www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Variables
with
prognostic
value
in
the
onset
of
idiopathic
sudden
sensorineural
hearing
loss
夽
,
夽夽
Eduardo
Amaro
Bogaz,
André
Souza
de
Albuquerque
Maranhão
∗,
Daniel
Paganini
Inoue,
Flavia
Alencar
de
Barros
Suzuki,
Norma
de
Oliveira
Penido
DepartmentofOtolaryngologyandHeadandNeckSurgery,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
Received19April2014;accepted14September2014 Availableonline22July2015
KEYWORDS
Prognosis;
Suddenhearingloss; Audiometry
Abstract
Introduction:Theestablishmentofanindividualizedprognosticevaluationinpatientswitha diagnosisofidiopathicsuddensensorineuralhearingloss(ISSHL)remainsadifficultand impre-cisetask,duemostlytothevarietyofetiologies.Determiningwhichvariableshaveprognostic valueintheinitialassessmentofthepatientwouldbeextremelyusefulinclinicalpractice.
Objective:To establish which variables identifiable at the onset ofidiopathic sudden sen-sorineuralhearinglosshaveprognosticvalueinthefinalhearingrecovery.
Methods:Prospective,longitudinalcohortstudy.PatientswithISSHLfollowedbythe Depart-mentofOtology-Neurotologyofaquaternaryhospitalwereincluded.Thefollowingvariables wereevaluatedandcorrelatedwithfinalhearingrecovery:age,gender,vertigo,tinnitus,initial degreeofhearingloss,contralateralearhearing,andelapsedtimetotreatment.
Results:127patientswithISSHLwereevaluated.Ratesofabsoluteandrelativerecoverywere 23.6dBand37.2%respectively.Completehearingimprovementwasobservedin15.7%patients; 27.6%demonstratedsignificantimprovementandimprovementwasnotedin57.5%.
Conclusion:DuringtheonsetofISSHL,thefollowingvariableswerecorrelatedwithaworse prognosis:dizziness,profoundhearingloss,impairedhearinginthecontralateralear,anddelay tostarttreatment.TinnitusattheonsetofISSHLcorrelatedwithabetterprognosis.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:BogazEA,MaranhaoASA,InoueDP,SuzukiFAB,PenidoNO.Variableswithprognosticvalueintheonsetof idiopathicsuddensensorineuralhearingloss.2015;81:520---6.
夽夽Institution:DepartmentofOtolaryngologyandHeadandNeckSurgery,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo
(UNIFESP-EPM),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](A.S.d.A.Maranhão). http://dx.doi.org/10.1016/j.bjorl.2015.07.012
PALAVRAS-CHAVE
Prognóstico;
Perdaauditivasúbita; Audiometria
Variáveiscomvalorprognósticonomomentodainstalac¸ãodaperdaauditiva neurossensorialsúbitaidiopática
Resumo
Introduc¸ão: Elaboraravaliac¸ãoprognósticaindividualizadaem pacientescomdiagnósticode perdaauditivaneurossensorialsúbitaidiopática (PANSI)permanecetarefaárduaeimprecisa devido,emgrandeparte,àvariedadedeetiologias.Adeterminac¸ãodequaisvariáveisteriam valorprognósticonaavaliac¸ãoinicialdopacienteseriadeextremautilidadenapráticaclínica.
Objetivo: Estabelecer quais variáveis, identificáveis no momento de instalac¸ão da perda auditiva neurossensorial súbita idiopática, têm valor prognóstico na recuperac¸ão auditiva final.
Método: Estudo de coorte prospectivo, longitudinal. Incluídos pacientes com PANSI acom-panhados pelaDisciplinadeOtologia---Neurotologiadeumhospitalquaternário. Asseguintes variáveisforamavaliadasecorrelacionadascomarecuperac¸ãoauditivafinal:idade,gênero, vertigem,zumbido,graudeperdaauditivainicial,audic¸ãonaorelhacontralateral,tempopara iníciodetratamento.
