PAIN REPORTING ACCURACY AND ABILITY TO ACCURATELY REPORT OTHER BODILY SENSATIONS IN DANCERS
Dissertação apresentada à Universidade Católica Portuguesa para obtenção do grau de mestre em
Neuropsicologia
Por
Diogo Manuel Garanito Mendonça
PAIN REPORTING ACCURACY AND ABILITY TO ACCURATELY REPORT OTHER BODILY SENSATIONS IN DANCERS
Dissertação apresentada à Universidade Católica Portuguesa para obtenção do grau de mestre em
Neuropsicologia
Por
Diogo Manuel Garanito Mendonça
Sob a orientação de Rita Canaipa, PhD e Roi Treister, PhD
I Abstract
Pain is a highly subjective experience. Researchers and clinicians have been struggling to measure pain, the effect of drugs and other therapies. One of the reasons for these difficulties is thought to be the high variability in pain reporting. Focused Analgesia Selection Test (FAST), was developed to assess pain reporting skills, and thus to discriminate between those that experience pain in accordance with the pain stimulation, and those that experience pain very differently from the external stimulation applied. Underlying differences in pain reporting could be explained through accuracy in other bodily sensations as well. Previous research has shown that in normal population pain accuracy is related to accuracy in the same modality but not between different interoception modalities, suggesting that accuracy is not cross-modal skill. Dancers are known to withstand and perceive pain differently and to have higher interoceptive accuracy comparing to non-dancers. Thus, the aim of the current study was to investigate if in dancers there were relations between pain reporting accuracy the accuracy in different modalities, i.e., interoception and taste. Thirty-three undergraduate and graduate dance students were recruited from a graduate school of dance. They were assessed with FAST procedure, heartbeat detection task and taste perception task. Psychological characteristics and a neuropsychological memory task were also assessed. The results showed significant relations between reporting accuracy within the same modality (taste), but no relations between different sensorial modalities. There were no relations between pain sensitivity and the pain reporting skills, but it was found that the years of dance practice were related to a higher pain reporting accuracy. Our data suggest that reporting accuracy is mostly a within modality characteristic, but further studies are needed to fully understand how higher practice related to body functions can increase accuracy in sensorial modalities.
II Resumo
A dor é uma experiência bastante subjetiva. Investigadores e médicos apresentam dificuldade na sua medição, no efeito real da medicação e noutras terapias. Uma das razões para estas dificuldades acredita-se estar relacionada com a grande variabilidade no reportar a dor. Focused Analgesia Selection Test (FAST) foi desenvolvido para medir a capacidade de reportar a dor, e assim discriminar entre os indivíduos que experienciam a dor de forma proporcional ao estímulo da dor, e aqueles que experienciam a dor de forma muito diferente da estimulação externa aplicada. Por detrás destas diferenças em reportar a dor pode estar a capacidade em reportar com precisão noutras modalidades sensoriais. Pesquisas anteriores mostraram que, em população normal, a precisão da dor está relacionada com precisão na mesma modalidade sensorial, mas não entre modalidades sensoriais, o que sugere que a precisão não é uma capacidade multimodal. Os bailarinos são estudados pela sua capacidade em suportar e sentir a dor de forma diferente, e ter uma maior capacidade de precisão interoceptiva comparado a não dançarinos. Assim, o objetivo do presente estudo foi investigar se, em bailarinos, havia relações entre a precisão em reportar dor e precisão de reportar estímulos noutras modalidades sensoriais. Trinta e três alunos não licenciados e licenciados em dança foram recrutados numa Escola Superior de Dança. Foi aplicado o procedimento do FAST, o procedimento de deteção do batimento cardíaco, e o procedimento de perceção do paladar. Características psicológicas e uma tarefa neuropsicológica da memória também foram medidos. Os resultados mostraram uma relação significativa entre a precisão em reportar estímulos da mesma modalidade sensorial (paladar), contudo, sem nenhuma relação entre as diferentes modalidades sensoriais. Não houve relações entre a sensibilidade à dor e na capacidade de reportar com precisão a dor, mas houve uma relação significativa entre os anos de prática em dança e a uma capacidade maior de reportar com precisão a dor. Os resultados sugerem que reportar com precisão estímulos é uma característica dentro da mesma modalidade sensorial, mas outros estudos são necessários para perceber como é que uma prática intensa com o corpo pode aumentar a precisão nas modalidades sensoriais.
III Agradecimentos
Um obrigado à vida!
Neste momento de desfecho gostaria de agradecer profundamente aos meus pais, bem como às minhas tias Albertina e Lúcia, que, muito acima das suas possibilidades, fizeram tudo ao seu alcance para que pudesse seguir o meu sonho e a minha paixão. Sem eles esta aventura jamais teria começado e que, por vezes, é essencial contemplar a beleza colateral da nossa vivência.
Um obrigado à Prof.ª Dr.ª Rita por ter acreditado sempre em mim e no que era capaz de produzir, proporcionou-me a oportunidade de uma tese bastante exigente e complexa, que me compeliu a ir mais além.
Gostaria igualmente de agradecer à Prof.ª Dr.ª Vanda, pela imensa entrega e disponibilidade para este projeto, como se do seu se tratasse, e por ter sido incansável no seu apoio à investigação, para que todo o estudo fosse avante nas melhores condições possíveis.
Deixo um agradecimento sincero à Mariana por todo o seu ensinamento, paciência e apoio no arranque deste projeto quando tudo parecia tão difícil e intrincado. A sua bondade tornou toda esta experiência mais gratificante.
Por fim, um agradecimento à Bia, amiga das aventuras e tontices de todo o mestrado, memórias que sempre perduraram, e pelo apoio quando as coisas estavam no seu ponto mais exasperante.
“The task is, not so much to see what no one has yet seen, but to think what nobody has yet thought, about that which everybody sees” Erwin Schrodinger
IV Contents 1. Introduction……….1 2. Literature review……….2 2.1. Pain………2 2.2. Interoception……….7 2.3. Dancers………....11
3. The present research………..13
4. Methods……….15
4.1. Participants………....15
4.2. Tools and procedures………15
4.2.1. The Focused Analgesia Selection Test………..15
4.2.2. Taste Perception task………..16
4.2.3. Heartbeat detection task……….17
4.2.4. Heat Pain Thresholds and Tolerance………..17
4.3. Neuropsychological assessment………18
4.3.1. Digit Span task………...18
4.4. Psychological Questionnaires………...18
4.4.1. Sociodemographic questionnaire………..18
4.4.2. Hospital Depression and Anxiety Scale………18
4.4.3. Perceived Stress Scale………...19
4.4.4. Multidimensional Assessment of Interoceptive Awareness……..19
4.4.5. Self-Consciousness Scale………...20 4.5. Procedure………...20 4.6. Statistical Analyses………....21 5. Results………....22 6. Discussion………..30 6.1 Limitations………34
6.2 Future research directions………..34
7. Conclusions………35
V List of tables and figures
Table 1: Demographic Characterization of the study population
(n=33)………...22
Table 2: FAST Outcome measures………..23
Table 3: Descriptive Statistics of Pain Sensitivity Measures (mean heat pain threshold and mean heat pain tolerance).……….24
Table 4. Salt and sugar Outcome measures……….25
Table 5: Descriptive statistics of the Heart beat detection task scores………...26
Table 6: Digit Span Task………26
Table 7: Descriptive Statistics of Questionnaires………...27
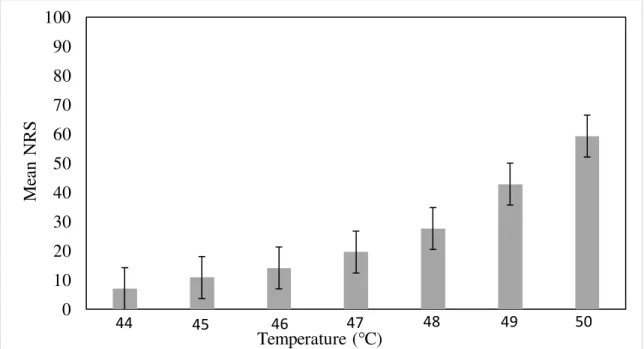
Figure 1: Graphic bars of mean and standard deviation for mean temperature NRS………..23
Figure 2: Graphic bars of mean and standard deviation for mean NRS for all salt and sugar intensities………25
1
1. Introduction
Pain serve as a function of preserving one’s body from potential external life threats, being modulated by sensorial, emotional and cognitive aspects. It is a complex experience highly subjective and difficult to assess both in clinical and experimental settings. The high variability in reporting pain by the individual has been considered one of the reasons for the challenges that clinical trials face in discriminating between an analgesic compound and placebo (Dworkin et al., 2010). High variability in pain may predict a high placebo analgesia response in clinical trials (Treister, Eaton, Trudeau, Elder & Katz, 2017; Wager et al., 2004), but there is still limited knowledge regarding this variability occurs and why subjects differ in their ability to report pain (Quiton & Greenspan, 2008).
