w w w . r b o . o r g . b r
Original
Article
Evaluation
of
the
results
from
arthroscopic
surgical
treatment
of
rotator
cuff
injuries
in
patients
aged
65
years
and
over
夽
Alberto
Naoki
Miyazaki
∗,
Luciana
Andrade
da
Silva,
Pedro
Doenux
Santos,
Sergio
Luiz
Checchia,
Carina
Cohen,
Taís
Stedile
Busin
Giora
FaculdadedeCiênciasMédicasdaSantaCasaSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25April2014 Accepted7July2014 Availableonline16June2015
Keywords:
Rotatorcuff Arthroscopy Elderlypeople
a
b
s
t
r
a
c
t
Objectives: Toevaluate the results from arthroscopic surgical treatment of rotator cuff injuriesinpatientsaged65yearsandover.
Methods:Between 1998 and 2009, 168 patients underwent operations. Five cases were excluded.Theremaining163patientswerestratifiedaccordingtotheiragegroup:65–69 years(49.1%),70–74(26.4%)and75yearsandover(24.5%).Theirmeanagewas71years (range:65–83).Therewere63malepatients(38.7%).Themeanlengthoftimewithpain, fromtheonsetofsymptomstothesurgery,was23months(range:2daysto240months). Sixty-twopatients(38%)reportedhistoriesoftraumaand26(16%)reportedthattheirpain worsenedthroughexertion.
Results:FromtheUCLAcriteria,80.4%oftheresultswereexcellent,16%good,1.8%fairand 1.8%poor.Complicationsoccurredin11%.Thefinalclinicalresultdidnotshowany correla-tionwithageprogression,injurysizeortendonsaffected.However,therewasasignificant association(p<0.001)betweenthepresenceoftraumaandlargerinjuries.Thelengthoftime betweentheonsetofsymptomsandthesurgicalprocedurehadasignificantrelationship (p<0.027)withthepostoperativeresults:thelongerthistimewas,theworsetheresults were.
Conclusion: Arthroscopictreatmentofrotatorcuff injuriesinpatientsaged65yearsand overpresentedexcellentandgoodresultsin96.4%ofthecases,accordingtotheUCLA assessment,withalowcomplicationrate.Advancedagedidnotshowanyinfluenceonthe postoperativeclinicalevolution,buttheearlierthesurgicaltreatmentwasinstituted,the bettertheresultswere.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedintheShoulderandElbowGroup,DepartmentofOrthopedicsandTraumatology,FaculdadedeCiênciasMédicasda SantaCasaSãoPaulo,FernandinhoSimonsenWing(DOT–FCMSCSP).
∗ Correspondingauthor.
E-mail:[email protected](A.N.Miyazaki). http://dx.doi.org/10.1016/j.rboe.2015.06.001
Avaliac¸ão
dos
resultados
do
tratamento
cirúrgico
artroscópico
das
lesões
do
manguito
rotador
em
pacientes
com
65
anos
ou
mais
Palavras-chave:
Manguitorotador Artroscopia Idoso
r
e
s
u
m
o
Objetivos: Avaliarosresultadosdotratamentocirúrgicoporviaartroscópicanaslesõesdo manguitorotador(LMR)depacientescom65anosoumais.
Métodos: Entre1998e2009foramoperados168pacientes.Cincocasosforamexcluídos.Os 163pacientesforamestratificadosdeacordocomafaixaetáriade65a69(49,1%),70a74 (26,4%)eacimade75(24,5%).Amédiafoide71anos(65a83).Eramdosexomasculino63 pacientes(38,7%).Amédiadetempodedor(iníciodossintomas)atéacirurgiafoide23 meses(2d–240m).Referiramhistóriadetrauma62pacientes(38%)e26(16%)algumesforc¸o compioriadador.
Resultados: PeloscritériosdaUniversidadedaCalifórniaemLosAngeles(UCLA)tivemos 80,4% de excelentes resultados, 16% bons, 1,8% regulare 1,8% ruim. Tivemos 11% de complicac¸ões.Oresultadoclínicofinalnãomostroucorrelac¸ãocomaprogressãodaidade, otamanhoda lesãoouostendõesacometidos.Masexisteumaassociac¸ãosignificativa (p<0,001)entreapresenc¸adetraumaelesõesmaiores.Otempoentreoiníciodossintomas eoprocedimentocirúrgicomostraumarelac¸ãosignificativa(p<0,027)comosresultados pós-operatórios:quantomaior,pioresosresultados.
