SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Functional
assessment
of
endoprosthesis
in
the
treatment
of
bone
tumors
夽
Denis
Kiyoshi
Fukumothi,
Hiran
Pupo,
Luciano
Augusto
Reganin
∗,
Silvia
Raquel
Fricke
Matte,
Bruno
Spagnuolo
de
Lima,
Carlos
Augusto
de
Mattos
PontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),HospitaleMaternidadeCelsoPierro,Servic¸odeOrtopediae Traumatologia,Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20October2015 Accepted7January2016 Availableonline30August2016
Keywords: Boneneoplasms
Reconstructivesurgicalprocedures Jointprosthesis
Limbsalvage
a
b
s
t
r
a
c
t
Objectives: Evaluatethefunctionalgradeofthesepatientsandtoidentifythetypesof com-plicationsfoundthatinfluencedtheaveragelifespanofendoprosthesesthefunctionsof theoperatedlimb.
Methods:Weanalyzed14post-operativecasesofendoprosthesis,patientswithmalignant bonetumorsandaggressivebenignbonetumorssubmittedtosurgerybetween2004and 2014.TheevaluationsystemusedwasproposedbyEnneking,recommendedbythe Muscu-loskeletalTumorSociety(MSTS),inadditiontotheradiologicevaluation.
Results:Endoprosthesisareexcellentchoicesforthetreatmentofbonetumorswithlimb preservation inrelationtopain,strength, andpatient’s emotionalacceptance. Another factorforgoodresultsistheimmediateweight-bearingcapacity,generatingagreater inde-pendence.
Conclusion: Theauthorsconcludethatallpatientsclassifiedthetherapyasexcellent/good, regardlessofthetypeofprosthesisused,extentofinjury,and/ortypeoftumorresection performed.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Avaliac¸ão
funcional
das
endopróteses
no
tratamento
de
tumores
ósseos
Palavras-chave: Neoplasiasósseas Procedimentoscirúrgicos reconstrutivos
r
e
s
u
m
o
Objetivo:Avaliarograufuncionaldessespacienteseidentificarostiposdecomplicac¸ões encontradasequeinfluenciaramnasobrevidadasendoprótesesenafunc¸ãodomembro operado.
Métodos:Foramanalisados14pós-operatóriosdeendoprótesesempacientesportadoresde tumoresósseosmalignosebenignosagressivoscomcirurgiaentre2004e2014.Osistema
夽
StudycarriedoutatthePontifíciaUniversidadeCatólicadeCampinas(PUC-Campinas),HospitaleMaternidadeCelsoPierro,Servic¸o deOrtopediaeTraumatologia,Campinas,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](L.A.Reganin). http://dx.doi.org/10.1016/j.rboe.2016.08.012
Prótesearticular Salvamentodemembro
deavaliac¸ãofoiopropostoporEnneking,preconizadopelaMusculoskeletalTumorSociety (MSTS),alémdaavaliac¸ãoradiográfica.
Resultados: Asendoprótesessãoótimasopc¸õesnotratamentode tumoresósseoscom preservac¸ãodomembro,emrelac¸ãoàdor,forc¸aeaceitac¸ãoemocionaldopaciente.Outro fator parabonsresultados éa capacidadedesuportede pesoimediato,quegerauma independênciamaior.
Conclusão:Todosospacientesclassificaramaterapiacomoexcelente/boa,indiferentemente dotipodeprótese,extensãodalesão,tipodetumoreressecc¸ãofeita.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Withadvancesinprotocolsandtreatmentofcancerpatients andconsequentincreaseinsurvival,thenumberofpatients with bone metastases has increased, as well as the inci-dence of complications.1–4 One ofthe complications often foundinthesepatientsarepathologicalfractures,especiallyin thelowerlimbs,whichinvariablyaffectthemeta-epiphyseal regionoftheboneandrequiresjointreconstruction.Regarding primarybonetumors,thesehavealsohadbetteroutcomes afteruseofmultidrugtherapy,resultinginlimbsalvage pos-sibility;that,inmostcases,isonlyobtainedwithlargebony resections,leadingtotheneedforreconstructionofthisbone segment, which in most cases can be attained with non-conventionalendoprosthesis.
