w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Metabolic
syndrome
in
patients
with
rheumatoid
arthritis
followed
at
a
University
Hospital
in
Northeastern
Brazil
Brenda
Maria
Gurgel
Barreto
de
Oliveira
a,
Marta
Maria
das
Chagas
Medeiros
b,∗,
João
Victor
Medeiros
de
Cerqueira
c,
Raquel
Telles
de
Souza
Quixadá
a,
Ídila
Mont’Alverne
Xavier
de
Oliveira
aaHospitalUniversitárioWalterCantídio(HUWC),UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil bMedicineSchool,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
cMedicalCourse,UniversidadedeFortaleza(UNIFOR),Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29January2014 Accepted29May2015
Availableonline12September2015
Keywords:
Metabolicsyndrome Rheumatoidarthritis Cardiovasculardiseases
a
b
s
t
r
a
c
t
Introduction:Patientswithrheumatoidarthritis(RA)are30–60%morelikelytodevelop car-diovasculardisease(CV)thanthegeneralpopulation.Metabolicsyndrome(MS),definedby anumberofcardiovascularriskfactors,confersagreaterriskofCVdiseaseanddiabetes. TheassociationofMSwithRAisnotyetfullyunderstoodanditsprevalencevariesfrom19 to63%acrossstudies.
Objectives: ToassesstheprevalenceofMSinapopulationofRApatientsfollowedina hos-pitalinNortheasternBrazilandanalyzeassociationsofdemographicandclinicalfactors withMS.
Methods:OutpatientswithRAwereevaluatedinacross-sectionalstudyregarding demo-graphic,clinical,laboratoryandanthropometricdata.ThecriteriafordefiningMSwerethose adoptedbyNCEPIII(2005)andIDF(2006).
Results:110patientswithRAwerestudied;97.3%werefemale,withameanageof55.5 years(SD=12.9)anddurationofillnessof11.2years(SD=7.3).TheMSprevalencefrom NCEPIII(2005)andIDF(2005)were,respectively,50%and53.4%.Advancedage(57.9±11.9
versus52.9±13.5;p=0.04)andsmokingload>20packs/year(29%versus9%,p=0.008)were associatedwithMS.Themajorcomponentsofthemetabolicsyndromewereabdominal obesity(98.1%),hypertension(80%)andlowHDLcholesterol(72.2%).
Conclusions: RApatientsinatertiarycenterinNortheasternBrazilshowedhighprevalence ofMS.ItisworthnotingthatalmostallpatientshadMSandabdominalobesity,whichhas importantpracticalimplications.InadditiontothecomponentsofMS,ageandsmoking wereassociatedwiththissyndrome.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](M.M.C.Medeiros).
http://dx.doi.org/10.1016/j.rbre.2015.08.016
Síndrome
metabólica
em
pacientes
com
diagnóstico
de
artrite
reumatoide
acompanhados
em
um
Hospital
Universitário
do
Nordeste
brasileiro
Palavras-chave:
Síndromemetabólica Artritereumatoide Doenc¸ascardiovasculares
r
e
s
u
m
o
Introduc¸ão:Pacientescomartritereumatoide(AR)têm30a60%maischancesdedesenvolver doenc¸ascardiovasculares(DCV)doquea populac¸ãogeral.Asíndromemetabólica(SM), definidaporumconjuntodefatoresderiscocardiovasculares,conferemaiorriscodeDCVe diabete.Aassociac¸ãodaSMcomARaindanãoestátotalmenteesclarecidaesuaprevalência variade19a63%entreosestudos.
Objetivos: AvaliaraprevalênciadeSMnumapopulac¸ãodepacientescomARacompanhada numhospitaldoNordestebrasileiroeanalisarassociac¸õesdefatoresdemográficoseclínicos comSM.
Métodos: PacientesambulatoriaiscomARforamtransversalmenteavaliadoscomrelac¸ãoa dadosdemográficos,clínicos,laboratoriaiseantropométricos.OscritériosparadefinirSM foramosadotadospeloNCEPIII(2005)eIDF(2006).
Resultados:Foramestudados110pacientescomAR,97,3%mulherescommédiade55,5anos (DP=12,9)edurac¸ãodadoenc¸ade11,2anos(DP=7,3).AsprevalênciasdeSMdoNCEPIII (2005)eIDF(2005)foram,respectivamente,50%e53,4%.Idadeavanc¸ada(57,9±11,9 ver-sus52,9±13,5;p=0,04)ecargatabágica>20mac¸osano(29%versus9%;p=0,008)estiveram associadascomSM.OsprincipaiscomponentesdaSMforamobesidadeabdominal(98,1%), hipertensãoarterial(80%)eHDLbaixo(72,2%).
Conclusões: PacientescomARdeumservic¸oterciáriodoNordestebrasileiroapresentaram altaprevalênciadeSM.Chamaatenc¸ãoaquasetotalidadedospacientescomSMeobesidade abdominal,oquetrazimplicac¸õespráticasimportantes.AlémdoscomponentesdeSM, idadeetabagismosemostraremassociadoscomSM.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Rheumatoidarthritis(RA)isasystemicinflammatory, autoim-mune,chronicdiseasewhichmainlyaffectsperipheraljoints. Recent epidemiological studies have suggested that RA is anindependentriskfactorforcardiovascular(CV)diseases, andRApatientsare30–60%morelikelytodevelop(CV) dis-eases, that are characterizedas the most importantcause of morbidity and mortality in patients with RA.1,2 The mostlikelyexplanation forthis isthe process of endothe-lial dysfunction and accelerated atherosclerosis that occur in these patients secondary to chronic inflammation and also to a higher prevalence of traditional cardiovascular riskfactors.Thepresenceofmetabolicsyndrome(MS),also knownasinsulinresistancesyndrome,characterizedbythe combination of cardiovascular risk factors such as hyper-tension, obesity, high blood glucose, insulin resistance(IR) and dyslipidemia,confers agreater cardiovascular morbid-itythanthesumoftherisksassociatedwitheachindividual component.3
Its etiology remains elusive, but studies point to IR as the main mediator in the pathophysiology of MS. Multi-plemetabolic pathwayshave been proposed toconnect IR andcompensatoryhyperinsulinemiatoothermetabolicrisk factors.4,5 Although the role of MS as a predictor of car-diovascularriskhasbeen hotlydebated,ameta-analysisof
2010involvingmorethan950,000patientsconcludedthatMS increasestwicetheriskof(CV)diseasesand1.5timesthe over-all mortality,aswellasanincreaseoffivetimesforriskof occurrenceoftype2diabetesmellitus.6MSandIRhavealso beenassociatedwithseveralotherdiseases,suchashepatic steatosis,fibrosisandcirrhosis,7polycysticovarysyndrome,8 cholelithiasis,9sleepapnea,10 chronickidney disease,11 and gout.12
Themainaimofthisstudy wastodeterminethe preva-lence of MS in a population ofRA patients followed in a university hospital in Northeastern Brazil, and to analyze associationsofdemographicandclinicalfactorswiththe pres-enceofMS.