Conclusão: OtratamentoartroscópicodaLMRempacientescom65anosoumais apresen-touresultadosexcelentesebonsem96,4%quandoavaliadospeloUCLA,combaixataxa decomplicac¸ões.Aidadeavanc¸adanãodemonstrouinfluêncianaevoluc¸ãoclínica pós-operatória.Entretanto,quantomaisprecocementeotratamentocirúrgicoforinstituído, melhoresosresultados.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Rotatorcuffinjuriesareverycommoninorthopedicpractice, withprevalencebetween5%and33%.Theyfrequentlyoccur intheelderlypopulation1,2,3,4andreach22%amongpatients overtheageof65years.5Individualsovertheageof50years are morecommonlyaffected bychronic injuriesofgreater severity as aresult ofthe degenerative process, whilethe youngpopulation(<40years)hasinjuriesthatare predomi-nantlyoftraumaticetiology.1,6
While some authors have demonstrated good results regardingimprovementofpain, functionandqualityoflife through conservative methods7,8 or through surgical treat-ment,includingbymeansofacromioplastyanddebridement alone,9,10 others havearguedthat surgicalrepairofrotator cuffinjuriesleadstobetterandlonger-lastingresults.2,3,4,11 Performing surgical procedures on elderly people may be a challenge. In 1995, Hattrup and Scottsdale2 suggested that patients aged 65 years or over present a significant chance of having larger lesions, which potentially adds difficulty to their repair. The bone quality is lower and this results in osteoporosis of the greater tubercle, sub-chondralcysticdegenerationandirregularityofthecortical bone,and it may complicateanchor fixation. Furthermore, elderlypeoplefrequentlypresentcomorbidities(diabetes mel-litus, rheumatoid arthritis or renal diseases), which may diminish the healing response and compromise surgical management.12
Thelongperiodbetweentheinitialpresentationof symp-tomsandthetimewhenarthroscopicsurgicalrepairofthe rotatorcuffinjuryisperformedisanegativeprognostic fac-torfortheclinicalresults.13Inaddition,thesizeofthelesion, retraction,fattydegenerationandthequalityofthetendon alsoinfluencethehealing.14,15
Someauthorshavebelievedthatthesepatients’advanced ageinterfereswiththehealingofrotatorcufflesionsuturing, suchthatyoungpatientstendtohavemorefavorable evolu-tion.Nonetheless,arthroscopicrepaironrotatorcuffinjuries inelderlypeopleproducessignificantfunctionalimprovement andpositivechangestoqualityoflife,16–20withadvantagesin relationtoopensurgeryandmini-openprocedures,because ofthesmallincision,absenceofdamagetothedeltoid mus-cle,lower painduringthe postoperativeperiodandshorter hospitalstay. Moreover,especially, itenablesdiagnosis and treatmentofassociatedlesionsthroughviewingthejointwith minimal tissue trauma.21–23 Thus, Charousset et al.15 and Grondeletal.17suggestedthatagealoneisunrelatedtopoor resultsfrominjuryrepairs.
The present study had the objective of evaluating the resultsfrom arthroscopic surgicaltreatment ofrotator cuff lesionsinpatientsaged65yearsorover.
Sample
and
methods
tearingoftherotatorcuffandunderwentarthroscopicsurgical treatmentperformedbytheshoulderandelbowgroupofour servicebetweenSeptember1998andAugust2009.
Theinclusioncriteriawerethatthepatientsshouldbe65 yearsofageorover,withcompletetearingoftherotatorcuff thatwasarthroscopicallysuturedinanoperationthattook placeatleast1year earlier.Thefollowingwereconsidered tobeexclusioncriteria:ageoflessthan65yearswitheither completeorincompletetearing;openprocedures;open proce-dures;andpostoperativelengthoffollow-uplessthan1year. Outofthe168shouldersevaluated, threewereexcluded duetolossfromthefollow-upandtwobecauseofdeath,for reasonsunrelatedtothetreatment.Theremaining163were stratified accordingtoage, withdivisioninto threegroups: 65–69(49.1%);70–74(26.4%)and75orover(24.5%).
