w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Epidemiological
profile
and
clinical
characteristics
of
patients
with
intestinal
inflammatory
disease
夽
Jhelly
Aparecida
Valcanaia
Arantes
a,b,∗,
Carlos
Henrique
Marques
dos
Santos
c,
Breno
Matos
Delfino
b,d,
Bruno
Alexandre
da
Silva
e,
Rafaela
Maria
Maran
de
Souza
a,
Thaynara
Maria
Maran
de
Souza
a,
Isabella
Demeis
Flávio
a,
Caroline
Gil
Ferreira
a,
Samuel
Bellin
Gomes
da
Cruz
aaUniversidadeAnhangueraUniderp,CampoGrande,MS,Brazil
bHospitalRegionaldeMatoGrossodoSul,CampoGrande,MS,Brazil
cSociedadeBrasileiradeColoproctologia,CampoGrande,MS,Brazil
dUniversidadeFederaldoAcre(UFAC),RioBranco,AC,Brazil
eUniversidadedeAquino(UDABOL),SantaCruzdelaSierra,Bolivia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10February2017 Accepted4June2017 Availableonline13July2017
Keywords:
Inflammatoryboweldiseases Epidemiology
Ulcerativerectocolitis Crohn’sdisease Infliximab
a
b
s
t
r
a
c
t
According toseveralepidemiological studies,thereisa significant increaseincasesof inflammatorydiseaseindevelopingcountries.
Objective:Todescribeepidemiologicaldataandclinicalfeaturesofpatientswith inflamma-toryboweldiseaseinpatientsenrolledinCampoGrande,MS.
Method:Aretrospectivedescriptivestudywithadatabaseanalysisofpatientswhowere enrolledandrenewedtheirprocessintheExceptionalMedicationsProgramoftheHealth DepartmentfromJanuary2008toDecember2016.
Results:423 patientsparticipatedinthe study,260womenand 163men.Ofthese,238 patientshadCrohn’sdiseaseand185hadulcerativerectocolitis.Thepatients’meanage was46years.Themostcommonlyusedmedicationforbothdiseaseswasmesalazineand 34.3%ofthepatientsneededtoswitchtheirmedicationduringthetreatment,mostofthem withCrohn’sdisease.InCrohn’spatients,themostaffectedsegmentwasthecolon(40.6%) andinpatientswithulcerativerectocolitistheentirelargeintestinewasinvolved(78.8%) wasmorecommon.Ofthetotalnumberofpatients,10.8%ofthewomenand18.4%ofthe menneededtouseananti-TNF.
夽
ThisresearchwasconductedattheCoordenadoriaEstadualde AssistênciaFarmacêutica(StateCoordinationofPharmaceutical Assistance)(CAFE)linkedtotheStateHealthDepartmentofCampoGrande,CampoGrande,MS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.A.Arantes).
http://dx.doi.org/10.1016/j.jcol.2017.06.004
Conclusion: MostpeopleontreatmentforIBDarefemale,withameanageof46yearsand sufferingfromCrohn’sdisease.Themostaffectedsegmentsweretheentirelargeintestine inURCcasesandthecoloninCrohn’sdiseasecases.Mesalazinewasthemostuseddrug inbothdiseases.TherewasmoredrugreplacementinCrohn’sdiseasepatients.InCrohn’s disease,youngerpatientsusedinfliximabmorefrequently.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Perfil
epidemiológico
e
características
clínicas
dos
pacientes
com
doenc¸a
inflamatória
intestinal
Palavras-chave:
Doenc¸asinflamatórias intestinais
Epidemiologia Retocoliteulcerativa Doenc¸adeCrohn Infliximabe
r
e
s
u
m
o
Deacordocomváriosestudosepidemiológicos,háaumentosignificativodecasosdedoenc¸a inflamatórianospaísesemdesenvolvimento.
Objetivo: Descreverosdadosepidemiológicosecaracterísticasclinicasdospacientescom doenc¸ainflamatóriaintestinalemCampoGrande-MS.
Método: Pesquisadescritivaretrospectiva,comanálisedosprontuáriosembancodedados, em pacientesquecadastraramerenovaramoprocessonoProgramadeMedicamentos ExcepcionaisdaSecretariadeSaúde,dejaneirode2008edezembrode2016.
