REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Effect
of
intraoperative
intravenous
lidocaine
on
pain
and
plasma
interleukin-6
in
patients
undergoing
hysterectomy
夽
Caio
Marcio
Barros
de
Oliveira
a,b,c,
Rioko
Kimiko
Sakata
d,∗,
Alexandre
Slullitel
e,
Reinaldo
Salomão
f,
Vera
Lucia
Lanchote
g,
Adriana
Machado
Issy
daUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil bPainService,HospitalSãoDomingos(HSD),SãoLuís,MA,Brazil
cSociedadedeAnestesiologiadoEstadodoMaranhão(SAEM),SãoLuís,MA,Brazil
dPainDivisionoftheDepartmentofAnesthesiology,PainandIntensiveCareoftheUniversidadeFederaldeSãoPaulo(UNIFESP),
SãoPaulo,SP,Brazil
eDepartmentofAnesthesiology,Associac¸ãoPaulistadeMedicina,SãoPaulo,SP,Brazil
fDepartmentofInfectiousDiseases,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
gFaculdadedeCiênciasFarmacêuticasdeRibeirãoPreto,UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
Received27April2013;accepted15July2013
Availableonline2January2015
KEYWORDS
Lidocaine; Intravenously; Postoperativepain; Hysterectomy; Interleukin-6
Abstract
Backgroundandobjectives: Interleukin-6 is a predictor of trauma severity. The purpose of
thisstudy was to evaluatethe effectofintravenous lidocaineonpain severity andplasma
interleukin-6afterhysterectomy.
Method: Aprospective,randomized,comparative,double-blindstudywith40patients,aged
18---60years.G1receivedlidocaine(2mgkg−1h−1)orG2received0.9%salinesolutionduring
theoperation.AnesthesiawasinducedwithO2/isoflurane.Painseverity(T0:awakeand6,12,
18and24h),firstanalgesicrequest,anddoseofmorphinein24hwereevaluated.Interleukin-6
wasmeasuredbeforestartingsurgery(T0),5hafterthestart(T5),and24haftertheendof
surgery(T24).
Results:Therewas nodifference inpain severitybetweengroups.Therewas adecreasein
painseveritybetweenT0andothermeasurementtimesinG1.Timetofirstsupplementation
wasgreaterinG2(76.0±104.4min)thaninG1(26.7±23.3min).Therewasnodifferencein
supplementaldoseofmorphinebetweenG1(23.5±12.6mg)andG2(18.7±11.3mg).There
wereincreasedconcentrations ofIL-6 inbothgroupsfromT0 toT5andT24.There wasno
differenceinIL-6dosagebetweengroups.Lidocaineconcentrationwas856.5±364.1ngmL−1
inT5and30.1±14.2ngmL−1inT24.
夽 StudyperformedattheUniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](R.K.Sakata).
http://dx.doi.org/10.1016/j.bjane.2013.07.017
Conclusion: Intravenouslidocaine(2mgkg−1h−1)didnotreducepainseverityandplasmalevels
ofIL-6inpatientsundergoingabdominalhysterectomy.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
PALAVRAS-CHAVE
Lidocaína; Viavenosa; Dorpós-operatória; Histerectomia; Interleucina-6
Efeitodalidocaínavenosaintraoperatóriasobredoreinterleucina-6plasmáticaem
pacientessubmetidasahisterectomia
Resumo
Justificativaeobjetivos: Ainterleucina-6(IL-6)épreditoradeintensidadenotrauma.O
obje-tivodesteestudofoiavaliaroefeitodalidocaínaporviavenosasobreaintensidadedadore
IL-6apóshisterectomia.
Método: O estudo foi prospectivo, randomizado, comparativo e duplo-encoberto em 40
pacientes, entre18e60 anos.Foi administradalidocaína (2mg.kg−1.h−1)noG1ousoluc¸ão
salina a0,9%noG2 duranteaoperac¸ão.A anestesia foicom O2/isoflurano.Foi avaliada a
intensidadedador(T0:despertareseis,12,18e24horas),aprimeirasolicitac¸ãode
anal-gésico,adosedemorfinanas24horas.AIL-6foimedidaantesdoiníciodaoperac¸ão(T0),após
cincohorasdoinício(T5)e24horasapósotérmino(T24).
