ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Rheumatic
fever:
update
on
the
Jones
criteria
according
to
the
American
Heart
Association
review
–
2015
Breno
Álvares
de
Faria
Pereira
a,∗,
Alinne
Rodrigues
Belo
a,
Nilzio
Antônio
da
Silva
baUniversidadeFederaldeGoiás(UFG),FaculdadedeMedicina,DepartamentodePediatria,Goiânia,GO,Brazil
bUniversidadeFederaldeGoiás(UFG),FaculdadedeMedicina,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5June2016 Accepted20December2016 Availableonline10April2017
Keywords:
Childhood Carditis Rheumaticfever Jonescriteria Classification
a
b
s
t
r
a
c
t
Rheumaticfeverisstillcurrentlyaprevalentdisease,especiallyindevelopingcountries. Trig-geredbyaGroupA-hemolyticStreptococcusinfection,thediseasemayaffectgenetically predisposedpatients.Rheumaticcarditisisthemostimportantofitsclinical manifesta-tions,whichcangenerateincapacitatingsequelaeofgreatimpactfortheindividualandfor society.Currently,itsdiagnosisismadebasedontheJonescriteria,establishedin1992by theAmericanHeartAssociation.In2015,theAHAcarriedoutasignificantreviewofthese criteria,withnewdiagnosticparametersandrecommendations.Inthepresentstudy,the authorsperformacriticalanalysisofthisnewreview,emphasizingthemostrelevantpoints forclinicalpractice.
©2017PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Febre
reumática:
atualizac¸ão
dos
critérios
de
Jones
à
luz
da
revisão
da
American
Heart
Association
–
2015
Palavras-chave:
Infância Cardite
Febrereumática,CritériosdeJones Classificac¸ão
r
e
s
u
m
o
Afebrereumáticaaindaéumadoenc¸aprevalentenostemposatuais,sobretudonospaíses emdesenvolvimento. Deflagrada por umainfecc¸ão pelo Streptococcus-hemolíticodo grupoA,podeafetarpacientesgeneticamentepredispostos.Acarditereumáticaéamais importantedasmanifestac¸õesclínicas,podendogerarsequelasincapacitantesedegrande impactoparaoindivíduoeparaasociedade.Atualmente,seudiagnósticoéfeitobaseado nosCritériosdeJones,estabelecidosem1992pelaAmericanHeartAssociation(AHA).Em 2015,aAHAprocedeuumasignificativarevisãodestescritérios,comnovosparâmetrose recomendac¸õesdiagnósticas.Nopresenteestudo,osautoresrealizamumaanálisecrítica destanovarevisão,enfatizandoospontosdemaiorrelevânciaparaapráticaclínica.
©2017PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](B.Á.Pereira).
http://dx.doi.org/10.1016/j.rbre.2017.03.001
2255-5021/© 2017 Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-ND license (http://
Introduction
Rheumaticfever(RF) isaninflammatory,systemic disease, triggeredbythegroupA-hemolyticStreptococcusinfectious agent,which occurs ingeneticallypredisposed individuals. Themostrelevantclinicalmanifestationofthedisease con-sistsofheartdisordersandischaracterized,inmostpart,by valvulitis,especiallyinthemitralandaorticvalves,whichcan bechronicandcausedisablingsequelae.
Note:thelevelsofevidenceindicatedthroughoutthetext arethoseendorsedbytheGuidelinesoftheFederalMedical Council(CFM)withtheBrazilianMedicalAssociation(AMB) andarelistedinTable1.
Diagnosis
Currently,thediagnosisofrheumaticfeverisstillbasedona setofcriteria,i.e.,theJonescriteria,whichhavebeenreviewed atirregularintervalsbytheAmericanmedicalassociations– currently,bytheAmericanHeartAssociation(AHA).According tothelatestreview,publishedin2015,12majorchangeshave beenmadeinrelationtothecriteriaestablishedin1992.2
Thefirstoneconsistedinthestratificationofsusceptible individualsinto2groups,basedonepidemiological consid-erationsregardingtherisktoacquirethedisease.Alow-risk groupisoneinwhichtheincidenceofRFislessthan2/100,000 schoolchildren(aged5–14years)peryearorthathasa preva-lenceofchronicrheumaticcarditisinanyagegrouplowerthan orequalto1/1000peryear.Childrenfromcommunitiesthat exhibitlevelsabovethesewouldhavemoderate-to-highrisk foracquiringthedisease.