Resultado: Foramavaliados127pacientescomPANSI.Astaxasderecuperac¸ãoabsolutae rela-tivaforam23,6dBe37,2%respectivamente.Apresentarammelhoracompletadaaudic¸ão15,7% dospacientes;27,6%apresentarammelhorasignificativae57,5%melhora.
Conclusão:Nomomentodainstalac¸ãodaPANSI,asseguintesvariáveiscorrelacionaram-secom piorprognóstico:vertigem,perdaauditivaprofunda,audic¸ãoalteradanaorelhacontralaterale demoraparainíciodotratamento.Presenc¸adezumbidonainstalac¸ãodaPANSIcorrelacionou-se commelhorprognóstico.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Idiopathicsuddensensorineuralhearingloss(ISSHL)is char-acterizedbytheoccurrenceofahearinglossofatleast30dB inthreecontiguousfrequencies,withitsonsetinaperiod fromafewhoursuptothreedays.1Despitebeingrelatively
common,withanincidenceof5---20casesper100,000
peo-pleperyear,2thephysiopathogenesisofISSHLremainstobe
clarified.ArecurringdrawbackinISSHLisadelayinits
diag-nosisand,duetoavarietyofetiologies,an individualized
prognosticassessmentremainsdifficulttoestablish,andis
frequentlyinaccurate.
Several case seriesindicate thatISSHL typicallyoccurs
inpatientsaged43---53years,withnopredilectionfor
gen-der.Spontaneousrecoveryofhearingthresholdisobserved
inaboutone-thirdto65%ofcases.1,3Despitethelackof
con-sistentdataontreatmentofISSHL,systemiccorticosteroids
havebeenusedinclinicalpracticeasthedrugofchoice.4,5
Studieswithafocusonprognosticfactorshavereceived
limited attention and are usually neglected in lieu of
research on treatment and etiology.6 Determining which
variableswouldhave prognosticvalue inan initialpatient
evaluationwould beextremely useful inclinical practice,
as it would allow an individual classification of patients
accordingtotheseverityofeachcase,aswellasthe
estab-lishmentofamoreaccurateprognosisfor eachindividual,
anddefiningwhichpatientswouldbebenefitedwiththeuse
ofcorticosteroids.Inaddition,itwouldbepossibletomore
preciselyinformpatientsabouttherealchancesofhearing
recovery,inadditiontoavoid theuseof corticosteroids
---an oftenunnecessarytherapy.Finally,it wouldstrengthen
the efforts to change the current paradigm of empirical
treatmentofISSHL.
Thisstudyaimstoestablishwhichvariablesidentifiable
attheonsetofidiopathicsuddensensorineuralhearingloss
haveprognosticvalueinthefinalhearingrecovery.
Methods
This was a prospective, longitudinal cohort study that
includedpatientswithISSHLattendedtoattheSudden
Deaf-nessOutpatientClinicandfollowed-upbytheDepartmentof
Otology-Neurotologyataquaternaryhospital.Thisproject
wasapprovedbytheinstitution’sEthicsCommittee,under
protocol0715/11.
Allpatientswere treatedwithprednisone1mg/kg/day
(maximumdailydose=60mg)POfor at leastaweek. The
dosewasreducedweeklyforupto21days.Thosepatients
withcontraindications to the use of this dosage of
pred-nisone had their dose reduced; or, in some rare cases,
replacedbydeflazacort.