To address this issue a procedure named the Focused Analgesia Selection Test (FAST) was recently developed. Its main goal is to assess individuals’ pain reporting skills by exposing them to thermal noxious stimuli of known intensities and ask them to rate their respective intensities. Merging these two elements, both the intensity of the stimuli and the subjective pain report to each stimulus, it is possible to measure how reliable and accurate is the subjects pain reporting. The first studies using FAST supported the claim that it measures specifically variability in pain reporting skills (Treister et al., 2017; Treister et al., 2018) yet further studies are needed in order to understand underlying mechanisms.
One of the possible explanations for the differences in pain reporting variability is that individuals more accurate in pain reporting might be more skilled in the ability to report interoception sensations, that is, “the sense of the physiological condition of the entire body” (Craig, 2003) than individuals that have lower pain report accuracy. In a recent study (Agostinho et al., under review) this line of research has been investigated. It was found that in healthy populations pain report accuracy is not related with the ability to report other bodily sensations, specifically interoception (measured by the mental tracking task, Schandry 1981) and taste (measure by a task developed similarly to FAST). Thus, it is still unclear if in populations known for having higher awareness of their body, such as dancers, a relation between pain reporting accuracy and interoception can be found. Dancers have higher awareness of their bodies and heightened interoception accuracy (Christensen, Gaigg, & Calvo‐Merino, 2018). They are also known for experiencing pain differently from non-dancers, developing strategies to overcome pain,
2
and therefore, showing higher pain thresholds and pain tolerance (Tajet-Foxell & Rose, 1997; Tesarz, Schuster, Hartmann, Gerhardt & Eich, 2012).
Accordingly, it is still unclear if this high ability to perceive and detect body signals in dancers due to training can be generalized to different sensory modalities. The purpose of this investigation was to compare the variability in pain reporting skills using FAST and the variability in reporting other sensory modalities tasks. In other words, the main goal was to understand how dancers, known to evidence increased interoception accuracy and exposed by long-term pain, would report pain, and how that relates to accuracy in other sensory modalities such as heartbeat and taste.
2. Literature Review
Life’s most fundamental basis is that it needs a constant preservation of ideal parameters, for example levels of oxygen, glucose, ion concentration or temperature to survive, and that is accomplished through the brain and his many neural pathways. It is vital the existence of brain areas that can detect and evaluate the distance of those parameters. This dynamic process is called homeostasis, accomplished through a brain’s mechanism that enables a continuous track of the living organism state, integrating numerous signals from the body and thus assessing the ongoing body’s state (Damasio & Carvalho, 2013). Three interdependent mechanisms, based on negative feedback, are necessary for each of their own specific parameter: The receptor, the control center and the effector. The receptor detects and sends the information, the main control centers, located in the brainstem and hypothalamus, correct the imbalance, and the effector is the target where it acts on (Cooper, 2008). Homeostasis, as a broader concept, can be found in all levels of the body, from the cellular to the autonomic, neuroendocrine and behavioral responses (Schulkin, 2004). The first theory describing the need for regulating the internal environment (milieu interieur) is due to Bernard in 1865 and later developed by Cannon (1926) coining the term homeostasis. Hitherto, both pain and interoception are believed to be homeostatic functions (Craig, 2003; Damásio & Carvalho, 2013).
2.1 Pain
According to Craig (2003) pain, instead of a previous thought exteroceptive sense or cutaneous sub-modality sensation, is a homeostatic emotion consisting both of a sensation
3
and motivation reaction. It results in autonomic and behavioral responses, and generates a negative affective component, which means sensing an environmental change and consequently producing different levels of action programs. Thus, conscious experience of pain emerges from a physiological condition that subconscious homeostatic systems alone were not able to fix. Behavioral drive and cognitive function are yet other mechanisms to repair pain. For example, significant pressure against a sharp object leads, which is painful, also involves a local vasodilation, an autonomic response, and several behavioral responses, as a retraction of the affected limb, facial muscles forming an expression of pain and the attention focused on the affected body part (Damasio & Carvalho, 2013; Johansen, Fields & Manning, 2001).
Although pain is not necessarily tied to a stimulus, it usually starts as nociception which means transduction of noxious stimuli, from de peripheric nervous system to the central nervous system. First, nociceptors, the sensory receptor neurons that are sensitive to noxious or tissue-damaging stimuli trigger a response and mediate further pain processing. They also respond to chemicals released from the traumatized tissue. Nociceptors possess higher thresholds than mechanical receptors from the somatosensitive system and are divided in three main classes: Thermal, mechanical and polymodal. Mechanical nociceptors are activated by tissue-damaging mechanical stimulus; polymodal nociceptors are activated by noxious thermal or mechanical stimuli and thermal nociceptors are activated by temperatures less than about five degrees or greater than forty-five (Dubner & Gold, 1999; Fitzgerald, 2005; Waxman & Zamponi, 2014). Also, nociceptors, in contrast with mechanoreceptors, have small diameter axons, which fall into C-fiber (unmyelinated) and A-δ fibers (thinly myelinated) (Olausson, 2002). Information enters the spinal cord into Lamina I and Lamina V, and then decussates in the ventral commissure, ascending onto the brainstem, namely reticular formation and parabrachial nucleus, to several thalamus nucleus, specifically ventral posterior lateral nucleus onto primary somatic sensory cortex, ventromedial posterior nucleus onto insular cortex, and medial dorsal nucleus which projects to the cingulate cortex. Sensory processing and pain perception involve temporal summation perceived as fast short-latency (sharp pain) and a slow long-latency (burning pain) (Craig & Andrew, 2002; Vierck, Cannon, Fry, Maixner & Whitsel, 1997). Pain originating on the face is mediated through the trigeminal cranial nerve and trigeminal nucleus (Blomqvist,
4
Zhang, & Craig, 2000; Gieslar, Nahin & Madsen, 1984; Olausson et al., 2002; Waxman & Zamponi, 2014).
This is anatomically denominated the anterolateral pathway, a collection of ascending pathways that, through the anterior portion of the lateral column of the spinal cord, travel and synapse in different brain regions. Besides pain, the anterolateral pathway also mediates temperature and itch (McHugh & McHugh, 2000; Peschanski, Kayser & Besson, 1986; Schnitzler & Ploner, 2000). Still, visceral pain is mediated by another pathway, namely, dorsal horn neurons whose axons ascend in the dorsal columns (Cervero & Connel, 1984; Cervero & Laird, 1999; Schnitzler & Ploner, 2000).