Resultados: Participaramda pesquisa423pacientes,260mulherese163homens.Deste total,238possuíamdoenc¸adeCrohne185RetocoliteUlcerativa.Amédiadeidadefoide 46anos.Omedicamentomaisutilizadoemambasdoenc¸asfoiamesalazinae34,3%dos pacientesnecessitaramrealizartrocademedicamentosaolongodotratamento,sendoa maioriaportadordadoenc¸adeCrohn.NospacientescomCrohnosegmentomaisacometido foiocólon(40,6%)enospacientescomRCUfoitodoointestinogrosso(78,8%).Dototalde pacientes,10,8%dasmulherese18,4%doshomensnecessitaramutilizaranti-TNF.
Conclusão: AmaioriadaspessoasemtratamentoparaDIIsãodosexofeminino,commédia deidadede46anoseportadoresdeDoenc¸adeCrohn.Ossegmentosmaisacometidosna RCUfoitodoointestinogrossoenaDoenc¸adeCrohnocolo.Amesalazinafoiomedicamento maisutilizadoemambasasdoenc¸as.HouvemaistrocademedicamentosnaDoenc¸ade Crohn.NaDoenc¸adeCrohnpessoasmaisjovensutilizarammaisoinfliximabe.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Inflammatoryboweldisease(IBD)representsagroupof idio-pathicchronicinflammatoryboweldisorders.This nomencla-tureencompassestwomainnosologicalcategories:Crohn’s disease (CD) and ulcerative rectocolitis (URC), which are characterizedbyanoverlappingofclinicopathological man-ifestationsandbyotherclearlydifferentfeatures.1
IBDs occur throughout the world and represent a seri-oushealthproblemsincethesedisordersaffectpreferentially youngpeople,leadtofrequentrecurrencesandtakeupclinical formsofhighseverity.2
It is believed that the etiopathogenesis of the disease, although not well understood, is related to the abnormal immuneresponsetothebacterialmicrobiotaofthe intesti-nal lumen, which would be associated with changes of the mucosal barrierfunction.There are genetic, socioenvi-ronmental, microbiologicaland immunological factors that wouldalsobeinvolvedasriskfactors,andoftheonsetand maintenanceofthedisease.3
Accordingtotheliterature,withregardtothe epidemiol-ogy,oneobservesaprevalenceofIBDinwhitepeople, who arebetween20and40years,withasecondpeakofthe dis-ease startingat age 55, and with a similar distribution in bothgenders,exceptforCD,inwhichwomenaremoreoften affected.4
Brazil is stillconsidered an area oflow IBDprevalence, despiteasignificantincreaseintheregistriesofthesediseases intheBrazilianliterature.Inthelast20years,CDhas gener-allyexceededURCinincidencerates.Indevelopingcountries whereIBDsareemerging,URCismorecommonthanCD.5
In ourworkingcontext,wenoticed thattherehas been a great increase in the demand for medical care of peo-plewithIBD,andtheepidemiologicalandmorbiditydatain theliteratureareinsufficienttoevaluatetheprofileofthese patients.
Objective
Thegeneralobjectiveofthepresentstudywastodescribethe epidemiologicaldataandclinicalcharacteristics ofpatients withinflammatoryboweldisease.
Method
A cross-sectional and retrospective study was conducted throughadescriptiveresearch,withananalysisofthe medi-calrecordsenteredinadatabase,performedinpatientswith IBDwhowereregisteredandwhorenewedtheirprocessesin theProgramofExceptionalMedicationsoftheDepartmentof HealthintheperiodfromJanuary2008toDecember2016,that is,theperiodinwhichthemedicalrecordsoftheavailabledata began.
Thisstudy was submitted tothe approval ofthe Ethics andResearchCommitteeofHRMSRegionalHospitalandof PlataformaBrasil.Thecostsofthisnon-profitresearchwere fullyfundedbytheresearcher.
Thepatientsstudiedcamefrompublicandprivatehealth systems, residents of the city of Campo Grande in the state of Mato Grosso do Sul and suffering from CD or URC.Thedatastudiedwere obtainedfrommedicalrecords dulyregistered inthe Health Center linked to SESAU, and thediagnosesofthe diseaseswereconfirmedbylaboratory and imaging studies, as well as bymedical consultations, a necessary condition for dispensing higher-cost drugs. Patientswho had inactiveprocesses, who were transferred toanothercity,withtheirtreatmentdiscontinued,and diag-nosedwithanundeterminedcolitis,wereexcludedfromthe sample.
