SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Epidemiological
profile
of
patients
diagnosed
with
athletic
pubalgia
夽
Anderson
Luiz
de
Oliveira
∗,
Carlos
Vicente
Andreoli,
Benno
Ejnisman,
Roberto
Dantas
Queiroz,
Osvaldo
Guilherme
Nunes
Pires,
Guilherme
Guadagnini
Falótico
UniversidadeFederaldeSãoPaulo,DepartamentodeOrtopediaeTraumatologia,CentrodeTraumatologiadoEsporte,Sa˜oPaulo,SP, Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22January2016 Accepted7March2016
Availableonline26October2016
Keywords:
Athleticinjuries Pubicsymphysis Hernia
Sports
a
b
s
t
r
a
c
t
Objective:Toevaluatetheclinicalandepidemiologicalcharacteristicsofpubalgiainpatients fromaSportsMedicineCenter.
Methods:Dataanalysisfrommedicalrecordsofpatientswithathleticpubalgiaattended tofromJanuary2007toJanuary2015.Thediagnosiswasmadebyanexperiencedhip sur-geon,complementedwithpelvicX-ray,abdominalwallultrasound,andmagneticresonance imagingofthepelvis.
Results:Among43patients,42weremen,withmeanageof33years.Asforsports,25(58.1%) athletesweresoccerplayersand13(30.2%)wererunners;37.2%wereprofessionalathletes. Inguinalherniawasdiagnosedin20.9%ofpatients,showingtheimportanceofitsroutine searchinthesepatients.Treatmentdurationrangedfrom1to12monthsand95.2%ofthe patientsreturnedtosport.
Conclusion:Thisstudypresentedtheepidemiologicalcharacteristicsofpatientsdiagnosed withathleticpubalgiaattended toina referencemedicalcenteranddemonstratedthe prevalenceofthislesioninmalepatients,soccerplayersandrunners.Italsodisclosed ahighsuccessrateofthenonoperativetreatment,andhighrateofreturntosportafter treatment.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
IworkattheSportsTraumatologyCenter(CETE),DepartmentofOrthopedicsandTraumatology,FederalUniversityofSãoPaulo,São Paulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.L.Oliveira). http://dx.doi.org/10.1016/j.rboe.2016.10.011
Perfil
epidemiológico
dos
pacientes
com
diagnóstico
de
pubalgia
do
atleta
Palavras-chave:
Traumatismosematletas Sínfisepubiana
Hérnia Esportes
r
e
s
u
m
o
Objetivo: Avaliar as características clínico-epidemiológicas da pubalgia do atleta nos pacientesdeumcentrodereferêncianoatendimentoaesportistas.
Métodos: Avaliac¸ãodosprontuáriosdepacientescompubalgiadoatletaatendidosentre janeirode2007ejaneirode2015.Odiagnósticofoifeitopeloexameclínicofeitopor ortope-distapós-graduadoemquadril,complementadocomradiografiadebacia,ultrassonografia deparedeabdominaleressonânciamagnéticadapelve.
Resultados: Dos43pacientesavaliados,42eramhomens,commédiade33anos.Quantoaos esportes,25(58,1%)atletaspraticavamfutebole13(30,2%)eramcorredores;37,2%eram atle-tasprofissionais.Foidiagnosticadahérniainguinalem20,9%dospacientes,oquedemonstra aimportânciadesuapesquisarotineiranessespacientes.Adurac¸ãodotratamentovariou deuma12mesese95,2%dospacientesretornaramaoesporte.
Conclusão: Opresenteestudoapresentaascaracterísticasepidemiológicasdospacientes comdiagnósticodepubalgiadoatletaatendidosnumcentrodereferênciaedemonstrao predomíniodessalesãonospacientesdosexomasculinopraticantesdefuteboledecorrida. Mostratambémaltataxadesucessodotratamentonãooperatório,bemcomoelevadoíndice deretornoàpráticaesportivaapóstratamento.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Pain in the groin area and the pubis is common cause of abandon and retirementinmany sports, whichshows the importanceofdiagnosis andtreatmentinthispopulation.1 The differential diagnoses include athletic pubalgia, intra-articular hip pathologies (such as labral/femoroacetabular impingement),traumaticmyotendinousruptures(hip adduc-tors,rectusabdominis),anddiseasesoftheabdominalwall, especiallyinguinalhernias.2
Athleticpubalgia ischaracterizedbychronicpaininthe pubic or inguinal area, associated with physical exertion in sports that require sudden changes in the direction of movement or repetitive kicks. The most common sports, in decreasing order of incidence, are: soccer, ice hockey, Americanfootball,athletics,baseball,basketball,tennis,and swimming.1,2 Data from MajorLeagueSoccerand fromthe National Hockey League in the United States suggest that 9–18%oftheirathletessufferorhavesufferedsomesortof discomfortcompatiblewithathleticpubalgia.3
A search for articles in Portuguese demonstrated the scarcityofpublicationsonthesubjectinBrazil.