Patients with a history of middle and inner ear
dis-ease with a defined etiology such as trauma, infection,
perilymphaticfistula,retrocochleardisease(schwannoma),
degenerativedisease of the centralnervous system
(mul-tiple sclerosis), exposure to ototoxic drugs, barotrauma,
middle or inner ear malformation, history suggestive of
mumps,definite Ménière’s disease, bilateral ISSHL cases,
andpatientswhohadtheonsetofmonitoringnotbeginuntil
45daysaftertheonsetofhearinglosswereexcludedfrom
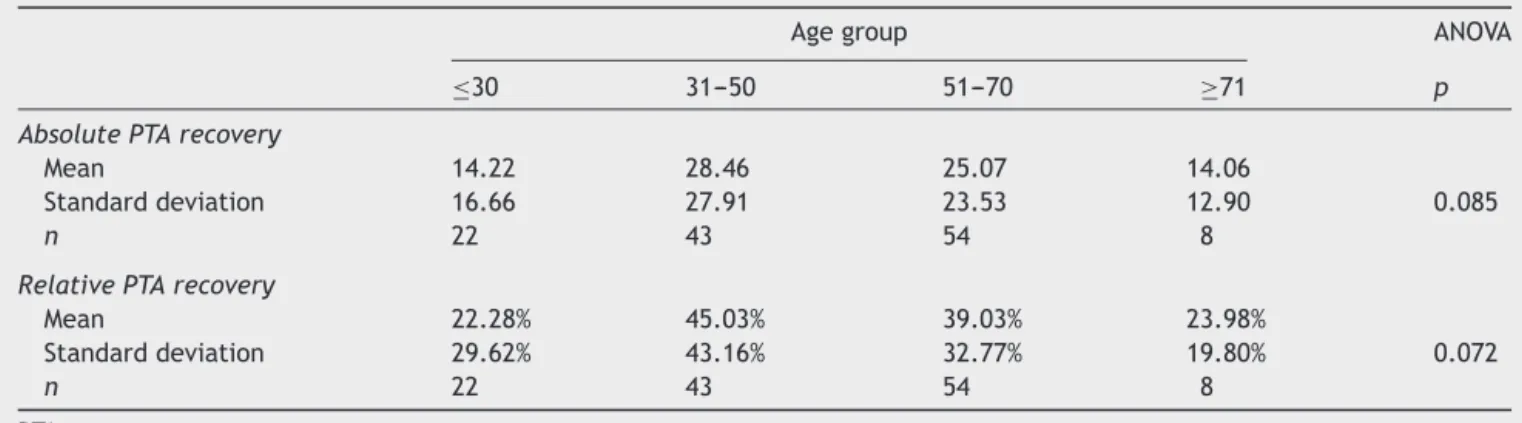
Table1 ANOVAtestsamongagegroupsforrecoveryrates.
Agegroup ANOVA
≤30 31---50 51---70 ≥71 p
AbsolutePTArecovery
Mean 14.22 28.46 25.07 14.06
Standarddeviation 16.66 27.91 23.53 12.90 0.085
n 22 43 54 8
RelativePTArecovery
Mean 22.28% 45.03% 39.03% 23.98%
Standarddeviation 29.62% 43.16% 32.77% 19.80% 0.072
n 22 43 54 8
PTA,puretoneaverage.
Thehearingassessmentofpatientswasperformedwith anMAICOMA-41audiometer,andalltestswereperformed bythe samespeechtherapist. The initialand final audio-metricparameterswereevaluated;thelastevaluationwas obtainedtwomonthsaftertheinitialaudiometry,orbefore inthosepatientswithafullrecovery.Inpatientswherethe hearingthresholdsofprofoundlosseswerenotdetected,the maximumaudiometriclimitwasconsideredastheresponse (inthiscase,120dB).
In all patients, the means of initial and final pure toneswere obtained, according to the group of frequen-ciesaffected.Whenlowandmediumtoneswereinvolved, themeansof 0.25,0.5,1, and2kHzfrequencies was cal-culated;whenmediumandhighfrequencieswereaffected, themeansof1,2,3,4,6,and8kHzfrequencieswere cal-culated;whenonlyhighfrequencytoneswereinvolved,the means of3, 4, 6,and 8kHz frequencies werecalculated; andfinallywhenlow,medium, andhigh frequencieswere affected,themeanofalleightfrequencieswascalculated. Levels of 250 and 500Hz; 1 and 2kHz; and 3, 4, 6, and 8kHzwereconsideredlow,medium,andhighfrequencies, respectively.
Thefollowinghearingrecoverycriteriawereused:
• Improvement: a change of functional category, and improvementof15dB.