Patients
and
methods
Patients diagnosed with RA according to the 1988 ACR criteria31andfollowedattheRheumatologyCenteroutpatient clinic, HospitalUniversitário Walter Cantídio, Universidade FederaldoCeará,weresequentiallyinvitedtoparticipatein thisstudy.Patientswithotherautoimmunediseases,except secondary Sjogren’s syndrome, were excluded. The study beganinJanuary2013andendedinDecember2013andthe data collection was made witha cross-sectional design in thesameperiod.Atotalof110patientswasstudied. Demo-graphic(gender,age,race,educationlevel)andclinicaldata relatedtoRA(diseasedurationsincediagnosis,thepresence of extra-articular manifestations, rheumatoid factor, cyclic citrullinatedpeptideantibody[anti-CCP],medicationsused, boneerosions)andthepresenceofcardiovascularriskfactors (hypertension,diabetesmellitus,dyslipidemia,heartdisease, smoking)werecollectedfromclinicalrecords.Giventhatdata onsmoking are often notrecorded properly inthe clinical records,informationaboutsmokingwasdirectlyaskedforthe patientattheassessmentday:neversmoked,smokedinthe past,currentlysmoking,numberofcigarettes/dayand smok-ingtime.Thepatientwasconsideredasasmokerifhe/she hadsmokedorstillwassmokingforatleast6monthsany numberofcigarettes.Pack-yearsofsmokingwascalculatedas theaveragenumberofcigarettesperdaymultipliedbyyears asasmoker,dividedby20.Ahistoryof>20packs/yearwas consideredasheavysmoking.32Informationaboutdoseand durationofprednisoneusealsoweretakenfromtherecords andcategorizedasfollows:no/verylowexposure:dailyuse ofprednisone<7.5mgduring<3months;lowexposure:daily useofprednisone<7.5mgduring>6months;medium expo-sure:dailyuseofprednisone≥7,5–30mgupfor>6months. Patients without any regular physical activity,or who per-formedsporadicphysicalactivity(<150minofactivity/week), wereclassifiedashavingasedentarylifestyle.
Duringthephysicalexamination,thenumberofswollen andtenderjointswasdetermined(28joints)andpatientswere evaluatedforthepresenceofjointdeformities(reversibleor irreversible).Measurementsofbloodpressure,weight,height andwaistcircumferenceweredeterminedintheassessment day.Waistcircumferencewasmeasuredincentimeterswith atape atthe midpoint between the lower part ofthe last ribandtheiliaccrest.BodyMassIndex(BMI)wascalculated usingtheformulaweightoverheightsquared.Disease activ-itywasmeasuredbytheinstrumentDiseaseActivityScore28 (DAS28)33alsointhestudyvisitday,alwaysusingthelastESR obtained.FunctionalcapacitywasassessedusingtheHealth AssessmentQuestionnaire(HAQ),34withscoresfrom0to3: 0meaningnolossofphysicalfunction,and3meaning com-pletephysicaldisability.Recentlaboratorydata(bloodcount, erythrocytesedimentationrate[ESR],C-reactiveprotein[CRP], fasting glucose, total cholesterol, high density lipoprotein
[HDL]cholesterol,triglycerides,creatinineandurea)werealso assessed.
MS
criteria
TherearefivedefinitionsforMS,allincludingdosagesofHDL cholesterol,triglycerides,fastingglucoseandbloodpressure, and waistcircumference measurement; and threeofthese includecriteriaforIR.Thesedefinitionsalsodifferwithrespect tocutoffpointsinbloodglucose,HDL,triglyceridesandblood pressurelevelsandabdominalcircumferencemeasurement. The mostwidelyused definitionsare the AdultTreatment PanelIIIoftheNationalCholesterolEducationProgram(NCEP ATPIII)35 andthe InternationalDiabetesFederation (IDF)36; therefore,weusedthesetwodefinitionsupdatedin2005and 2006,respectively,tocalculateonlytheprevalence.To com-paredemographicandclinicalfactorsbetweenthegroupof patientswithRAandMSversuspatientswithRA,butwithout MS,weusedtheMSratecalculatedbyNCEPATPIII.
The NCEP ATP III (2005) criteria requires three out of five factors to establish the diagnosis as follows: fasting glucose ≥100mg/dL or use of hypoglycemic agents; HDL <40mg/dL(men)or<50mg/dL(women)oruseofLDLlowering drugs;triglycerides≥150mg/dLoruseoftriglyceride-lowering medications;waistcircumference≥102cm(men)or≥88cm (women);andbloodpressure≥130/85mmHgoruseof antihy-pertensivedrugs.ThecriteriatoconsiderMSaccordingtoIDF are:mandatorypresenceofabdominalcircumference≥94cm (men)or≥80cm(women)andatleasttwooftheotherfour criteriadescribedabove.
Statistical analysis was performed using Stata software version9.0.Fordescriptiveanalysisofgeneralcharacteristics ofthesample,proportionsandmeans±standarddeviations (SD)were calculated.Student’st testforindependent sam-pleswas usedtocomparemeans betweengroups,and the chi-squared test was applied to compare proportions. The levelofstatisticalsignificancesetat5%(p<0.05)wasusedfor allstatisticaltests.ThestudywasapprovedbytheResearch Ethics CommitteeoftheHospitalUniversitárioWalter Can-tídio(HUWC) –Universidade FederaldoCeará(Protocol.N. 086.08.11).