Theobjectiveofthisstudywastoevaluatetheclinicaland epidemiologicalcharacteristicsoftheathletic pubalgia ina sports traumatology service, and to establish a correlation withthesportspracticed,gender,age,andrateofreturnto thesportaftertreatment.
Material
and
methods
Inthisobservationalstudy,themedicalrecordsofallpatients attendinganoutpatientsportshipclinicfromJanuary2007to
January2015weremanuallyanalyzed.Forthepresentstudy, onlychartsofpatientswithdefinitediagnosisofathletic pub-algia(59)were included.Ofthese,15 wereexcludeddueto lossoffollow-upandonerecurrenceofthecondition.Thus, theanalyzedsamplewascomposedof43patients.Inthe med-icalcharts,datawererecordedinaprotocolofcareforthese athletes(Appendix1).Physicalexaminationwasperformed bytheorthopedicsurgeonresponsibleforthehipclinicatthe timeofcare.
Criteriausedfordiagnosisofathleticpubalgiawere pres-ence of insidiousand progressivepain inthe pubic region and/or adductor zone; positive clinical test (squeeze test and adduction againstresistance) and hip radiographwith hyperdensityinthepubicsymphysiswithorwithoutthe pres-ence of osteophytes, or positive flamingo test (asymmetry in the pubic symphysis greater than 2mm). The radio-graphicchangesshouldbecomplementedbyultrasound,with evidenceofalteredechogenicityoftheadductorlongus ten-don, with chronic aspect, and absence of abdominal wall hernias. In the cases of diagnostic uncertainty after clini-calexamination,radiography,ultrasonography,andmagnetic resonance imaging(MRI) of the pelvis was requested.The diagnosis was defined classically by signal change in the aponeurosis of the adductor longus tendon and/or rectus abdominalis.4–7
The variables were analyzed descriptively with the rel-evant descriptivemeasures: mean,standarddeviation(SD), quartiles (Q1:first quartile,Q2: median,Q3: thirdquartile), minimum and maximum valuesfor quantitativevariables, andabsolute(n)andrelativefrequency(%)forcategorical vari-ables.
Therecurrencerateandits95%confidenceintervalwere estimatedbytheWilsonmethod.
Table1–Descriptiveanalysisofthesampleof43 patients.
Age(years)
Mean(SD) 32.8(12.4)
Median 31
Minimum–maximum 16–67
Age–n(%)
<20years 4(9.3)
20–29years 16(37.2)
30–39years 12(27.9)
40–49years 5(11.6)
≥50years 6(14.0)
Gender–n(%)
Female 1(2.3)
Male 42(97.7)
Sport–n(%)
Athletics 10(23.3)
Athleticsandcapoeirafight 1(2.3)
Athleticsandswimming 1(2.3)
ClassicalBallet 1(2.3)
Basketball 1(2.3)
Cyclingandsoccer 1(2.3)
Circusandfootball 1(2.3)
Soccer 22(51.2)
Soccerandathletics 1(2.3)
Jiujitsu 1(2.3)
Judo 1(2.3)
Karate 1(2.3)
Rodeo 1(2.3)
Category–n(%)
Amateur 21(48.8)
Professional 16(37.2)
Recreational 6(14.0)
Dominance–n(%)
Left 9(20.9)
Right 34(79.1)
Resistancetraining–n(%)
No 25(58.1)
Yes 18(41.9)