Resultados: Nãohouvediferenc¸anaintensidadedadorentreosgrupos.Ocorreudiminuic¸ão
daintensidadedadorentreT0eosoutrosmomentosavaliadosnoG1.Otempoparaprimeira
complementac¸ãofoimaiornoG2(76,0±104,4min)doquenoG1(26,7±23,3min).Nãohouve
diferenc¸anadosedemorfinacomplementarentreG1(23,5±12,6mg)eG2(18,7±11,3mg).
Houveaumentodasconcentrac¸õesdeIL-6emambososgruposdeT0paraT5eT24.Nãohouve
diferenc¸anadosagemdeIL-6entreosgrupos.Aconcentrac¸ãodelidocaínafoi856,5±364,1
ng.mL−1emT5e30,1±14,2ng.mL−1emT24.
Conclusão:A lidocaína(2mg.kg−1.h−1)porviavenosanão promoveureduc¸ãodaintensidade
dadoredosníveisplasmáticosdeIL-6empacientessubmetidasahisterectomiaabdominal.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Both the dose and duration of lidocaine infusion remain controversial. Moreover, its effectiveness has not yet been determined. Surgical trauma results in the release of cytokines that are responsible for local inflammatory responsesandpromotetissuehealing.1Interleukin-6(IL-6)is
acytokinethatisearlydetectedinresponsetoinjuryandits increaseiscorrelatedwiththedegreeoftissuedamage.1,2
Some authorshave reportedthatintravenous lidocaine promotesreductionofcytokines,3,4inhaledanesthetics5and
opioidsconsumption,6,7andpostoperativepainseverity.3,6,7
Furthermore, low doses of intravenous lidocaine (plasma concentrations less than 5gmL−1) do not interfere with
normal nerveconduction andare associatedwitha lower incidenceofopioid-relatedadverseeffects.3,6,8
Lidocainehasanalgesic,6anti-hyperalgesic,6,9and
anti-inflammatory effects.4,10 Analgesia maypersist evenafter
plasmaconcentrationreduction.10,11
The voltage-gated sodiumchannels arethe classic tar-gets of lidocaine.12 The analgesic and anti-inflammatory
action also occurs through calcium and potassium chan-nelsandreceptorscoupledtoGprotein.13,14The neuronal
transmissionblockadeandreducedneurogenicresponseare
causedbytheactiononsodiumandpotassiumchannels.13,15
Lidocaine metabolite, monoethylglycinexylidide (MEGX), may also exert analgesic effect.16 Unlike MEGX,
lido-cainereducesglycineuptakeonlyattoxicconcentrations. However, other studies reported no analgesic effect of lidocaine.17,18
Thus, theprimary objective of thisstudy wasto eval-uatetheeffectof intraoperativeintravenous lidocaineon postoperativepainseverityandplasmalevelsofIL-6after abdominalhysterectomy.
Methods
AfterapprovalbytheResearchEthicsCommitteeofthe Fed-eralUniversityofSãoPauloandobtainingwritteninformed consent,40patients,ASA1or 2,agedbetween18and60 years, undergoing elective total hysterectomy by laparo-tomythroughaPfannenstielincisionwereincluded.
surgeryorreceivedbloodproductsduringthestudyperiod wereexcluded.
This was a prospective, double blind and randomized study.Patientswererandomlyallocatedintotwogroupsof equalsize by lottoreceive either lidocaineinfusion (G1) or 0.9% saline infusion (G2/control). Randomization was performed using G1 and G2 registers, which were placed in sealed envelopes prior to study initiation and opened approximately30minpriortoanesthesiabyaphysicianwho preparedtheintravenoussolutionandidentifieditwiththe patientnumber,accordingtotheenvelopedrawn.The solu-tionwashandedtoanotherphysician,blindtotheprepared solutions’content,whowasresponsiblefortheanesthesia. Thesolutionvolumewasequal.The responsible investiga-torremainedblindtothechosengroupuntiltheendofthe study.
