www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
CASE
REPORT
Acute
urinary
retention
in
a
pre-school
girl
with
constipation
Guillermo
A.
Ariza
Traslavi˜
na
a,
Luiz
Antonio
Del
Ciampo
b,∗,
Ivan
Savioli
Ferraz
baHospitaldasClínicas,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),RibeirãoPreto,SP,Brazil bDepartmentofChildCareandPediatrics,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),
RibeirãoPreto,SP,Brazil
Received9December2014;accepted5March2015 Availableonline29August2015
KEYWORDS
Urinaryretention; Constipation; Child
Abstract
Objective: Toreportacaseofapreschoolgirlwhodevelopedacuteurinaryretentionassociated withconstipation.
Casedescription: Agirlagedsixyearsoldpresenteda24hhistoryofinabilitytourinate.She waswent twicetotheemergencyroomduringthisperiod.In thefirstadmission,12hafter theonsetofthesymptoms,shepresentedabdominalpainandacuteurinaryretention.After thedrainagebyurinarycatheterizationof300mLofclearurine,shepresentedreliefofthe symptomsand,asurinalysishadnochange,thepatientwasdischargedhome.Twelvehoursafter thefirstvisit,shereturnedtotheemergencyroomcomplainingaboutthesamesymptoms.At physicalexamination,therewasonlyapalpableanddistendedbladderuptotheumbilicuswith nootherabnormalities.Again,aurinarycatheterizationwasperformed,whichdrained450mL ofclearurine,with immediatereliefofthe symptoms.Urinalysis andurine culturehadno abnormalities.Duringtheanamnesis,thediagnosisofconstipationwasconsideredandaplain abdominalradiographywasperformed,whichidentifiedlargeamountoffecesthroughoutthe colon(fecalretention).Anenemawitha12%glycerinsolutionwasprescribedforthreedays. Duringfollow-up,thechildusedlaxativesanddietarymodifications,thiscontributedtothe resolutionoftheconstipation.Therewerenootherepisodesofurinaryretentionafter6months offollow-up.
Comments: Acuteurinaryretentioninchildrenisararephenomenonandconstipationshould beconsideredasacause.
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-license(https://creativecommons.org/licenses/by/4.0/).
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.03.007 ∗Correspondingauthor.
E-mail:[email protected](L.A.D.Ciampo).
PALAVRAS-CHAVE
Retenc¸ãourinária; Constipac¸ão intestinal; Crianc¸a
Retenc¸ãourináriaagudaempré-escolarfemininacomconstipac¸ãointestinal
Resumo
Objetivo: Relatar umcaso decrianc¸a quedesenvolveuretenc¸ãourinária agudaassociada à constipac¸ãointestinal.
Descric¸ãodocaso: Menina,6anosdeidade,há24horasapresentouincapacidadedeliberac¸ão deesfínctervesical.Foiatendidaporduasvezesemumservic¸odeemergêncianesseperíodo. Naprimeiraconsulta,12horasapósoiníciodoquadro,apresentavadorabdominaleretenc¸ão urináriaaguda,sendorealizadasondagemdealíviocomsaídade300mLdeurinaclara.Houve alívioimediatodossintomase,comooexame deurinatipo1nãoapresentou alterac¸ões,a pacienterecebeualta.Nosegundoatendimento,12horasapósaprimeiraconsulta, apresen-tavaasmesmasqueixas.Aoexamefísico,observou-seapenasbexigapalpáveledistendidaaté acicatrizumbilical,semoutrasalterac¸ões.Novasondagemvesicalfoirealizadacomsaídade 450mL deurinaclara, comalívioimediato dossintomas.Nenhumaanormalidadefoi obser-vadanoexame deurinatipo1eurocultura.Duranteaanamnese, foilevantadaahipótese diagnóstica de constipac¸ão intestinal, sendo realizada radiografia simples de abdome,que identificougrandequantidadedefezesemtodocólon(retenc¸ãofecal).Enemacomsoluc¸ão glicerinadaa12%foiprescritoportrêsdias.Duranteoseguimentoacrianc¸afezusode laxa-tivosemodificac¸õesnadietaquecontribuíramparaaresoluc¸ãodaconstipac¸ãointestinal,não havendorepetic¸ãodoquadroderetenc¸ãourináriaagudaapós6mesesdeacompanhamento. Comentários: A retenc¸ão urinária agudaem crianc¸as é um fenômeno raro ea constipac¸ão intestinaldeveserconsideradacomoumadascausas.