There were 63 male patients (38.7%) and 100 female patients(61.3%).Theirmeanagewas70yearsand10months (range:65–83).Thelengthoftimewithpain, fromthestart ofthesymptomsuntilthesurgicaltreatmentrangedfrom2 daysto240months,withmeanof22monthsand25days. Thedominantsidewasaffectedin108cases(66.3%).Only62 patients(38%)reportedhavinghistoriesoftrauma,while26 (16%)saidthatthestartoftheirpainanditsworseningwere relatedtoexertionofsometype.Amongthepatients evalu-ated,45(27.6%)saidthattheypracticedsportsinwhichthey usedtheirupperlimbs.
Allthepatientsunderwentthesurgicalprocedureinthe “deckchair” position, under general anesthesia in associa-tionwithanestheticblockofthebrachialplexus.Wemade aninitialarthroscopicinspectionofthejointandidentified theassociatedlesions.Eighty-threepatients(50.9%)presented lesionsinthelongheadofthebicepsbrachiimuscle.Among these,thetendonwasabsentin17cases(10.4%)anditwas foundtobeadheringtothebicipitalgrooveintwo(1.2%).In theother casesinwhichweobserveddislocationorinjury affectingmorethan50%ofthediameterofthetendonofthe longheadofthebiceps, weperformed tenotomy(20cases; 12.3%).Weperformedtenotomyinassociationwith tenode-sisin44cases(27%),beforerepairingtherotatorcuff.Wealso foundSLAPlesions(superiorlabrum,anteriorandposterior) infourcases,Bankartlesionsinthree,calcareoustendinitis ofthetendonofthesupraspinatusmuscleinone,adhesive capsulitisintwoandshoulderarthrosisin12(Table1).When thesurgeondeemeditnecessary,theselesionsweretreated duringthesamesurgicalprocedure(Table2).
Followingthis,wedealtwiththesubacromialspaceand performedbursaldebridementandmobilizationofthe ten-dons.Acromioplastywasperformedin145cases(89%)and resectionofthedistalportionoftheclavicle(Mumford),which wasindicatedinthe casesofpaininthe acromioclavicular joint,wasperformed in54 cases(33.1%).Wethen induced bleedinginthebonebedofthegreatertubercleofthehumerus andsuturedthelesion.Thenumberoftendon-to-tendonor tendon-to-bonestitchesrangedfrom1to12(meanof5). Sutur-inganchorswereusedin158cases,witharangefrom1to5 (meanof2).
Therotatorcufflesionswereclassifiedassmall,foundin26 cases(16%);medium,43cases(26.4%);large,25cases(15.3%); orextensive,69cases(42.3%),inaccordancewiththe classifi-cationofHawkins.24Thosethatinvolvedatleasttwotendons
Table1–Frequenciesoflesionsassociatedwithrotator cuffinjuries.
Associatedlesions No.ofcases %
LHB 83 50.9
SLAPlesion 4 2.5
Bankartlesion 3 1.8
CTSE 1 0.6
Adhesivecapsulitis 2 1.2
Shoulderarthrosis 12 7.4
TOTAL 105 64.4
Source:MedicalfilesofIrmandadeSantaCasadeMisericórdiade SãoPaulo.
LHB,tendonofthelongheadofthebicepsbrachiimuscleofthe arm;CTSE,calcareoustendinitisofthetendonofthesupraspinatus muscle.
were alsoconsidered tobeextensive,as definedbyGerber etal.25
Fromanalysisonthetendonsaffected,100%ofthecases presentedinvolvement ofthe tendonof thesupraspinatus muscle; 43.6%the tendonoftheinfraspinatus muscle; and 33.1%thetendonofthesubscapularismuscle.
Aftertheoperation,thepatientswereimmobilizedfor6–8 weeksbymeansofafunctionalsling.Accordingtothesize ofthelesionandtheretractionofthetendons,passive exer-cisessuchaspendulumexerciseswereallowed.Ifthelesion wasextensive,theshoulderwaskeptimmobilizedforatleast 4weeks.Passiveelevationwasstartedinthefourthweekand activeelevationinthesixthweek.Musclestrengthening exer-ciseswereonlyallowedstarting4monthsaftertheoperation. Themeanlengthofpostoperativefollow-upwas50months and18days,witharangefrom12to144months.Duringthis period,thepatientswereevaluatedbymeansofthemethod oftheUniversityofCaliforniainLosAngeles(UCLA).26
In the statistical analysis, the SPSS software (Statistical Package forthe SocialSciences), version 17.0,was usedto obtain theresults,and95%intervalswereconsidered tobe statisticallysignificant(p<0.05).
