www.jped.com.br
ORIGINAL
ARTICLE
Evaluation
of
human
milk
titratable
acidity
before
and
after
addition
of
a
nutritional
supplement
for
preterm
newborns
夽
,
夽夽
Cibelle
Iáskara
do
Vale
Pereira
a,∗,
Juliana
Fernandes
dos
Santos
Dametto
b,c,
Janaína
Cavalcanti
Costa
Oliveira
aaUniversidadeFederaldoRioGrandedoNorte(UFRN),MaternidadeEscolaJanuárioCicco(MEJC),Natal,RN,Brazil bUniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil
cUniversidadeFederaldoRioGrandedoNorte(UFRN),DepartamentodeNutric¸ão,Natal,RN,Brazil
Received20August2015;accepted14December2015 Availableonline21June2016
KEYWORDS Newborn; Humanmilk; Titratableacidity; Dietarysupplements; Metabolicbone diseases
Abstract
Objective: ToevaluatetheinitialDornicacidityinrawhumanmilk,afterpasteurizationand afterheatinganddilutionofadietarysupplementforpreterminfants.
Methods: Aquantitative, descriptive,andexperimentalstudywascarried outwitha conve-niencesampleatthehumanmilkbankataBrazilianpublicmaternity,withspecializedcare forpregnantwomenandnewbornsatrisk.Theeligibilitycriteriaforthestudysampleincluded 93frozenrawhumanmilkinsuitablecontainerswithvolumes≥100mLandinitialDornic acid-ity≤8◦ Dornic(◦D).Milkacidityofhuman milkwasmeasuredinfour stages:inrawhuman milk (initial);afterpasteurization;after theheatingofpasteurizedmilkanddilutionofthe supplement;andafterthirtyminutesofsupplementation.
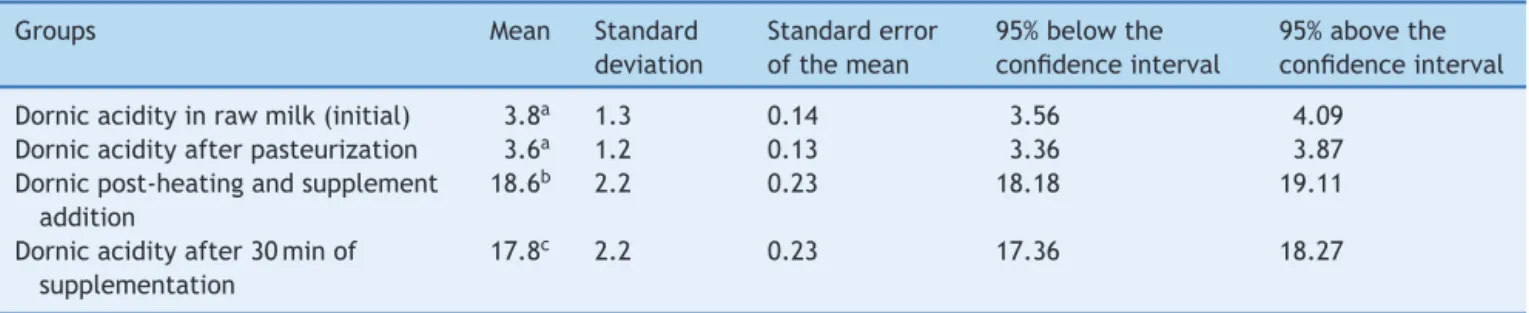
Results: Theinitialaciditywas3.8◦D±1.3(95%CI:3.56---4.09)withnosignificantdifference inDornicacidityinpasteurizedmilk,whichwas3.6◦D
±1.2(95%CI:3.36---3.87).Thedilution ofthe supplementin pasteurizedmilk thatwas heatedsignificantlyincreasedmean Dornic acidity to18.6◦D±2.2(95% CI:18.18---19.11),which remainedhigh after thirtyminutes of supplementationat17.8◦D±2.2(95%CI:17.36---18.27),consideringp<0.05.