Metastatic bone disease is the most common bone
malignancy,1primarilyaffectingtheaxialskeleton,pelvisand femur.5,6 Metastaticinvolvementofthelowerlimbsis asso-ciatedwithagreater number ofpathologicalfractures and promotesincreasedmorbidity/mortalityduetoprolonged bedrest,increasedriskofpneumoniaandthromboembolic events.6Underthesecircumstances,replacementofthebone segment can be attained with an endoprosthesis, which rapidlyrehabilitatesthispatient,whobecomesanambulatory patient.1,7–9
Regardingprimarybonetumors,osteosarcomaandEwing’s sarcoma,aswellasgiantcelltumors(GCT)ofthebone,also occurmoreofteninthelower limbs,withthedistalfemur andproximaltibiabeingthepreferredlocations,affectingthe jointregionwhileresultingintheneedforjointreplacement. Asintheupperlimbs,thesetumorsnotinfrequentlyaffect theproximalhumerus.2,7
For primarymalignant and aggressivebenign tumors, a wide resection to achieve necessary safety margin results in largebony resections and, therefore, the need for local reconstruction.8,10
Amongthe techniquesbased on limbsalvage principle, onethat has been recommended fortreating bone metas-tases in the lower limbs and the proximal humerus, due tobetterresponseandeffectiveness,islesionresectionand replacementoftheresectedsegmentbyanunconventional endoprosthesis,5,11,12themethodofchoiceinourservice.
For malignant primary bone tumors (osteosarcoma,
Ewing’s sarcoma, chondrosarcoma) and aggressive benign tumors (Enneking’s B3) obtaining a broad or radical mar-gin invariably results in large meta-epiphyseal bone loss,
requiringbiologicalorprostheticreconstruction.13Largebone resectionsoccurringduringsurgicalrevisionsofconventional arthroplastiesareanotherconditionthatrequirestheuseof endoprostheses.
Insuchcases,thebiological reconstructionscanbe per-formed with autologous bone graft, free or vascularized, homologous graft (tissue bank) or other autograft meth-ods.Althoughmorenatural,biologicalreconstructionshows severelimitationsinmostcases.13
Prosthetic reconstructions are performed with non-conventionalendoprostheses,whichreplacebonesandjoints. Theyareofeasyaccess,providesanatomicalreconstructionof thelimb,functionallyandfast,resultinginearlyambulation recovery.However,theyalsohaveahighnumberof compli-cationswithinshort-andlong-termfollow-up.Postoperative complicationsofbonetumorresectionsandreplacementof the resected segment by an endoprosthesis are: infection, aseptic implant loosening, periprosthetic fracture, implant fractureandtumorrecurrence.1,7,14
Thesecomplicationscanberesponsibleforthefunctional impairmentoftheaffectedlimb,implantlossandeventhe amputationoftheaffectedlimb.
Thepurposeofthisstudyistoidentifythetypesof com-plicationsfoundthatinfluencedtheaveragelifespanofthe endoprostheses and function of the operated limb of our patients, according tothe functional analysisofthe MSTS. These datacanbeusedtoimprove implantmanufacturing and surgicaltechniques,astheimprovementoforthopedic implants and techniques usedin bonedefect replacement afterneoplasticresectioniscrucialtoachievegreater dura-bility,withfewercomplicationsand increasedfunctionality oftheoperatedlimb.5,12–15
Material
and
methods
Thisisaretrospectivestudywith14patientswithmalignant andaggressivebenign(Enneking’sB3)tumors,whorequired reconstructive surgerywithnon-conventional endoprosthe-sis.Patientswithincompletemedicalrecordsthatwouldnot allowassessmentandthosewhodiedorweretransferredto anotherservicebeforecompletingoneyearoffollow-upwere excluded.PatientswhodidnotsignanInformedConsentForm werealsoexcluded.
Table1–Patientdata.