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Acuteurinaryretentionisdefinedastheincapacityto vol-untarilyurinate for more than12h, despite thepresence ofan intravesicalurinevolumehigherthan thatexpected for age [(age in years+2)×30mL]1 or the presence of a distendedbladderonphysicalexamination.Itisacommon symptomintheadultmalepopulation,mainlyduetobenign prostatichyperplasia,2 whereas itspresentation is rarein children, beingassociatedtoneurological diseases, infec-tions in the urinary tract and other sites, severe voiding dysfunction, side effects of some drugs (especially anti-cholinergics),tumors,anatomicalandemotionalproblems, as well as trauma.3---5 Although mentioned in some stud-ies,constipationdoesnotappearamongthemostcommon causes of acute urinary retention.3---5 Although the preva-lenceofintestinalconstipationinourpediatricpopulation is high,6 the report of its association with urinary reten-tioninthe Brazilianmedicalliteratureis rare.Therefore, theaimofthisarticle istopresentthecase ofa six-year-old child with acute urinary retention and constipation, aiming toexpand the possibilitiesfor differential diagno-sisandalertpediatriciansattheinitialevaluationofthese patients.
Case
report
A female child, aged six years old, born to non-consanguineousparents,withanectopicleftkidney(pelvic) andnormal kidney function,came for thesecond timeto theemergencydepartmentofa districthealthunitin the
RibeirãoPretocity(stateofSãoPaulo)showingirritability, generalizedabdominalpainofmoderateintensityand inca-pacitytoreleasethebladdersphincterfor 24h.According tothemother,thechildhadnopriorvoidingdisorderand didnotuseanymedication,havingbeentreated12hbefore atthesameemergencydepartmentwithsimilarcomplaints. Atthefirstconsultation,anincreaseinbladdervolumewas observedandurinarycatheterizationwasperformed, with 300mLoutputofclearurine,followedbyimmediate abdom-inalpainimprovement.Onthat occasion,aurinalysis test wasrequested,whichshowednoalterations,andthechild wasdischarged home. However,the symptoms had reap-pearedinthelast12handthechildwasonceagainbrought totheemergencydepartment.
At the second consultation, the child was afebrile, weighed 18kg, had a respiratory rate of 20 breaths per minute,heartrateof90beatsperminuteandblood pres-sureof 90/60mmHg, andwasbetweenthe 25thand50th percentilesforheight/ageindexbygender.Additionally,she presentedwithpainonpalpationofthelowerabdomenand shifting dullness in the hypogastric region,where a mass ofcysticconsistency waspalpable,compatiblewith blad-derdistention,whichreachedtheumbilicus.Therewereno alterationsin the vulvovaginal area.New bladder decom-pression was performed through catheterization, with a 450mLoutputofclearurine,followedonceagainbymarked painreliefaftertheprocedure.Urinesampleswereobtained for urine culture and urinalysis, which showed no alter-ations.
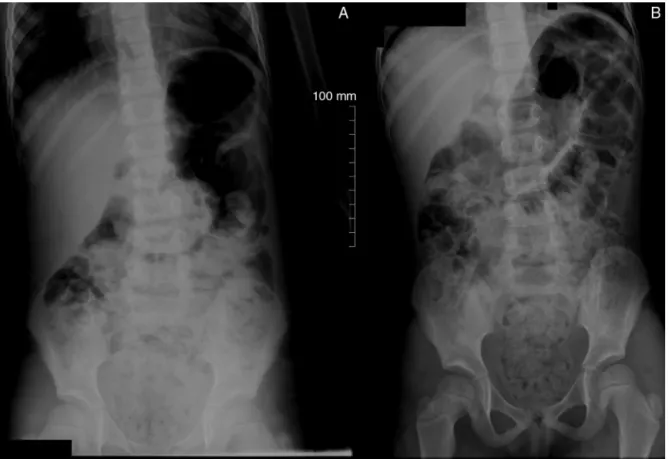
Figure1 AbdominalX-raysinthestanding(A)andsupine(B)position,disclosinglargeamountofstoolintheascendingand descendingcolon, sigmoid andrectum. Dilationinthe rectosigmoidsegment,secondary tothepresence ofstool, canalso be observed.