Conclusions: ThestudyobservednosignificantdifferencesinDornicacidityofrawhumanmilk andpasteurizedhumanmilk;however,thedilutionofahumanmilksupplementationcauseda significantincreaseinacidity.Furtherinvestigationsarenecessaryontheinfluenceofthis find-ingonthequalityofsupplementedmilkanditsconsequencesonthehealthofpreterminfants. ©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradePediatria.Thisis anopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/
by-nc-nd/4.0/).
夽 Pleasecitethisarticleas:PereiraCI,DamettoJF,OliveiraJC.Evaluationofhumanmilktitratableaciditybeforeandafteradditionof
anutritionalsupplementforpretermnewborns.JPediatr(RioJ).2016;92:499---504.
夽夽
StudyconductedatUniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil.
∗Correspondingauthor.
E-mail:[email protected](C.I.Pereira). http://dx.doi.org/10.1016/j.jped.2015.12.008
PALAVRAS-CHAVE Recém-nascido; Leitehumano; Acideztitulável; Suplementos nutricionais; Doenc¸asósseas metabólicas
Avaliac¸ãodaacideztituláveldoleitehumanoanteseapósadic¸ãodeumsuplemento nutricionalpararecém-nascidopré-termo
Resumo
Objetivo: AvaliaraacidezDornicinicialnoleitehumanocru,apóspasteurizac¸ãoeapós aque-cimentoediluic¸ãodeumsuplementonutricionalpararecém-nascidosprematuros.
Métodos: Estudo quantitativo, descritivo, experimental comamostragem porconveniência, realizado noBanco deLeiteHumano de umamaternidade pública brasileira, com assistên-ciaespecializadaàsgestanteserecém-nascidosderisco.Oscritériosdeelegibilidadedas93 amostrasdoestudoincluíramleiteshumanoscruscongeladosemembalagensapropriadas,com volumes≥100mLeacidezDornicinicial≤8◦Dornic(◦D).AacidezDornicdosleiteshumanosfoi mensuradaemquatromomentos:noleitehumanocru(inicial);apóspasteurizac¸ão;após aque-cimentodoleitepasteurizadoediluic¸ãodosuplemento;eapóstranscorridostrintaminutosde suplementac¸ão.
Resultados: Aacidezinicialfoide3,8◦D±1,3(IC3,56---4,09)nãoapresentandodiferenc¸a signi-ficativaemrelac¸ãoàacidezDornicnoleitepasteurizado,quefoi3,6◦D±1,2(IC3,36---3,87).A diluic¸ãodosuplementonoleitepasteurizadoeaquecidoaumentousignificativamenteamédia daacidezDornica18,6◦D±2,2(IC18,18---19,11),aqualsemanteveelevadaem17,8◦D±2,2 (IC17,36---18,27)após30minutosdadiluic¸ão,considerandop<0,05.
Conclusões: OestudodemonstrouqueaacidezDornicdoleitehumanocruedoleitehumano pasteurizadonãoapresentaramdiferenc¸assignificativasentresi,porém,adiluic¸ãodo suple-mentodeleitehumanopromoveu elevac¸ãosignificativadaacidez.Maiores investigac¸õesda influênciadesseachadosobreaqualidadedoleitesuplementadoesuasconsequênciasnasaúde deprematurossãonecessárias.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileiradePediatria.Este ´
eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/
by-nc-nd/4.0/).