Patient Gender Age Surgery Site Primarytumor Amputation
1 M 41 2004 Knee GCT No
2 M 52 2008 Hip Chondrosarcoma No
3 F 61 2008 Knee Chondrosarcoma Yes
4 F 66 2008 Knee Chondrosarcoma No
5 M 58 2010 Knee Chondrosarcoma Yes
6 F 81 2011 Knee Metastasis No
7 F 28 2012 Knee GCT No
8 F 60 2013 Knee Metastasis–Breast No
9 F 74 2013 Knee Chondrosarcoma Yes
10 M 65 2014 Shoulder Chondrosarcoma No
11 F 56 2014 Hip Metastasis–Kidney No
12 M 19 2014 Knee EwingSarcoma No
13 F 49 2014 Knee MultipleMyeloma No
14 F 31 2014 Knee GCT No
Fig.1–Preoperativeradiographiesofoneofthestudy patients,diagnosedwithGCTintheleftdistalfemur.
locatedinthe shoulder, two (14%)inthe hip and 11 (78%) intheknee(Fig.1).Consideringtumortype,one(7%)wasa myeloma,one(7%)anEwing’stumor,three(21%)werebone metastasesandsix(42%)werechondrosarcomas.Allsurgeries
wereperformedbetween2004and2014(Fig.2).Threepatients underwent amputation due to late complications of the endoprosthesisprimaryprocedure.Thesedataareshownin Table1.
Functional assessment was performed according to the classification recommended by Enneking, adopted by the Musculoskeletal Tumor Society (MSTS), whose parameters aremobility,pain,function,emotionalacceptance,supports, walking,gait,rangeofmotion(ROM)andstrength.Each func-tionalassessmentparameterwasevaluatedwithsixscoring levels,withthehighestscorebeingfiveandthelowest,zero. Radiographicimagingwasalsoevaluatedregardingthe endo-prosthesisstability,asshowninTable2.
UsingtheRandExcelsoftwareprograms,theexploratory data analysiswas carried out with11 patients(threewere excludedfromthedataanalysisduetoamputation) submit-tedtoendoprosthesistreatment.Thisworkaimstoevaluate whethertheendoprosthesisisaneffectivetreatment.Using aQQplotofthemeanscores,theassumptionofnormalityof scoreswasconfirmed,thatis,asthepointsareclosetothe line,thet-testcanbeusedtocomparethemeansofthedata, asshowninTable3andFig.3.
Table2–Questionnaireresults.
Patient Pain Function Emotionalacceptance Supports Walking Gait Strength ROM
1 3 5 4 6 5 4 6 2
2 6 5 6 2 4 3 6 5
3 – – – – – – – –
4 4 4 6 1 3 2 4 6
5 – – – – – – – –
6 6 2 6 2 3 2 6 3
7 6 5 4 6 6 4 6 5
8 6 2 6 1 2 2 6 6
9 – – – – – – – –
10 4 1 4 6 – – 0 0
11 4 3 5 1 3 2 6 4
12 5 5 4 6 5 5 6 4
13 4 3 2 3 4 3 6 5
14 3 3 6 6 6 2 6 2
–0.5 –1.0 –1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0
0.0 Theoretical quantiles
Sample quantiles
1.5 1.0 0.5
Fig.3–Q–Qplotofthemeantotalscores.
Results
Thescorevalueforeachpatientmayvary fromeightto48 andthemeanvalueobtainedwas32.Halfofthepatientswho answeredthequestionnairehadascorebetween30and36. Thelowestobservedscorewas15andthehighestwas42.