The pharmacological agents used for the treatment of inflammatoryboweldiseasesthatarefundedbythestateare corticoids,salicylates,antibiotics,immunosuppressants,and anti-tumornecrosisfactor(anti-TNF)antibody.
Thevariablesstudiedwere:age,gender,bodymassindex (BMI),diagnosisandlocalizationofthedisease,colonoscopy report,thetherapyusedanddosesavailable,andalsoifthe medicationwaschanged.
Data were collected bythe CEAF program– Specialized ComponentofPharmaceuticalAssistanceoftheMinistryof Health,based onthenumber ofCNSofeachpatient regis-tered;afterthat,thesedatawereenteredandaccountedin tablesfromtheMicrosoftExcelprogram,withstatistical anal-ysiscarriedoutwithuseofSPSS19.0(StatisticalPackagefor theSocialSciences)software,withwhichonecancalculate means,medians,percentages,andstandard deviations.For thecalculations,theUFPaChi-Squaredtestwasappliedforthe formulationofthetables,andANOVAwasusedforthe calcu-lationofmeans.Thestatisticalsignificanceleveladoptedwas
p<0.05.
Results
Duringthestudiedperiod,423activepatientswhorenewed theirclinicalreportsatthehigh-costpharmacyoftheHealth CenterofthecityofCampoGrandewereincludedinthisstudy.
Table1–PlacesofbowelimpairmentinIBD.
Crohn’sdisease(n=208/238) n %
Rectum 113 54.30
Smallintestine 93 44.70
Colon 164 78.80
Rightcolon 84 40.40
Transversecolon 27 13.00
Leftcolon 84 40.40
URC(n=160/185) n %
Rectum 38 23.80
Leftcolon 57 35.60
Theentirelargeintestine 65 40.60
Table2–Medicationsused.
Medication Crohn’sdisease URC
n % n %
Azathioprine 84 35.3 29 15.7
Infliximab 48 20.2 10 5.4
Mesalazine 123 51.7 153 82.7
Adalimumab 80 33.6 10 5.4
Sulfasalazine 3 1.3 3 1.6
Methotrexate 0 0.0 1 0.5
Ofthistotal,238(56.3%)sufferedfromCDand185(43.7%) suf-feredfromURC.Ahigherpercentageofwomen(61.5%)versus men(38.5%)wereobserved;inrelationtoage,ameanof46.01 yearsandamedianof44yearswerefound,withagesranging from9to97years.
Of the total number of patients studied (423), 55 patientswere excludedduetoalackofinformationinthe medical records regarding the affected intestinal segment (a colonoscopy report unavailable). Therefore, of the 208 patientswithCDandwithanavailablereport,themost fre-quentlocationofthediseasewasthecolon(78.8%),followedby therectum(54.3%)andthesmallintestine(44.7%).Ofthe160 patientswithURCandwithanavailablereport,theentirelarge intestine(40.6%),followed bythe leftcolon(35.6%)and the rectum(23.8%)havebeenthesegmentsmoreofteninvolved
(Table1).
Among the medications used by the patients, it was observedthat,inthecaseofCD,themajorityofthepatients were beingmedicatedwithmesalazine(51.7%),followedby azathioprine(35.3%),adalimumab(33.6%),infliximab(20.2%), andsulfasalazine(1.3%).OfthepatientswithURC,the major-ity alsoused mesalazine (82.7%), followed byazathioprine (15.7%), infliximab (5.4%) adalimumab (5.4%), sulfasalazine, andmethotrexate(0.5%)(Table2).
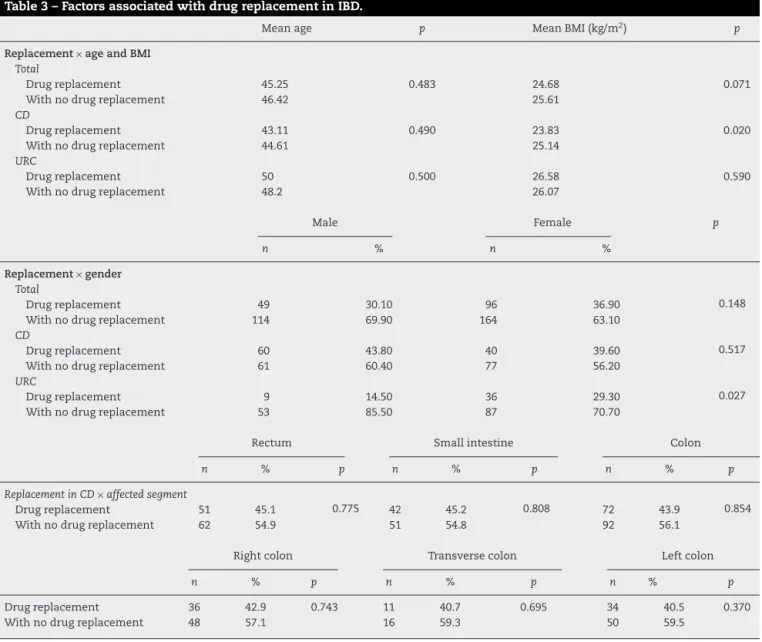
Ofthetotal numberofpatientsstudied, 34.3%switched their medication over time; however, it was not possible to establishthe reasonforthese changes,orto assess the severityofthediseases.Wecouldinquirethat thechanges were more frequent in patients with CD, 100 (42%), com-pared topatients suffering from URC, 45 (24.3%) (p<0.001)
(Table3).