Introduction
Thetechnologicaladvancesofthe20thcenturyinthearea ofNeonatologyallowedforthecreationofNeonatal Inten-siveCareUnitsandfavoredthesurvivalofpretermandvery lowbirthweight(VLBW)newborns.1Thisrealityhasimposed several challenges on the care of this population, which requiresgreater attention in relationto growth, develop-ment,andnutrition.2
Regardingthedietaryaspects,theWorldHealth Organi-zationrecommendstheuse ofthemother’sownmilkalso for preterm infants, asin additionto being better toler-atedduetoitseasydigestibility,italsohashighnutritional quality and benefits the mother---child binomial through breastfeeding.3 Italsoaidstheimmuneprotectionagainst infections,sepsis,andnecrotizingenterocolitis,favorsthe preterminfant’smentaldevelopment,4andappearsto mod-ulate risk factors for cardiovascular diseases in the long term,4constitutingapowerfuloptionamongthestrategies toreducechildmortality.5
As for the nutritional composition, the human milk (HM) of a preterm infant’s mother initially has a higher concentrationofprotein,lipids,minerals(suchassodium, calciumandphosphorus), electrolytes,andimmunological properties, when compared to the milk of a full-term newborn’smother;butattheendofthefirstmonth,these differencesdecrease,makingthemilkofapreterminfant’s mother resemble that of a full-term infant’s.6,7 With a decreaseinthenutritionalreservesofpreterm infants,in contrast with their high metabolic demands, inadequate
nutritional support can lead to adverse and permanent effectsontheirgrowthanddevelopment.3
Therefore, HM supplementation has been indicated to meet thenutritionalrequirements of thispopulation, and to prevent or treat metabolic bone diseases in these individuals,3,8 a well-established nutritional practice in neonatology.9 Among the HM supplements used in Brazil, thosebasedonbovinewheyproteinhydrolysates,combined with several vitamins and minerals (especially calcium, phosphorus,andpotassium),aremostcommonlyused.10
Inspiteofrecommendationsforsupplementationofthe preterm mother’sownmilk, ifthe nursing mothercannot meet thebaby’s requirements, theadministrationof milk fromaHMbank(HMB)isproposed.5,11Inthiscase,it under-goesstrictqualitycontrolbeforedistribution,amongwhich isthemeasurementofDornicacidity(DA).Variationswithin therangeof1.0---8.0Dornicdegrees(◦
D)classifythefoodfor consumption, whereashighervaluesdisqualify itfromthe microbiologicalpointofviewandmayalsoinfluencethe bio-logicalavailabilityofnutrients,suchascalcium,12,13 which isessentialforbonemineralizationinpreterminfants.14,15
notyetfullyunderstood,9justifyingtheperformanceofthis study.
Inlightofthisproblem,thepresentstudyaimedto eval-uatetheinitialDAinrawHMafterpasteurizationandafter heatinganddilutionofthesupplementusedtocomplement very-low birth weight preterm infants’ nutrition and/or those undergoing treatment for metabolic bone diseases, toverifywhethertherearefluctuationsinthebehaviorof theDAvariable,consideringthesefoodhandlingsteps.
Methods
This was a quantitative, descriptive, experimental study witha conveniencesampling, conducted inthe state ref-erenceHMBofMaternidadeEscolaJanuárioCiccoinNatal, state ofRio GrandedoNorte,Brazil,which is partof the Brazilian Unified Health System and provides specialized care to at-riskpregnant women, mothers,and newborns. The HMcollected andpasteurizedonsiteareintended to benefit preterm newborns in the Neonatal Intensive Care Unitofthehospitalandrooming-inwards.
The study was approved by the Research Ethics Com-mittee of the school maternity and Hospital Universitário OnofreLopes,ofthehospitalcomplexofUniversidade Fed-eraldoRioGrandedoNorte.
Sample collection was preceded by signing an institu-tionalauthorizationformandtookplaceover24days,during theafternoonshift,betweenthemonthsofAugustand Octo-ber2014.
Toestimatethenumberofsamples,thesamplesizewas simulated in relation to the assessed effect size, based on two fixed parameters: alpha=0.05 (5% of statistical probability to reject the null hypothesis) and statistical power=0.8(testpowertodetectagenuine,actualeffect, ifitexists).Also,withoutpredictingadirection,the differ-encebetweenthemeanswasinvestigatedfromatwo-tailed analysis.Itwasobservedthatforanexpectedeffectof0.5 (meaneffectaccordingtoCohen),itwouldbenecessaryto collectaminimumsamplesizeof34elements.
Studyeligibilitycriteriaincluded104samplesofrawHM fromnursingmothersthathadexpressedtheirmilkathome, in the HM collectionroom at the school maternity, or at theHMB; werereceived for pasteurizationfrozen in glass containerswithplasticlids, withvolumes >100mL andan initialDA<8◦D.Theexclusioncriteriaweretheoccurrence
ofrepetitionsamples(fromthesamedonor)andfailureto followthestepsestablishedbythestudymethodologywith a givensample. There were11 sample losses,totaling 93 assessedsamples.