laxativeswithoutmedicaladvice;shehadreceiveda diag-nosisofintestinalconstipationtwoyearsbeforeinaPrimary CareCenter,butadherencetothedietaryguidelineswasnot adequate(there wasnomentionoflaxativeprescription). Consideringthesefacts, aplainabdominalradiographwas performedintheanteroposteriorview(AP)inthesupineand standingpositions(Fig.1),whichdisclosedimages compat-iblewiththe presenceof stool intherectum, cecumand alongthecolon,inadditiontofecalimpaction(retention) anddilationintherectalampulla.
Whilestillattheemergencydepartment,shewas submit-tedtofecaldisimpactionwitha12%glycerinenemasolution andthistreatmentwasmaintainedfor3consecutivedays. Mineraloil(1mL/kg/dayorally,dividedintotwodoses)was prescribedforcontinuoususeathome.Thechild’smother receivedrecommendations for modification of the child’s eating habits, aiming mainly at increasing the intake of waterandfiber-richfoods.Stoolsamplesforparasitological examinationwerealsorequested.
The child returned for consultation at the outpatient clinicofthePrimaryCareCentereightdaysaftersymptom onset,beingingoodhealthstatus,withoutabdominalpain, maintainingadequatediuresisandshowingnorelevant find-ings onphysical examination. At this time,the results of urinecultureandparasitologicaltestswereverified,which werenegative.
Duringasix-monthfollowup,thechilddidnothavenew episodesofacuteurinaryretention.Shewasregularly fol-lowed at the Primary Care Center, showing improvement
in the eating habits (increased fiber and water intake) andevacuatingtwicedailywithoutdifficulty,withsoftand thinnerstools.Consideringtheimprovementofthechild’s constipation, the use of mineral oil was suspended after threemonths.
Discussion
Acute urinary retention is a relatively uncommon phe-nomenoninchildren.Wereportonacaseofacuteurinary retentioninasix-year-oldfemalechildwho,concomitantly, hadchronicconstipationandapelvickidneytotheleft.
Despite the high prevalence of chronic constipation in children,acuteurinaryretention episodesassociatedwith thismorbidityarerarelymentionedintheinternationaland Brazilian medicalliterature. In asurvey carriedout inan Americanhospitalfrom1993to2000,53patientsagedsix monthsto17yearsoldwereidentified.
threeIranianhospitalsfrom1996to2003,theauthorsfound 86childrenagedupto14yearswithacuteurinaryretention, ofwhichmaincauseswerelowerurinarytractstones(28%), neurologicaldisorders(10%)andlocaltrauma(10%). Consti-pation showedtobeanuncommon cause,beingobserved in only 5% of patients.4 In both abovementioned surveys, individualsintheimmediatepostoperativeperiodusing opi-oids,thosewithmentalretardationandchronicneurological disorders, and immobile ones were excluded. In a more recent survey, carried out in a tertiary hospital in Israel, 56patientsyoungerthan18yearstreatedforacuteurinary retentionbetweentheyears2000and2012werefound.In thesepatients, themost commoncauses of acuteurinary retentionwere:mechanicalobstruction(25%),infectiousor inflammatory processes(18%) and fecalimpaction (13%).5 Inthelatterstudy,inadditiontonewborns, allindividuals intheimmediatepostoperativeperiod,thosesubmittedto urethralprocedures andthosewithneurological disorders were excluded. In a Brazilian study performed with 163 childrenwithchronicfunctionalconstipationfollowedina pediatricgastroenterology clinicinBotucatucity (stateof SãoPaulo),therewasaprevalenceof8.6%ofurinary reten-tionasacomplicationofthebaselinemedicalcondition.It isnoteworthythatinthelatterstudy,43.4%ofthechildren hadoneormoreurinaryalterations(enuresis,infectionsand urinaryretentionoutbreaks)associatedwithconstipation.7 Regardingthepatientdescribedinthiscasereport,the onlyalterationfoundwasthelargeamountofstoolobserved intheplainabdominalradiography.Thisexamination---when performedin theAPview,inthesupineandstanding pos-itions,andeventhough itdoesnotestablishthediagnosis of constipation ---, allows,assessing the presence of fecal retentionandpossibleabdominalorpelvicmassesoreven