G1 patients (n=20) received 2mgkg−1h−1 of lidocaine
andG2patients(n=20)receivedan equalvolumeof0.9% saline,whoseinfusionwasinitiatedatthetimeofinduction ofanesthesiaandcontinueduntiltheendoftheoperation. Midazolamwasadministeredatadoseof15mgorally1h beforeanesthesia.Patientsweremonitoredwithcontinuous electrocardiography and pulse oximetry and intermittent noninvasive blood pressure measurements every 5min. Induction of anesthesia was performed with fentanyl (5gkg−1)andpropofol (2mgkg−1);neuromuscular
block-adewasachievedwithatracurium(0.5mgkg−1).Anesthesia
was maintained with O2/isoflurane at sufficient dose to
maintainsystolicbloodpressurewithinthelimitof20% base-line value. Neuromuscular blockade was maintained with atracurium(0.2mgkg−1)administeredevery30min.During
surgery,additionaldosesofopioidsorotheranalgesicswere notused.Therewasnoprophylaxisforpostoperativenausea andvomiting.
Aftersurgery, patientswere monitoredin therecovery room and later taken to the ward. Morphine (5mg) was administeredsubcutaneouslyusinga 23Gscalp,as neces-sary.
Bloodsampleswerecollectedinethylenediaminetetra acetate(EDTA)tubesimmediatelyaftercontralateralupper limbvenipuncture,beforetheoperation(T0),5hafterthe startofsurgery(T5),and24haftersurgery(T24).Blood sam-pleswerecentrifugedandplasmawasseparatedandstored at−70◦Cup toanalysis.The levelsofIL-6wereanalyzed
using the enzyme-linked immunoassay (ELISA). Lidocaine anditsmetabolite MEGXwereanalyzed usinghigh perfor-manceliquidchromatography(HPLC)5hafterthestartof surgeryand24haftersurgery.
Painseveritywasassessedatrestusingaverbalnumeric scale(VNS)fromzeroto10(where0=nopainand10=most severepainpossible).Averbaldescriptivescale (VDS)was also used: 0=no pain, 1=mild pain, 2=moderate pain, and 3=severe pain. The scores were recorded at the following times: T0=immediately at awakening; T6=6h afterawakening;T12=12hafterawakening;T18=18hafter awakening;T24=24hafterawakening.
Forpostoperative analgesia, morphine (5mg) was sub-cutaneouslyadministeredby anurse,asneeded. Thefirst analgesicrequest,thesupplementaldoseofmorphine nec-essary for the first 24h, and the dose of isoflurane used intraoperatively were recorded; side effects were also recorded.
Statisticalanalysis
Sample size calculation was performed with GraphPadInstat® program (GraphPad Software Inc., San
Diego, CA, USA). For such, we considered the reduction of pain severity caused by lidocaine. Based on a pilot studyconductedbythesameresearchgroup,thestandard deviation(SD)wasestimatedat2.2.Adifferenceofatleast 3inVNS(0---10)wasconsideredclinicallyrelevant.Because painissubjectiveandindividual,threelevelsofdifference were considered a significant pattern of change or an improvementfactoror asignificantworsening.Confidence interval was 95%. Thus, a sample with a minimum of 20 patientspergroupwascalculated.Thefollowingtestswere used: Mann---Whitneytest tocompare age and body mass index (BMI); Student t-test to compare weight, height, duration of anesthesia, duration of surgery, time to first analgesicsupplementation,totalmorphineconsumption in 24h, painintensity,totalisofluraneconsumption,andIL-6 plasmalevels.Datawereexpressedasmean±SD.
Results
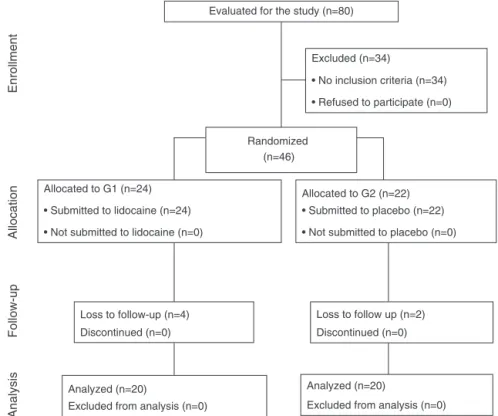
Fig.1shows the studyflowchart.19 Thegroups were
simi-larregardingdemographicdataanddurationofsurgeryand anesthesia(Table1).