Results
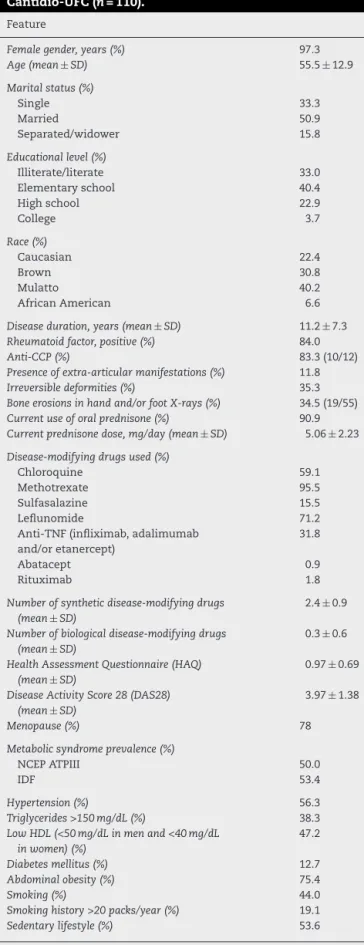
Table1–Characteristicsofpatientswithrheumatoid arthritisfollowedattheHospitalUniversitárioWalter Cantidio-UFC(n=110).
Feature
Femalegender,years(%) 97.3
Age(mean±SD) 55.5±12.9
Maritalstatus(%)
Single 33.3
Married 50.9
Separated/widower 15.8
Educationallevel(%)
Illiterate/literate 33.0
Elementaryschool 40.4
Highschool 22.9
College 3.7
Race(%)
Caucasian 22.4
Brown 30.8
Mulatto 40.2
AfricanAmerican 6.6
Diseaseduration,years(mean±SD) 11.2±7.3
Rheumatoidfactor,positive(%) 84.0
Anti-CCP(%) 83.3(10/12)
Presenceofextra-articularmanifestations(%) 11.8
Irreversibledeformities(%) 35.3
Boneerosionsinhandand/orfootX-rays(%) 34.5(19/55)
Currentuseoforalprednisone(%) 90.9
Currentprednisonedose,mg/day(mean±SD) 5.06±2.23
Disease-modifyingdrugsused(%)
Chloroquine 59.1
Methotrexate 95.5
Sulfasalazine 15.5
Leflunomide 71.2
Anti-TNF(infliximab,adalimumab and/oretanercept)
31.8
Abatacept 0.9
Rituximab 1.8
Numberofsyntheticdisease-modifyingdrugs (mean±SD)
2.4±0.9
Numberofbiologicaldisease-modifyingdrugs (mean±SD)
0.3±0.6
HealthAssessmentQuestionnaire(HAQ) (mean±SD)
0.97±0.69
DiseaseActivityScore28(DAS28) (mean±SD)
3.97±1.38
Menopause(%) 78
Metabolicsyndromeprevalence(%)
NCEPATPIII 50.0
IDF 53.4
Hypertension(%) 56.3
Triglycerides>150mg/dL(%) 38.3
LowHDL(<50mg/dLinmenand<40mg/dL inwomen)(%)
47.2
Diabetesmellitus(%) 12.7
Abdominalobesity(%) 75.4
Smoking(%) 44.0
Smokinghistory>20packs/year(%) 19.1
Sedentarylifestyle(%) 53.6
NCEP ATPIII 2005, Adult Treatment Panel III of the National CholesterolEducationProgram;IDF 2005,InternationalDiabetes Federation.
assessedbyDAS28atthetimeofevaluationwas3.97±1.38, andfunctionalcapacityassessedbyHAQwas0.97±0.69.
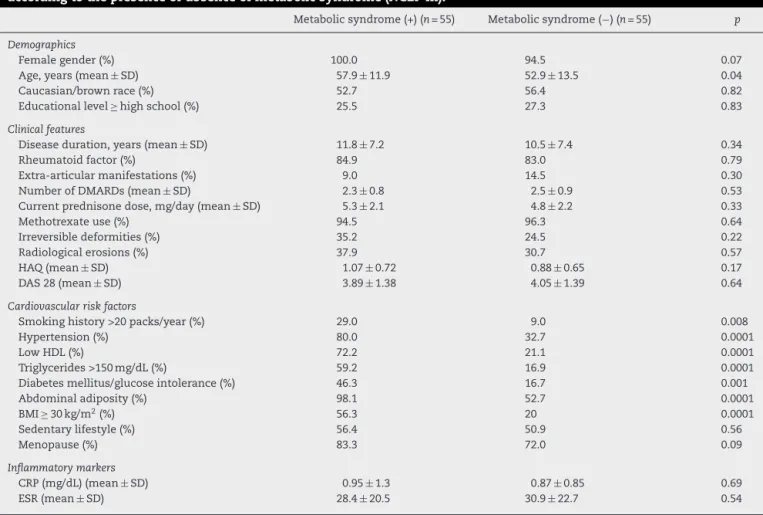
Theprevalence ofMSwas 50% and 53.4%byNCEP ATP IIIandIDFdefinitions,respectively.Whendemographicand clinicalcharacteristicsofpatientswithandwithoutMSwere compared(accordingtoNCEPATPIII),onlyageshowed sta-tistically significant difference, with older subjects in MS group (57.9 versus 52.9 years; p=0.04). Cardiovascular risk factors (hypertension, low HDL, high triglycerides, glucose intolerance or diabetesmellitus, abdominaladiposity, obe-sity, smoking history >20 packs/year) were more frequent inpatientswithMS.There wasnostatisticaldifferencefor inflammatorymarkers(Table2).Norelationshipwasfound between exposure to oral prednisone and presence of MS (Table3).
The most frequent components of MS definition were abdominal adiposity (98.1%), hypertension (80%) and low HDL (72.2%). Hypertriglyceridemia and glucose intoler-ance/diabetes mellitus were present in 59.2% and 46.3%, respectively(Table4).