Frequencyofresistancetraining–n(%)
None 25(58.1)
1x/week 2(4.7)
2x/week 8(18.6)
3x/week 6(14.0)
4x/week 2(4.7)
Timebetweensportinitiationandsymptomonset(years) (n=30)
Mean(SD) 11.7(8.6)
Median(Q1;Q3) 10(5;17.25)
Minimum–maximum 1–40
Timebetweensymptomonsetanddefinitivediagnosis(months)
Mean(SD) 9.2(10.9)
Median(Q1;Q3) 6(3;12)
Minimum–maximum 1–53
Diagnosespriortothedefinitivediagnosis–n(%) (n=42)
No 40(95.2)
Yes 2(4.8)
Otherorthopedicpathologies–n(%)
No 29(67.4)
Yes 14(32.6)
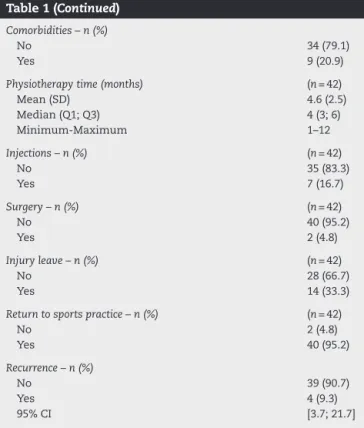
Table1(Continued)
Comorbidities–n(%)
No 34(79.1)
Yes 9(20.9)
Physiotherapytime(months) (n=42)
Mean(SD) 4.6(2.5)
Median(Q1;Q3) 4(3;6)
Minimum-Maximum 1–12
Injections–n(%) (n=42)
No 35(83.3)
Yes 7(16.7)
Surgery–n(%) (n=42)
No 40(95.2)
Yes 2(4.8)
Injuryleave–n(%) (n=42)
No 28(66.7)
Yes 14(33.3)
Returntosportspractice–n(%) (n=42)
No 2(4.8)
Yes 40(95.2)
Recurrence–n(%)
No 39(90.7)
Yes 4(9.3)
95%CI [3.7;21.7]
ThestudywasapprovedbytheResearchEthicsCommittee throughthePlatformBrazil,undertheCertificateof Presenta-tionforEthicalAssessment(CertificadodeApresentac¸ãopara Apreciac¸ãoÉtica[CAAE])No.1993615.5.0000.5505.
Results
Patients were predominantly male (97.7%), and ageranged from16to67years,mean32.8years(SD=12.4years).
Regardingsports,itisnoteworthythat25(58.1%)athletes practicedsoccerand13(30.2%),athletics.Asforthecategory, 37.2%(16patients)wereprofessionalathletes,whopracticed athletics(two),classicalballet,circus,soccer(ten),judo,and karate.
Ofthe25soccerplayers,14reportedaposition:21.4%were strikers;14.3%,goalkeepers;14.3%,full-backs;7.1%,right mid-fielders;7.1%,leftmidfielders;and35.7%,defenders.
Most patientswere right-handed(79.1%)and 41.5% per-formedresistancetrainingonetofourtimesaweek.
Thetimebetweenstartofthesport andsymptoms var-iedbetweenoneand40years,withamedianoften(Q1=5 years;Q3=17);thetimebetweensymptomonsetand defini-tivediagnosisrangedfromoneto53months,withamedian ofsixmonths(Q1=3;Q3=12months).
injury,synovialplicaintheknee,andanteriorkneepain syn-drome.
Non-orthopedic diagnoses were present in 20.9% of patients;allthesediagnoseswereofinguinalhernia.
Therapyduration variedfrom oneto12months,with a medianoffour(Q1=3months;Q3=6months).
Asfortheothertreatments,16.7%ofpatientshadbetween oneandsixinjectionsand4.8%underwentsurgery:tenotomy oftheadductorlongusanddebridementofthepubic symphy-sis.
Regardinginjuryleaves,33.3%ofpatientsrequiredleaves ofonemonthtooneyearand95.2%returnedtothesport;only onepatientsubjectivelyreportedareturntoalevelinferiorto thatpriortotheinjury.
Reoccurrenceswereobservedinfourpatients(9.3%),with the95%CIrangingbetween3.7%and21.7%.
Table 1 presents the detailed analysis of the results observedinthesampleof43patients.