From an individual perspective, pain is considered a conscious experience, regulated by (un)conscious responses, and modulated by numerous factors such as sensory, emotional and cognitive experiences, and that eventually will influence action, learning and regulatory behaviors (Craig, 2009; Pollatos, Füstös & Critchley, 2012; Wiech & Tracey, 2013). The experience of pain is highly individual and subjective, depending on neural and behavioral responses to the painful event, i.e. identical noxious stimulus can produce vastly different and unique pain responses across individuals. Pain suppression, as a survival mechanism, relies on descending information from insula, amygdala and anterior cingulate cortex, using serotoninergic, noradrenergic and dopaminergic circuits to inhibit pain transmission through the periaqueductal gray matter and raphe nuclei (Gebhart, 2004; Suzuki, Rygh & Dickenson, 2004; Treister et al., 2009). Endogenous analgesia is, therefore, the outcome of previous circuits promoting release of endogenous opioids such as enkephalins, endorphins and dynorphins acting both in the central and peripheric nervous system (Akil, Watson, Young, Lewis, Khachaturian & Walker, 1984; Fields, 2004).
Hence, through this system, cognition and emotion modulate and bypass the experience of pain increasing tolerance and thresholds, or on the other hand, lowering it (Apkarian, Bushnell, Treede & Zubieta, 2005; Bushnell, Čeko, & Low, 2013; Craig, 2009). Accordingly, for example, negative emotions may impact the affective component of pain negatively (even though this may depend on other factors, as the arousal of this emotion, for a review Wiech & Tracey, 2013), consequently decreasing pain tolerance, and, on the other and, positive emotion can increase pain tolerance (Carter et a., 2002; Zweyer et al., 2004; Wiech, & Tracey, 2013). Likewise, it is known that expectation or
5
anticipation of pain also enhances greatly their response and suffering (Sawamoto et al., 2000).
At pathological level this can end up in hyperalgesia, an exaggerated pain response to noxious stimuli and/or allodynia, feeling pain as a stimulus that is usually innocuous. These processes are due to peripheral sensitization and central sensitization (Sandkühler, 2009; Sommer, & Kress, 2004). Hence, chronic pain, is currently defined as a reoccurring pain, weeks or months after an experienced pain event, with no longer biological value to withstand their complaints. Likewise, pain management can be extremely difficult to deal with, both as physician and patient and, as a consequence, leads to high prevalence and burden of pain in society (Bushnell et al, 2013; Porreca, Ossipov, & Gebhart, 2002). Because pain is a personal and complex experience, mutually influenced by bottom-up and top-down information, it is a huge challenge to measure, study and treat it (Apkarian et al., 2005; Dworkin et al., 2010; Katz, 2005). Throughout the literature, pain measures rely on constructs such pain thresholds and pain tolerance using typically cold, heat or pressure tasks (Williams & Craig, 2016). These tasks depend on verbal numeric responses (Numerical Rating Scale) of the subjects, indicating pain intensity on a 10-cm line, from “no pain” to “ worst pain imaginable” (Visual Analog Scale), or even a list of adjectives to denote increasing pain intensities, such as “no pain”, “mild pain”, “moderate pain” and “severe pain” (Verbal Rating Scale) (Williamson & Hoggart, 2005). Others rely on self-report measures, as questionnaires.
After an increasing number of clinical trials in which the effect of the drugs did not differ significantly from placebo had been described, Dworkin et al., (2010) claimed that the lack of adequate pain treatments and medication may be a consequence, at least in part, of the failure of analgesic clinical trials in discriminating between effective analgesic compound and placebo, leading to low statistical power. One of the reasons for this fail is believed to be the high variability of participants’ pain scores (Harris et al., 2015), which erodes study power. Quinton & Greenspan (2008) suggests that variation in pain reports is understudied and inconsistency in pain reporting tends to be an unchangeable trait in patients with inconsistent pain reports. Although part of this variability may be caused by real pain processing characteristics such as sensory processing called true variance, another part may be due to error variance, related to any reason, including individuals’ inaccuracies in perceiving and measuring pain. In other words, accurate
6
subjects report pain levels reliably to a similar experience, and proportionally to intensity of the stimulation. Individuals who exhibiting high pain variability may compromise the ability of clinical trial to find the true analgesics’ effect (Treister et al., 2017).
As an attempt to address this issue, it was recently developed the Focused Analgesia Selection Test (FAST) . The FAST measures pain reporting skills, specifically its variability. It was developed to assess pain reporting accuracy by recording subject’s pain reports in response to administration of thermal noxious stimuli of various intensities. Knowing both the intensity of the stimuli and the pain score reported by the subject in response to each stimulus, it allows the assessment of how consistent and reliable each subject is in reporting pain. FAST is not biased by peripheral habituation or sensitization and is well tolerated by individuals (Treister et al., 2017). Recent studies using FAST suggest that, in fact, subjects may differ in their pain reporting skills and that selecting good pain reporters into clinical trials can improve assay sensitivity.
In a two-stage randomized and double-blind trial in patients with painful diabetic neuropathy, Treister et al., (2018) demonstrate that in a first stage directed to training, Accurate-Pain-Report-Training group (APRT), where participants received feedback on their pain report, had lower placebo response and higher accuracy in pain reporting skills opposite to the No-Training group. Hence, it is possible that pain reporting skills might be in fact a trainable skill.
However, reasons explaining these differences on pain reporting skills are still yet to know. Since subjects previous experiences and the need to compare between noxious stimuli in pain tasks has been considered to influence pain report, authors suggest that neuropsychological factors can be related to subjects responses on pain tasks (Koyama, McHaffie, Laurienti, & Coghill, 2005; Shackman et al., 2011). Previous studies suggest a link amongst central sensitization and long-term potentiation, i.e., between pain and memory (Han, Soleiman, Soden, Zweifel, & Palmiter, 2015; Ji, Kohno, Moore, & Woolf, 2003; Price & Inyang, 2015), so it is still an open question if people under pain accuracy assessment could forget noxious stimuli easier than others and so, memory performance could explain some of these differences. Therefore, memory being a complex construct as well, it is measured through a number of test performances. One of them is through memory span, the longest list of items that a subject can reproduce in immediately correct order (Conway et al., 2005). Digit Span Task is neuropsychological measure of
short-7
term memory which consists in reproducing a growing list of numbers previously heard, first in the same order they heard, and then repeating in inverse order. The first task requires immediate memory and the second working memory (Guerreiro, 1998). Other individual characteristics may be involved such as attention to one’s body and the tendency to think about themselves (Nakamura & Chapman, 2002) or even stress (Geva & Defrin, 2018), and so, self-report measures such as Multidimensional Assessment Interoceptive Awareness (Mehling et al., 2012), Self-Consciousness Scale (Fenigstein, Scheier, & Buss, 1975), Perceived Stress Scale (Cohen, Kamarck & Mermelstein, 1994) and Hospital Anxiety and Depression Scale (Zigmong & Snaith, 1983) could help explain these differences.
