w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Thymidylate
synthase
genetic
polymorphism
and
plasma
total
homocysteine
level
in
a
group
of
Turkish
patients
with
rheumatoid
arthritis:
relationship
with
disease
activity
and
methotrexate
toxicity
Pınar
Borman
a,∗,
Özgur
Tas¸bas¸
a,
Halil
Karabulut
b,
Ajlan
Tukun
b,
Rezan
Yorgancıo ˘glu
aaAnkaraTrainingandResearchHospitalClinicofPhysicalMedicineandRehabilitation,Ankara,Turkey
bDepartmentofGenetics,FacultyofMedicine,AnkaraUniversity,Ankara,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received19May2014 Accepted1December2014 Availableonline9March2015
Keywords:
Rheumatoidarthritis Thymidylatesynthase Homocystein Polymorphism Methotrexate
a
b
s
t
r
a
c
t
Background:Thepolymorphismofthymidylatesynthase(TS)geneandhomocysteineare reportedtohavearelationshiptomethotrexate(MTX)metabolism,withconflictingresults. TheaimofthisstudywastodeterminehomocysteinelevelsandthefrequencyofTSgene triple repeat(TS3R)anddoublerepeat(TS2R)polymorphismsina groupofTurkishRA patientsandevaluateitsassociationwithMTXtoxicityanddiseaseactivity.
Methods:Sixty-fourpatientswithRAand31controlsubjectswithameanageof48.7±12.5 and46.2±13.4yearswereenrolledforthestudy.Demographiccharacteristicswereobtained andanumberofpatientswithMTX-relatedadverseaffectswererecordedinthepatient group.ThehomocysteinelevelsandTS2R/TS3RpolymorphismsoftheTSgenewere ana-lyzedandthedistributionofgenotypesaccordingtoMTXtoxicityanddiseaseactivitywas determined.
Results:The demographicpropertiesweresimilarbetweenthepatient andcontrol sub-jects.Folicacidsupplementationwithameandoseof5mgfolicacid/weekwaspresentin allpatients.Thirty-sixofthe64patientsshowedadverseeffectstoMTXtreatment.The respectivefrequency ofTS2Rand TS3Rpolymorphismswasfoundtobesimilarinthe patientandcontrolgroups.TS2RandTS3Rgenepolymorphismswerefoundtobe simi-larinpatientswithandwithoutMTX-relatedadverseevents.Themeanhomocysteinelevel wasalsosimilarinpatientswithandwithoutTSgenepolymorphism,butwasfoundto behigher(12.45mol/Lvs10.7mol/L)inpatientswithMTX-relatedsideeffectsthanin patientswithoutsideeffects.Themeanlevelofhomocysteinewascorrelatedwithlevelsof ESRinthepatientgroup.
∗ Correspondingauthor.
E-mail:[email protected](P.Borman). http://dx.doi.org/10.1016/j.rbre.2014.12.001
Conclusions: Inconclusion,homocysteinelevelsmightaffectthediseaseactivityand toxic-ityofMTXbut2Rand3RpolymorphismsintheTSgenewerenotrelatedwithMTX-related toxicityinRApatientsreceivingfolatesupplementation.Furtherstudiesareneededto illu-minatethepolymorphismsinotherenzymesthatmightberesponsiblefortheMTXtoxicity inpatientssufferingfromRA.
©2015ElsevierEditoraLtda.Allrightsreserved.
Polimorfismo
do
gene
timidilato
sintase
e
nível
plasmático
total
de
homocisteína
em
um
grupo
de
pacientes
turcos
com
artrite
reumatoide:
relac¸ão
com
a
atividade
da
doenc¸a
e
toxicidade
ao
metotrexato
Palavras-chave: Artritereumatoide Timidilatosintase Homocisteína Polimorfismo Metotrexato
r
e
s
u
m
o
Introduc¸ão: Relata-sequeopolimorfismodogenetimidilatosintase(TS)eahomocisteína têmrelac¸ãocomometabolismodometotrexato(MTX),comachadosconflitantes.Oobjetivo desteestudofoideterminarosníveisdehomocisteínaeafrequênciadepolimorfismosde repetic¸ãotripla(TS3R)edupla(TS2R)dogeneTSemumgrupodepacientesturcoscomAR eavaliarsuaassociac¸ãocomatoxicidadeaoMTXeaatividadedadoenc¸a.
Métodos: Foramincluídosnoestudo64pacientescomARe31indivíduosnogrupocontrole, commédiade48,7±12,5e46,2±13,4anos.Foramobtidasascaracterísticasdemográficas efoiregistradoonúmerodepacientesquerelataramefeitosadversosaoMTXnogrupoAR. ForamanalisadososníveisdehomocisteínaeospolimorfismosTS2R/TS3R.Foideterminada adistribuic¸ãodegenótiposdeacordocomatoxicidadeaoMTXeaatividadedadoenc¸a. Resultados:Osdadosdemográficosforamsemelhantesentreospacientesecontroles.Todos faziamsuplementac¸ãodeácidofólicoaumadosemédiade5mg/semana.Dos64pacientes, 36apresentaramefeitosadversosaotratamentocomMTX.Encontrou-seumafrequência depolimorfismosTS2ReTS3RsemelhantenosgruposARecontrole.Encontrou-sequeos polimorfismosTS2ReTS3Reramsemelhantesempacientescomesemeventosadversos relacionadoscomoMTX.Onívelmédiodehomocisteínatambémfoisimilarempacientes comesempolimorfismodogeneTS,maseramaiselevado(12,45mol/Lvs.10,7mol/L) empacientescomdoquesemefeitosadversosrelacionadoscomoMTX.Onívelmédiode homocisteínasecorrelacionoucomoVHSnogrupoAR.