Table3–FactorsassociatedwithdrugreplacementinIBD.
Meanage p MeanBMI(kg/m2) p
Replacement×ageandBMI Total
Drugreplacement 45.25 0.483 24.68 0.071
Withnodrugreplacement 46.42 25.61
CD
Drugreplacement 43.11 0.490 23.83 0.020
Withnodrugreplacement 44.61 25.14
URC
Drugreplacement 50 0.500 26.58 0.590
Withnodrugreplacement 48.2 26.07
Male Female p
n % n %
Replacement×gender Total
Drugreplacement 49 30.10 96 36.90 0.148
Withnodrugreplacement 114 69.90 164 63.10
CD
Drugreplacement 60 43.80 40 39.60 0.517
Withnodrugreplacement 61 60.40 77 56.20
URC
Drugreplacement 9 14.50 36 29.30 0.027
Withnodrugreplacement 53 85.50 87 70.70
Rectum Smallintestine Colon
n % p n % p n % p
ReplacementinCD×affectedsegment
Drugreplacement 51 45.1 0.775 42 45.2 0.808 72 43.9 0.854
Withnodrugreplacement 62 54.9 51 54.8 92 56.1
Rightcolon Transversecolon Leftcolon
n % p n % p n % p
Drugreplacement 36 42.9 0.743 11 40.7 0.695 34 40.5 0.370
Withnodrugreplacement 48 57.1 16 59.3 50 59.5
years (p=0.49). With regard to BMI, we found a mean of 23.83kg/m2 (p=0.02). With regard to the affected segment,
there was no statistically significant difference (p=0.808)
(Table3).
WhenanalyzingpatientswithURCandwithdrug replace-ment, a greater number ofshifts occurred among women (29.3%)versus men(14.5%)(p=0.027).Themean age ofthe patientswas50years,withaBMIof26.58kg/m2.Takinginto accounttheaffectedsegment,norelevantstatistical differ-encewasfound(Table3).
Amongthosepatientswhousedtheanti-TNFagent inflix-imab,the majoritywere men,30 (18.4%)versus women,28 (10.8%)(p=0.026),but nostatisticaldifferencewasobserved betweenmenwithCDandURC. Themeanage ofpatients withCD treatedwith the anti-TNFagent (37.63years)was lowerversuspatientswithCDwhodidnotusethisdrug(46.79 years)(p<0.001).Amongpatientswhousedthe immunosup-pressivedrugazathioprine,therewasnodifferencebetween genders(p=0.742).Thegeneralmeanageofthepatientswas 43.19years(p=0.031).
Discussion
Inthestudiedsample,agreaternumberofwomenwithIBD were observed, which agrees with the findings described in the literature.2,6 Thepeak ofincidence described varies
betweenthethirdandfourthdecadesoflife.1InthecaseofCD,
theliteraturesituatesthehighestincidencevaryingbetween thesecondandthirddecadesoflife.7Inthepresentstudy,the
meansforIBDandCDfallintothefourthdecadeoflife.These dataleadustobelievethataperiodofhighproductivityof thepopulationiscompromised,duetotheimportant reper-cussions on the patients’ quality oflife, motivated by the disease.