Discussion
Itisbelievedthat athleticpubalgiahasamultifactorial eti-ology;twotheoriesarenoteworthy.Thefirstisbasedonthe conceptofmuscleinjuryinthepubicsymphysis,popularized byTayloretal.,3Gilmore,8andWilliamsandFoster.9 Consid-ering the pubic symphysisas a fulcrum, the imbalance of forcesbetweenthe(weakened)abdominalmusclesandthe hipadductorsleadstoinjuryoftheabdominalmuscles.3,8,9 Thesecondtheoryinvolvestheconceptofhiddenhernia (pre-hernia,incipienthernia)secondarytoadefectoftheposterior walloftheinguinalcanal(formedbythetransversefascia), whosediagnosiscanbeconfirmedthroughthevisualization ofaprotuberanceintheposteriorwalloftheinguinalcanal duringdynamicultrasonography(Valsalvamaneuver).10,11 A literaturereviewarticleproposedthatthesetheoriesshouldbe merged;thatis,themuscleinjury(singleormultiple microle-sions),whichinvolvesoneormoremuscles/pubicstructures (e.g.,theaponeurosisofthe externalobliquemuscle,rectus abdominalis,conjointtendon),wouldsecondarilycausethe incipienthernia,butthemuscleinjurywouldbethesourceof pain.12
Morerecentclinicalandbiomechanicalstudiesalso postu-latefemoroacetabularimpingement(FAI)asanotherpossible precursorofathleticpubalgia.Thedecreaseinthe internal rotationamplitudeofthehipinpatientswithFAIcausesan increasein the physiological rangeof motionofthe pubic symphysis.Inathletes withhighdemandon thehip joint, FAIwouldtriggerinjuryduetopubicsymphysisoverload.13,14 Recentliteratureshowsanassociationofpubalgia withhip diseasesin15%ofcases.15
Thesyndromeismore commonin men;inthe present study,therewasonlyonefemale,anamateursoccerplayer. Itis believed that the gynecoid pelvis actsas a protective factorforthe disease,probablyduetothegreaterinsertion area to the abdominal muscles, which would increase the surface for the distribution of forces.12 Nevertheless, in a studywith8,490patients,Meyersetal.15observedanincrease from1%to15%inthenumberofwomenaffectedinthelast 20years.
The syndrome has an insidious characteristic; the ath-lete usually seeks care several months after the onset of symptoms. Evenwithpain,it isnotedthatthe patientcan compete despite losing performance during the competi-tion/season.Adecreaseintheintensityoftrainingcanalsobe observed, butnotnecessarilyabsencefrom competitions.12 In the present study, one-third of patients required injury leave.
Thepubicregionhasbeencharacterizedasthe“Bermuda Triangle”ofsportsmedicine,duetothechallenging diagno-sisinthisanatomicalregion.Thesyndromelacksadefinitive diagnostic criteria and, therefore, the diagnosis should be madebyexclusion.16,17Hippathologies(labraltear,IFA)and injuries ofthe adductor muscles are difficult to differenti-ateandmayevencoexist.Stressfracturesofthepelvisand hip should alsobeincluded in thedifferential diagnosis.17 Genitourinarydiseasessuchasepididymitis,prostatitis,and testicular tumors should be ruled out in men, as well as intrapelvic diseases in women, such as endometriosis, ovarian cysts, and inflammatory pelvicdisease. Inflamma-tory/infectiousdiseasessuchasinflammatoryboweldisease, diverticulitis, urinary tract infection, and osteomyelitis, as wellastumorlesions,shouldbeexcluded.12Inthisstudy,nine patients were diagnosed with inguinal hernia; ultrasounds are routinelyperformedinthisservice.Ofthefivepatients whounderwentconventionalherniarepairperformedbythe general surgery team of the institution, two evolved with persistent symptoms of pubalgia, which demonstrates the diagnosticchallenge,suggestingthecoexistenceof patholo-giesindifferentsystemsandthattheinguinalherniaisnotthe singlecausepainintheathleticpubalgia.12,15Meyersetal.15 observedthat4.6%of5460patientsoperatedforpubalgiahad previouslyundergonetraditionalherniarepairwithout suc-cess.
Therecommended initialtreatment isconservative and consists of rest, physical therapy, and non-steroidal anti-inflammatoryinjectionwithcorticoidsintheinsertionregion oftherectusabdominisandadductorlongusmuscles.Surgery is indicated in cases of failure of conservative treatment, whichisstipulatedtohaveameandurationofthreemonths.12 In thepresent study,asuccessrateof95.2% wasobserved intheconservativetreatment.Thetwopatientswho under-wentsurgicaltreatment(adductortenotomyandoneadductor tenotomyassociatedwithtrapezoidalresectionofthepubic symphysis)developedrecurrenceofthepainfulclinical pic-ture,butwerelosttofollow-up,andthustheexactcausesof recurrencewasnotdetermined.AccordingtoMeyerset al., thereareatleast17anatomicalstructuresaroundthepubic symphysis that may be altered in athletic pubalgia, in an isolatedorcombinedmanner.15Theseauthorsreportthe pos-sibility of26 differentprocedures that encompass all such structures,withover100possiblecombinationsofprocedures forpatients withmultiplestructuresthatare uni-or bilat-erallyinvolvedwithrespecttothesymphysispubis.Ofthe 5460patientsoperatedbytheauthors,95%returnedtosport practiceaftersurgery.15
Conclusion
Thisstudy presentedthe epidemiologicalcharacteristics of patients diagnosedwith athletic pubalgia attended toin a referencemedicalcenterforathletesanddemonstratedthe prevalenceofthislesioninmalepatients,soccerplayers,and runners.Italsodisclosedahighsuccessrateofnon-operative treatment,andhighrateofreturntosportaftertreatment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Annex
1.