N/9sodiumhydroxide (N/9NaOH---Dornic solution)was usedasthetitrantsolutiontodeterminetheDAoftheHM. Each 0.01mLusedtoneutralize 1mL ofHM corresponded to1◦D (oneDornicdegree). Forthedetection ofthe
tur-ningpoint, onedropof phenolphthaleinindicatorsolution inhydroalcoholicsolutionat 1%wasadded,whichinitially appeared as a clear solution and, after the pH turned, becamelightpink incolor,indicating thepHchange. Sub-sequently,thespenttitrantvolumewasreadusinganacid meter.12,13
ThenutritionalsupplementaddedtoHMwasa commer-cialnutrientpowderformulaforat-risknewborns,basedon
bovinewhey protein hydrolysate, maltodextrin, vitamins, and minerals; a single type was used for all evaluations carried out in study. According to the protocol of nutri-tion and dietetics of the maternity service, the HM was heatedto37◦
Cbeforethemulticomponentsupplement dilu-tion.Themanufacturer’s recommendations werefollowed regardingproductdilution(1g/20mLHM),althoughatthe proportionalamount of 0.05g for 1mL of HM usedin the measurements.
In the case of very-low birth weight preterm infants, whosesuckingandswallowingreflexesaredelayeddue to theneurologicalsystemimmaturity,itbecomesimpossible tocarryoutthecontinuousandpromptdietadministration andthesupplementedmilkisnotfullyconsumedat once. Shortintervalsduringthedietadministrationarerequiredto preventrefluxand/orbronchoaspiration,bothinthecaseof offeringthefoodusingadosingcupdirectlytothemouthof preterminfant,andthroughenteralfeedingforthosewho cannotbefedorally.
Considering the consequences of the interval between preparationand the completionof the administration, as wellasthestagesofitsprevioushandling,theDAoftheHM includedinthestudywasmeasuredatfourdifferenttimesin ordertocharacterizeitspossiblefluctuations:intherawHM (initialacidity);afterpasteurization;afterthepasteurized HMwasheatedandnutritionalsupplementwasdiluted;and 30(thirty)minutesafterHMsupplementation.
Thefirstmoment(DAmeasuredinrawHM)wasbasedon datacollectionof samplesbyconsultingthe HMBrecords, astheactivityisdevelopedandrecordeddailybylocal pro-fessionals.Theresearcherswereresponsibleforcarryingout themeasurementsatthesecond,third,andfourthmoments ofthestudy.
The data collected fromthe samples werestored in a specific formand subsequently stored in Microsoft Excel®
spreadsheets (Microsoft Excel®, V 2010. Microsoft®, WA,
USA).TheDAofsamplesattherespectivemomentsofthe studywasmeasuredintriplicate,usingthearithmeticmean ofthevaluesobtainedfromtheindividualanalysisofeach aliquot. The mean DA obtained at the appropriate study momentswereusedforthestatisticaltests.
Theone-wayANOVAstatisticaltestwasappliedto deter-minethevariabilitybetweenthemeansofeachstageofthe study;Tukey’spost-testwasthenusedformultiple compar-isons.Thelevelofsignificancewassetat5%.
Results
Atfirst,thestatisticaltestshowedthatatleastoneofthe groupshadastatisticallysignificantdifferencecomparedto theothers(p<0.0001).
The post-test indicated no significant difference (p>0.05) betweenDAinraw HMandafterpasteurization. However, the mean DA in raw HM showed a statistically significant difference (p<0.05) in DA means after the pasteurizedHMwasheatedandthenutritionalsupplement wasaddedwhen comparedwiththe DA registered30min aftersupplementation.
Table1 Mean,standarddeviation,standarderrorofthemean,andvariationaboveandbelowthe95%confidenceintervalsof Dornicacidityofhumanmilkateachstageofthestudy.