Thesecondimportantchangewastoincludethepossibility ofusingtheJonescriteriatodiagnoserheumaticfeverrelapses (untilthenitspurposewasonlytodiagnoseearlyepisodesof thedisease).
- AtthediagnosisofinitialRFoutbreaks:
Forlow-riskindividuals,theinterpretationofthe diagnos-ticcriteriaremainsthesameasforthe1992review.2Inthese cases,aninitialoutbreak(1stepisode)ofrheumaticfeverwill behighlylikelywhen,inthepresenceofevidenceofaprevious
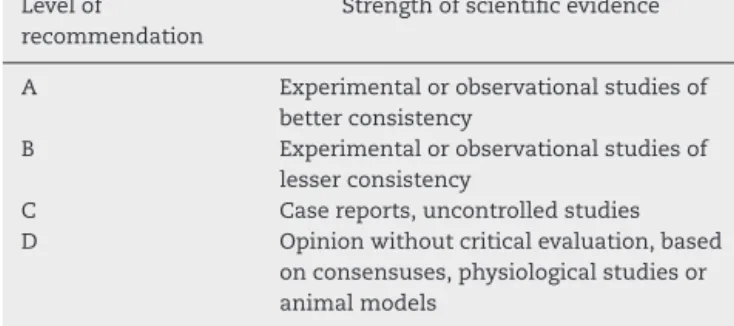
Table1–LevelofScientificEvidencebyTypeofStudy– “OxfordCentreforEvidence-BasedMedicine”–last updatedinMay2001.19
Levelof recommendation
Strengthofscientificevidence
A Experimentalorobservationalstudiesof betterconsistency
B Experimentalorobservationalstudiesof lesserconsistency
C Casereports,uncontrolledstudies D Opinionwithoutcriticalevaluation,based
onconsensuses,physiologicalstudiesor animalmodels
infectionbygroupA-hemolyticStreptococcus,2majorcriteria aremet,or1majorand2minor.
Moreover,regardlessoftheriskclassification,the Echocar-diographywithDopplerfindingssuggestiveofcarditis–even iftheyarenotaccompaniedbyheartmurmurorotherclinical signs (“subclinicalcarditis”),areconsidered enoughto con-template1majorsignofthecriteria.
Concerningjointinvolvement,forindividualswith moder-atetohighrisk,polyarthralgiaandmonoarthritis(andnotonly polyarthritis,asinthepast)alsostartedtobeconsideredas majorsignsofthecriteria.Additionally,monoarthralgiawas alsoconsideredasaminorsignforthisriskgroup.
Inbothriskgroups, therewereno changesintheother minorsignsofthecriteria.IsolatedChorea,withanundefined etiology,remainssufficientforthediagnosistobeattained, evenintheabsenceofothermanifestations1(D).
- Atthediagnosisofdiseaserelapse(recurrentRF):
ForpatientsthathavealreadyhadtheinitialRFoutbreak, thecriteriaremainthesameasthoselistedaboveforlow-risk andmoderate-to-highriskpopulations–whatchangesisthe minimumnumberofcriteriatobemet.Fortheseindividuals, inadditiontomeeting2majorcriteriaor1majorand2minor ones(asintheinitialoutbreak),onecanalsoconsiderthe pos-sibilityofmeetingthreeminorcriteriaasadiseaserecurrence diagnosis,regardlessoftheriskgrouptowhichthepatient belongs(Table2).