Results
ThemeanUCLAscoreamongthe163patientsevaluatedwas 33.6points(range:11–35).80.4%ofthecaseswereconsidered tohaveattainedexcellentresults,16%were goodand3.6% wereunsatisfactory:threefairandthreepoor.
The evaluationof the clinical resultsdid not show any statisticallysignificantcorrelationwithageprogression,such that we found that 97.6% of the results in the age group between 65 and 69 years were good or excellent; 95.4% betweentheagesof70and74years;and95%aged75yearsor over(p=0.49).
Table2–Treatmentoflesionsassociatedwithrotatorcuffinjuriesfoundduringthesurgicalprocedure.
Associatedlesions Debridement Tenotomy Tenodesis Suture Capsulotomy Resection Boneperforations
LHB 2 20 44
SLAPlesion 3 1
Bankartlesion 3
CTSE 1
Adhesivecapsulitis 2
Shoulderarthrosis 9 3
TOTAL 14 20 44 4 2 1 3
Source:Medicalfilesoftheinstitution.
LHB,tendonofthelongheadofthebicepsbrachiimuscleofthearm;CTSE,calcareoustendinitisofthetendonofthesupraspinatusmuscle.
Thetendonoftheinfraspinatuswasaffectedin43.6%of thecasesandtherewasaslightincreaseinincidencewith ageprogression(p=0.31).
Thetimethatelapsedbetweenthestartofsymptomsand thesurgicalprocedureshowedastatisticallysignificant rela-tionship(p<0.027)withthepostoperativeresults,giventhat thegreaterthetimethatelapsedbetweenthesymptomsand thesurgerywas,theworsethefinalresultswere.
Theincidenceofcomplicationswas6.1%(10cases):one caseofadhesivecapsulitis,oneoftendinitisofthebiceps,two oflimitationofrange ofmotionregardingmedialrotation, twoofpainfulrenewedtearing,twoofnon-painfulrenewed tearingwithfunctionalimpotence,oneofarthropathyofthe rotatorcuffandoneofpainintheacromioclavicularjoint.
Discussion
In the light of increasing longevity among the population andhigherlevelsofphysicalactivity,surgicalrepairof symp-tomatic lesions of the rotator cuff that do not present improvementthrough conservative treatment hascome to beconsideredtobeatreatmentoptionforpatientsaged65 yearsandover.Manyformsofinterventionhavebeen advo-catedand there issome controversyregarding the typeof surgical approach, i.e.whether torepair the lesion or just toperformdebridementinisolation,amongelderlypatients. Some pioneering studies have demonstrated good results fromsubacromialdecompressionandarthroscopic debride-ment,whichleadtotemporarypainrelief,buthaveinferior andlesslong-lastingresultsthanlesionrepair.6,9,10,27Our find-ingsfromarthroscopicrepairweregoodorexcellentin96.4% ofthecases(157shoulders)andwereinlinewithsomereports intheliterature,inwhichrepairstorotatorcufflesions per-formedarthroscopicallyhavebeenindicatedasconsistently better.3,4,11,20
In 1995,Hattrup and Scottsdale2 found aclear associa-tion between the size of the lesion and the patient’s age. Thepresenceoflargeandextensivelesionswassignificantly greater amongthe older patients.Our study demonstrated thistrend,sincetheincidenceofextensivelesionswas37.5% amongpatientsupto69yearsofage;44.2%amongthoseaged 70–74yearsand50%amongthoseaged75yearsorover.The lesionsfoundinelderlypatientsaregenerallyofdegenerative etiology,ratherthan oftraumaticetiology;themusculature
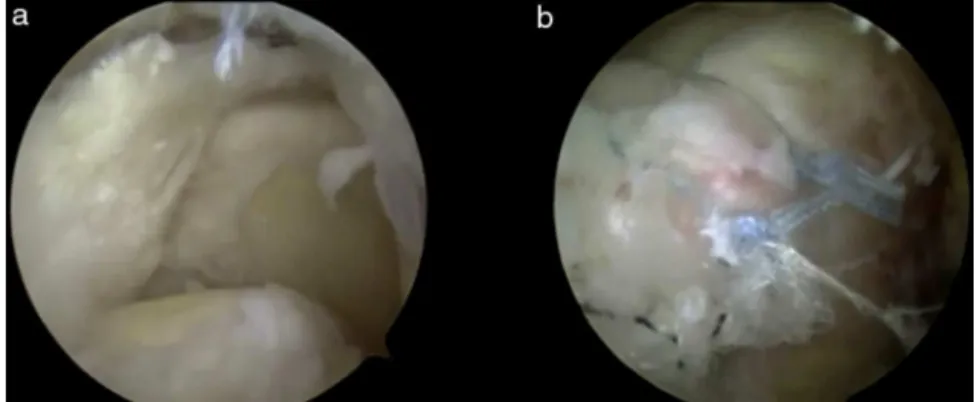
is found to have atrophied and the tendonshave become thinnedandpresentpoorqualityforsuturing(Figs.1and2).