• Significantimprovement:therewasimprovement,witha finalhearinglossofmildintensity.
• Fullimprovement:therewasimprovement,withhearing thresholdsreturningtonormal(25dB).
Tocalculatehearingrecovery,Tuccietal.7hassuggested
the use of audiometric thresholds for the unaffected ear
asa baseline value, under the premise that therewas a
symmetrical hearing level before the ISSHL episode. For
this calculation, the author took into account only the
initial pure tone average (PTA) from the unaffected ear.
However, in the present study used the initial and final
PTAvalues for theunaffected side, withthe objectiveof
reducing both systematic and random errors, taking into
accountthatthemeasuresontheaffectedandunaffected
sides were obtained at the same time. Therefore, PTA
relative recovery was calculated using the following
for-mula,indB:
PTArecovery(dB)=(PTAIA−PTAINA)−(PTAFA−PTAFNA).
ThecalculationofPTArelativerecovery(asapercentage)
wascarriedoutwiththeuseofthefollowingformula:
PTArecovery(%)=(PTAIA−PTAINA)−(PTAFA−PTAFNA)
×100/(PTAIA−PTAINA).
where PTAIAis theinitialPTAof theaffectedear;PTAINA
is theinitial PTAofthe unaffectedear;PTAFAisthe final
PTAoftheaffectedear;andPTAFNAisthefinalPTAofthe
unaffectedear.
The following variableswere evaluatedand correlated
withPTArecoveryrates:age,gender,vertigo,tinnitus,
ini-tialdegreeofhearingloss,hearinginthecontralateralear,
andtimetoonsetoftreatment.
Inthestatisticalanalysis,independentStudent’st-tests
wereusedwhencomparingtwogroups,andANOVA(analysis
ofvariance)testswereusedwhencomparingthreeormore
groups,consideringasignificancelevelof5%.
Results
From2000to2010,277patientswithISSHLwereevaluated
attheSuddenDeafnessOutpatientClinic.Ofthistotal,eight
patients didnotmeet thedefinitioncriteriaforloss ofat
least30dBinatleastthreeconsecutivefrequencies.In
addi-tion,tencaseswerebilateral;andin33patientsthecause
ofhearinglosswasfound.Seventy-fivepatientswerelostto
follow-up,andin24patientstheinformedconsentwasnot
obtained.Therefore,takingintoaccounttheinclusionand
exclusioncriteria,thefinalsamplecontained127patients.
The absolute and relative recovery rates were 23.6dB
and 37.2%, respectively. 15.7% of patients showed full
improvement,27.6% showedsignificant improvement,and
57.5%showedimprovement.
The average age was 48 years (range 12---82 years).
Table 1shows PTArecovery rates in differentagegroups.
Table2 Independent Student’s t-tests between genders forrecoveryrates.
Gender t-test
Female Male Patient
AbsolutePTArecovery
Mean 24.06 23.23
Standarddeviation 25.01 23.22 0.847
n 64 63
RelativePTArecovery
Mean 36.74 37.70
Standarddeviation 35.57 37.18 0.882
n 64 63
PTA,puretoneaverage.
Table3 IndependentStudent’st-testsbetweenpresence andabsenceoftinnitusforrecoveryrates.
Tinnitus t-test
No Yes p
AbsolutePTArecovery
Mean 5.81 25.17
Standarddeviation 17.07 23.99 0.014
n 10 117
RelativePTArecovery
Mean 13.44% 39.25%
Standarddeviation 41.63% 35.20% 0.030
n 64 63
PTA,puretoneaverage.
female.PTArecoveryratesbetweengendersareincludedin
Table2.
Tinnitusoccurredin92.1%(n=117)ofcases.PTArecovery
rates for those with and without symptoms are shown in
Table3.Vertigowaspresentin52.8%(n=67)ofcases.PTA
recoveryrates werecomparedbetween patientswithand
withoutthissymptom,asshowninTable4.
TheresultsshowninTable5comparethedegreeofthe
initialhearinglosswithPTArecoveryrates.