2.2 Interoception
Homeostatic dynamic processes require maintenance of body’s physiological parameters in optimal levels. Therefore, central nervous system continuously monitors and represent both interior and exterior environments making internal representations based in their sensorial input. Changes concerning the internal environment, like heart rate or levels of oxygen, are sensed by the interoceptive system, a collection of nerve pathways and central nervous system nuclei keen to detect and map homeostatic signals (Damasio & Carvalho, 2013). Specifically, interoceptive system gathers and integrates multisensorial signals sensed by numerous receptors in the viscera and skin, such as nociceptors, chemosensors and baroreceptors, ultimately, influencing individual’s perception of body states. Thus, the brain seems to form a high order percept organization conveying into a cortical interoceptive image located mainly in the insula (Craig, 2009a). Anatomically, there are two main pathways that carry and gather information from the viscera and internal milieu to the brain. One is Lamina I pathway, which consists of C and A-δ fibers that start from every area of the body and carry information regarding the peripheral blood pressure, muscle contraction in vessel walls, temperature, pH, tissue injury and pain (Craig, 2002; Guyenet, 2006; Sato & Schmidt, 1973; Taylor & Rachman, 1988). This pathway projects to Lamina I (posterior horn of grey matter of the spinal cord and trigeminal nucleus), and then ascends to the brainstem, namely nucleus tractus solitarius, parabrachial nucleus, main integration site for all homeostatic afferent activity, and periaqueductal grey matter. These nuclei are connected or project to cortical and
8
subcortical structures, mainly through thalamic nuclei and to posterior insula (Craig, 1995; Farkas, Jansen, & Loewy, 1997; Herbert, Moga, & Saper, 1990; Zhang & Oppenheimer, 2000). Then, information processing is made posterior-mid-anterior insula which, ultimately, will connect to other cortical structures such as anterior cingulate cortex and orbitofrontal cortex, though some lamina I pathway fibers project directly to the insula, bypassing the brainstem (Craig, Chen, Bandy & Reiman, 2000; Craig, 2009a; Craig 2009b; Saper, 1982).
A second pathway develops through the vagus nerve carrying information from the viscera to the nucleus tractus solitarius. It projects to the parabrachial nucleus, periaqueductal gray matter and hypothalamus and, also, to the insula via thalamus (Critchley & Garfinkel, 2017; Herbert, & Saper, 1990). Still, extensive crosstalk information between vagal pathway and lamina I pathway allows the formation of integrated maps of one’s body state. Besides, area postrema, a circumventricular organ, directly senses the internal milieu and projects to the nucleus tractus solitarius and superior colliculus, being a humoral pathway bypassing the blood brain barrier (Critchley & Garfinkel, 2017; Kamermans & Fahrenfort, 2004; Shapiro & Miselis, 1985).
In spite of all physiologically and anatomic studies, neurocognitive construct of interoception has changed across time, lacking a precise definition, having both a restrictive and broader meaning. The initial and more restrictive definition considers interoception as result of sensations only stemming from the viscera (Talland, 1968) and a broader and more recent definition, contemplates interoception as a measure of one’s body state as a total, i.e., multimodal integration in the brain, influenced by emotion, health or well-being (Ceunen, Vlaeyen, & Van Diest, 2016; Dworkin, 2007). These two conceptualizations have wielded an extensive range of scientific areas, such as medicine and psychology, studying topics like pain (Duschek, Montoro, & Reyes Del Paso, 2015), anxiety (Paulus, & Stein 2010), emotions (Wiens, 2005; Critchley & Garfinkel, 2017), eating disorders (Pollatos et al., 2008) and decision making (Dunn et al., 2010).
How these different concepts of interoception relate to each other is still under debate, but both are being used in contemporary research (Ceunen, et al., 2016; Dworkin, 2007). Methodological approaches to measure interoception comprise the use questionnaires and behavioral tests that, either exploit natural fluctuations in internal physiological signals (Heartbeat Task) or manipulate organ physiology experimentally
9
(Water Load Test). Subjects appear to differ substantially on performance regarding interoceptive measures, though reasons for these differences are still yet to be understood (Ceunen, et al., 2016).
Garfinkel, Seth, Barrett, Suzuki & Critchley (2015) dissociate three forms of interoception paradigm, viz. Interoceptive Accuracy, Interoceptive Sensibility and Interoceptive Awareness. Interoceptive Accuracy is assessed via objective tests of interoceptive accuracy where two paradigms were developed: heartbeat discrimination task developed by Katkin, Reed & Deroo, (1983) and heartbeat tracking task established by Schandry, (1981). Heartbeat discrimination task involve the presentation of a periodic external stimuli, like tones or lights. Participants are asked to indicate whether this external stimulus is synchronous or asynchronous with their own heartbeat (Katkin, et al., 1983). Heartbeat tracking task requires participants to feel and count silently their own heartbeats, in rest, without any manual manipulations. This task is repeated several times on specific time windows of 10 to 60 seconds, intertwined with rest periods. At the same time, it is being monitored and recorded participant’s own heartbeats. The closer the two, the greater the accuracy (Schandry, 1981). However, methodological variations of both tasks do exist (Ceunen et al., 2016). Interoceptive Sensibility is defined by the self-perceived dispositional tendency to be internally focused and interoceptively cognizant, in other words, to what extent an individual believes that he can focus and detect internal bodily sensations. This is assessed via subjective self-report measures probing perceived aptitude. One example of these measures is the Multidimensional Assessment of Interoceptive Awareness (MAIA). Interoceptive Awareness is a metacognitive awareness of interoceptive accuracy, i.e., how confident is the person on whether he is accurately or inaccurately assessing their heartbeat. (Garfinkel et al., 2015). Despite the widespread use, these methods have limitations and Kleckner, Wormwood, Simmons, Barrett & Quigley (2015) alert that there is an enhanced performance as the number of trails increase. This may suggest it could be a trainable skill as well.
Nonetheless, heartbeat tasks are not the only measures of interoception. Water Load Test is another frequently used measure (Van Dyck et al., 2016). It was first developed to induce gastric distention and to assess gastrointestinal symptoms in patients with functional digestive disorders. Water Load Test stimulate the stomach using a natural distention stimulus, the ingestion of water without the complex hormonal response of a
10
caloric meal. However interesting, an important limitation of current use this measure concerns the lack of standardization in procedures or instructions (Jones, Hoffman, Shah, Patel & Ebert, 2003; Koch, Hong, & Xu, 2000; Van Dyck et al., 2016).
A few studies correlated both measures, heartbeat task and water load test. For example, and, although studies are scarce, Herbert, Muth, Pollatos, & Herbert, (2012) found that accurate cardioreceptive perceivers also had more accurate perception of sensations that correlates with Water Load Test. Ceunen, Van Diest & Vlaeyen (2013) remain cautious stating that for now, it is premature to generalize beyond what has been found and that is still unknown to what extent, performance in heartbeat detection correlates with other forms of interoceptive sensations. If the correlations between these tasks was true, results from the Heartbeat Tasks or Water Load Test could be considered to reflect accuracy and perception of an overall interoceptive sense. On the contrary, Ferentzi, Bogdány, Szabolcs, Csala, Horváth, & Köteles (2018) results showed that interoception cannot be a generalized feature. Authors measured multimodal interoceptive measures, such as gastric perception, heartbeat perception, proprioception, ischemic pain and, at last, taste perception where correlational analysis showed significant associations only between the same sensorial modality, which means that interoceptive information do not crossover and that information regarding one channel only cannot be possibly generalized. Hence, one of the reasons for different results on these studies concerning interoception is thought to be related with methodological differences, consequently leading to extrapolate hazards.
Growing use of taste task perception concerning interoceptive measures have been lately common to assess sensitivity and accuracy (Ceunen et al., 2016). These tasks usually require individuals to taste different flavors, typically sweet and salt, and rate their respective intensity on a scale, whether NRS or VAS. Additionally, same scales can be used to rate how pleasant or unpleasant flavors are to them, which higher levels correspond to higher subjective perceptions (Ferentzi et al., 2018; Hendi & Leshem, 2014). Taste receptor cells are epithelial cells that transduce chemical stimuli. There are four receptors, each receptor parallels to different taste qualities, namely, sweet, sour, bitter and salty, located on the tongue, palate, pharynx, larynx and epiglottis. Information is then carried ipsilaterally through facial, glossopharyngeal and vagus cranial nerves, responsible also for innervation of the gut, cardiovascular system and lugs. Hence, taste’s
11
neural system is organized towards identifying nutrients and harmful agents, in relation to particular physiological processes, such as maintaining proper energy stores, electrolyte balance, pH and avoid toxins (Bermudez-Rattoni, 2004; Dulac, 2000; Hernes & Gilbertson, 1999).