Discussion
Although several studies on prevalence of MS in RA have already been performed worldwide, the frequency found varies from 14 to 63% among the various populations studied, not always the values found are higher than in controls, and the associationoffactors related to rheuma-toidarthritis(diseaseactivity,inflammatorymarkers,severity of the disease, treatment) with MS varies greatly in the literature.14–16,18,23–27,29Afrequentexplanationforthese dis-crepanciesistheuseofdifferentcriteriaforMSclassification. However,evenwhenobserving studiesthat usedthe same criteria,theprevalenceratesvarywidely(Table5).Therefore,it islikelythatotherfactorsrelatedtothecharacteristicsofthe study population,includinggenetic,ethnic,cultural, demo-graphic, socioeconomic and clinical factors, also influence theprevalencerates.Thus,studiesconductedwithdifferent populations are critical to try todetect other factors more associatedwithMSspecificofthatpopulationand,fromthis point,onecouldtrytointerfereonsuchfactors,inadditionto offeringinformationtoabetterunderstandingofthe patho-physiologicalrelationshipbetweenthedifferentcomponents andothercardiovascularriskfactors.
Table2–CharacteristicsofrheumatoidarthritispatientsfollowedattheHospitalUniversitárioWalterCantídio-UFC accordingtothepresenceorabsenceofmetabolicsyndrome(NCEPIII).
Metabolicsyndrome(+)(n=55) Metabolicsyndrome(−)(n=55) p
Demographics
Femalegender(%) 100.0 94.5 0.07
Age,years(mean±SD) 57.9±11.9 52.9±13.5 0.04
Caucasian/brownrace(%) 52.7 56.4 0.82
Educationallevel≥highschool(%) 25.5 27.3 0.83
Clinicalfeatures
Diseaseduration,years(mean±SD) 11.8±7.2 10.5±7.4 0.34
Rheumatoidfactor(%) 84.9 83.0 0.79
Extra-articularmanifestations(%) 9.0 14.5 0.30
NumberofDMARDs(mean±SD) 2.3±0.8 2.5±0.9 0.53
Currentprednisonedose,mg/day(mean±SD) 5.3±2.1 4.8±2.2 0.33
Methotrexateuse(%) 94.5 96.3 0.64
Irreversibledeformities(%) 35.2 24.5 0.22
Radiologicalerosions(%) 37.9 30.7 0.57
HAQ(mean±SD) 1.07±0.72 0.88±0.65 0.17
DAS28(mean±SD) 3.89±1.38 4.05±1.39 0.64
Cardiovascularriskfactors
Smokinghistory>20packs/year(%) 29.0 9.0 0.008
Hypertension(%) 80.0 32.7 0.0001
LowHDL(%) 72.2 21.1 0.0001
Triglycerides>150mg/dL(%) 59.2 16.9 0.0001
Diabetesmellitus/glucoseintolerance(%) 46.3 16.7 0.001
Abdominaladiposity(%) 98.1 52.7 0.0001
BMI≥30kg/m2(%) 56.3 20 0.0001
Sedentarylifestyle(%) 56.4 50.9 0.56
Menopause(%) 83.3 72.0 0.09
Inflammatorymarkers
CRP(mg/dL)(mean±SD) 0.95±1.3 0.87±0.85 0.69
ESR(mean±SD) 28.4±20.5 30.9±22.7 0.54
DMARDs,disease-modifyingantirheumaticdrugs;BMI,bodymassindex;HAQ,HealthAssessmentQuestionnaire;DAS28,DiseaseActivity Score;ESR,erythrocytesedimentationrate.
almostalwaysalittlehigherthan2005NCEPIII’s.Withrespect todemographicandclinicalfactors,onlyolderagewas asso-ciatedwithMSinthisstudy.Wefoundnoassociationwith diseaseduration,useofglucocorticoids,functionalcapacity anddiseaseactivity.Whatdrewalotofattentionwasthehigh prevalenceofabdominalobesityinpatientswithMS(98.1%) andtheassociationbetweenheavysmokingstoryandMS.
TheprevalenceofMSinourstudy hasbeenamongthe largesteverrecordedinallstudies(Table5).Comparingonly studies using the definition of NCEPIII, MS prevalence in RA among various international populations ranged from 19%to55.5%.Also,consideringonlystudiesthatincludeda
Table3–Exposuretooralcorticosteroids(prednisone)in rheumatoidarthritispatientswithmetabolicsyndrome (NCEPIII)andwithoutmetabolicsyndromefollowedat theHospitalUniversitárioWalterCantídio-UFC.
Corticosteroiddose Patientswith metabolic syndrome(n/%)
Patientswithout metabolic syndrome(n/%)
Notexposed,orvery lowexposure
4(7.27%) 7(12.96%)
Lowexposure 44(80%) 42(77.78%)
Mediumexposure 7(12.73%) 5(9.26%)
controlgroup,somedidnotfindarelationshipbetweenMS and RA,14,15,20,24 othershavefoundincreasedMS,16,22,25,26,28 and two studies showed higher rates in controls than in patientswithRA.21,29ThestudybyLaMontagnaetal.,15 con-ducted atthe University ofNaples, Italy, with 45 patients and48controls(patientswithmyofascialpain,carpaltunnel syndromeandshoulderperiarthritis),foundaMSrateinRA similartoours(55.5%).LaMontagna’spatientshadclinicaland demographiccharacteristicssimilartothoseofourpatients withregardtoage,diseaseduration,genderandcurrentdose of glucocorticoids. However,they alsofound a high preva-lenceofMSincontrols(45.8%),withnostatisticaldifference betweenthetwogroups.Althoughourstudylackedacontrol
Table4–Metabolicsyndrome(NCEPIII)
parameterspresentinpatientswithrheumatoidarthritis followedattheHospitalUniversitárioWalter
Cantídio-UFC.
Metabolicsyndromecomponent Percentage(%)
Hypertension 80.0
Abdominaladiposity 98.1
LowHDL 72.2
Hightriglycerides 59.2
Table5–Prevalenceofmetabolicsyndromeinpatientswithrheumatoidarthritisaccordingtoseveralstudies.