Table4 IndependentStudent’st-testsbetweenpresence andabsenceofvertigoforrecoveryrates.
Vertigo t-test
No Yes p
AbsolutePTArecovery
Mean 25.83 21.70
Standarddeviation 26.01 22.16 0.330
n 60 67
RelativePTArecovery
Mean 47.69% 27.83%
Standarddeviation 42.44% 26.60% 0.002
n 60 67
PTA,puretoneaverage.
Fig.1shows thepercentages of patientsachieving
sig-nificantimprovementintheirhearingacuity,separatedby
groupsofaffectedfrequencies.
Contralateralearhearinginvolvementwascomparedvs.
individualswithouthearingalterationintheircontralateral
ear,andtheresultsareshowninTable6.
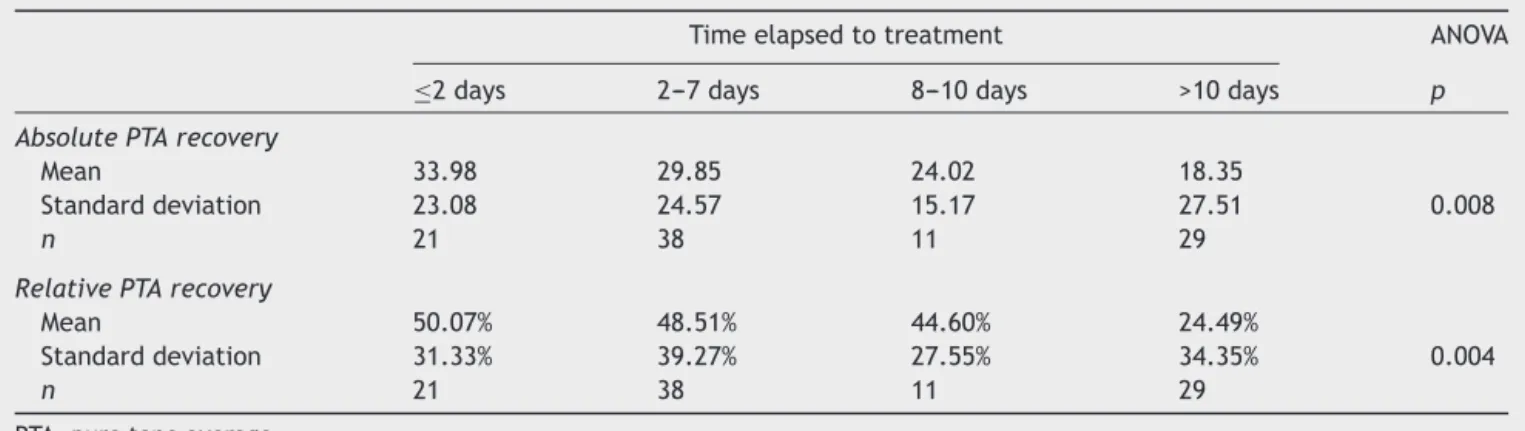
Thetimeelapsedtotreatment,at differenttimes,and
theirrespectivecorrelationwithPTArecovery,areshownin
Table7.
Discussion
The word ‘‘prognosis’’, etymologically derived from the
Greek,means‘‘toknowbeforehand.’’Establishedasakey
conceptofmedicinebyHippocrates,8theactof
prognostica-tiononlyisjustifiedifbased---inanecessaryandmandatory
way --- on a sufficient medical diagnosis. An apocryphal
phraseteaches:‘‘Therefore,thereisnocredibleprognosis
withoutdiagnosis.’’
Thus,achallengearisesindeterminingtheprognosisofa
diseaselikeISSHLthat,bydefinition,isanidiopathicevent.
Infact,ISSHLwouldbebetterlabeledasasymptomcommon
tomultiple diseases and,therefore,withdifferent
etiolo-gies ---and for each etiology,witha respectiveprognosis.