Groups Mean Standard
deviation
Standarderror ofthemean
95%belowthe confidenceinterval
95%abovethe confidenceinterval
Dornicacidityinrawmilk(initial) 3.8a 1.3 0.14 3.56 4.09
Dornicacidityafterpasteurization 3.6a 1.2 0.13 3.36 3.87
Dornicpost-heatingandsupplement addition
18.6b 2.2 0.23 18.18 19.11
Dornicacidityafter30minof supplementation
17.8c 2.2 0.23 17.36 18.27
a,b,cDifferentlettersrepresentstatisticallysignificantdifference(p<0.05).
heatingandsupplementadditionandDA30minafter supple-mentation,asshowninTable1.
Discussion
Milkisa buffersolution,withalow concentrationoffree hydrogenions(H+).Becauseofthebufferresultingfromits intrinsiccomposition,smallchangesdetectedinpHvalues areprecededbyconsiderableincreasesinDA.12,18
About the association between these two chemical parameters,ingeneralitisconsideredthatDAismore sensi-tivetothetotalcontentofsolutesinHMandthatthelower the pH, the higher the DA of the food. As the pH varies dependingontheenergycontentofHM,itissuggestedthat DAisalsodirectlyinfluencedbythelipidcontentofthefood. Milkwithhigherfatconcentrationshasincreasedchancesof developinghighacidity.18
ThepasteurizationofHMwithhighaciditydoesnotaim toimprovequality.18 Therefore,it isimportanttoknowif therewasbacterialgrowthpriortothisprocessing,asthat producesfermentationandacidificationofthemilk,which inturnleadtoareductioninnutritionalandimmunological componentsinherenttothefood,disqualifyingitsuse.12,13,19 AcidifiedHMcannotmeetthespecificnutritionalneeds of very-low birth weight or immunologically-vulnerable preterminfants. The high acidityand the releaseof pro-tons originating from the ionization of lactic acid in an aqueous medium causedestabilization of solubleproteins andcaseinmicelles,favoringitscoagulation;increasethe osmolarity;alter theflavor (taste and smell);and reduce theimmunologicalvalueofthefood.Thiscationicattack, by destabilizing the casein in suspension in HM, impairs the availability of the calcium and phosphorus content, which are chemically associated to casein, creating sta-blemicelles,thusmakingtheabsorptionoftheseminerals dependentontheproteindigestionprocess.19---21
Inthisstudy,theDAfoundinrawHM(3.8◦D±1.3)showed
nostatisticaldifferencewhencomparedwiththat in pas-teurized HM (3.6◦D±1.2), suggesting that the analyzed
milkswereadequateforconsumptionbynewborns,withno furtherinterference of theinitial DA valueson the nutri-tionalcontentofthefood.
After the addition of the nutritional supplement to HM pasteurized and heated to 37◦C, there was a
signifi-cantincreaseinthemeanDA(18.6◦D±2.2,p<0.05).This
increase was maintained even after 30min post-dilution
(17.8◦D±2.2,p<0.05).Bothmeans werehigherthan the
8◦
DlimitrecommendedforHMconsumptionbynewborns. Consideringthe importance of HM acidity onits nutri-tionalquality,itshouldbeemphasizedthatacidoralkaline overloadsresultinmetabolicacidosisoralkalosis,anditsuse cancausenecrotizingenterocolitisinvery-lowbirthweight preterminfants.18
It is important to emphasize that the HM (either raw orpasteurized andfrozen)canundergolipolysis,releasing greateramountsoffreefattyacids,whichcontributetothe increaseinacidity,asinterpretedbyNovakandCordeiro.22 Consequently,higherconcentrationsofthesecomponentsin themilk,combinedwiththehighsupplyofmineralssuchas calciumthroughtheadditionofsupplements,wouldresult intheformationofinsolublesoaps,anotherfactorcontrary to theabsorption of the mineral by the body.6 Also,it is reasonable tosuggest that, despite beingthesame event (increaseinDA),whenpromotedbydifferentreasons(such astheoccurrenceoflipolysis,theincreaseofacidifying com-ponentsduetoHMsupplementation,orthedevelopmentof aciditythroughtheformationoflacticacidastheresultof bacterialactivity),itisnotpossibletoaffirmthatthe con-sequences arethe same,especially astointerferingwith calcium bioavailability andmetabolism of preterm recep-tors.Therefore,furtherstudiesonthesubjectarerequired toclarifytheseissues.
