgonisT. Treatmentofdisplacedintra-articularcalcanealfractures withtriangulartube-to-barexternalfixation:long-term
clinicalfollow-upandradiographicanalysis.ClinPodiatrMed Surg.2008;25(2):285–99.
7.AliAM,ElsaiedMA,ElmoghazyN.Managementofcalcaneal fracturesusingtheIlizarovexternalfixator.ActaOrthopBelg. 2009;75(1):51–6.
8.OznurA,KomurcuM,MarangozS,TasatanE,AlparslanM, AtesalpAS.Anewperspectiveonmanagementofopen calcaneusfractures.IntOrthop.2008;32(6):785–90.
9.HuangP,HuangH,ChenTB,ChenJC,LinYK,ChengYM,etal. Openreductionandinternalfixationofdisplaced
intra-articularfracturesofthecalcaneus.JTrauma. 2002;52(5):946–50.
10.BarlaJ,BuckleyR,McComarckR,PateG,LeightonR,PetrieD, etal.Displacedintra-articularcalcanealfractures:long-term outcomeinwomen.FootAnkleInt.2004;25(12):853–6. 11.WestphalT,PiatekS,HalmJ-P,SchubertS,WincklerS. Outcomeofsurgicallytreatedintraarticularcalcaneus fractures–SF-36comparedwithAofasandMFS.ActaOrthop Scand.2004;75(6):750–5.
12.BeschL,WaldschmidtJS,Daniels-WredenhagenM,VarogaD, MuellerM,HilgertRE,etal.Thetreatmentofintra-articular calcaneusfractureswithseveresofttissuedamagewitha hingedexternalfixatororinternalstabilization:long-term results.JFootAnkleSurg.2010;49(1):8–15.
13.BareiD,BellabarbaC,SangeorzeanB,BenirschkeS.Fractures ofthecalcaneus.OrthopClinNorthAm.2002;33(1):263–85. 14.SandersR,GregoryP.Operativetreatmentofintra-articular
fracturesofthecalcaneus.OrthopClinNorthAm. 1995;26(2):203–14.
15.BucholzRW,HeckmanJD.RockwoodeGreen.Fraturasem adultos.5ed.SãoPaulo:Manole;2006.
16.MonseyR,LevineB,TrevinoS,KristiansenT.Operative treatmentofacutedisplacedintra-articularcalcaneus fractures.FootAnkleInt.1995;16(2):57–63.
17.RammeltS,AmlangM,BarthelS,ZwippH.
Minimally-invasivetreatmentofcalcanealfractures.Injury. 2004;35Suppl.2:SB55–63.
18.AsikM,SenC.Surgicalmanagementofintraarticular fracturesofthecalcaneus.ArchOrthopTraumaSurg. 2002;122(6):354–9.
19.MurachovskyJ,MartinelliM,FerreiraRC,FonsecaFilhoF. Fraturaarticulardocalcâneo:resultadoclínicoefuncionaldo tratamentocirúrgico.RevBrasOrtop.2000;35(8):314–24. 20.BurdeauxBD.Fracturesofthecalcaneus:openreductionand
internalfixationsfromthemedialside:a21-yearprospective study.FootAnkleInt.1997;18(11):685–92.
21.ZwippH,RammeltS,BarthelS.Calcanealfractures–open reductionandinternalfixation(ORIF).Injury.2004;35Suppl. 2:SB46–54.
22.DooleyP,BuckleyR,ToughS,McComarckB,PateG,Leighton R,etal.Bilateralcalcanealfractures:operativeversus nonoperativetreatment.FootAnkleInt.2004;25(2):47–52. 23.LimEVA,LeungJP.Complicationsofintraarticularcalcaneal
fractures.ClinOrthop.2001;(391):7–16.