Therearesomecharacteristicsthatarespecifictothe clini-calmanifestationsofrheumaticfever,which,whenidentified, increasethepositivepredictivevalueofthatfinding.Although it cannotbe said that there isa typical clinical picture of rheumaticfever,themostcommonformsofinvolvementare:
• Arthritis–Largejointssuchasknees,elbows,wrists,and
anklesarethemostaffectedones.Thepatternof involve-ment ismigratoryand can befully resolved,mostoften leavingnosequelae.Theresponsetononsteroidal inflam-matorydrugsisexcellent,withsymptomremissionwithin 48–72h1,3(D)4(B).
• Carditis–theaffectedleafletistheendocardiuminmore
than90%ofthecases,whichisexpressedasmitral regur-gitation, manifesting as an apical systolic murmur. In approximately50%ofthecases,itmaybeaccompaniedby basaldiastolicmurmur,duetoaorticregurgitation.The con-comitanceofmitralandaorticregurgitationinapreviously healthy patient is highly suggestive of rheumatic fever. Occasionally,myocarditisandpericarditismaybepresent. Intheabsenceofvalvulitis,thesemanifestationsarerarein rheumaticfever1(D)4(B)5(D)6(B).
• Chorea – disordered, involuntary, abrupt movements of
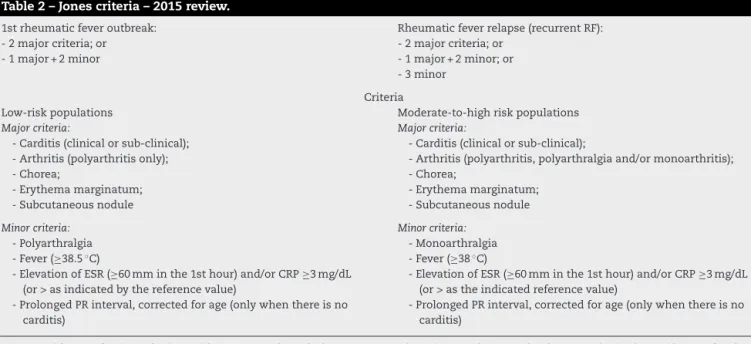
Table2–Jonescriteria–2015review.
1strheumaticfeveroutbreak: -2majorcriteria;or -1major+2minor
Rheumaticfeverrelapse(recurrentRF): -2majorcriteria;or
-1major+2minor;or -3minor
Criteria
Low-riskpopulations Moderate-to-highriskpopulations
Majorcriteria:
-Carditis(clinicalorsub-clinical); -Arthritis(polyarthritisonly); -Chorea;
-Erythemamarginatum; -Subcutaneousnodule
Majorcriteria:
-Carditis(clinicalorsub-clinical);
-Arthritis(polyarthritis,polyarthralgiaand/ormonoarthritis); -Chorea;
-Erythemamarginatum; -Subcutaneousnodule
Minorcriteria: -Polyarthralgia -Fever(≥38.5◦C)
-ElevationofESR(≥60mminthe1sthour)and/orCRP≥3mg/dL (or>asindicatedbythereferencevalue)
-ProlongedPRinterval,correctedforage(onlywhenthereisno carditis)
Minorcriteria: -Monoarthralgia -Fever(≥38◦C)
-ElevationofESR(≥60mminthe1sthour)and/orCRP≥3mg/dL (or>astheindicatedreferencevalue)
-ProlongedPRinterval,correctedforage(onlywhenthereisno carditis)
ProvenevidenceofpriorinfectionwithA-groupB-hemolyticStreptococcus(positiveoropharyngealculture,positivityinrapidtestsforthe detectionofstreptococcalantigens,hightitersofanti-streptococcalantibodies).
• Erythemamarginatumandsubcutaneousnodules–arerare buthighlyspecifictorheumaticfever.Erythema margina-tumisapinkmacularlesionwitharoundedmarginand palecenter. Itisusually notpruriginousand sparesthe face.Thesubcutaneousnodulesarepainlessandare usu-ally located on the extensor surfaces of the joints and alongthetendons.Theyareassociatedwiththepresence ofcarditis1,3,7–9(D).