Therewasnodifferencebetweenthetwogroupsinthe timepointsevaluated(Table2).Therewasnostatistically significantdifferenceinIL-6concentrationbetweengroups (Table3).
The postoperative timeto firstmorphine dose request for analgesia was higher in G2 (76±104.4) than in G1 (26.7±23.3) (Table 4). Therewas nodifference between groupsregardingsupplementarymorphinedoseandvolume of isoflurane (Table 4). Table 5 shows the concentrations oflidocaineanditsmetabolite,MEGX.Nauseaoccurredin sevenpatientsineachgroup.
Discussion
There was no analgesic effect with intravenous lidocaine infusion andalso noreductionin plasmaconcentration of IL-6.
Inthisstudy,theopenhysterectomywaschosenbecause it is associated with severe postoperative pain, with a greatchanceof changesintheneuronalprocessingofthe spinal dorsal horn, which would allow us to compare the groups.20
Previousstudieshave usedlargerdosesoflidocainefor intravenousinfusionandsomeusedinitialbolus,whichmay explainthelackofanalgesiceffectinthisstudy.3,5---7
Inonestudy,3lidocaine(2mgkg−1)wasadministeredas
a bolus and maintained with infusion of 3mgkg−1h−1. In
anotherstudy,6theanalgesicandsparingeffectofmorphine
wasmost evidentonthe thirdpostoperativeday, but this studywaslimitedto24h.
Itmust beremembered that the dose and duration of lidocainevenous infusion, withthe objectiveof obtaining postoperativeanalgesia,havenotbeenwelldefined.21
Evaluated for the study (n=80)
Excluded (n=34)
• No inclusion criteria (n=34)
• Refused to participate (n=0)
Randomized (n=46)
Allocated to G2 (n=22)
• Submitted to placebo (n=22)
• Not submitted to placebo (n=0) Allocated to G1 (n=24)
• Submitted to lidocaine (n=24)
• Not submitted to lidocaine (n=0)
Loss to follow-up (n=4)
Discontinued (n=0)
Loss to follow up (n=2)
Discontinued (n=0)
Analyzed (n=20)
Excluded from analysis (n=0)
Analyzed (n=20)
Excluded from analysis (n=0)
Enrollment
Allocation
Follow-up
Analysis
Figure1 FlowchartbasedonConsort.19
Table1 Demographicdata,operationandanesthesiatimes.
G1 G2 p
Age(years) 44.1±6.6 42.9±5.7 0.646a
Weight(kg) 72.2±13.7 74.2±12.6 0.379b
Height(cm) 159.12±6.5 158.0±6.6 0.343b
BMI(kgm−2) 28.5±5.4 29.7±5.3 0.133a
Operationtime(min) 102.6±49.4 93.0±48.2 0.122b
Anesthesiatime(min) 145.1±51.8 124.0±43.8 0.172b
G1,lidocaine;G2,salinesolution;BMI,bodymassindex.
aMann---Whitneytest. bStudent’st-test.
Table2 Painintensitybynumericalratingscale.
Times(h) G1(n=20) G2(n=20) p
Scores IC95% Scores CI95%
T0 3.2±3.9 1.3---5 2.5±3.7 0.7---4.2 0.602
T6 1.4±1.8 0.5---2.3 1.8±1.6 1---2.5 0.307
T12 0.8±1.5 0---1.4 1.3±1.8 0.4---2.1 0.307
T18 0.9±1.5 0.1---1.5 1±1 0.5---1.5 0.476
T24 1±1.6 0.3---1.8 1.3±1.6 0.5---2 0.602
G1,lidocaine;G2,salinesolution;CI 95%,95%confidenceinterval;T0,awakening;T6,T12,T18 andT24,6,12,18and 24hafter awakening.
Because themeasurementof plasma lidocainewasnot partof thepurposeofthisstudy andserved onlyas addi-tionalinformation,itsanalysiswasmadeatthesamedosage timesof IL-6: beforebeginningsurgery(T0),5hafter the
Table3 PlasmaconcentrationofIL-6(pcgmL−1).