The interpretation and comparison of studies on
progno-sticfactorsinpatientswithISSHLstillconstituteadifficult
Table5 ANOVAtestsamonggradesofinitiallossforrecoveryrates.
Gradeofinitialloss ANOVA
Moderate Severe Profound p
AbsolutePTArecovery
Mean 20.29 23.60 25.88
Standarddeviation 17.45 25.20 27.59 0.546
n 34 37 52
RelativePTArecovery
Mean 48.21% 34.79% 28.76%
Standarddeviation 38.25% 37.10% 31.81% 0.046
n 34 37 52
60%
% of patients
50% 50%
44.4%
25%
0% 40%
30%
20%
10%
0%
Low and middle Middle and high Low, middle, and high
Only high
Figure1 Distributionofsignificanthearingrecoverypercentagebygroupsofaffectedfrequencies.
Table6 IndependentStudent’st-testsbetween contralat-eralearhearingstatesforrecoveryrates.
Contralateralear t-test
Normal Changed p
AbsolutePTArecovery
Mean 25.70 11.22
Standarddeviation 24.02 20.73 0.017
n 109 18
RelativePTArecovery
Mean 39.78% 21.67%
Standarddeviation 34.41% 43.73% 0.049
n 109 18
PTA,puretoneaverage.
and imprecise task, and there is no consensus regarding the actual influence of the factors studied in the clini-cal outcome of patients. Several prognostic factors have been studied in recent decades,with inconsistent results regardingtheindividualinfluenceofeachfactor.2,9---16
In the present study,there was nostatistically
signifi-cant differencefor improvementof PTArecovery rates in
those different age groups studied. However, there was
a trend of a better performance in age groups of 31---50
and 51---70 years. In extreme ages, absolute and relative
recoveryrateswerelowerthanthosefortheglobalsample.
A well designed eight-year prospective study found
simi-lar results, withpoorerhearing recovery inpatients aged
under 15years andabove60 years;that study attributed
these findings to a vulnerability of the immune system,
peculiar to extremes of age, as a probable explanation.2
Nakashima et al.17 found higher rates of profound losses
in children under14 years.Several studiesconsider older
ageasapoorprognosisfactorforhearingrecovery.11,13,18---20
It ispostulatedthat thecellulardegenerationinherentto
thenaturalprocessofaging,inassociationwithareduced
capacity for metabolic and cellular regeneration, have a
negativeinfluence.13Otherstudies,however,foundnosuch
correlation.10,12,14
Nocorrelation was found between gender and hearing
recovery degree in this study, confirming the findings of
otherpublications.13,19,21
Tinnituswas present in 92.1% of patients, a very high
prevalence. This group of patients had statistically
sig-nificant higher rates of absolute and relative recovery
comparedtothegroupwithouttinnitus,corroborating
pre-viousstudies.10,22,23Itisassumedthatpresenceoftinnitus
aftercochlearinjury wouldindicatethathair cellsremain
viable.24
Vertigowas present in 52.8% of subjects,who showed
lowerrelativerecoveryratescomparedtothegroup
with-out this symptom (p=0.002). It is well-established that
Table7 ANOVAtestsamonggroupsfortimeelapsedtotreatmentandrecoveryrates.
Timeelapsedtotreatment ANOVA
≤2days 2---7days 8---10days >10days p AbsolutePTArecovery
Mean 33.98 29.85 24.02 18.35
Standarddeviation 23.08 24.57 15.17 27.51 0.008
n 21 38 11 29
RelativePTArecovery
Mean 50.07% 48.51% 44.60% 24.49%
Standarddeviation 31.33% 39.27% 27.55% 34.35% 0.004
n 21 38 11 29
vertigo is a factor for worse prognosis.2,3,9---11,13,14,18,22,23,25
A study analyzing 13 patients diagnosed with ISSHL with
and without vertigo revealed that those with losses in
high frequencies showed better recovery in the absence
of vertigo.17 The authors concluded that the
inflamma-tory response located in the basal region of the cochlea
couldovercomethebarriersoftheanteriorlabyrinth,reach
thevestibuleandsemicircularcanalsandtriggervestibular
symptoms.