Althoughwedidnotfindanystudiesintheliterature cor-relating the size of the rotator cuff lesion with traumatic episodes,traumawasreportedby62patients(38%)andwas presentin12casesoflargelesions(19.4%)and37of exten-sivelesions(59.7%).Thus,thisstudypresentedastatistically significantcorrelationbetweenhistoriesoftraumaand inci-denceoflargeandextensivelesions(p<0.01).Therewasalso aslightincreaseintheincidenceofsuchlesionsinrelationto ageprogression(p=0.11).
In an imaging study conducted by Boileau et al.,14 the healing rate for arthroscopically repaired lesions of the supraspinatusamong65patientsaged29–79yearswas71%. Agewasaninfluentialfactor,giventhatpatientsovertheage of65yearshadahealingrateof43%(p=0.001).Nonetheless, despite thetendency towardworse resultsamongpatients over theageof65years,whichwasalsodescribed by Hat-trupandScottsdale,2Charoussetetal.15andLamandMok,18 ourfindingsdidnotshowanysignificantcorrelationbetween advancingagegroupsandthefinalfunctionalclinicalresult.
Boileau et al.14 reportedthat the size ofthe lesion and delaminationofthetendonoftheinfraspinatusand/or sub-scapular muscle significantlyimpaired healing subsequent to arthroscopic suturing (p=0.02). Charousset et al.15 also reportedthatthesizeofthelesiongenerallycorrelatedwith theprognosis.However,ourstudydemonstratedthatthesize ofthelesionwasnotrelatedtothefinalresults,andthis find-ingwasinlinewiththatofBittar,28 whoreportedthat83% oftheresultsfromarthroscopicrepairofextensivelesionsin patientsofmeanage67yearsweresatisfactory.Itisalsoin agreementwiththeresultsfromGartsmanetal.21and Stoll-steimer andSavoie,29 whoshowed that all sizesoflesions couldbetreatedarthroscopically,independentofagegroup. There were no differences between the results relating to small,medium-sizedorlargelesions.
Fig.1–Intraoperativeimageoftherightshoulderviewedthroughtheposteriorportal,showing:(A)lesionofthetendonof thesupraspinatusandinfraspinatus,whicharegreatlydegenerated;(B)closureofthelesionusingtendon-to-tendon stitchesandanchors.
thelargerthesizeofthelesionwouldbeand,consequently, themoredifficultitwouldbetorepairit,withaworse prog-nosis.
Thedecision regardingwhich surgical techniqueto use (open,mini-openortotally arthroscopic)isgenerallybased onthesurgeon’spreferenceandexperience.Inananalysison theresultsobtainedfromarthroscopicrepairofrotatorcuff injuries,Checchia et al.23 concludedthat this technique is moreefficient,bothinrelationtotheresultsobtained(93.7% were excellentor good,according tothe UCLAscores)and inrelationtopreventionofcomplications(9.2%).Inrelation topostoperative complications and treatment failures, our resultsaresimilartothoseintheliterature,withanincidence of6.1%.Inareviewof40 articlesontheresultsfromopen repairofrotatorcuffinjuriesconductedin1997,Mansatetal.30 founda complicationrate of10.5%.In1992, Curtis et al.31 reportedacomplicationrateof4.8%fromarthroscopic pro-ceduresand8.8%fromthemini-opentechnique.Incontrast, in1998,Berjanoetal.32reportedratesof10.6%from arthro-scopicproceduresand 5.3%from mini-openprocedures.In 2001,Grondeletal.17reportedacomplicationrateof6%,from analysisonextensivelesionsrepairedusingthearthroscopic andmini-opentechniques.Ontheotherhand,from exami-nationof263patientswhounderwentarthroscopicrepairof rotatorcufflesionsin2007,Brislinetal.33reporteda compli-cationrateof10.6%(28cases).Jointstiffnessoccurredmore frequently (23cases) and this was unrelatedto the extent ofthelesion.In2010,Vermaetal.20 alsoreportedasimilar
complicationrate(7.7%)andstatedthatthecomplicationrate wasnogreateramongelderlyindividualsandthereforewas unrelatedtoageprogression.