Times(h) G1(n=20) G2(n=20) p
T0 0.95±4.25 2.56±7.55 0.602
T5 20.34±17.83 19.44±17.88 0.841
T24 24.95±14.82 34.73±15.62 0.056
G1,lidocaine;G2,salinesolution;T0,beforesurgicalincision;T5,5haftertheincision;T24,24hafterskinsuture.
Table4 Volume ofisoflurane used, time to first analgesic request, and additional analgesic dose of morphine over24h
(mean±SD).
G1(n=20) G2(n=20) p
Timetofirstsupplementation(min) 26.7±23.3 76.0±104.4 0.046
Additionaldoseofmorphinein24h(mg) 23.5±12.6 18.7±11.3 0.217
Volumeofisofluraneused(mL) 25.2±8.9 26.5±10.6 0.679
G1,lidocaine;G2,salinesolution;Student’st-test.
tomeasurethepeakconcentrationoflidocaine.AtT5and T24,themeasurementof lidocaineaveraged0.86gmL−1 and0.55gmL−1,respectively.Theseresultsarewellbelow concentrations considered effective, which range from 2 to 10gmL−1.22 In this study, intravenous lidocaine did
not reduce postoperative pain severity, similar to some studies,16---18probablybecauseoftheshortinfusiontimeand
absenceofinitialbolusdose.
Although it has been reported that there would be a higher analgesic effect that would increase the infusion time,insteadoflidocainedose,thestudyofKoppertetal.,6
using low dose infusion of lidocaine for up to 1h after surgery, showedpositive prolonged results for upto 72h. Inourstudy,lidocaineinfusionwasdiscontinuedattheend ofsurgery,asinother studies.3,5,8,23-26 Lidocainedose was
based on the study by Lauwick et al.5 Indeed, lidocaine
boluswasnot usedbeforeinfusionbecause insome stud-iestherewasa reductionin postoperative painwithonly theinfusion.23,27
In thisstudy, patients whoreceivedlidocaine required theirfirstanalgesicsupplementation earlierthanthe con-trolgroup.Onepossibleexplanationforthisresultmaybea greatindividualvariabilityinpainthresholdsandpatients’ responsetoanalgesics.Becausetherewasconsiderable dis-crepancyinthefirstanalgesicrequesttimeamongpatients inG2, the groupstandard deviation wasgreater thanthe mean.
Interleukin-6(IL-6)isan earlymarkeroftissuedamage anditsexcessiveandprolongedincreaseisrelatedtogreater postoperativemorbidity.2 Inour study,IL-6wasmeasured
beforethestartofsurgery(T0),5hfromthestartofsurgery
Table 5 Plasma levels of lidocaine and
monoethyl-glycinexylidide(MEGX)(ngmL−1)inG1.
Times(h) Lidocaine MEGX
T5 856.5±364.1 545.6±212.9
T24 30.1±14.2 ND
G1,lidocaine;T5,5haftertheincision;T24, 24hafterskin suture;ND,notdetectable.
(T5),and24haftertheendofanesthesia(T24),according totheplasmapeakdescribedintheworkbyHongetal.,28
inwhichIL-6isdetectedin60minwithbloodpeakbetween 4and6handmaypersistfor10days.
Therewasastatisticallysignificantprogressiveincrease in IL-6 dosage in each group. The highest value was at the last collection time (24h after surgical suture). This factcontrastswiththeworksbyLinetal.1 andHerroeder
etal.,4withIL-6peakbetween4and6hinthe
postopera-tiveperiod,andKuoetal.,3withIL-6peak10and12hafter
surgery. Therewasan increasingtrendinthe lastdose of IL-6 in G2 compared to G1, which shows a possible anti-inflammatory effectof lidocaine or itsactive metabolite, MEGX,evenaftertheendofinfusionandbeyondthehalf-life of elimination. Probably, a statistically significant differ-encewouldbeshownbetweengroupsifthesamplesizewas increased.
