Braz. J. Cardiovasc. Surg. vol.17 número4
Texto
Imagem

Documentos relacionados
There has been an explosion of new developments in cardiac surgery such as robotics, minimally invasive valve and coronary artery surgery, a variety of surgical procedures for
[2] demonstrated an excellent durability of mitral valvuloplasty using Carpentier’s technique with only 6.2% of the patients who underwent surgery for degenerative disease
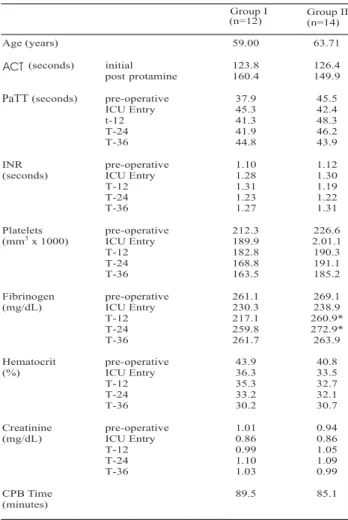
The present investigation shows that the epsilon- aminocaproic acid, in the prescribed dose, was able to reduce the amount of bleeding and need for blood products in the
In the article “Epsilon-aminocaproic acid influence in bleeding and hemotransfusion postoperative in mitral valve surgery”, page 510, the correct title is:
It was not found statistical differences between groups, nevertheless there was a trend in the group using two drugs reaching lower values in migraine index, frequency of attacks
As for reported symptoms (Table 2), there was a significant difference between the two groups: flatulence, postprandial fullness and abdominal pain were more prevalent in the
In 1995, EPEC was divided into two groups, typical EPEC (tEPEC) and atypical EPEC (aEPEC).. The basic difference between the two groups is the presence of the EPEC adherence factor
There was no significant difference (p > 0.05) between the two methods of cultivation studied in terms of the palmitic, linoleic, oleic and stearic fatty acid contents,