• Complementaryexaminations:
o There is an increase in the concentration of serum proteinsthat arereferred toasacutephasereactants, erythrocyte sedimentation rateand C-reactive protein, beingminormanifestationsofthedisease.Leukocytosis andmildanemiaarefrequentnonspecificfindings1,3,7–9 (D).
o Anti-streptolysinO–themostcommonlyusedmethod in ourcountry todemonstrateaprevious infection by groupA-hemolyticStreptococcus.Ideally,each commu-nityshouldpromotestudiesthatcouldestablishwhich levelsorcutoffpointsofthisantibodyshouldbe consid-eredashigh.Asthisisnotourcurrentreality,forchildren, levelsabove320UToddareconsideredhigh.Other meth-odsofdocumentationofpreviousinfectionbyGroupA
-hemolyticStreptococcusarelistedinTable21(D). o Antidesoxyribonuclease B –like anti-streptolysinO, is
anotherantibodyagainststreptococcalproduct,but per-sists athigher levels for longer periods in the serum ofpatientswithrheumaticfever.AsChoreafrequently occursmonthsafterinfectionwithGroupA-hemolytic
Streptococcus,ithasahigherpositivitypercentagewhen comparedtoother methodsofdocumentationforthis infection inpatientswiththisclinical manifestation8,9 (D).
o DopplerEchocardiogram–isconsiderablymoresensitive thanauscultationtodetectvalvularheartlesionsinthe acutephaseofthedisease.Whenavailable,itshouldbe
requestedinallsuspectedrheumaticfevercasestodetect “silent”valvularlesions10(D)11(A)12–14(B).
Treatment
The first therapeutic measure is the eradication of the causative infectious agent, the group A -hemolytic
Streptococcus15 (D): penicillin G benzathine, IM, 1,200,000U, forchildrenweighingmorethan20kg;600,000Uforchildren weighingupto20kg.
Alternatives
• For patients with hemorrhagic disorders (that cannot
receive medication through IM route) penicillin-V, orally (50mg/kg/day,4timesdaily)oramoxicillin(50mg/kg/day, takenthreetimesdaily),bothfor10days.
• For atopic patients, allergicto penicillin and derivatives:
erythromycin(40mg/kg/day,fourtimesdailyfor10days)or azithromycin(20mg/kg/day,oncedailyfor3days). Tetracy-clines(highprevalenceofresistance),sulfonamides(donot eradicatetheagent),chloramphenicol(hightoxicity)should notbeused15(D).
Treatmentofthedifferentclinicalmanifestations:
• Arthritis3,8 (D): nonsteroidal anti-inflammatory drugsfor
about7–10days,preferablyorally:
o Acetyl-salicylicacid(80–100mg/kg/day); o Naproxen(10–20mg/kg/day);
o Ibuprofen(30–40mg/kg/day); o Ketoprofen(1,5mg/kg/day)
• Carditis3(D):prednisone(1–2mg/kg/day),orally,maximum
Note:incaseofconcomitantarthritisandcarditis,thereis noneedtousenonsteroidalanti-inflammatorydrugs;when promotingthegradualreductionofprednisone,itisnot nec-essarytointroducenonsteroidalanti-inflammatorydrugs, providingthataweeklyreductionhigherthan25%isnot intended.
• Chorea:haloperidol,orally,atadoseof1mg/day(andnot
perkg)twicedaily.Increase0.5mgevery3daysuntilagood responseisattained(morethan75%remissionofthe move-ments)oruptoamaximumdoseof5mg/day.Treatment durationofthreemonths3(D)16(B).
Note: Doses close to the maximum dose may cause impregnation or extrapyramidal syndrome.Valproic acid (30mg/kg/day, orally, starting with 10mg/kg/day and increasing10mg/kg,weekly)isindicatedasanalternative3 (D)17(B).
Prophylaxis
Primary prophylaxis – appropriateidentification and treat-mentofupperairwayinfections,suchaspharyngotonsillitis, causedbyGroupA-hemolyticStreptococcus.Theantibiotics recommendationisthesameasthatusedfortheagent erad-icationduringtreatment,asdescribedabove15(D).