Author,year Studydesign Numberof
patientswith RA/controls
Age,years (mean±SDor
median,IQR)
Disease duration,years
(mean±SDor median,IQR)
Prevalenceof metabolic syndromein
RA(%)
Deisseinetal.,2006 Cross-sectional 74 55.8(53.2–58.3) 12.8(12.3–15.2) 19%(NCEPIII
2005) 14%(WHO)
Karvounarisetal.,2007 Case–control 200/400 63±11 9.3±8.8 44%(NCEPIII
2001)
LaMontagnaetal.,2007 Case–control 45/48 53.8±11.6 12.6±8.2 55.5%(NCEPIII
2005)
Chungetal.,2008 Case–control 154/85 59(52–67) 20(14–24) 42%(NCEPIII
2001) 42%(WHO)
Zonana-Nacachetal.,2008 Cross-sectional 107 48±12 11.2±9.3 18.7%(NCEPIII
2001)
Tomsetal.,2009 Cross-sectional 400 63.0(55.4–69.2) 10(4–18) 40.1%(NCEPIII
2005) 45.3%(IDF) 19.4%(WHO)
Elkanetal.,2009 Cross-sectional 80 61.4±12 6(2–15) 20%(women)
(IDF)
63%(men)(IDF)
Gilesetal.,2010 Case–control 131/121 61±9 9(5–17) 36%(NCEPIII
2005)
Sahebarietal.,2011 Case–control 120/500 45.5±13 5.5±5.2 30.8%(IDF)
45.2%(NCEPIII 2001)
Crowsonetal.,2011 Case–control 232/1241 58.8±12.8 7(4.1–12.8) 33%(NCEPIII
2005)
Moketal.,2011 Cross-sectional 699 53.3±12 5.3±5.4 20%(NCEPIII
2005)
Karimietal.,2011 Case–control 92/96 48.3±14.6 8(5–14) 27.2%(NCEPIII
2001) 19.6%(WHO)
DaCunhaetal.,2012 Case–control 283/226 56.8±12.3 11.1(4.9–16) 39%(NCEPIII
2005)
Karakocetal.,2012 Case–control 54/52 49.7±11.1 7.6 42.6%(NCEPIII
2005)
Leeetal.,2013 Case–control 84/109 50.6±11.3 3.5(2.0–6.3) 19%(NCEPIII
2005)
Rostometal.,2013 Case–control 120/100 49±12 7.8 32.4%(NCEPIII
2005) 48.6%(IDF) 20%(WHO)
Salinasetal.,2013 Case–control 409/624 55.5±13.2 8(4–15) 30%(NCEPIII
2005) 35%(IDF)
Medeirosetal.,2014a Cross-sectional 110 57.9±11.9 11.8±7.2 50%(NCEPIII
2005) 53.4%(IDF)
IQR,interquartilerange. a Currentstudy.
group,asystematicreviewrecentlypublished(2013)onthe prevalenceofMSintheBrazilianadultpopulationincluded 10studiesconductedinseveralBrazilianregions,showinga mean rateof29.6% forMS.37 Theonlystudy conductedin NortheasternBrazilwasinarandompopulation-based sam-plethatconsistedof240subjectsaged25–87yearsinatown ofthesemi-aridregionofBahia,whereanage-adjustedrate of24.8%wasfoundwiththeuseofNCEPIII2001definitions (cutoffpointforglucose >110mg/dL,rather than100mg/dL
interestingfactwasobservedinthisstudy:amuchhigher pro-portionofcontrolswithabdominalobesity(83%ofcontrols
versus71%ofpatients)andhypertension(77.5%ofcontrols
versus66% ofpatients)– featureswhich may berelated to dietaryhabitsofthispopulation.Glucocorticoidswereused bylessthan 30% ofpatients andanti-TNF-alpha agentsby about40%.Thelittleuseofglucocorticoidsandthe consider-ablerateofbiologicalusersmayhavecontributedtoflattenthe MSrateamongpatients,narrowingthegapbetweenpatient andcontrolgroups.Favorableeffectofanti-TNF-alphaagents inIR in patients withRA has been documented.38,39 With regardtocorticosteroids,bothcumulativedoseandchronic corticosteroid use were associated with IR and subclinical atherosclerosisintheItalianstudy,anditsauthorsbelievethat exposuretoglucocorticoidsmaybethetriggeringfactorfor IRandatherosclerosis.Inourstudy,wefoundnoassociation betweenexposuretooralglucocorticoidsandMS,butIRand subclinicalatherosclerosisareearlieralterationsthanMS; fur-thermore,over90%ofoursampleofpatientswithRAwasin continueduseoflow-doseprednisone,makingitdifficultthe demonstrationofastatisticallysignificantdifferencebetween groups,ifinfactthisdifferenceoccurred.Otherstudiesalso showedthatthecontinuoususeofcorticosteroidsisan inde-pendentpredictorofIRandMSinpatientswithRA,13,28while other authors have found no such association.18 It seems that,thankstotheirsystemicanti-inflammatoryeffect, short-termglucocorticoidscouldimproveIR,40,41butthelong-term side effects (dyslipidemia, hyperglycemia, hypertension, IR and abdominal obesity) could collectively contribute to an increaseofinsulinresistanceandthedevelopmentofMSand atherosclerosis.
An American study with 131 patients and 121 controls withoutRAshowedMSratesof36%inRAand27%incontrols, withnostatisticallysignificantdifference.20AlthoughBMIand waistcircumferencevaluesweresimilarbetweengroups,the quantificationofvisceralfatbyabdominalCTwashigherin malepatientsthaninmalecontrols,whilesubcutaneousfat washigherinfemalepatientsthaninfemalecontrols. Fur-thermore,theauthorsfoundamoreimportantassociationof visceralfatwithcardiometabolicriskfactorsinpatientswith RAofbothgendersversuscontrols,eveninthefaceof simi-larwaistcircumferencevalues.Thishasimportantpractical implications,becausemeasurestoreducevisceralfat(weight loss)appeartoexertmostimpactinreducingcardiovascular riskinpatientswithRAthan inthegeneralpopulation.In ourstudy,themostfrequentcomponentofMSwas abdom-inal obesity, found in almost all patients (98.1%); and BMI ≥30kg/m2,indicatingbodyobesity, wasalsofoundinmore
thanhalfofourpatientswithMS.Thesetwofindings char-acterize a population of overweight patients, that may be secondarytocarbohydrate-based eatinghabits, characteris-ticoftheNortheasternBrazilpopulation,sedentarylifestyle (morethanhalfofpatients),andchronicuseofglucocorticoids (90.9%).Nutritionalguidance, anadequate physicalactivity programandamorerationaluseofglucocorticoidscan con-tributetodecrease thecardiovascular riskinpatients with RA.