The relativerecoveryratewashigherfor patientswith
moderatevs.profoundloss,withstatisticalsignificance
dif-ference.Manystudiesconsidertheinitialdegreeofhearing
lossasanimportantprognosticfactor.Inpatientswitha
pro-nouncedinitialhearingloss,theworstaudiologicalresultis
expectedat the end offollow-up.2,3,9,10,20,22 Itis believed
thatincasesofprofoundloss,theextentofhaircellinjury
issoextensive,itdoesnotallowasignificantstructuraland
functionalrecovery.
Withtheindividualizationofhearingrecoveryby group
of affected frequencies, it was noted that high
frequen-cies, whenviewed in isolation,were not accompaniedby
asignificant hearingrecovery (Fig.1),while thelow- and
middle-frequencygroupsachievedbetterresults.Itshould
be borne in mind that most studies do not include this
differentiation by frequency, a fact which certainly
com-promisestheanalysisofresults.Itisestimatedthatabout
one-thirdto65%ofcasesofISSHLachievespontaneous
hear-ing recovery,1,3 but the parametersusedtomeasure such
improvement are, as a rule, speech reception threshold
(SRT),speechrecognitionthresholdindex(SRTI),andPTA,
which do not cover higher frequencies, especially 6 and
8kHz.
Subjectswithnormalcontralateralhearingshowed
abso-lute and relative recovery rates higher than those with
alteredcontralateral hearing,with statisticallysignificant
differenceforbothrates.Previousstudieswithlarger
sam-ples also concluded that altered contralateral hearing is
associatedwithaworseprognosis.2,10Itisbelievedthatthis
changeindicatessomepre-existingdysfunctionofthe
audi-torysystem,orofother systemsofthebody,thatreduces
thepotentialforrecovery.
Patientswhostartedtheirtreatmentbeforesevendays
had higher rates of absolute and relative recovery
com-pared topatients included in the categories above seven
and ten days(p=0.008), a resultsimilar toseveral other
studies.10,12---14,18,19,25 There was no statistically significant
difference in recovery rates among patients who started
theirtreatmentwithin48handuptosevendays,suggesting
thattreatmentwithcorticosteroidshasthesame
effective-ness,ifstartedwithinsevendays.Inastudyof347subjects,
nobenefitwasnotedwithanearlyonsetoftreatment,
com-paringpatientswhostartedcorticosteroidswithintwodays
orbetweenthreeandsevendays.26
Conclusion
At thetimeof ISSHL onset,the followingvariables
corre-lated witha worse prognosis: dizziness, profound hearing
loss,changeincontralateralearhearing,andadelayedstart
oftreatment.PresenceoftinnitusatISSHLonsetcorrelated
withabetterprognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.WilsonWR,BylFM,LairdN.Theefficacyofsteroidsinthe treat-mentofidiopathicsuddenhearingloss.Adoubleblindclinical study.ArchOtolaryngol.1980;106:772---6.
2.BylFMJr.Suddenhearingloss:eightyearsexperienceand sug-gestedprognostictable.Laryngoscope.1984;94:647---61. 3.MattoxDE,SimmonsFB.Naturalhistoryofsuddensensorineural
hearingloss.AnnOtolRhinolLaryngol.1977;86:463---80. 4.ConlinAE,ParnesLS.Treatmentofsuddensensorineural
hear-ing loss: a meta-analysis.Arch Otolaryngol Head Neck Surg. 2007;133:582---6.
5.Stachler RJ, Chandrasekhar SS, Archer SM, Rosenfeld RM, SchwartzSR,BarrsDM,etal.Clinicalpracticeguideline:sudden hearingloss.OtolaryngolHeadandNeckSurg.2012;146:S1. 6.Royston P, Moons KGM, Altman DG, Vergouwe Y. Prognosis
andprognosticresearch:developingaprognosticmodel.BMJ. 2009;338:b604.