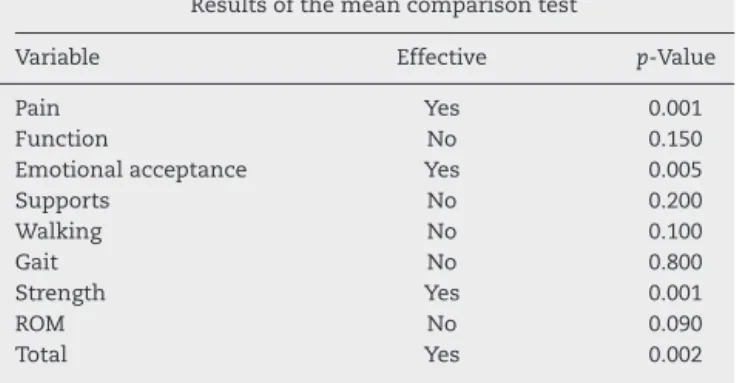
Intheoverallanalysisoftheendoprosthesiseffectiveness andafterestablishingthatmeanscoreshigherthanthreeis consideredagoodresultandusingStudent’st-test (compari-sonofmeans)todeterminethemeanscores,apvalue=0.002 wasobtained,astatisticallysignificantresult.
Allvariableswerealsoanalyzedseparately,usingthesame Student’stmethod,consideringaresponsehigherthanthree asatisfactoryresult.Theresultsrangedfrom0.005pto0.8. Pain, emotional acceptance and strength were statistically
Table3–Meanoftotalscoresofquestionsperpatient.
Patient Meanofscores
1 4.375
2 4.625
4 3.75
6 3.75
7 5.25
8 3.875
10 1.875
11 3.5
12 5
13 3.75
14 4.25
significantandshowedapvalue<0.05.Asforfunction, sup-ports,walking,gaitandROM,theyallshowedapvalue>0.05. Regardingradiographies,allprostheseswerestable,with no apparentsigns ofloosening orinfection, exceptforthe patients who underwent amputation due to postoperative complications or tumor recurrence. All radiographies were performedinthesameservice.
Discussion
Thecurrentliteratureisscarceregardingfunctionalresults after limb salvage surgery inpatients with malignant and aggressive benign tumors, most likelydue to the rarity of primarybonetumors.Inrecentdecades,treatmentofbone tumors went through changes, since the previously pre-ferred treatment for most cases was amputation. In the beginningofthiscentury,limbsalvagesurgerybecame pre-dominantamongsurgeons,andamputationsbecomeonlyan option,orthetreatmentofcomplicationsafterlimbsalvage surgeries.15,16
InastudycarriedoutatCentroInfantilBoldrinipublished in2008,authorscomparedtwogroupsofpatientswithbone sarcomasinthedistalendofthefemur,onewithtotaland anotherwithpartialendoprostheses,therewasnoinfluence ontheoverallfunctionaloutcomeandastatistically signifi-cantdifferencewasobservedonlyregardingstability.17
In general, non-conventional endoprostheses are excel-lent devicesinthe reconstruction oflarge boneresections; however, theyhavemechanical limitations,which mustbe consideredbeforetheirindication.
Thisstudyagreeswiththecurrentliteratureandobtained thesameresults,showingthattheendoprosthesisisan excel-lentoptioninthetreatmentofbonetumorswithlimbsalvage, especiallyinrelationtopain,strengthandpatientemotional acceptance,accordingtotheresultsshowninTable4.During the interview, all patients emphasized emotional improve-mentaftersurgery,mainlyduetopainimprovement.Another factor thatcontributestothe goodresultsdemonstratedin this study is the immediate load-bearing capacity, which resultsingreaterpatientindependence.
Table4–Resultsoftests,theirefficacyandrespective
p-value.
Resultsofthemeancomparisontest
Variable Effective p-Value
Pain Yes 0.001
Function No 0.150
Emotionalacceptance Yes 0.005
Supports No 0.200
Walking No 0.100
Gait No 0.800
Strength Yes 0.001
ROM No 0.090
Total Yes 0.002
resectionduringsurgery.Thislossofmusclemassalso wors-ensambulationcapacityandincreasestheneedforassistance duringgait.Asaconsequenceoflimbdeterioration,limb func-tionbecomeslimited,whichagaindemonstratestheresults showninthisstudy.
Conclusion
Allpatientsclassifiedthetherapyasexcellent/good, regard-lessoftheprosthesistype,lesionextension,tumortypeand resectionperformed.