Another question that remains to be answered is the relation between these interoceptive tasks and pain perception. It is still open to debate the problem of whether the perception pain stimuli and the perception of interoceptive stimuli are correlated and on what level (neural or behaviorally) (Di Lernia, Serino & Riva, 2016). Werner, Duschek, Mattern & Schandry (2009) showed that experience of pain is not correlated with high or low interoceptive sensitivity and that there were no significant relationships between pain experience and cardiac interoceptive sensitivity. This would suggest that peripheral pain pathway is, at someway, partially independent of interoceptive sensations. Moreover, Pollatos et al., (2012) observed that healthy people, with high interoception sensitivity and accuracy measured through heartbeat detection task, demonstrated enhanced pain perception, through decreased tolerance to pain; Borg, Emond, Colson, Laurent, & Michael, (2015) based in questionnaires, found no changes in fibromyalgia patients on interoceptive sensibility. Although, Duschek, Montoro & Reyes Del Paso (2015) demonstrated that fibromyalgia patients exhibited a significantly reduced interoceptive accuracy as well as inverse correlation between interoceptive accuracy and symptoms severity. Thus, the relation between interoception and pain perception in chronic pain conditions is controversial.
2.3 Dancers
It is known that dance training, in particular long-term training, results in significant changes in body, brain function, and its structures (Calvo-Merino, Glaser, Grèzes, Passingham & Haggard, 2004; Hänggi, Koeneke, Bezzola & Jäncke, 2010). Regardless of the dancing genre, dancers are considered athletes with physical training requiring physical load embodiment, comprising numerous hours of training per week or even per day. Dance training demand both aerobic and anaerobic exercises, and similar to other sports, it involves high metabolic energy which makes nutritional and healthy lifestyle play an important optimization role to endure exercise. In addition, optimizing motor fitness skills entails development of strength, balance and flexibility essential to unnatural
12
physical movements and wider range of movements. Flexibility allows for increased range of motion and accomplishes the aesthetic of dance. Muscular strength creates speed and force, making more powerful movement. Thus, dance requisites physical fitness, movement control and automatization as well as effortlessness, only possible through physical training. It is also worth mentioning other common features of dancers, such as competitiveness, performance anxiety and shorter life time job expectancy. Still, variation of these characteristics does happen depending on the dancing style (Ainsworth et al., 2011; Dowse, McGuigan & Harrison, 2017; Koutedakis & Jamurtas, 2004).
Just like athletes, dancers too withstand both acute and long-standing effects of intense exercise such as pain, i.e., joint displacement or induced muscular high metabolic rates. These populations develop special strategies in bearing pain, whether long or short-term. Hence, reluctance in report injuries or ignoring medical advice for rest is a common behavior of dancers mainly due to fear of losing roles or being considered unreliable. Even though it might be of a dancer’s best interest to bear acute lesions, it also may lead to chronic pain and injuries on the long term. Therefore, the more common acute lesions are those by overuse, where intense training needles muscular inflammation, spine and joint displacement, or even lesions on peripheral nerves. If untreated or forced to, it may lead to chronic injuries and chronic pain (Bronner, Ojofeitimi & Spriggs, 2003; Hansen & Reed, 2006; Hincapié, Morton, & Cassidy, 2008; Jacobs et al., 2017).
Following several minutes after exercise, pain thresholds and tolerance seem to increase which suggests endogenous analgesia action (Black, Chesher, Starmer, & Egger, 1979; Koltyn, 2000). It has been described that repeated exposure to high metabolic muscular stress (noxious stimuli through inflammation) enhances muscle pain tolerance (O’Leary, Collett, Howells & Morris, 2017). Moreover, those exhibiting greater endogenous pain modulatory ability, measured by Conditioned Pain Modulation paradigms, a counter-irritation protocol, tolerate better the fatigue exercises (Flood, Waddington & Cathcart, 2017), thus explaining in part the increased tolerance to pain in dancers. Tajet-Foxell and Rose (1995) showed that professional ballet dancers endure high levels of pain, having higher levels of pain thresholds and pain tolerance using Cold Pressure Test, when compared to normal population. The main reasons are thought to be related to highly modulated emotional, motivational and cognitive aspects (Tesarz et
13
al.,2012) granting that most studies describing the pain response of dancers were performed on ballet dancers (Smith et al., 2016).
However, a paradox seems to exist since on the long-term, pain exposure seems to alter physiological parameters differently, in form of peripheral sensitization and central sensitization, which, consequently, alter pain perception (Butha et al., 2001; Victoria & Murphy, 2016) for injuries in the post-dancing career are indeed frequent (Smith et al., 2017). To what extent perception of pain seems to be changed across time or bypassed in dancers, or athletes for that matter, it is still yet to find (Claus & MacDonald, 2017).
Professional dancer’s training involves a strong focus on attention to bodily signals with multisensory integration (especially auditory-motor integration) (Koutedakis & Jamurtas, 2004). Regarding interoception, Christensen, Gaigg, & Calvo‐Merino (2018) showed, for the first time, higher interoception accuracy, using heartbeat detection task, in professional dancers compared to controls. This effect was independent of difference in heartbeats or time-measure intervals. Also important, is that there was a difference in interoception accuracy between less experienced dancers compared to more experienced in favor of the latter. The reasons that can explain these differences in higher interoception accuracy are unknown, but the authors suggest that this may be related to the emotional characteristics of dancing beside its physical training. Further studies are thus needed to corroborate and better understand these findings (Christensen et al., 2018).
3. The present research
Even though it has been described a higher interoception accuracy in dancers, to the best of our knowledge there is only one study on interoception in this population (Christensen et al., 2018). To our best, there are also no studies on other modalities, such as taste. Accordingly, is yet to know if this higher accuracy is related to a higher accuracy in other bodily sensations, specifically in pain and taste. In a previous study from our lab (Agostinho, under review) it was found that that in healthy population interoception accuracy (measured by heart beat task) is not related with the accuracy in reporting pain and taste, thus supporting the claim that interoception accuracy is specific to each modality. Thus, it becomes important to ascertain whether these results sustain in population showing increased interoception ability. Therefore, the first aim of the current study was to investigate if dancers, known for their increased interoception accuracy, are
14
also more accurate in reporting other bodily sensations, such as pain, measured by FAST procedure and taste, measured by a task analogous to FAST.
Extensive literature exists concerning pain in dancers, particularly on pain thresholds and tolerance (Tesarz et al., 2012). These studies found both higher pain thresholds and tolerance compared to healthy populations (Tajet-Foxell & Rose, 1995; Tesarz et al., 2012). However, to our best, the relationship between pain sensitivity and accuracy in dancers has never been investigated. Therefore, the second aim of this study was to investigate if there were relations between pain reporting accuracy, measured by FAST outcome measures and sensitivity to pain, measured specifically through a pain threshold and tolerance task.
Finally, the third aim of the current study is to further investigate if neuropsychological and psychological characteristics could be related to the accuracy in reporting these three bodily signals (pain, interoception task and taste task) in dancers. Granting rather extensive memory studies related to dancers with positive results, they’re related to measure recall of complex non-verbal motor sequences (Stevens, Ginsborg, & Lester, 2011), spatial memory (Cortese & Rossi‐Arnaud, 2010) and comparison between motor and verbal memory of specific dance choreographies (Starkes, Deakin, Lindley & Crisp, 1987). To our best no study addressed specifically short-term memory on a cognitive approach using a neuropsychological measure, digit span task. Additionally, were used four self-questionnaires, Multidimensional Assessment Interoceptive Awareness, Perceived Stress Scale, Self-Consciousness Scale and Hospital Anxiety and Depression Scale as a possible explanation for cross-modal accuracy.