calcificationsintheurinarytractthatcouldhelpexplainthe acuteurinaryretention.Symptomdisappearancewithbowel habitimprovementanddecreasedstoolconsistencyindicate thatchronicconstipationwasthecauseoftheacuteurinary retentioninthispatient.Thischildhadaonce-dailybowel habitwithhard,dryandthickstoolsforatleastthreeyears andwasundergoinganirregularfollow-upataPrimaryCare Centerwithadiagnosisof constipationfortwoyears.The motherhadreceiveddietaryrecommendationstoincrease the child’s intake of fiber and water, and she occasion-allygavethechildlaxatives.Thedelay inseekingmedical care,poor adherencetothetreatment planand prescrip-tion of inadequate treatments are commonly reportedin the literature regarding constipation.8,9 The low morbid-ityoftheinitialpictureofconstipation,lackofknowledge regarding the children’s normal pattern of evacuation by their parents, lack of an individualized nutritional plan andthe prescription of unpalatable laxativesmay explain poortreatment adherence.8,10---12 Theabsenceofacorrect approachtothetreatmentofconstipationcanleadto dis-ease complications, as described in the child in our case report.8
The association of constipation with urinary disor-ders is well established in the medical literature.13,14 In the pediatric population, several studies have shown a strong association betweenconstipation andthepresence of urinary disorders, such as incontinence and urinary urgency15,16;additionally,largervolumesofpost-micturition residual urine and urinary tract dilation, including the
ureteropelvic tract, have been most commonly observed inconstipated children.17,18 Thus, acuteurinary retention probably constitutes one of the clinical presentations of incompleteemptyingof thebladder inchildren with con-stipation.The physiopathologyoftheassociation between constipation and voiding disorders could be explained by severalfactors.The bladderandtherectumsharea close embryologicalassociation (cloaca) during the pelvic floor formation,sharingthesameinnervation,nerverootsS2to S4,whichcontrolmotorfunctionoftheinternalanaland uri-narysphincters.13,18Experimentswithratsfoundthatrectal distentionwithaballoondiminishedbladdercontractility.19 Chronicretentioncouldalsoleadtoinvoluntarycontraction ofthepelvicfloormusclesandtheexternalanalsphincter, makingbladderemptyingdifficult.14,18Additionally, consid-ering the close anatomical association, the presence of impacted stool in the rectum reduces bladder functional capacity,resultinginafeelingofearlierbladderemptying.14 Moreover,achronicallyfullrectalampullacanleadto vesi-caltrigoneirritation,invaginationsintheposteriorwallof thebladderandurethralobstruction.20
Thechildwhosecasewasreportedinthispaperhadan ectopickidney to the left.The literature has shown few reports of acute urinary retention episodes in individuals withgenitourinarytractdeformities,suchasmalformations ofthefemale(didelphicuterusandimperforatehymen)21,22 and male genital tracts (seminal vesicle cyst)23 associ-atedwithunilateralrenalagenesis; however,thereareno reportedcasesinvolvingapictureofacuteurinaryretention withectopickidney.Intheauthors’opinion, thepatient’s ectopickidneydescribedheredidnotcontributeinanyway totheacuteurinaryretention.
It can be concluded that acute urinary retention is a rareeventinthepediatricagegroup.Therefore,although it is not oneof the most common causes, intestinal con-stipation,givenitshigh prevalence, shouldbe considered whentreatingchildrenandadolescentswithacuteurinary retention.
Funding
Thisstudydidnotreceivefunding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Koff SA. Estimating bladder capacity in children. Urology. 1983;21:248.
2.Sarma AV, WeiJT. Clinical practice. Benign prostatic hyper-plasia and lower urinary tract symptoms. N Engl J Med. 2012;367:248---57.
3.GattiJM,Perez-BrayfieldM,KirschAJ,SmithEA,MassadHC, Broecker BH. Acute urinary retention in children. J Urol. 2001;165:918---21.