Experimental studies have shown that MEGX, but not lidocaine,increasedtheglycinergicactivity(inhibitory neu-rotransmission)throughGlyT1blockade(glycine transporter-1) in central nervous system in clinically relevant concentrations.16,29,30Inourstudy,themeanconcentration
of MEGX reached was 0.55gmL−1 5h after the start of
surgery,similartothelevelwhichleadstotheinvitro inhi-bitionofglycinetransport,whichwasobservedduringthe continuousinfusionoflidocaine.29
Unlike some previous studies,6,7 lidocaine showed no
isoflurane and morphine-sparing effect in our study. Fur-thermore, there was no difference in total morphine consumptionbetweengroups.Similarly, somestudieshave reportedanalgesic effectwithlidocaine.17,18 It is possible
thatthesefindingsarerelatedtouniquepatternsof periph-eraland centralsensitizationthat varywiththedifferent typeandlocationofsurgeries.23
Theanalgesiceffectsoflidocainearemorepronounced when it is infusedintraoperatively6 and maycontinue for
days or weeks, that is, beyond infusion time and plasma half-life,11,31 indicating its action on other targets, not
decreasedthedurationofparalyticileus,postoperativepain severity,andopioidconsumption.32---34
A clinically significant reduction in pain severity was observedin theawakeningtimein relationtoother mea-suredtimewithlidocaine,butnotinG2,whichmayreflect thebeneficialeffectoflidocaineoranalgesiceffectof mor-phine.
Noother differenceswereobservedbetween groupsat any assessment time. In this study,intravenous lidocaine infusionduringsurgery(2mgkg−1h−1)withoutinitialbolus
did not improve postoperative analgesia or reduce IL-6 plasma levelsinpatients undergoingopen abdominal hys-terectomy.
More studies are needed to confirm these results and evaluate the beneficial effects of lidocaine in patients undergoingothertypesofsurgery.Moreover,theappropriate dose, the onset time,and the durationof lidocaine infu-sionrequiredtoreducethepostoperativepainremaintobe determined.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LinE,CalvanoSE,LowrySF.Inflammatorycytokines andcell responseinsurgery.Surgery.2000;127:117---26.
2.GebhardF,PfetschH,SteinbachG,etal.Isinterleukin6anearly markerofinjury severityfollowing majortrauma inhumans? ArchSurg.2000;135:291---5.
3.Kuo CP,Jao SW, ChenKM, et al. Comparison of theeffects ofthoracicepiduralanalgesiaandi.v. infusionwithlidocaine on cytokine response, postoperative pain, and bowel func-tion in patients undergoing colonic surgery. Br J Anaesth. 2006;97:640---6.
4.Herroeder S, Pecher S, Schonherr ME, et al. Systemic lido-caineshortenslengthofhospitalstayaftercolorectalsurgery: a double-blinded, randomized, placebo-controlled trial. Ann Surg.2007;246:192---200.
5.LauwickS,KimJ, MichelagnoliG,et al.Intraoperative infu-sionoflidocainereducespostoperativefentanylrequirements in patients undergoing laparoscopic cholecystectomy. Can J Anaesth.2008;55:754---60.
6.KoppertW,WeigandM,NeumannF,etal.Perioperative intra-venouslidocainehaspreventiveeffectsonpostoperativepain and morphine consumption after major abdominal surgery. AnesthAnalg.2004;98:1050---5.
7.Kaba A, Laurent SR, Detroz BJ, et al. Intravenous lido-caineinfusionfacilitatesacuterehabilitationafterlaparoscopic colectomy.Anesthesiology.2007;106:11---8.
8.WuCT,BorelCO,LeeMS,etal.Theinteractioneffectof peri-operativecotreatmentwithdextromethorphanandintravenous lidocaineonpainreliefand recoveryofbowelfunctionafter laparoscopiccholecystectomy.AnesthAnalg.2005;100:448---53.
9.KoppertW, OstermeierN, Sittl R, et al. Low-dose lidocaine reducessecondaryhyperalgesiabya centralmodeofaction. Pain.2000;85:217---24.
10.Kawamata M, Takahashi T, Kozuka Y, et al. Experimen-tal incision-induced pain in human skin: effects of sys-temic lidocaine on flare formation and hyperalgesia. Pain. 2002;100:77---89.
11.AmirR,ArgoffCE,BennettGJ,etal.Theroleofsodium chan-nels in chronic inflammatory and neuropathic pain. J Pain. 2006;7:S1---29.