Amongourpatients,wefoundonecaseofadhesive cap-sulitis, which underwent serial block of the suprascapular nerve, which led to remission ofthe condition (UCLA 34); onecaseoftendinitisofthebiceps,whichwastreatedusing non-steroidalanti-inflammatorydrugs(UCLA35);twocases oflimitationoftherangeofmotioninmedialrotation,which were treated bymeans of physiotherapy(UCLA13 and 33, respectively);twocasesofpainfulrenewedtearing:thefirst underwentnewsurgicalrepairandevolvedwithUCLA33and thesecondwaskeptunderexpectantmanagement,because of the patient’s satisfaction (UCLA 29); two cases of non-painful renewed tearingwith functional impotence, which weretreatedusingphysiotherapy,bothwithUCLA33;onecase ofarthropathyoftherotatorcuff,whichunderwentreverse shoulderarthroplasty(UCLA34);andonecaseofpaininthe acromioclavicularjoint,which underwent corticoid infiltra-tionandevolvedwithUCLA35.
The incidence ofdehiscence ofsuturing of rotator cuff injuriesafteropenrepairisaround13–68%.34Slabaughetal.35 reportedthatthisrateisprobablygreaterthanwhatiscited in the literature,because most ofthese cases are asymp-tomaticanddonotimplyanypainorsignificantfunctional loss.In2005,Ozbaydaretal.36usedmagneticresonance imag-ingtoevaluatefattydegenerationandrecurrenceoftearing of the rotator cuff subsequent to arthroscopic repair and
observed renewed tearing in 31.8%, even though 90.9% of thepatientsweresatisfied.Theextentofthefatty degener-ationdidnotpresentanydifferencefrombeforetoafterthe operation.In2010,Godinhoetal.37evaluatedthefunctional andanatomicalresultsfromarthroscopicsurgicaltreatment of complete tearing of the rotator cuff in 100 patients of meanage60years,andinvestigatedthecorrelationbetween ultrasound images and the Constant–Murley index. They foundthat there was no statisticallyvalid correspondence betweenthem.Theyreportedthat67%oftheshoulders stud-iedpresentedexcellentorgoodresults,although30%ofthem presented ultrasound reports showing renewed tearing. In ourservice,wedidnotroutinelyperformpostoperative mag-netic resonance imagingexaminations.In ourstudy, these examinations were requested for two symptomatic cases thatshoweddehiscenceofthesuture.Anothertwocasesof asymptomaticdehiscencewereobservedinpatientswhohad undergonetheexaminationthroughrequestsfromanother service.
Inoursample,wefoundfourcasesofdehiscenceofthe suture,butonlytwooftheseshownanysymptoms.
All the rotator cuff lesions in our study were repaired completely, independentlyofthe sizeof thelesion,or any retractionorfattydegeneration.Innocaseweresubacromial decompressionanddebridementaloneperformed.Although weareawarethatdehiscenceofthesutureprobablyoccurs often,webelievethatgoodresultscanbeexpectedthrough thistechnique.
Itisimportanttoemphasizethatourstudyhadthelargest sampleintheliteraturerelatingtoarthroscopicrepairof rota-torcufflesions amongthis agegroup. However,this study presentslimitationsduetoitsretrospectivenature,absenceof acontrolgroupandshortminimumfollow-upof12months, althoughthemaximumrecoveryisachievedby6–9months aftertheoperationandfromthetwelfthmonthonwards,there arealmostnofurtherchanges.20Anotherlimitationwasthe lackofanalysisonthedegreeoffattydegenerationof mus-cles,asdescribedbyGoutallieretal.,38giventhatnotallthe magneticresonanceexaminationsofourpatientsincludedT1 sagittalslicesforcompleteanalysisasdescribedbyMellado etal.39in2005.