CD can affect any partof thegastrointestinal tract, but oftenthemostaffectedsegmentsaretheterminalileumand thecolon.7–9Inoursample,weobservedahighernumberof
patientswithcolon involvement,afinding whichdisagrees withthefindingsintheliterature.
rectosigmoid,35% tothe left colon, and up to 20% ofthe patientssuffer from pancolitis, incaseswherethe disease hasspreadbeyondthesplenicflexure.10Inthepresentstudy,
weobservedahigherfrequencyofpancolitis,whichagrees withthefindingsreportedinthestudybyCabral etal.6 We
werenotabletoclassifytheseverityofthedisease;however, intheevaluationthattookintoaccounttheextensionofthe affectedsegment,wenoticedthatthesamplestudiedcould beatgreaterriskforthedevelopmentofcolorectaldysplasia andneoplasia,sincetheriskvariesaccordingtotheextentof thedisease.10
Thegroupofpatientsmedicatedwithmesalazine consti-tutesthemajorityinbothdiseasesevaluatedinthepresent study.Accordingtotheliterature,thetreatmentofchoicefor URCisdonewithaminosalicylates;usually,thesedrugs,alone orincombinationwithcorticosteroids,maintainthedisease inremission.9,11,12Inthepresentstudy,weobservedalower
needfordrugreplacementinpatientswithURC.
In patients with CD, even though oral mesalazine has proved beneficial in the past, new evidence suggests that thisapproachisminimallyeffectiveversusplacebo,andless effectivethan budesonide orconventional corticosteroids.7
Publishedclinicaltrialswerenotsufficienttoadequately com-paremesalazineversussulfasalazine.Ameta-analysisofthree majorstudieswithmesalazine(4g/day)showedasignificant, butnotclinicallyrelevant,statisticaldifferencecomparedto placebo.7 Therefore, in the present study,it was seen that
manypatientssufferfromCDandusemesalazine,atherapy withnoconsistentefficacy.
For CD patients, the therapy is chosen according to thelocation ofthe disease,its severity,and extraintestinal complications.1,5,7,9
Immunosuppressantsandbiologicalagentsarethemost relevant pharmacological classes for this purpose.12 The
tumornecrosisfactoralphaisacriticalcytokinefortheorigin, amplification,andmaintenanceoftheinflammatory dysfunc-tionobservedinCDpatients.13
Duetothegeneticheterogeneityofthedisease,CDpatients are expectedtohave agreater need fordrugreplacement, doseadjustment,orevensurgicalindication.11,12Oursample
issimilartothosefoundintheliterature.However,agreater useofaminosalicylateshasbeenobservedinpatientswith CD,differentfromwhatisrecommendedasabettertherapy toinduceremissionofthisdisease,whichcouldsupportthe highnumberofdrugreplacementsinCDpatients.
Unfortunately, thereis no cure for CD, and the patient depends on therapeutic approaches forthe induction and maintenance of its symptomatic control, improvement of thequalityoflifeandminimizinglong-termcomplications.7
Eveninthefaceofthesefacts,atechnicalreviewevaluated thesafetyandefficacyofimmunomodulatoryandbiological agentsasinductivetherapiesforremissionandmaintenance inpatientswithCD.14
Thetherapywithbiologicalsallowsmucosalhealingand isoneofthetreatmentsmostoftenusedinthecurrent ther-apeuticmanagementofCD.12,15Infliximab(IFX)isachimeric
monoclonalantibodyinwhich25%ofitsstructureconsistsof murineproteinand75%ofhumanprotein,withintravenous administration.Adalimumab(ADA)isa100%human mono-clonalantibody,administeredsubcutaneously.16
Despitetheinitialbenefitachievedwiththeshort-termuse ofanti-TNF,theliteratureshowsthatupto30%ofpatientsfail torespondthroughoutthetreatment,andinthelongterm,up to40%donotshowsustainedbenefits.12Inthesesituations,
strategiesforrescuetherapieswereandarestillbeingstudied fortheremissionofthedisease,eitherwithanincreaseofthe doseorreducingtheintervalofuseofthemedication.Inthe literature,thereare reportsthatshow greaterefficacy with thecontinuoususeofanti-TNFtreatment,inrelationtoits episodicuse.18
Inthestudiedgroup,148patients(34.9%)werebeing med-icated with this pharmacological class and, of this total, 128(86%)sufferedfromCD.Whenanalyzingthenumberof patientsstudiedinthispaper,thenumberofpatientsusing biologicalagentsisstillsmall,giventhehighcostofthis med-ication,itssideeffects,andcontraindicationstoitsuse.