12.CanaveroS,BonicalziV.Drugtherapyoftrigeminalneuralgia. ExpertRevNeurother.2006;6:429---40.
13.McLureHA,RubinAP.Reviewoflocalanaestheticagents.Min Anesth.2005;71:59---74.
14.Heavner JE. Local anesthetics. Curr Opin Anaesthesiol. 2007;20:336---42.
15.KindlerCH,YostCS.Two-poredomainpotassiumchannels:new sites oflocalanesthetic actionand toxicity.RegAnesth Pain Med.2005;30:260---74.
16.WerdehausenR,KremerD,BrandenburgerT,etal.Lidocaine metabolitesinhibitglycinetransporter1:anovelmechanism fortheanalgesicactionofsystemiclidocaine?Anesthesiology. 2012;116:147---58.
17.Martin F, Cherif K, Gentili ME, et al. Lack of impact of intravenous lidocaine on analgesia, functional recovery, and nociceptivepainthresholdaftertotalhiparthroplasty. Anes-thesiology.2008;109:118---23.
18.Bryson GL, Charapov I, Krolczyk G, et al. Intravenous lidocaine does not reduce length of hospital stay fol-lowing abdominal hysterectomy. Can J Anaesth. 2010;57: 759---66.
19.Moher D, Schulz KF, Altman DG. The Consort statement: revised recommendations for improving the quality of reportsofparallel-grouprandomisedtrials.Lancet.2001;357: 1191---4.
20.Katz J. Pre-emptive analgesia: importance of timing. Can J Anaesth.2001;48:105---14.
21.Omote K. Intravenous lidocaine to treat postoperative pain management.Anesthesiology.2007;106:5---6.
22.TanelianDL,MacIverMB.Analgesicconcentrationsoflidocaine suppresstonicA-deltaandCfiberdischargesproducedbyacute injury.Anesthesiology.1991;74:934---6.
23.Cui W, Li Y, Li S, et al. Systemic administration of lidocaine reduces morphine requirements and postopera-tive pain of patients undergoing thoracic surgery after propofol---remifentanil-basedanaesthesia. EurJAnaesthesiol. 2010;27:41---6.
24.YardeniIZ,BeilinB,MayburdE,etal.Theeffectof perioper-ativeintravenouslidocaineonpostoperativepainandimmune function.AnesthAnalg.2009;109:1464---9.
25.Kang H, Kim BG. Intravenous lidocaine for effective pain relief after inguinal herniorrhaphy: a prospective, random-ized, double-blind,placebo-controlled study.J IntMed Res. 2011;39:435---45.
26.Kim TH, Kang H, Hong JH, et al. Intraperitoneal and intravenous lidocaine for effective pain relief after laparoscopic appendectomy: a prospective, randomized, double-blind,placebo-controlledstudy.SurgEndosc.2011;25: 3183---90.
27.Swenson BR, Gottschalk A, WellsLT, et al. Intravenous lido-caineisaseffectiveasepiduralbupivacaineinreducingileus duration,hospital stay,and painafteropencolonresection: a randomized clinical trial. Reg Anesth Pain Med. 2010;35: 370---6.
28.HongJY, LimKT. Effect ofpreemptive epiduralanalgesiaon cytokineresponseandpostoperativepaininlaparoscopic rad-ical hysterectomyfor cervical cancer.Reg Anesth Pain Med. 2008;33:44---51.
29.Muth-SelbachU, Hermanns H,Stegmann JU,et al. Antinoci-ceptive effects of systemic lidocaine: involvement of the spinal glycinergic system. Eur J Pharmacol. 2009;613: 68---73.
31.McCleaneG. Intravenouslidocaine:anoutdatedor underuti-lizedtreatmentforpain?JPalliatMed.2007;10:798---805.
32.MarretE,Rolin M,BeaussierM,etal.Meta-analysisof intra-venouslidocaineand postoperativerecoveryafterabdominal surgery.BrJSurg.2008;95:1331---8.
33.McCarthyGC,MegallaSA,HabibAS.Impactofintravenous lido-caineinfusion onpostoperative analgesiaand recovery from
surgery:asystematicreviewofrandomizedcontrolledtrials. Drugs.2010;70:1149---63.