15 4. Methods 4.1 Participants
Undergraduate and graduate dance students were recruited from the Higher School of Dance of Lisbon (Escola Superior de Dança do Instituto Superior Politécnico de Lisboa). Information regarding the study was provided orally to the students during different school activities. Those who voluntarily decided to participate and signed the informed consent were included according to the follow inclusion criteria: age above 18; absence of acute pain at the moment of evaluation or chronic pain condition; absence of psychiatry, cognitive, and /or neurological disorders; no chronic use of medications except for oral contraceptives; completion of pre-selection dance tests, including practical dance evaluations by the dance school; current ongoing attendance of the dance course; a minimal of 3 hour of dance practice per week, professionally or not (Tesarz et al., 2012). Participants were also screened for current medication for pain in the last 48 hours and on daily basis; any uncontrolled chronic medical condition (e.g., uncontrolled diabetes mellitus, unstable ischemic heart disease); persistent or severe infection, drug use with exception of contraceptives.
4.2 Tools and procedures
4.2.1 The Focused Analgesia Selection Test (FAST)
FAST is an instrument designed to assess pain reporting skills when thermal noxious stimuli of varying intensities are applied to ventral surface of the subject’s non-dominant forearm (Treister et al., 2017). It uses the Medoc® Thermal Sensory Analyzer II incorporating a Peltier element-based thermode (30 x 30 mm). The subject rates the pain intensity of each stimulus on a 0-100 numerical rating scale (NRS), in which 0 means “no pain” and 100 “the worst pain imaginable”. The thermal noxious stimuli were applied to ventral surface of the subject’s dominant arm, for the familiarization task, and to the non-dominant forearm for the procedure. The temperature was raised from a baseline of 32°C, peaked for 3 seconds at one out of 7 determined temperatures in random order (44, 45, 46, 47, 48,49, or 50°C). Total stimulus duration was 8 seconds, intertwined with a 15 second interval. Each temperature was presented 7 times in a random block-ordered design (total of 49 stimuli) for each and every subject. The location of the thermode was adjusted every 10 stimuli to every individual to minimize sensitization and/or habituation
16
effects. After each stimulus the subject would rate the pain intensity they perceived through the NRS. Total FAST procedure length was approximately 35 minutes.
The FAST method allows outcome measures such as R2, ICC and Mean CoV. Concerning R2 and based on regression, namely power model regression, it measures agreement (or correspondence) between actual and predicted scores, suggesting that higher scores mean greater accuracy and reliability. The ICC measures the agreement or consistency in responses to the same stimulus over several presentations independent of their order. High value for R2 and ICC denotes a high degree of reliability. Moreover, CoV is the ratio of the standard deviation to the mean, in which average or mean CoV was calculated for every individual based on total mean of every seven mean CoV, i.e., mean of all seven-temperature mean CoV’s. High CoV result suggest a larger variability in individuals’ reporting.
Familiarization task consisted of three stimuli, presented one time in random order between subjects, amongst three different temperatures (44, 46 and 49°C) that the subject should rate after each temperature.
4.2.2 Taste Perception Task
The Taste Perception Task is a modification of the Hendi & Leshem (2014) procedure aimed to assess the sensitivity to sweet and salty taste. In the current study this task was performed according to Agostinho et al (under review) protocol, aimed to assess the accuracy of tastes. Subjects were asked to grade 5 different concentrations for both sweet and salty taste, administered by oral sprays. Preparation of the sprays was as follows: for the most concentrated salty solution (vial 5), 37.45 g of NaCl was added to 250 cc (quarter-litter) of mineral water. For the second solution (vial 4), the first concentration was diluted by 1.5. For the third concentration (vial 3), the first solution was diluted by ratio of 1:3. The last two concentrations were diluted from the third (vial 2) and the fourth (vial 1) concentrations, by 1:3. Preparation of the sugar solution was as follows: The highest concentration (vial 5) was of 67.5 grams of sugar in 250 cc (quarter-litter) of mineral water. The further sprays were prepared by repeated dilution at a ratio of 1:2, except the second concentration (vial 4), that was prepared from the high concentration and diluted in ratio of 1:1. Mineral water with a maximum of 9mg of NaCl /L was used for both the salty and sugar solutions. Subjects were instructed to rate, for
17
each concentration, its intensity on a NRS ranging from 0 to 100, using the 0 for “not feeling flavor” and 100 “most strong flavor”, Between every spray subjects were requested to drink swallow a bit of water, therefore washing their oral cavity. These sprays were applied in pseudo-random order (excluding the subsequent stimulus intensity) and, in each experiment, the order of the test was replaced between the sweet and salty series, making it a total of 25 repetitions for each taste. Subjects also received instructions before the day of the experiment to avoid eating heavy meals drinking any beverages, with the exception of water, one hour before the test session. In accordance with FAST, the taste task outcomes were R2, ICC and CoV.
4.2.3Heartbeat detection task
The heart beat detection task measures accuracy in the perception of one’s heartbeat (Schandry, 1981). The participants were asked to sit still and attend to their heartbeats counting silently, and without manually checking, in four intervals (10, 25, 35 and 45 seconds) while the equipment assessed their true heartbeat, i.e., they sat still for 6 minutes and from that point, when they heard the word “now” they counted the heart beats, and when they heard “stop” they said to the experimenter the counted number. Additionally, after each count subjects were asked to give their confidence, between 0 “no confidence” and 10 “total confidence” on their subjective heartbeat count. Scores of each subject was performed according to the following equation:
Score =1/3[1 – (recorded heartbeats – counted heartbeats) /recorded heartbeats] Furthermore, participants screened physiological recording equipment to assess true heartbeat through electrocardiography, using Ag/AgCl electrodes connected to BITalino device hardware (Plux Wireless Biosignals, SA, Lisbon, Portugal) and Open Signal Software (v.2017) (Kleckner et al., 2015).
4.2.4 Heat Pain Thresholds and Tolerance
Pain thresholds and tolerance on the individual’s dominant forearm were obtained with the Medoc Thermal Sensory Analyzer II . Temperature raised from 30ºC baseline and subjects were instructed to click on a PC mouse, when they would feel a minimal amount of pain, a change from 0 to 100, which the final NRS corresponded to the mean of three attempts. Likewise, between every stimulus was an interval of 15 seconds. The
18
tolerance task consisted of a similar stimulus, but they were required to click only when they felt that they could not tolerate pain any longer, that is, once they feel that the heat reached an unbearable point. Also, Medoc TSA II has a safety measure that stops at 52ºC.
4.3 Neuropsychological assessment 4.3.1 Digit Span task
Digit Span Attention Task is a subtest of Wechsler Memory Scale, designed to assess short-term memory, which is divided in two tasks, frontward and reverse order. In the forward order, individuals were told a list of random numbers, designed by Guerreiro (1998) with growing levels of difficulty, that they have to listen and then reproduce in the same order they heard. Therefore, the first level is a list of 2 numbers and the last level a list of 9 numbers. This is a measure of immediate verbal memory. The reverse order task required listening to another list of random numbers, with the same growing difficulty, but this time they had to reproduce in the opposite order on what they heard. In each task it would be given to the individual a second chance to complete each level, with a different list, only if they missed the first. The reverse order task is a measure of working memory. Thus, this task took around 4 minutes and ended when completed or when the subjects’ failed the two changes of the level. The Portuguese version of this task was validated by Guerreiro (1998).