Anotherstudythatdidnotfindanincreasedprevalenceof MSinRAwasheldinIranwith92female RApatients,and 96healthywomen,withratesof27.2%inpatientsand35.4%
incontrols.24Themeanageofpatients(48.3±14.6years)and thedurationofillness(median:8years)werelowerthanour findings.Aninterestingfindingofthisstudyisthatover90% of patientswere taking hydroxychloroquine.A multicenter studyinArgentinapublishedquiterecently(2013)evaluated 409patients withRAand 624controlsandfounda protec-tiveeffectofhydroxychloroquineinMS.29IntheArgentinian studythecontrolgroupconsistedofpatientswithoutRAand diagnosedwithotherrheumaticdiseases:osteoarthritis,low backpain,fibromyalgia.TheprevalenceofMSbyNCEPIII(2005) criteriawasof30%and39%forpatientsandcontrols, respec-tively,withnostatisticallysignificantdifference.Perhapsthe patientcharacteristicsinthecontrolgroupcausedanincrease in the MS rate for this group, narrowing the gap between this group and RA patients’ group. Theonly other factors associatedwithMSinthisstudy wereageand rheumatoid factorandanti-CCPpositivity.Leeetal.27fromKoreareported thelowestprevalenceofMSinbothARandcontrolgroups (19%and15.6%),with84casesand109healthycontrols,all female.Thesepatientspresentedanearlierdisease(median: 3.5 years)and were younger (50.6±11.3 years). In addition to thesedemographic factors,genetic and cultural charac-teristicsandfactorsrelatedtodietaryhabitsspecificofthis populationmayhavecontributedtosuchlowMSrate.Inthe Koreanstudy,RApatientshadabdominalobesity(29.8%)and hypertension(44%)rateslowerthaninourstudy.
ThefirststudyshowinganincreaseofMSinRAwas con-ducted attheUniversity ofTennessee,USA,and published in2008with154 patientsand 85 controls(withoutchronic inflammatorydisease).16 Using NCEPIII2001definition, 42% ofpatientswithlong-standingRA(median:20years),30%of patientswithearlyRA(median:2years)and22%ofcontrols had MS. Compared to the present study, a higher propor-tion ofmalepatientswas includedinthe Tennesseestudy (27%versus2.7%),thesubjectshad ahigherlevel of educa-tion, and therehad moreCaucasian patients (∼90% versus
22.4%).Thesefactorsmayexplain,inpart,anMSrateslightly lower than thatfoundinourstudy.Alsointhat study,the authors demonstratedaprotectiveeffect of hydroxychloro-quine.In2011,anotherAmericanstudy byCrowsonetal.22 waspublished.Thisstudyrecruited232casesand1241 con-trols (patients without RA), showing33% and 25% for MS, respectively.Theauthorsbelievethattheexclusionofpatients withpreviouscardiovasculardiseasemayhavedecreasedthe actualprevalenceofMSintheirpatients.Twootherstudiesin Turkey26andMorocco28showedprevalenceratesof42.6%and 32.4%, respectively, withstatistically significant differences comparedtocontrols.Inbothstudies,patientswereyounger andhadless-lengthydisease,comparedtoourpatients.High ESRandglucocorticoiduse wereassociatedwithMSinthe Moroccanstudy.
diseaseactivityandaworstHAQscore.Olderagehasbeen associatedwithpresenceofMSinseveralstudies,aswellasin ourstudy.Alikelyexplanationforthisistheincreasedchance ofdevelopingfactors relatedtoMSwiththeprogressionof age.Diseaseduration,presenceofrheumatoidfactor, extra-articular manifestations, smoking history ≥20 packs/year, use of glucocorticoids, antimalarials or methotrexate and inflammatorymarkerswere notassociatedwithMS inthe studybyCunhaetal.25Anassociationbetweeninflammatory activity and MS has been found by some authors,14,16,23,27 but not byothers.21,24,26,29 Inflammatory cytokines present in RA, especially TNF-alpha and IL-6, increase IR, which promotes hyperglycemia, compensatory hyperinsulinemia anddyslipidemia,23favoringahigherriskfordevelopingMS. Thecontroversialassociationbetweeninflammatoryactivity ofRAandMScanbeexplainedbytheinstrumentsusedin studies to assess inflammation. Both the Disease Activity Score (DAS28) and serological inflammatory markers (ESR, CRP)evaluatetime-pointactivity,notactivityovertime.
Cross-sectionalstudieshaveshownMSprevalenceinRA rangingfrom17%to40.1%byNCEPIIIcriteria.13,17–19,23 AUK study byToms et al.18 examined the relationship of expo-suretoglucocorticoidswithMS,categorizingtheexposurein “noexposure”,“lowexposure”(<7.5mg/dayfor>6months),or “mediumexposure”(7.5–30mg/dayfor>6months),similarto ourstudy.Neithertheauthors’northepresentstudyfound anyassociation ofcorticosteroidusewithMS. Inthe Mexi-canstudybyZonana-Nacachetal.17evaluatingMSinpatients withRAandsystemiclupuserythematous,thefrequencyof MSwas18.7%and16.7%,respectively.Thevariablesassociated withMSwere olderage,educationallevel,monthlyincome andsmoking.Inourstudy,wefoundanassociationbetween smoking history >20 packs/year and MS. The association betweensmokingandMSisnotfullyunderstood.Although thereareseveralstudiesshowinganassociation,especially inmales,42thepresenceofotherfactorsrelatedtosmokers’ lifestylecouldexplainthisassociation.Forexample,sedentary lifestyleandalcoholismareadmittedlymorecommonamong smokersandcouldactasconfoundingvariables.43
Thisstudyhassomelimitations.Thelackofacontrolgroup withoutRAprecludesacomparisonofMSprevalenceamong RApatientsandindividualswithoutthediseaseinthis popu-lation.Thus,whileaprevalenceof50%inpatientsmayseem high,onecannotsaythatMSoccursmoreofteninRApatients thaninpeoplewithoutRA.MSprevalencestudiesinanadult Brazilianpopulationbyotherauthors37makeusbelievethat theratefoundinthepresentstudyhasbeenlargerthanin thegeneralpopulation(29.6%).However,genetic,culturaland nutritionalcharacteristicsspecificofBrazilianregionsshould beconsidered,andperhapstheBrazilianrateisnotagood referenceofcontrolforaNortheasternpopulation.Another limitationofthestudywasrelatedtosamplesize,whichmay haveinfluenced the lackofstatistical significanceofsome comparisons.