Furthermore, the use of multicomponent HM supple-mentsmayincreasetheriskofinfectionbycontamination secondary tothe manipulation of thesupplement powder andcausechangesinfoodosmolarity,affectingthe absorp-tion of itsnutrients.23 In this respect,a limitation of the present studyis relatedtotheabsenceof microbiological teststoruleoutthepossibilityofcontaminationbythe sup-plement,aswellasthepreviouslack ofknowledgeonthe productacidity, conditionsthat couldinfluence the inter-pretationoftheresultsfoundhere.
However, the HM supplementation offered to preterm infants becomes important considering the findings that breast milk from their nursing mothers, even with a dif-ferent composition in relation to the milk of mothers of full-term newborns,stillhasinsufficient protein,calcium, andphosphoruscontents.23,26
In a systematic review carried out by the Cochrane DatabaseofSystematicReviews,itwasconcludedthatthe multicomponentsupplementationofHMforpreterminfants wasassociatedwithaquickerincreaseinweight,length,and headcircumference,althoughnoeffectswereobservedon bonemineralizationintheassessedgroup.27
Inastudycarriedoutin2010intheintensivecareunitof ahospitalinPortoAlegre,stateofRioGrandedoSul,Brazil, the authors comparedtwo groups of 19 preterm infants: onegroupreceivedonlyHMandtheotherreceivedtheHM supplemented withFM85®, milkfortifier (FM85®, Nestlé,
München,Germany).Bothgroupswerefollowed regarding theindividualanthropometricmeasurements,whereasbone mineralization wasassessed by whole-bodybone densito-metry with dual energy X-ray absorptiometry (DEXA) and laboratory tests ofalkaline phosphatasecontrol, calcium, phosphorus,aswellasurinarycalciumandphosphorus.The results showeda clear improvement in the supplemented groupwhencomparedwiththenon-supplementedgroup;a decreaseinalkalinephosphatasewasalsoobservedin the lattergroup,demonstratingbettermineralhomeostasisin thissituation.28
ManystudiesonHMsupplementationforpreterminfants withbone mineralization deficitshave been developed to demonstrate the consequences of this conduct for this specific population.6,8,9,19 However, the results are still conflicting,sometimesshowingbenefitsformineralization, sometimesshowingnosignificantresponseswhencompared to HM without supplementation and/or specific formu-las for preterm infants. However, it must be considered thatthemethodologiesusedtoassesstheseoutcomesare quite diverse --- ranging from the ‘‘classic’’ investigation basedonanthropometricdata,X-rays,andserum biochem-icalanalysisofcalcium,phosphorus,alkalinephosphatase, parathyroidhormone,vitaminDmetabolites, calcium,and phosphorusin urine; or more recently,by DEXA --- making itdifficulttocomparethefindings.Moreover,thedifferent types ofsupplementation usedinHM andthe sample size (usuallysmall)areobstaclestoattainconsistentconclusions frompreviouslyperformedstudies.28
Thus, the present study is relevant, as it proposed the observation of acid---basic characteristics of supple-mented HM in vitro, reducing the influences caused by metabolicactivityin vivo,which canbecomeconfounding factorswhen interpretingresults aboutthe physicochemi-calfoodmodificationsaftersupplementation.Nonetheless, themethodologyusedheredidnotallowforadirect assess-mentoftheconsequencesofincreasedDAinsupplemented HMoncalciumandphosphorusbioavailability,orthe under-standingoftheir effectsonthehealth andmetabolismof very-lowbirthweightpreterminfantsand/orthose under-goingtreatmentformetabolicbonediseases.