Secondary prophylaxis – sporadic and long-term use of antibioticsthatmaintainminimuminhibitoryconcentrations for Group A -hemolytic Streptococcus, aiming to prevent rheumaticfeverrecurrenceinpatientswhohavealreadyhad afirstoutbreakofthedisease.Themostcommonlyusedand mosteffectivedrugis:
• PenicillinGbenzathine,IM,every21days,1,200,000U,for
childrenweighingmorethan20kgand600,000Ufor chil-drenweighingupto20kg.
Asanalternative,thefollowingisindicated:
• Patientswithhemorrhagicdiseases(whichcannotreceive
IMmedications):oralV-penicillin(250mg,twiceaday,every day).
• Atopicpatientsallergictopenicillinandderivatives:
eryth-romycin (250mg twice daily) or sulfadiazine (500mg for patientsupto30kg,1gforthoseweighingmorethan30kg), bothdaily15(D).
Durationofsecondaryprophylaxis:
• Patientsthatdidnothavecarditis–theprophylaxisshould
lastuntiltheageof21yearsoruptofiveyearsafterthelast episode,incasesofrecurrence,whicheverlastslonger.
• Patientswhohadpreviouscarditiswithmoderatetosevere
valvedamage–prophylaxisshouldlastuntiltheageof40 years oruntil 10 years after the last episode, incase of recurrence(whicheverlastslonger);andincaseswherethe riskofre-infectionpersists(highriskofexposuretoGroup A-hemolyticStreptococcus),prophylaxisshouldlastfora lifetime.
• Patientswhohadpreviouscarditiswithmildresidualmitral
regurgitationorvalvelesionresolution–prophylaxisshould
lastuntiltheageof25yearsorupto10yearsafterthelast outbreak,whichevercoversthelongestperiod15(D).
Note: The antibiotics and/ordoses listed herein are not effectiveintheprophylaxisofinfectiveendocarditis.Patients withorovalvularlesionsshouldundergospecificprophylactic regimens18(D).
Conclusion
ThereviewoftheJonescriteriaincorporatedchangesthathad longbeenrequestedbythemedicalcommunity.Threeofthem were themainpillarsofthisreview.First,thepossibilityof diagnosingrheumaticfeverrelapseswasincludedintheJones criteria–previously,thepurposeofthecriteriawasto diag-noseonlythefirst episode.Diseaserecurrence cannowbe diagnosedwiththepresenceofthreeminorcriteria.
Thesecondchangewastheseparationofindividuals sus-ceptible to rheumatic fever into two major groups based ondisease prevalence(onewithlowriskand anotherwith moderate to high risk). For individuals with moderate to highrisk,“atypical”jointmanifestationswereincluded,both in the major criteria (polyarthritis, polyarthralgia and/or monoarthritis),andintheminorones(monoarthralgia).
Finally, considering the several publications in the last fewyearsonthesubject,westartedtoconsidersubclinical carditis,diagnosedthroughechocardiographicalterations,as amajorcriterionforthediagnosisofrheumaticfever–and notonlyclinicalcarditis(presenceofmurmur)asbefore.
Thus,consideringthehighprevalenceofthedisease, espe-cially in the developing countries, the review ofthe Jones criteria was an important measure to increase diagnostic sensitivity, resulting inearlier disease identification,better clinicaloutcomefortheindividualand,consequently,a reduc-tioninthesocialimpactofthisdisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GewitzMH,BaltimoreRS,TaniLY.RevisionoftheJones
criteriaforthediagnosisofacuterheumaticfeverintheera
ofdopplerechocardiography.Ascientificstatementfromthe
AmericanHeartAssociation.Circulation.2015;131:1806–18.
2.DajaniAS,AyoubE,BiermanFZ.Guidelinesfordiagnosisof
rheumaticfever:Jonescriteria.Updated1992.Circulation.
1993;87:302–7.
3.daSilvaNA,PereiraBA.Acuterheumaticfever:stilla
challenge.RheumDisClinNorthAm.1997;23:545–68.