Insummary,patientswithadiagnosisofRAfollowedina tertiarycenterofauniversityhospitalinNortheasternBrazil presentoneofthehighestprevalenceratesofMS,when com-paredtostudiesinvariouspartsoftheworld,includingBrazil. Regarding the componentsofMS, it should benoticedthe highproportionofpatientswithabdominaladiposity(98.1%),
hypertension (80%)and low HDL (72.2%). Greater attention shouldbegiventothesepatientsregardingnutritional guid-anceandphysicalactivity,inordertopromoteweightlossand abettercontrolofmetabolicchanges.Heavysmokingwasalso significantlyassociatedwithMSinthisstudy,butonecannot saythatsmokingisariskfactorforMS.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Avina-ZubietaJA,ChoiHK,SadatsafaviM,EtminanM,Esdaile JM,LacailleD.Riskofcardiovascularmortalityinpatients withrheumatoidarthritis:ameta-analysisofobservational studies.ArthritisRheum.2008;59:1690–7.
2.NaranjoA,SokkaT,DescalzoMA,Calvo-AlénJ,
Hørslev-PetersenK,LuukkainenRK,etal.Cardiovascular diseaseinpatientswithrheumatoidarthritis:resultsfrom theQUEST-RAstudy.ArthritisResTher.2008;10:R30.
3.GamiAS,WittBJ,HowardDE,ErwinPJ,GamiLA,SomersVK, etal.Metabolicsyndromeandriskofincidentcardiovascular eventsanddeath:asystematicreviewandmeta-analysisof longitudinalstudies.JAmCollCardiol.2007;49:403–14.
4.ReavenG.Themetabolicsyndromeortheinsulinresistance syndrome?Differentnames,differentconcepts,and differentsgoals.EndocrinolMetabClinNAm. 2004;33:283–303.
5.EckelRH,GrundySM,ZimmetPZ.Themetabolicsyndrome. Lancet.2005;365:1415–28.
6.MottilloS,FilionKB,GenestJ,JosephL,PiloteL,PoirierP,etal. Themetabolicsyndromeandcardiovascularrisk:a
systematicreviewandmeta-analysis.JAmCollCardiol. 2010;56:1113–32.
7.HamaguchiM,KojimaT,TakedaN,NakagawaT,TaniguchiH, FujiiK,etal.Themetabolicsyndromeasapredictorof nonalcoholicfattyliverdisease.AnnInternMed. 2005;143:722–70.
8.ApridonidzeT,EssahPA,IuornoMJ,NestlerJE.Prevalenceand characteristicsofthemetabolicsyndromeinwomenwith polycysticovarysyndrome.JClinEndocrinolMetab. 2005;90:1929–35.
9.GrundySM.Cholesterolgallstones:afellowtravelerwith metabolicsyndrome.AmJClinNutr.2004;80:1–2.
10.CoughlinSR,MawdsleyL,MugarzaJA,CalverleyPM,Wilding JP.Obstructivesleepapnoeaisindependentlyassociatedwith naincreasedprevalenceofmetabolicsyndrome.EurHeartJ. 2004;25:735–41.
11.ChenJ,MuntnerP,HammLL,JonesDW,BatumanV,Fonseca V,etal.Themetabolicsyndromeandchronickidneydisease inUSadults.AnnInternMed.2004;140:167–74.
12.ChoiHK,FordES,LiC,CurhanG.Prevalenceofthemetabolic syndromeinpatientswithgout:theThirdNationalHealth andNutritionExaminationSurvey.ArthritisCareRes. 2007;57:109–15.
13.DeisseinPH,TobiasM,VellerMG.Metabolicsyndromeand subclinicalatherosclerosisinrheumatoidarthritis.J Rheumatol.2006;33:2425–32.
diseaseactivity:aretrospective,cross-sectional,controlled, study.AnnRheumDis.2007;66:28–33.
15.LaMontagnaG,CacciapuotiF,BuonoR,ManzellaD,Mennillo GA,ArcielloA,etal.Insulinresistanceisanindependentrisk factorforatherosclerosisinrheumatoidarthritis.Diabetes VascDisRes.2007;4:130–5.
16.ChungCP,OeserA,SolusJF,AvalosI,GebretsadikT,Shintani A,etal.Prevalenceofthemetabolicsyndromeisincreasedin rheumatoidarthritisandisassociatedwithcoronary atherosclerosis.Atherosclerosis.2008;196:756–63.
17.Zonana-NacachA,Santana-SahagunE,Jimenez-BalderasFJ, Camargo-CoronelA.Prevalenceandfactorsassociatedwith metabolicsyndromeinpatientswithrheumatoidarthritis andsystemiclupuserythematosus.JClinRheumatol. 2008;14:74–7.
18.TomsTE,PanoulasVF,DouglasKMJ,GriffithsHR,KitasGD. Lackofassociationbetweenglucocorticoiduseandpresence ofthemetabolicsyndromeinpatientswithrheumatoid arthritis:across-sectionalstudy.ArthritisResTher. 2008;10:R145.