Therefore,consideringtheresultsobtainedinthisstudy, whichshowednosignificantdifferencebetweentheinitial DA of raw and pasteurized HM, aswell asthe significant acidificationofsupplementedHM(usedforpreterminfants
withvery-lowbirthweightand/orincasesofmetabolicbone diseases),andgiventhespeculationthatthisacidification observedinthesupplementedHMmayhindertheabsorption ofnutrients suchas calcium,it must beemphasized that thereisnotenoughevidencefromthescientificliterature tosustainsuchassertion.Therefore,furtherstudies, includ-ingmethodologiesthatwillallowassessingtheoccurrence ofmetabolicbonediseaseinvery-lowbirthweightpreterm infantsreceivingsupplementedandnon-supplementedHM, withandwithoutDAincreaseintheconsumedmilk,are rec-ommendedin ordertodemonstrate theeffectivenessand safetyofsupplementation,whicharenotyetfullyclarified. Consequently, such studies are also essential to indi-cate the optimal composition of HM supplements used tofeed these preterm infants. Considering that the con-sequences of HM supplementation remain questionable, indications/prescriptionsalwaysrequirecriticalaccuracy.
Furthermore, considering the results discussed in the presentstudy,itisworthemphasizingthecontrastbetween theinitialdisposalofHMsamplescarriedoutinHMBdueto thepresenceofDA>8◦D,whichisinterpretedasanincrease
intheproductionoflacticacidduetobiological contami-nationoffood,andtheelevation ofthisparameterin HM causedbyadditionofthenutritionalsupplement, suggest-ing that samples with high DA discarded by HMBs would notalways be justifiedby high contamination, andcould therefore be caused by changes in the chemical compo-sitionof the fooditself,as proposedby a previous study. Therefore,furtherdiscussionisnecessarytopropose solu-tionstominimizethedisposalofHM supposedlyadequate forconsumption.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Sá Neto JA, Rodrigues BM. Tecnologia comofundamento do cuidaremNeonatologia.TextoContextoEnferm,Florianópolis. 2010;19:372---7.
2.BragaLP,PalharesDB.Effectofevaporationandpasteurization inthebiochemical andimmunologicalcompositionofhuman milk.JPediatr(RioJ).2007;83:59---63.
3.Brasil, Ministério da Saúde, Secretaria de Atenc¸ão à Saúde, DepartamentodeAc¸õesProgramáticaseEstratégicas.Atenc¸ão àsaúdedorecém-nascido:guiaparaosprofissionaisdesaúde: cuidadoscom o recém-nascido pré-termo,v.4. Brasília: Min-istériodaSaúde;2011(SérieA:NormaseManuaisTécnicos).
4.Arslanoglu S, Ziegler EE, Moro GE. WAPM Working Group on Nutrition. Recommendations and guidelines for perinatal practice.Donorhumanmilkinpreterminfantfeeding:evidence andrecommendations.JPerinatMed.2010;38:347---51.
5.WorldHealthOrganization.Essentialnutritionactions: improv-ing maternal, newborn, infant and young child health and nutrition.Geneva:WorldHealthOrganization;2013.p.144.
6.MatalounMM,LeoneCR,OnoN,VazFA.Repercussõesneonatais dousodeleitematernocomaditivosefórmulaparapré-termo emrecém-nascidosdemuitobaixopesoaonascer.Pediatr(São Paulo).2004;26:247---56.
8.MartinsEC,KrebsVL.Effectsoftheuseoffortifiedraw mater-nal milkon verylowbirth weightinfants. JPediatr (Rio J). 2009;85:157---62.
9.Tanaka A, Rugolo LM, Miranda AF, Trindade CE. Fractional sodium excretion, urinary osmolality and specific gravity in preterminfantsfedwithfortifieddonorhumanmilk.JPediatr (RioJ).2006;82:335---40.
10.Tavares LV [Dissertation] Determinac¸ão de aminoácidos em RNPT alimentados com dietas modificadas de leite humano. Campo Grande,MS:UniversidadeFederal doMato Grossodo Sul;2011.
11.WorldHealth Organization. Guidelineson optimalfeedingof lowbirth-weightinfantsinlow-andmiddle-incomecountries. Geneva:WorldHealthOrganization;2011.