Conclusion
MostpeopleontreatmentforIBDarewomen,withameanage of46years,andareCDpatients.Themostaffectedsegments weretheentirelargeintestineinURCpatientsandthecolon inCDpatients.Mesalazinewasthemostuseddruginboth diseases.ThereweremoredrugreplacementsinCDpatients. InfliximabwasmostcommonlyusedbyCDpatients;inthis group,youngerpeopleusedinfliximabmoreoften.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.WorldGastroenterologyOrganisationPracticeGuidelines. Doenc¸aInflamatóriaIntestinal:umaperspectivaglobal– 2009.Availablefrom:http://www.worldgastroenterology. org/UserFiles/file/guidelines/inflammatory-bowel-disease-portuguese-2009.pdf
2.OliveiraFM,EmerickAPC,SoaresEG.Aspectos
epidemiológicosdasdoenc¸asintestinaisinflamatóriasna
macrorregiãodesaúdelestedoestadodeminasgerais.Ciênc
SaúdeColetiv.2010;15:1031–7.
3.MaranhãoDDA,VieiraA,CamposT.Característicase
diagnósticodiferencialdasdoenc¸asinflamatóriasintestinais.
JBrasMed.2015;103:9–15.
4.SouzaMM,BelascoAGS,Aguilar-NascimentoJE.The
epidemiologicalprofileofpatientswithinflammatorybowel
diseaseintheStateofMatoGrosso.RevBrasColoproct.
2008;28:324–8.
5.Projetodiretrizes.In:Doenc¸adeCrohnintestinal:manejo;
2008.
6.CabralMG,AbbyF.Diganósticodasdoenc¸asinflamatórias
intestinais.RevHospUnivPedroErnesto.2012;11:17–21.
7.ConsensusguidelinesforthemanagementofCrohn’sdisease inadults.AmJGastroenterolAdvOnline.2009,
http://dx.doi.org/10.1038/ajg.2008.168.
8.BrazilianStudyGroupofInflammatoryBowelDiseases.
Consensusguidelinesforthemanagementofinflammatory
9. Kleinubing-JúniorH,PinhoMSL,FerreiraLC,BachtoldGA,
MerkiA.Perfildospacientesambulatoriaiscomdoenc¸as
inflamatóriasintestinais.ABCD:ArqBrasCirDig.
2011;24:200–3.
10.Projetodiretrizes.In:Doenc¸asinflamatóriasintestinais:
acompanhamentoendoscópico;2008.
11.StrongS,SteeleSR,BoutrousM,BordineauL,ChunJ,Stewart
DB,etal.ClinicalPracticeGuidelinesCommitteeofthe
AmericanSocietyofColonandRectalSurgeons.Clinical
PracticeGuidelinesfortheSurgicalManagementofCrohn’s
Disease.DisColonRectum.2015;58:1021–36.
12.Habr-GamaA,CerskiCTS,MoreiraJPT,CasertaNMG,Oliveira
JúniorO,AraújoSEA.Doenc¸adeCrohnintestinal:manejo.
RevAssocMedBras.2011;57:10–3.
13.VandenBrandeJMH,BraatH,VandenBrinkGR,VersteegHH,
BauerCA,HoedemaekerI,etal.Infliximabbutnot
Etanereceptinducesapoptosisinlaminapropria
TlymphocytesfrompatientswithCrohn’sdisease.
Gastroenterology.2003;124:1774–85.
14.TerdimanJP,GrussCB,HeidelbaughJJ,SultanS,Falck-Ytter
YT,AGAInstituteClinicalPracticeandQualityManagement
Committee.AmericanGastroenterologicalAssociation
Instituteguidelineontheuseofthiopurines,methotrexate,
andanti-TNF-␣biologicdrugsfortheinductionand
maintenanceofremissionininflammatoryCrohn’sdisease.
Gastroenterology.2013;145:1459–63.
15.KotzePG,AlbuquerqueIC,KotzeLMS,FormigaGJS.Reinduc¸ão
daremissãoclínicacomadalimumabeapósinterrupc¸ãodo
tratamento:umaalternativanomanejodadoenc¸adeCrohn.
RevBrasColoproctol.2010;30:135–40.
16.TarganSR,HanauerSB,VanDeventerSJH,MayerL,Present
DH,BraakmanT,etal.Ashort-termstudyofchimeric
monoclonalantibodycA2totumornecrosis-factoráfor
Crohn’sdisease.NEnglJMed.1997;337:1029–35.
18.RutgeertsP,VanAsscheG,VermeireS.Reviewarticle:
infliximabtherapyforinflammatoryboweldisease–seven