19.ElkanAC,HakanssonN,FrostegardJ,CederholmT,Hafstrom I.Rheumatoidcachexiaisassociatedwithdyslipidemiaand lowlevelsofatheroprotectivenaturalantibodiesagainst phosphorylcholinebutnotwithdietaryfatinpatientswith rheumatoidarthritis:across-sectionalstudy.ArthritisRes Ther.2009;11:R37.
20.GilesJT,AllisonM,BlumenthalRS,PostW,GelberAC,PetriM, etal.Abdominaladiposityinrheumatoidarthritis.
Associationwithcardiometabolicriskfactorsanddisease characteristics.ArthritisRheum.2010;62:3173–82.
21.SahebariM,GoshayeshiL,MirfeiziZ,RezaieyazdiZ,HatefMR, Ghayour-MobarhanM,etal.Investigationoftheassociation betweenmetabolicsyndromeanddiseaseactivityin rheumatoidarthritis.SciWorldJ.2011;11:1195–205.
22.CrowsonCS,MyasoedovaE,DavisJM,MattesonEL,RogerVL, TherneauTM,etal.Increasedprevalenceofmetabolic syndromeassociatedwithrheumatoidarthritisinpatients withoutclinicalcardiovasculardisease.JRheumatol. 2011;38:29–35.
23.MokCC,KoGTC,HoLY,YuKL,ChanPT,ToCH.Prevalenceof atheroscleroticriskfactorsandthemetabolicsyndromein patientswithchronicinflammatoryarthritis.ArthritisCare Res.2011;63:195–202.
24.KarimiM,MazloomzadehS,KafanS,AmirmoghadamiH.The frequencyofmetabolicsyndromeinwomenwithrheumatoid arthritisandincontrols.IntJRheumDis.2011;14:
248–54.
25.daCunhaVR,BrenolCV,BrenolJCT,FuchsSC,ArlindoEM, MeloIMF,etal.Metabolicsyndromeprevalenceisincreased inrheumatoidarthritispatientsandisassociatedwith diseaseactivity.ScandJRheumatol.2012;41:186–91.
26.KarakocM,BatmazI,SariyildizMA,TahtasizM,CevikR, TekbasE,etal.Therelationshipofmetabolicsyndromewith diseaseactivityandthefunctionalstatusinpatientswith rheumatoidarthritis.JClinMedRes.2012;4:279–85.
27.LeeSG,KimJM,LeeSH,KimKH,KimJH,YiJW,etal.Isthe frequencyofmetabolicsyndromehigherinSouthKorean womenwithrheumatoidarthritisthaninhealthysubjects. KoreanJInternMed.2013;28:206–15.
28.RostomS,MengatM,LahlouR,HariA,BahiriR, Hajjaj-HassouniN.Metabolicsyndromeinrheumatoid
arthritis:casecontrolstudy.BMCMusculoskeletDisord. 2013;14:147.
29.SalinasMJH,BertoliAM,LemaL,SaucedoC,RosaJ,Quintana R,etal.Prevalenceandcorrelatesofmetabolicsyndromein patientswithrheumatoidarthritisinArgentina.JClin Rheumatol.2013;19:439–43.
30.PereiraIA,HenriquedaMotaLM,CruzBA,BrenolCV,Fronza LSR,BertoloMB,etal.Consenso2012daSociedadeBrasileira deReumatologiasobreomanejodecomorbidadesem pacientescomartritereumatoide.RevBrasReumatol. 2012;52:474–95.
31.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF, CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
32.FrareeSilvaRL,CarmesER,ScwartzAF,BlaszkowskiDS, CirinoRHD,DucciRDP.Cessac¸ãodetabagismoempacientes deumhospitaluniversitárioemCuritiba.JBrasPneumol. 2011;37:480–7.
33.PrevooML,van’tHofMA,KuperHH,vanLeeuwenMA,vande PutteLB,vanRielPL.Modifieddiseaseactivityscoresthat includetwenty-eight-jointcounts.Developmentand validationinaprospectivelongitudinalstudyofpatientswith rheumatoidarthritis.ArthritisRheum.1995;38:44–8.
34.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP.
Crossculturalreabilityofthephysicalabilitydimensionofthe HealthAssessmentQuestionnaire.JRheumatol.
1990;17:813–7.
35.GrundySM,CleemanJI,DanielsSR,DonatoKA,EckelRH, FranklinBA,etal.Diagnosisandmanagementofthe metabolicsyndrome.AnAmericanHeart
Association/NationalHeart,Lung,andBloodInstitute Scientificstatement.Circulation.2005;112:2735–52.
36.AlbertiKG,ZimmetP,ShawJ.Metabolicsyndrome:anew worldwidedefinition.Aconsensusstatementfromthe InternationalDiabetesFederation.DiabetMed. 2006;23:469–80.
37.VidigalFC,BressanJ,BabioN,Salas-SavadoJ.Prevalenceof metabolicsyndromeinBrazilianadults:asystematicreview. BMCPublicHealth.2013;13:1198.
38.StagakisI,BertsiasG,KarvounarisS,KavousanakiM,VirlaD, RaptopoulouA,etal.Anti-tumornecrosisfactortherapy improvesinsulinresistance,betacellfunctionandinsulin signalinginactiverheumatoidarthritispatientswithhigh insulinresistance.ArthritisResTher.2012;14:R141.
39.Gonzalez-GayMA,Gonzalez-JuanateyC,Vazquez-Rodriguez TR,Miranda-FilloyJA,LlorcaJ.Insulinresistancein
rheumatoidarthritis:theimpactoftheanti-TNF-alpha therapy.AnnNYAcadSci.2010;1193:153–9.
40.SvensonKLG,PollareT,LithellH,HallgrenR.Impaired glucosehandlinginactiverheumatoidarthritis:relationship toperipheralinsulinresistance.Metabolism.1998;37:125–30.
41.DeissenPH,JoffeBJ,StanwixAE,ChristianBF,VellerM. Glucocorticoidsandinsulinsensitivityinrheumatoid arthritis.JRheumatol.2004;131:867–74.
42.SunK,LiuJ,NingG.Activesmokingandriskofmetabolic syndrome:ameta-analysisofprospectivestudies.PLoSONE. 2012;7:e47791.