7.Tucci DL, Farmer JC Jr, Kitch RD, Witsell DL. Treatmentof suddensensorineural hearinglosswithsystemicsteroids and valacyclovir.OtolNeurotol.2002;23:301---8.
8.Hippocrates onairs,waters and places.AdamsF,editor. The genuineworksofHippocrates.Baltimore:WilkinsandWilkins; 1939.
9.CeylanA,CelenkF,KemalogluYK,BayazitYA,GoksuN,Ozbilen S.Impactofprognosticfactorsonrecoveryfromsuddenhearing loss.JLaryngolOtol.2007;121:1035---40.
10.CvorovicL,DericD,ProbstR,HegemannS.Prognosticmodelfor predictinghearingrecoveryinidiopathicsuddensensorineural hearingloss.OtolNeurotol.2008;29:464---9.
11.SuzukiH,MoriT,HashidaK,ShibataM,NguyenKH,Wakasugi T,etal.Predictionmodelforhearingoutcomeinpatientswith idiopathicsuddensensorineuralhearingloss.EurArch Otorhi-nolaryngol.2011;268:497---500.
12.Xenellis J, Karapatsas I, Papadimitriou N, Nikolopoulos T, MaragoudakisP,TzagkaroulakisM,etal.Idiopathicsudden sen-sorineural hearing loss: prognosticFactors. J Laryngol Otol. 2006;120:718---24.
13.ChangNC,Kuen-YaoHoMD,KuoWR.Audiometricpatterns prog-nosisinsuddensensorineuralhearinglossinSouthernTaiwan. OtolaryngolHeadNeckSurg.2005;133:916---22.
14.MamakA,YilmazS,CansizH,InciE,GucluE,DerekoyluL.A studyof prognosticfactors insudden hearingloss. Ear Nose ThroatJ.2005;84:641---4.
15.NagaokaJ,AnjosMF,TakataTT,ChaimRM,BarrosFA,PenidoNO. Idiopathicsuddensensorineuralhearingloss:evolutioninthe presenceofhypertension,diabetesmellitusanddyslipidemia. BrazJOtorhinolaryngol.2010;76:363---9.
16.PenidoNO,RamosHVL,BarrosFA,CruzOLM,ToledoRN.Fatores clínicos,etiológicoseevolutivosdaaudic¸ãonasurdezsúbita. BrazJOtorhinolaryngol.2005;71:633---8.
17.NakashimaT,YanagitaN.Outcomeofsuddendeafnesswithand withoutvertigo.Laryngoscope.1993;103:1145---9.
18.Byl FM. Seventy-six cases of presumed sudden hearing loss: prognosisandincidence.Laryngoscope.1977;87:817---25. 19.Nosrati-Zarenoe R, Arlinger S, Hultcrantz E. Idiopathic
sud-densensorineuralhearingloss:resultsdrawnfromtheSwedish nationaldatabase.ActaOto-Laryngologica.2007;127:1168---75. 20.LairdN,WilsonWR.Predictingrecoveryfromidiopathicsudden
hearingloss.AmJOtolaryngol.1983;4:161---5.
steroid,dextranandpiracetam:experiencewith68cases.Eur ArchOtorhinolaryngol.2004;261:187---90.
22.SaekiN,KitaharaM.Assessmentofprognosisinsudden deaf-ness.ActaOtolaryngol(Stockh).1994:S56---61.
23.ParkHM,JungSW,RheeCK.Vestibulardiagnosisasprognostic indicatorinsuddenhearinglosswithvertigo.ActaOtolaryngol (Stockh).2001:S80---3.
24.Danino J, Joachims HZ,Eliachar I,Podoshin L, Ben-David Y, FradisM.Tinnitusas aprognosticfactorinsuddendeafness. AmJOtolaryngol.1984;5:394---6.
25.ShaiaFT,SheehyJL.Suddensensori-neuralhearingimpairment: areportof1220cases.Laryngoscope.1976;86:389---98. 26.HuyPT,SauvagetE.Idiopathicsuddensensorineuralhearingloss