Mostpatientswithbonetumorswithlimbsalvage indi-cationhadalifeprognosisbelowthatfoundinthegeneral population,so theearlyreturn toeverydayactivities, inde-pendenceandambulationcapacityarethetreatmentgoals, makingendoprosthesisaviableandeffectiveoptionforthese patients.
Despitethelimitedstudysample,theresultsobtainedfrom the questionnairesupportthe current literature.Giventhe limitationofpatientsthatareadequateforthissampleand thefactthatitisacurrentissue,webelievethatthe endo-prosthesisiscurrentlyanexcellentchoice.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. FinnHA.Generalconsiderations.In:SimonMA,SpringfieldD, editors.Surgeryforboneandsofttissuetumors.Philadelphia: Lippincott-Raven;1998.p.609–13.
2.BritishOrthopaedicAssociationandtheBritishOrthopaedic OncologySociety.Metastaticbonedisease:aguidetogood practice;2001.
3.EilberFR,GrantTT,EckhardtJ,MortonDL.Prosthetic replacementaftersegmentalboneandjointresectionfor malignantbonetumors.In:ChaoEY,IvinsJC,editors.Tumor prosthesisforboneandjointreconstruction.NewYork: Thieme-Stratton;1983.p.321–7.
4.TeixeiraLEM,MirandaRH,GhediniDF,AguilarRB,Novais ENV,SilvaGMA,etal.Complicac¸õesprecocesnotratamento ortopédicodasmetástasesósseas.RevBrasOrtop.
2009;44(6):519–23.
5.CapannaR,CampanacciDA.Thetreatmentofmetastasesin theappendicularskeleton.JBoneJointSurgBr.
2001;83(4):471–81.
6.SilverbergE.Cancerstatistics.CACancerJClin. 1986;36(1):9–25.
7.WedinR,BauerHC.Surgicaltreatmentofskeletalmetastatic lesionsoftheproximalfemur:endoprosthesisor
reconstructionnail?JBoneJointSurgBr.2005;87(12): 1653–7.
8.AhlmannER,MenendezLR,KermaniC,GothaH.Survivorship andclinicaloutcomeofmodularendoprosthetic
reconstructionforneoplasticdiseaseofthelowerlimb.JBone JointSurgBr.2006;88(6):790–5.
9.KawaiA,MuschlerGF,LaneJM,OtisJC,HealeyJH.Prosthetic kneereplacementafterresectionofamalignanttumorofthe distalpartofthefemur.JBoneJointSurgAm.
1998;80(5):636–47.
10.MirelsH.Metastaticdiseaseinlongbones.Aproposed scoringsystemfordiagnosingimpendingpathologic fractures.ClinOrthopRelatRes.1989;(249):256–64. 11.SharmaS,TurcotteRE,IslerMH,WongC.Experiencewith
cementedlargesegmentendoprosthesesfortumors.Clin OrthopRelatRes.2007;459:54–9.
12.OrlicD,SmerdeljM,KolundzicR,BergovecM.Lowerlimb salvagesurgery:modularendoprosthesisinbonetumour treatment.IntOrthop.2006;30(6):458–64.
13.MalawerMM,ChouLB.Prostheticsurvivalandclinicalresults withuseoflarge-segmentreplacementsinthetreatmentof high-gradebonesarcomas.JBoneJointSurgAm.
1995;77(8):1154–65.
14.HealeyJH,BrownHK.Complicationsofbonemetastases: surgicalmanagement.Cancer.2000;8812Suppl.:2940–51. 15.TorbertJT,FoxEJ,HosalkarHS,OgilvieCM,LackmanRD.
Endoprostheticreconstructions:resultsoflong-termfollowup of139patients.ClinOrthopRelatRes.2005;438:51–9.
16.ParkDH,JaiswalPK,Al-HakimW,AstonWJ,PollockRC, SkinnerJA,etal.Theuseofmassiveendoprosthesesforthe treatmentofbonemetastases.Sarcoma.2007;2007:621–51. 17.Mendonc¸aSMH,CassoneAE,BrandaliseSR.Avaliac¸ão