4.BitarFF,HayekP,ObeidM,GharzeddineW,MikatiM,Dbaibo
GS.Rheumaticfeverinchildren:a15-yearexperienceina
developingcountry.PediatrCardiol.2000;21:119–22.
5.MarijonE,MirabelM,CelermajerDS,JouvenX.Rheumatic
heartdisease.Lancet.2012;379:953–64.
6.AraújoFD,GoulartEM,MeiraZM.Prognosticvalueofclinical
andDopplerechocardiographicfindingsinchildrenand
adolescentswithsignificantrheumaticvalvulardisease.Ann
7. CommerfordPJ,MayosiBM.Acuterheumaticfever.Medicine. 2006;34:239–43.
8. ChakravartySD,ZabriskieJB,GibofskyA.Acuterheumatic
feverandstreptococci:thequintessentialpathogenictrigger
ofautoimmunity.ClinRheumatol.2014;33:893–901.
9. Guzman-CottrillJA,JaggiP,ShulmanST.Acuterheumatic
fever:clinicalaspectsandinsightsintopathogenesisand
prevention.ClinApplImmunolRev.2004;4:263–76.
10.SaxenaA.Diagnosisofrheumaticfever:currentstatusof
Jonescriteriaandroleofechocardiography.IndianJPediatr.
2000;67:283–6.
11.MirabelM,FauchierT,BacquelinR,TaffletM,GermainA,
RobillardC,etal.Echocardiographyscreeningtodetect
rheumaticheartdisease:acohortstudyschoolchildrenin
FrenchPacificislands.IntJCardiol.2015;188:89–95.
12.FigueroaFE,FernandezMS,ValdesP,WilsonC,LanasF,
CarrionF,etal.Prospectivecomparisonofclinicaland
echocardiographicdiagnosisofrheumaticcarditis:longterm
followupofpatientwithsubclinicaldisease.Heart.
2001;85:407–10.
13.HilárioMO,AndradeJL,GasparianAB,CarvalhoAC,Andrade
CT,LenCA.Thevalueofechocardiographyinthediagnosis
andfollowupofrheumaticcarditisinchildrenand
adolescents:a2yearprospectivestudy.JRheumatol.
2000;27:1082–6.
14.KaneA,MirabelM,TouréK,PérierMC,FazaaS,TaffletM,
etal.Echocardiographicscreeningofrheumaticheart
disease:agematters.IntJCardiol.2013;168:888–91.
15.BarbosaPJB,MülleRE,AndradeJP,BragaALL,AchuttiAC,
RamosAIO,etal.Diretrizesbrasileirasparadiagnóstico,
tratamentoeprevenc¸ãodefebrereumática.ArqBrasCardiol.
2009;93:1–18.
16.TumasV,CaldasCT,SantosAC,NobreA,FernandesRMF.
Sydenham’schorea:clinicalobservationsfromaBrazilian
movementdisorderclinic.ParkinsonismRelatDisord.
2007;13:276–83.
17.GenelF,ArslanogluS,UranN,SaylanB.Sydenham’schorea:
clinicalfindingsandcomparisonoftheefficaciesofsodium
valproateandcarbamazepineregimens.BrainDev.
2002;24:73–6.
18.WilsonW,TaubertKA,GewitzM,LockhartPB,BaddourLM,
LevisonM,etal.Preventionofinfectiveendocarditis.
GuidelinesfromtheAmericanHeartAssociation:aguideline
fromtheAmericanHeartAssociationRheumaticFever,
Endocarditis,andKawasakiDiseaseCommittee,Councilon
CardiovascularDiseaseintheYoung,CouncilonClinical
Cardiology,CouncilonCardiovascularSurgeryand
Anesthesia,andtheQualityofCareandOutcomesResearch
InterdisciplinaryWorkingGroup.Circulation.
2007;116:1736–54.
19.BaracatEC,JateneFB,NobreMCR,BernardoWM.Projeto Diretrizes.Availablefromwww.projetodiretrizes.org.br/