Protocol:
Athletic
pubalgia
Name: _______________________________________________________
Age: ____ Sex: ______
Sport: __________________ Category: __________________________
Position: _____________________ Dominance: Right Left
Frequency of resistance training/week: ______________________________
Time between sport initiation and symptom onset:_____________________
Time between symptom onset and definitive diagnosis (months):__________
Diagnoses prior to the definitive diagnosis: YES NO
Which: ________________________________________________________
Other orthopedic pathologies: YES NO
Which: _______________________________________________________
Comorbidities: YES NO
Which: _______________________________________________________
Treatment:
Conservative Physiotherapy duration: __________________________
Number of injections: _____________
Surgical: _____________________________________________________
Demanded injury leave YES NO Duration: _____________________
Return to sport practice: YES NO At the same level as before the injury: YES NO
r
e
f
e
r
e
n
c
e
s
1. MeyersWC,SzalaiLJ,PotterND,NaikA,RyanJ.Extraarticular sourcesofhippain.In:ByrdJW,editor.Operativehip arthroscopy.2nded.NewYork:Springer;2005.p.86–99.
2.ReisFA,RosenfeldA,IkawaMH,SilvaFD,CostaJD,NatourJ, etal.Aimportânciadosexamesdeimagemnodiagnóstico dapubalgianoatleta.RevBrasReumatol.2008;48(4): 239–42.
3.TaylorDC,MeyersWC,MoylanJA,LohnesJ,BassettFH, GarrettWEJr.Abdominalmusculatureabnormalitiesasa causeofgroinpaininathletes.Inguinalherniasandpubalgia. AmJSportsMed.1991;19(3):239–42.
4.RobinsonP,BarronDA,ParsonsW,GraingerAJ,SchildersEM, O’ConnorPJ.Adductor-relatedgroinpaininathletes: correlationofMRimagingwithclinicalfindings.Skeletal Radiol.2004;33:451–7.
5.CunninghamPM,BrennanD,O’ConnellM,MacMahonP, O’NeillP,EustaceS.Patternsofboneandsoft-tissueinjuryat thesymphysispubisinsoccerplayers:observationsatMRI. AmJRoentgenol.2007;188(3):W291–6.
6.AndersonK,StricklandSM,WarrenR.Hipandgroininjuries inathletes.AmJSportsMed.2001;29:521–7.
7.OmarIM,ZogaAC,KavanaghEC,KoulourisG,BerginD,Gopez AG,etal.Athleticpubalgiaandthesportshernia:MRimaging findings.Radiology.2008;247:3797–807.
8.GilmoreOJ.Gilmore’sgroin:tenyearsexperienceofgroin disruption–apreviouslyunsolvedprobleminsportsmen. SportsMedSoftTissueTrauma.1991;1(3):12–4.
9.WilliamsP,FosterME.Gilmore’sgroin’–orisit?BrJSports Med.1995;29(3):206–8.
10.MuschaweckU,BergerL.Minimalrepairtechniqueof sportsmen’sgroin:aninnovativeopen-suturerepairtotreat chronicinguinalpain.Hernia.2010;14(1):27–33.
11.JoestingDR.Diagnosisandtreatmentofsportsman’shernia. CurrSportsMedRep.2002;1(2):121–4.
12.LitwinDEM,SneiderEB,McEnaneyPM,BusconiBD.Athletic Pubalgia(SportsHernia).ClinSportsMed.2011;30(2): 417–34.
13.BirminghamPM,KellyBT,JacobsR,McGradyL,WangM.The effectofdynamicfemoroacetabularimpingementonpubic symphysismotion:acadavericstudy.AmJSportsMed. 2011;40(5):1113–8.
14.LarsonCM,PierceBR,GiveansMR.Treatmentofathleteswith symptomaticintra-articularhippathologyandathletic pubalgia/sportshernia:acaseseries.Arthroscopy. 2011;27(6):768–75.
15.MeyersWC,McKechnieA,PhilipponMJ,HornerMA,ZogaAC, DevonON.Experiencewithsportsherniaspanningtwo decades.AnnSurg.2008;248(4):656–65.
16.BizziniM.Thegroinarea:theBermudatriangleofsports medicine?BrJSportsMed.2011;45(1):1.
17.HegedusEJ,SternB,ReimanMP,TararaD,WrightAA.A suggestedmodelforphysicalexaminationandconservative treatmentofathleticpubalgia.PhysTherSport.