4.4 Psychological Questionnaires
4.4.1 Sociodemographic questionnaire
Individuals were asked to complete a demographic questionnaire asking questions about their age, sex, height and weight, health condition, medication including contraceptives and consumption habits (alcohol, tobacco, or any other drugs). Subjects specified too the number of years of practice, an estimate of their hours of dancing practice per week and quantify their passion for dance.
4.4.2 Hospital Depression and Anxiety Scale
The Hospital Depression and Anxiety Scale is an instrument of brief application developed for physically ill populations. It determines the levels of depression and anxiety in individuals with no psychiatric medical condition, (Zigmond & Snaith, 1983). This instrument is composed by four-point Likert scale (0-3) with 14 items and two
19
subscales: depression and anxiety, with seven items each. The answers are based on how the subjects felt the last seven days and takes about 2 to 5 minutes to complete. The results will form a range from 0 to 21, for each subscale with the higher score indicating higher levels of depression and anxiety. The Portuguese version of this instrument evidenced good psychometric properties and will be used (McIntyre, Pereira, Soares, Gouveia & Silva, 1999).
4.4.3 Perceived Stress Scale
Perceived Stress Scale is a psychological instrument of brief application for normal population and it measures the degree in which participants’ life are considered as stressful and its impact in one’s life (Cohen, Kamarck, & Mermelstein, 1983). Its questions are related to how unpredictable, uncontrollable and overloaded events are felt by the individual. This instrument has a total of 14 items, divided by 7 positive and 7 negative items, in a five-point Likert scale, with subjects’ answers based on how they have been feeling throughout the last month. Higher scores indicate higher self-perceived stress. The validated Portuguese version is composed by 10 items with good psychometric measures (Trigo, Canudo, Branco & Silva, 2010).
4.4.4 Multidimensional Assessment of Interoceptive Awareness
Multidimensional Assessment of Interoceptive Awareness (MAIA) is an instrument of self-report measure of interoceptive body awareness, aimed to measure between beneficial versus maladaptive interoception attention (Mehling, et al., 2012). MAIA has a total of 33 items and 8 subscales. Each item is answered on a 6-point Likert scale, from 0 – 5, 0 meaning “never” and 5 “always”. Higher total and subscale scores indicate higher levels of positive awareness. Portuguese version include 7 subscales viz. (i) Noticing: awareness of uncomfortable, comfortable and neutral bodily sensations; (ii) Not-Distracting: the tendency to not ignore or distract oneself from sensations of pain or discomfort; (iii) Not-Worrying: the tendency to not react with emotional distress or worry to sensations of pain or discomfort; (iv) Attention Regulation: the ability to sustain and control attention to bodily sensation; (v) Emotional Awareness: the awareness of the connection between bodily sensations and emotional states; (vi) Self-Regulation: the ability to regulate psychological distress by attention to bodily sensations; and (vii)
20
Trusting: experiencing one’s body as safe and trustworthy. Moreover, the Portuguese version of this subscales revealed good psychometric properties (Machorrinho, 2017).
4.4.5 Self-Consciousness Scale
Self-Consciousness Scale aims to assess equally private self-consciousness and public self-consciousness in normal population, being private self-consciousness a tendency to introspect and examine one's inner self and feelings and, public self-consciousness, an awareness of the self as it is viewed by others (Scheier, & Carver, 1985). This instrument is composed of 23 items answered in a 5-point Liker Scale ranging from 0-4, 0 being “extremely uncharacteristic” and 4 “extremely characteristic”. It has 3 subscales: private self-consciousness (10 items), public self-consciousness (7 items) and social anxiety (6 items). This instrument is validated for the Portuguese population, showing good psychometric characteristics (Neto, 1986).
4.5 Procedure
All instruments and materials were prepared prior to the participants’ arrival, as well as an email sent the day before the experiment with instructions to not drink coffee, tea, or alcoholic beverages, not smoking or consume of any substance abuse, and have only a light meal two hours prior the experience . Participants arrived at the study site, specifically an office at local dance college, where explanations regarding the purpose of the study were provided and corresponding inform consent signed. Then participants completed the sociodemographic questionnaire, also designed for inclusion and exclusion criteria. Experimental tasks started with FAST procedure, namely instructions and the familiarization task, followed by FAST procedure per se, and then digit span task in the pause until the heat thresholds and tolerance tasks. Next, heartbeat detection task was performed, in which electrodes were placed by the participants according to researcher instructions and consequently verified. Afterward, the taste perception task was performed, first with one of the two flavors, then the remaining questionnaires as a break between the two tastes, finishing with the remaining flavor; salt or sugar first was performed randomly between subjects. Each participant received a code number, which was used along the data analysis. The results and the documents derived from this study
21
were analyzed for the total cohort without any mention to one’s identification. For each participant, there was an estimate time of one hour and a half.
4.6 Statistical Analyses
Data was collected and processed via Excel (Microsoft Corp, Redmond, WA, USA), and was analyzed by using the SPSS software version 24 (SPSS, Inc., Chicago, IL, USA). Descriptive statistics were used to present demographic and baseline characteristics. Since data failed normality tests regarding ANOVA repeated measures, it was analyzed with nonparametric tests. Friedman’s tests (followed by Wilcoxon post hoc test, when applicable) used to assess differences in pain and taste (sugar and salt) scores. Spearman’s correlations were used to assess relations between the accuracy tasks (FAST and taste) and interoception tasks, as well associations with pain-related psychological questionnaires. Statistical significance is defined as P≤0.05.
22 5. Results Participants demographic characterization
Thirty-three undergraduate and graduate students (twenty-six women) from a local dance university, aged between 18 and 24 (M=19.67; SD=2.03) with 3 to 18 years of dance practice (M=11.12; SD=3.83). Demographic data from the study population can be found in table 1.
Table 1.
Demographic Characterization of the study population (n=33)
Mean Frequency (%) Minimum Maximum
Age 19.67±2.03 18 24
Body Mass Index 20.85±1.78 17.48 25.18
Years of Practice 11.12±3.83 3 11
Passion for Dance 90.58±9.08 70 100
Sex Female 26 (79%) Male 7 (21%) Education High School 25 (76%) Graduate 8 (24%) Pain Assessment Pain Accuracy
FAST Mean pain scores
Descriptive statistics of mean pain intensity of each FAST temperature is shown in graphic 1. Mean pain scores ranged from M=7.04 and SD=5.84 for 44ºC, the lowest intensity stimulus, to M=59.29 and SD=25.36 for the 50 ºC, the highest intensity stimulus. Friedman Test revealed significant statistical differences between participants scores given to different stimuli intensities (Friedman, χ2= 177.74, P=0.000). Additionally, Post hoc Wilcoxon test showed significant differences amongst scores of each stimuli intensity, specifically between temperature 44 ºC and 45 ºC (Z= -3.622; P=0.00), 45 ºC and 46 ºC (Z= -2.244; P=0.025) 46 ºC and 47 ºC (Z= -3.539; P=0.00), 47 ºC and 48 ºC
23
(Z= -4.021; P=0.00), 48 ºC and 49 ºC (Z= -4.798; P=0.00) and, at last, between 49 ºC and 50 ºC (Z= -5.013; P=0.00).
Figure 1: Graphic bars of mean and standard deviation of pain scores (NPR) in response to each FAST stimulus temperature.
FAST Outcome measures
FAST outcome measures can be found in table 2. R2 had an average M=0.493 with a SD= 0.130, including a minimum of 0.286 and a top of 0.702. Moreover, ICC had an average score of M=0.687 and SD=0.097 with a minimal score of 0.502 and a maximal of 0.822. Finally, CoV had a mean score of M=0.751 with SD=0.305, and a lowest score of 0.275 and a highest score of 1.479.
Table 2.