12.AlmeidaJA,GuimarãesV,NovakFR.Normastécnicas Redeblh-Brparabancosdeleitehumano:selec¸ãoeclassificac¸ão.Riode Janeiro:FIOCRUZ/IFF-BLH;2005.
13.Brasil, Agência Nacional de Vigilância Sanitária. Banco de leitehumano:funcionamento,prevenc¸ãoecontrolederiscos. Brasília:Anvisa;2008(SérieTecnologiaemServic¸osdeSaúde).
14.TrindadeCE.Importânciadosmineraisnaalimentac¸ãodo pré-termoextremo.JPediatr(RioJ).2005;81:S43---51.
15.American Academy of Pediatrics. Calcium and vitamin D requirements of enterally fed preterminfants: guidance for theclinicianinrenderingpediatriccare.Pediatrics.2013;131: e1676.Availablefrom:http://www.sbp.com.br/pdfs/CLINICAL REPORT-Calcium VitaminDRequirementsEnterallyFed Preterm Infants.pdf[accessed08.08.15].
16.CostaEC[Dissertation]Caracterizac¸ãomicrobiológicae físico-químicadeleitehumanoemdiferentesperíodosdelactac¸ão. Vic¸osa(MG):UniversidadeFederaldeVic¸osa;2012.
17.Grazziotin MC [Dissertation] Efeito dos diferentes modos e temposdeestocagemsobreaacidezeovalorcalóricodoleite humanoordenhadocrudemãescomrecémnascidosinternados numaunidadedeneonatologia.Curitiba:UniversidadeFederal doParaná;2014.
18.Cavalcante JL, Telles FJ, Peixoto MM, Rodrigues RC. Uso da acidez titulável no controle de qualidade do leite humanoordenhado.CiêncTecnolAliment(Campinas).2005;25: 103---8.
19.RonaMSS,NovakFR,PortilhoM,PelissariFM,MartinsABT, Mati-oli G. Efeito dotempo e datemperatura de estocagem nas determinac¸õesdeacidez,cálcio,proteínaselipídeosdeleite dedoadorasdebancosdeleitehumano.RevBrasSaudeMater Infant.2008;8:257---63.
20.PessotoMA[Thesis]Avaliac¸ãodalactac¸ãoemmãesde recém-nascido pretermo com peso de nascimento inferior a 1.250 gramassegundodiferentesmétodosdeordenha:manual,com bombamanualoucombombaelétrica.Campinas,SP: Universi-dadeEstadualdeCampinas;2009.
21.Aprile MM [Dissertation] Crescimento de recém-nascidos de muito baixo peso alimentados com leite de banco de leite humanoselecionadosegundoovalorcalóricoeproteico.São Paulo,SP:UniversidadedeSãoPaulo;2006.
22.Novak FR, Cordeiro DM. The correlation between aero-bic mesophilic microorganism counts and Dornic acidity in expressedhumanbreastmilk.JPediatr(RioJ).2007;83:87---91. 23.CukierFN [Dissertation]Eficácia eseguranc¸ados aditivosde leitehumanoparaprematuroscompesodenascimento≤1500g ou idade gestacional≤34 semanas: uma revisão sistemática commetanálise.RiodeJaneiro,RJ:Fundac¸ãoOswaldoCruz, InstitutoNacionaldeSaúdedaMulher,daCrianc¸aedo Adoles-centeFernandesFigueira;2014.
24.DeCurtis M,Candusso M,PieltainC,RigoJ.Effectof fortifi-cationontheosmolalityofhumanmilk.Arch DisChildFetal NeonatalEd.1999;8:F141---3.
25.AgarwalR,SingalA,AggarwalR,DeorariAK,PaulVK.Effectof fortificationwithhumanmilkfortifier(HMF)andotherfortifying agentsontheosmolalityofpretermbreastmilk.IndianPediatr. 2004;41:63---7.
26.TudehopeDI.Humanmilkandthenutritionalneedsofpreterm infants.JPediatr.2013;162:S17---25.
27.KuschelCA,HardingJE.Multicomponentfortifiedhumanmilk forpromotinggrowth inpreterminfants. CochraneDatabase SystRev.2004;1:1---6.