Conclusion
Arthroscopictreatmentofrotatorcufflesionsinpatientsover theageof65yearspresentsgoodorexcellentresultsin96.4%, whenevaluatedusingtheUCLAfunctionalmethod,withalow complicationrate.
Giventhattheobjectiveofsurgeryistoimprovepainand function, we believe that our study strongly suggests that indicationsforrepairingrotatorcuffinjuriesamongelderly peoplearevalid,consideringthatadvancedagedoesnot influ-encegoodpostoperativeclinicalevolution.Likewise,thesize oflesion is unrelatedto the postoperative prognosis, even thoughlargeandextensivetearingisassociatedwiththe pres-enceoftrauma. Wecanalsoconclude thattheearlierthat thesurgical treatmentisimplemented, the betterthefinal functionalresultswillbe.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.EllmanH,KaySP,WirthM.Arthroscopictreatmentof full-thicknessrotatorcufftears:2-to7-yearfollow-upstudy. Arthroscopy.1993;9(2):195–200.
2.HattrupSJ,ScottsdaleA.Rotatorcuffrepair:relevanceof patientage.JShoulderElbSurgAm.1995;4(2):95–100. 3.MelilloAS,SavoieFH,FieldLD.Massiverotatorcufftears:
debridementversusrepair.OrthopClinNAm. 1997;28(1):117–24.
4.MontgomeryTJ,YergerB,SavoieFH.Managementofrotator cufftears:acomparisonofarthroscopicdebridementand surgicalrepair.JShoulderElbSurgAm.1994;3(2):70–8. 5.FehringerEV,SunJ,VanOeverenLS,KellerBK,MatsenFA.
Full-thicknessrotatorcufftearprevalenceandcorrelation withfunctionandco-morbiditiesinpatientssixty-fiveyears andolder.JShoulderElbSurg.2008;17(6):881–5.
6.GartsmanG.Massive,irreparabletearsoftherotatorcuff. Resultsofoperativedébridementandsubacromial decompression.JBoneJointSurgAm.1997;79(5):715–21. 7.ItoiE,TabataS.Conservativetreatmentofrotatorcufftears.
ClinOrthopRelatRes.1992;(275):165–73.
8.GhroubiS,ChaariM,ElleuchH,GuermaziM,BakloutiS, ElleuchMH.Functionalandqualityoflifeoutcomeofnone operatedrotatorcufftears.AnnReadaptMedPhys. 2008;51(9):714–21.
9.ZvijacJE,HowardJL,LemakLJ.Arthroscopicsubacromial decompressioninthetreatmentoffullthicknessrotatorcuff tears:a3to6yearfollow-up.Arthroscopy.1994;10(5):518–23. 10.RockwoodCAJr,WilliamsGJr,BurkheadWZJr.Débridement ofdegenerative,irreparablelesionsoftherotatorcuff.JBone JointSurgAm.1995;772(6):857–66.
11.WeberSC.Arthroscopicdebridementandacromioplasty versusmini-openrepairinthemanagementofsignificant partial-thicknesstearsoftherotatorcuff.OrthopClinNAm. 1997;28(1):79–82.
12.BrewerBJ.Agingoftherotatorcuff.AmJSportsMed. 1979;7(2):102–10.
13.FlurinPH,LandreauP,GregoryT,BoileauP,LafosseL,GuilloS, etal.Cuffintegrityafterarthroscopicrotatorcuffrepair: correlationwithclinicalresultsin576cases.Arthroscopy. 2007;23(4):340–6.
14.BoileauP,BrassartN,WakinsonDJ,CharlesM,HatzidakisAM, KrishnanSG.Arthroscopicrepairoffull-thicknesstearsofthe supraspinatus:doesthetendonreallyheal?JBoneJointSurg Am.2005;87(6):1229–40.
15.CharoussetC,BellaicheL,KalraK,PetroverD.Arthroscopic repairoffull-thicknessrotatorcufftears:istheretendon healinginpatientsaged65yearorolder?Arthroscopy. 2010;26(3):302–9.
16.WorlandRL,ArredondoJ,AnglesF,Lopez-JimenezF.Repairof massiverotatorcufftearsinpatientsolderthan70years.J ShoulderElbSurg.1999;8(1):26–30.
17.GrondelRJ,SavoieFH,FieldLD.Rotatorcuffrepairsinpatients 62yearsofageorolder.JBoneJointSurgAm.2001;10(2):97–9. 18.LamF,MokD.Openrepairofmassiverotatorcufftearsin
patientsagedsixty-fiveyearsorover:isitworthwhile?J ShoulderElbSurg.2004;13(5):517–21.