5.NevoA,ManoR,LivnePM,SivanB,Ben-MeirD.Urinaryretention inchildren.Urology.2014;84:1475---9.
6.Del Ciampo IR, Galvão LC, Del Ciampo LA, Fernandes MI. Prevalência de constipac¸ão intestinal crônica em crianc¸as atendidas em unidade básica de saúde. J Pediatr (Rio J). 2002;78:497---502.
7.Maffei HV, Moreira FL, Kissimoto M, Chaves SM, El Faro S, Aleixo AM. História clínica e alimentar de crianc¸as atendi-dasemambulatóriodegastroenterologiapediátrica(GEP)com constipac¸ãointestinalcrônicafuncional(CICF)esuaspossíveis complicac¸ões.JPediatr(RioJ).1994;70:280---6.
8.InabaMK,PéretFilhoLA,CostaValA, PennaFJ. Prevalência ecaracterísticasclínicasdascrianc¸ascomconstipac¸ão intesti-nalcrônicaatendidasemclínicadegastroenterologia.Pediatria (SãoPaulo).2003;25:157---63.
9.Morais MB, Tahan S. Constipac¸ão Intestinal. Pediatr Mod. 2009;45:79---98.
10.Del Ciampo IR, Del Ciampo LA, Galvão LC, Fernandez MI. Constipac¸ão intestinal: um termo desconhecido e dis-túrbio frequentemente não reconhecido. Rev Paul Pediatr. 2006;24:111---4.
11.GomesPB,Duarte MA,MeloMC. Comparac¸ãodaefetividade entrepolietilenoglicol4000semeletrólitosehidróxidode mag-nésionotratamentodaconstipac¸ãointestinalcrônicafuncional emcrianc¸as.JPediatr(RioJ).2011;87:24---8.
12.Karagiozoglou-LampoudiT,DaskalouE,AgakidisC,SavvidouA, ApostolouA, VlahavasG. Personalizeddiet management can optimizecompliance to a high-fiber, high-waterdiet in chil-drenwithrefractoryfunctionalconstipation.JAcadNutrDiet. 2012;112:725---9.
13.BallekNK,McKennaPH.Lowerurinarytractdysfunctionin child-hood.UrolClinNAm.2010;37:215---28.
14.HalachmiS,FarhatWA.Theimpactofconstipationonthe uri-narytractsystem.IntJAdolescMedHealth.2008;20:17---22.
15.SureshkumarP,JonesM,CummingR,CraigJ.Apopulationbased studyof2856school-agechildrenwithurinaryincontinence.J Urol.2009;181:808---15.
16.VazGT,VasconcelosMM,OliveiraEA,FerreiraAL,MagalhãesPG, SilvaFM,etal.Prevalenceoflowerurinarytractsymptomsin school-agechildren.PediatrNephrol.2012;27:597---603.
17.Dohil R, Roberts E, Jones KV, Jenkins HR. Constipation and reversible urinary tract abnormalities. Arch Dis Child. 1994;70:56---7.
18.ChangSJ,HsiehCH, YangSS.Constipationisassociatedwith incomplete bladder emptyingin healthy children. Neurourol Urodyn.2012;31:105---8.
19.MiyazatoM, SugayaK, NishijimaS, MorozumiM, OhyamaC, OgawaY.Rectaldistentioninhibitsthespinalmicturitionreflex viaglycinergicorGABAergicmechanismsinratswithspinalcord injury.UrolInt.2005;74:160---5.
20.Chase JW,Homsy Y, SiggaardC,Sit F,BowerWF. Functional constipationinchildren.JUrol.2004;171:2641---3.
21.BrosetaE,BoronatF,DomínguezC,AlonsoM,RuizJL.Acute urinary retention caused by hematocolpos associated with uterusdidelphysandipsilateralrenalagenesis.ArchEspUrol. 1989;42:885---8.
22.BenítezNavioJ,CasanuevaLuisT,LagunaUrracaG,Gallardo GalánC,GarcíaVelascoS.Righthematocolposand hematome-trawithleftrenalagenesis.Arareassociation.Aproposacase. ArchEspUrol.1993;46:824---7.