FAST Outcome measures
R2 ICC CoV Mean (SD) 0.493 (0.130) 0.687 (0.097) 0.751 (0.305) Median 0.494 0.703 0.714 Minimum 0.286 0.502 0.275 Maximum 0.702 0.822 1.479 0 10 20 30 40 50 60 70 80 90 100 M ea n N RS Temperature (°C) 44 45 46 47 48 49 50
24 Pain sensitivity
Descriptive statistics on pain sensitivity measures can be found in table 3. Mean thresholds revealed a minimum of 36ºC temperature and a maximum of 51 with an average threshold temperature of M= 45.24ºC and SD=3.42 for the least amount of pain. Furthermore, tolerance revealed a mean temperature of M= 49.05 and a SD=5.34 with a minimal tolerance of 48.8 and a maximal of 52ºC.
Table 3.
Descriptive Statistics of Pain Sensitivity Measures (mean heat pain threshold and mean heat pain tolerance).
Heat Pain Thresholds (°C)
Heat Pain Tolerance (°C) Mean (SD) 45.24 (3.42) 50.41 (0.90) Median 46.33 50 Minimum 36.0 48.8 Maximum 51.0 52.0 Taste Task
Mean taste scores
Descriptive Statistics of mean salt and sugar intensities are depicted in graphic 2. Mean taste intensities ratings for salt ranged from M=1.04 and SD=2.37 concerning the lowest intensity stimuli to M=35.60 with SD= 18.32 for the highest intensity stimuli. Friedman Test revealed significant statistical differences between mean intensity ratings for different salt stimuli intensities (Friedman, χ2= 198.93, P=0.000). Furthermore, post hoc Wilcoxon test showed significant differences amongst all mean intensities scores, specifically between Salt 1 and Salt 2 (Z= -4.93; P=0.00), Salt 2 and Salt 3 (Z= -5.01; P=0.00) Salt 3 and Salt 4 (Z= -4.096; P=0.00), and finally Salt 4 and Salt 5 (Z= -5.013; P=0.00).
Sugar descriptive statistics are presented in graphic 2 . Sugar 1 had a mean intensity score of M=1.62 and SD= 3.60 and Sugar 5 a mean of M=35.88 and SD=21.03. Friedman Test showed significant differences between each stimuli intensities (Friedman, χ2= 120.63, P=0.000), and post hoc Wilcoxon test showed significant differences amid all intensities scores, specifically, between Sugar 1 and Sugar 2 (Z= -3.51; P=0.00), Sugar 2
26
Minimum 0.135 0.338 0.232
Maximum 0.878 0.934 1.250
Interoception
Heart beat detection task
The overall result of Interoception accuracy task are presented in table 4. The mean heartbeat detection score was M=0.422 and SD=0.316, with a lowest score of 0 and a highest score of 0.993. Thus, these results suggest a high variability of subjects scores in response to this task.
Table 5.
Descriptive statistics of the Heart beat detection task scores
Mean ±SD Minimum Maximum
Interoception Score 0.422±0.316 0.000 0.993 Neuropsychological task
Digit Span
Average scores of Digit Span task can be found in table 7.
Table 6.
Digit Span Task
Mean ± SD Minimum Maximum
Direct Order 5.76± 0.83 4 7
Inverse Order 4.61± 1.01 2 7
Total 10.36± 1.64 7 14
Psychological Questionnaires
Descriptive statistics of the scales and subscales used to assess psychological characteristics can be found in table 8.
27 Table 7.
Descriptive Statistics of the Questionnaires scores
Mean ±SD Minimum Maximum
HADS
Anxiety Subscale 10.12 ± 3.97 2 19
Depression Subscale 5.18 ± 2.65 1 11
Total 15.30 ± 5.10 4 24
Perceived Stress Scale 22.33± 3.23 15 29
MAIA
Noticing subscale 11.97 ± 2.186 5 15
Not Distracting subscale 5.06 ± 4.394 0 17
Not Worrying subscale 11.91 ± 3.565 4 18
Attention Regulation subscale 24.09 ±5.288 15 33 Emotional Awareness subscale 20.30± 3.729 11 25 Self-Regulation subscale 9.12 ±3.130 2 15 Trusting 11.33 ±2.146 6 15 Self-Consciousness Scale Private Consciousness 28.70± 2.65 15 40 Public Consciousness 20.39± 4.690 12 27 Social Anxiety 12.70± 5.682 1 23 Total 61.79± 8.302 43 77
Correlations between pain reporting accuracy and accuracy in other modalities
Positive correlations were found between FAST CoV and Sugar CoV (Spearman’s r=0.356, P=0.042), meaning that those more accurate in pain reporting were more accurate in the sugar task. Correlations between Interoception, measured by the heartbeat detection task and FAST outcomes were not found, as well as between Interoception and taste task outcomes.
28 Correlations within the same modality
There were positive correlations between ICC of Salt and Sugar (Spearman’s r=0.508, P=0.003), meaning that those more accurate in reporting salty intensities were also more accurate in reporting sugar intensities. No other correlations were found in the other outcome measures.
Correlations between FAST and pain sensitivity
No correlations were found between FAST outcome measures and both pain thresholds and tolerance, i.e., between mean heat pain threshold and R2 (r= -0.212, P=0.253), ICC (r=0.273, P=0.125) and CoV (r= -0.93, P=0.606) nor between heat pain tolerance and correspondingly FAST measures ( R2, r= -0.175, P=0.346; ICC, r=0.285, P=0.108; CoV r=0.017, P=0.924).
Correlations between interoception and pain sensitivity
There was an inverse correlation between interoception and mean pain thresholds (Spearman’s r= -0.396, P=0.023), which means that subjects with high interoception accuracy had lower heat pain threshold. There were no correlations between between interoception accuracy and pain tolerance (Spearman’s r= -0.319, P=0.070).
Correlations between FAST and neuropsychological tasks
There was a positive correlation between inverse digit span and CoV (Spearman’s r=0.364, P=0.037). Thus, subjects with higher performance on this memory task had higher pain reporting ability. No other significant correlations were found between this digit span task measures and the other two sensorial modalities (taste and interoception).
Correlations between accuracy and dance experience
Years of dance practice correlated with FAST measure ICC (Spearman’s r=0.447, P=0.009). Those with more years of dance experience had higher pain reporting accuracy. Years of dance practice did not correlate with mean thresholds (Spearman’s r= -0.073, P=0.685) or pain tolerance (Spearman’s r= 0.106, P=0.559). However, positive correlations were found between passion for dance and pain threshold (Spearman’s
29
Spearman’s r=0.358, P=0.041). No other correlations were found between dance experience and accuracy and pain sensitivity tasks.
Correlations between outcomes and psychological characteristics
There was a significant correlation between SCC Social Anxiety subscale and salt outcome measures, R2 (Spearman’s r=0.351, P= 0.045), ICC (Spearman’s r=0.381, P=0.029) and CoV (Spearman’s r= -0.492, P=0.04). Thus, the higher the social anxiety the more accurate in perceiving salt intensities. No other correlations were found between SCC and HADS and other task outcome.
Still, MAIA questionnaire correlated in one subscale with FAST Outcome measures, Attention Regulation with FAST CoV, (Spearman’s r=0.392, P=0.024). Furthermore, Not Distracting MAIA Subscale correlated with taste task outcome measures, specifically a negative correlation with ICC in salt (Spearman’s r= -0.354, P=0.043), which means higher the distraction, lower the accuracy. We also found a positive correlation with CoV (Spearman’s r=0.419, P=0.015) from salt, that means higher levels of distraction, higher the variability in subject’s accuracy . In terms of sugar, it was found positive correlations, namely R2 (Spearman’s r=0.411, P=0.019), meaning higher levels of distraction, higher precision in regression models, and ICC (Spearman’s r=0.350, P= 0.046) which means higher levels of distraction, higher values for accuracy. No other correlations were found.