20.VermaNN,BathiaS,BakerCL,ColeBJ,NicholsonGP,Romeo AA,etal.Outcomesofarthroscopiccuffrepairinpatients aged70yearsorolder.Arthroscopy.2010;26(10):1273–80. 21.GartsmanGM,KhanM,HammermanSM.Arthroscopicrepair
offull-thicknesstearsoftherotatorcuff.JBoneJointSurg Am.1998;80(6):832–40.
22.BurkhartSS.Astepwiseapproachtoarthroscopicrotatorcuff repairbasedonbiomechanicalprinciples.Arthroscopy. 2000;16(1):82–90.
23.ChecchiaSL,SantosPD,MiyazakiAN,FregonezeM,SilvaLA, IshiM,etal.Avaliac¸ãodosresultadosobtidosnaavaliac¸ão artroscópicadomanguitorotador.RevBrasOrtop. 2005;40(5):229–38.
24.HawkinsRJ,MisamoreGW,HobeikaPE.Surgeryforfull thicknessrotator-cufftears.JBoneJointSurgAm. 1985;67(9):1349–55.
25.GerberC,FuchsB,HodlerJ.Theresultsofrepairofmassive tearsofrotatorcuff.JBoneJointSurgAm.2000;82(4):505–15. 26.EllmanH,HankerG,BayerM.Repairoftherotatorcuff:
end-resultstudyoffactorsinfluencingreconstruction.JBone JointSurgAm.1986;68(8):1136–44.
27.KempfJF,GleyzeP,BonnometF,WalchG,MoleD,FrankA, etal.Amulticenterstudyof210rotatorcufftearstreatedby arthroscopicacromioplasty.Arthroscopy.1999;15(1):55–66. 28.BittarES.Arthroscopicmanagementofmassiverotatorcuff
tears.Arthroscopy.2002;18(9Suppl2):104–6.
29.StollsteimerGT,SavoieFH3rd.Arthroscopicrotatorcuff repair:currentindications,limitations,techniquesand results.InstrCourseLect.1998;47:59–65.
30.MansatP,CofieldRH,KerstenTE,RowlandCM.Complications ofrotatorcuffrepair.OrthopClinNAm.1997;28(2):205–13.
31.CurtisAS,SnyderSJ,DelPizzoW,FriedmanMJ,FerkelRD, KarzelRP.Complicationsofshoulderarthroscopy. Arthroscopy.1992;8(3):395.
32.BerjanoP,GonzalezBG,OlmedoJF,PerezLA,MunillaMG. Complicationsinarthroscopicshouldersurgery.Arthroscopy. 1998;14(8):785–8.
33.BrislinKJ,FieldLD,SavoieFH.Complicationsafter
arthroscopicrotatorcuffrepair.Arthroscopy.2007;23(2):124–8. 34.JostB,PfirrmannCW,GerberC,SwitzerlandZ.Clinical
outcomeafterstructuralfailureoftherotatorcuffrepairs. BoneJointSurgAm.2000;82(3):304–14.
35.SlabaughMA,NhoSJ,GrumetRC,WilsonJB,RomeoAA, VermaNN,etal.Doestheliteratureconfirmsuperiorclinical resultsinradiographicallyhealedrotatorcuffsafterrotator cuffrepair?Arthroscopy.2010;26(3):393–403.
36.OzbaydarMU,TonbulM,YalamanO.Theresultsof
arthroscopicrepairoffull-thicknesstearsoftherotatorcuff. ActaOrthopTraumatolTurc.2005;39(2):114–20.
37.GodinhoGG,Franc¸aFO,FreitasJMA,WatanabeFN,NobreLO, AlmeidaNetoMA,etal.Avaliac¸ãodaintegridadeanatômica porexamedeultrassomefuncionalpeloíndicedeConstant &Murleydomanguitorotadorapósreparoartroscópico.Rev BrasOrtop.2010;45(2):174–80.
38.GoutallierD,PostelJM,BernageauJ,LavauL,VoisinMC.Fatty muscledegenerationincuffruptures–preandpostoperative evaluationbyCTscan.ClinOrthopRelatRes.1994;(304):78–83. 39.MelladoJM,CalmetJ,OlonaM,EsteveC,CaminsA,Palomar