Conclusões: Osníveisdehomocisteínapodemafetaraatividadedadoenc¸aeatoxicidade aoMTX,masospolimorfismos2Re3RnogeneTSnãosecorrelacionaramcoma tox-icidadeaoMTXempacientescomARquerecebemsuplementac¸ãodeácidofólico.São necessáriosmaisestudosparaesclarecerospolimorfismosemoutrasenzimasquepodem serresponsáveispelatoxicidadeaoMTXempacientescomAR.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Methotrexate(MTX) isthe cornerstone andthe most com-monlyuseddiseasemodifyinganti-rheumaticdrug(DMARD) forthe treatmentofrheumatoid arthritis (RA). The benefi-cialeffectsofMTX inRAstem primarilyfrom two aspects ofthemechanismofaction.Itdirectlyinhibitsseveralfolate dependent enzymes such as dihydrofolate reductase and thymidylatesynthase(TS);leadingtodisrupted purineand pyrimidinesynthesisandextracellularreleaseofadenosine, apotentantiinflammatoryagentrespectively.1,2Several
stud-iesdemonstratedtheeffectofgenepolymorphismsonMTX efficacy and safety but the available evidence is not yet conclusive.1–13 Thymidylate synthase is an important
tar-getformethotrexateand overexpressionofTSis linkedto resistanceofTS-targeteddrugs.14 PolymorphismofTSgene
isreportedtohavearelationshiptoMTX metabolismwith conflicting results.3–13 Homocysteine is an aminoacid
con-tainingthethiolgroupandisanintermediateproductofthe metabolismofmethionine.Somepreviousauthorsconcluded thatplasmahomocysteinemaybeimportantinmediatingthe sideeffectsofMTX.15–17Increasingpharmacogeneticstudies
showthatavarietyofgenepolymorphismsincludingthe TS-5′UTR3R/2Rvariantresultinhyperhomocysteinaemia,which could be responsible for more common and severe MTX-relatedsideeffects.7,17,18Besideshyperhomocysteinaemiahas
been linked to inflammation in RA. Homocysteine levels are alsoknown tobe influencedbynutrients suchas folic acidandthevitaminBcomplex,andanti-RAdrugssuchas MTX.6,7,16
toevaluatetheirrelationshipwithdiseaseactivityandMTX toxicity.
Methods
Sixty-fourRApatientswhomettheACRrevisedcriteria19were
recruitedfromtheoutpatientrheumatologyunitofClinicof Physical Medicineand Rehabilitation, AnkaraTraining and ResearchHospitalbetweenFebruaryandJuly2009.
CurrentorpasttreatmentwithMTXwasthemain crite-rionfortheinclusionofRApatientsintothestudy.Patients withameanBMI>35,aged<18,and >80years,havingB12 and folic acid depletion and patients with these comorbid diseases(chronicrenalfailure,hepaticinsufficiency,thyroid disease,heartfailureanduncontrolleddiabetesmellitus)were notincludedtothestudy.Onehundredandfourpatientswith rheumatoidarthritiswereassessedforeligibility.Ninety-eight patientshadcurrentorpastMTXtreatment,5patientsrefused toparticipateinthestudyand29patientswereexcludeddue toageorcomorbiddiseases.Therefore64RApatientswere includedtothestudy.Thirty-oneageandsexsimilar(within
±2years)healthycontrolsubjectswhowerethemembersof thehospitalstaffandvolunteeredtoparticipateinthestudy, werecomprised.Informedconsentwasobtainedfromallthe patients and controls, and the study was approved bythe ethicscommitteeofthehospital.
Demographiccharacteristicsincludingage,sex,bodymass indexofall subjects,and diseaseduration anddrugintake of RA patients were recorded. All the patients underwent adetailedclinicalinterview andphysicalexamination.The number ofpatientshaving MTX-related adverseevent was determinedfromthefilesandpatientinterviews.
Clinicalmeasurements
Thenumbersoftenderandswollenjointsaswellasdisease andtreatmentdurationwerecollectedfrompatientfiles.DAS 28wascalculatedforeach patientusingwell-known calcu-lations which included the number oftender and swollen joints, erythrocyte sedimentation rate (ESR), and patients’ globalassessmentofgeneralhealthexpressedonvisual ana-logscale.20ThescoresofHealthAssessmentQuestionnaire
(HAQ) indicatingthe functional status ofRApatients were recordedfromthefiles.21,22TheESR,Creactiveprotein(CRP),
DiseaseActivityScore(DAS)28andHAQwereconsideredas diseaseactivityparameters.
Laboratorymeasurements
Blood samples of the patients were taken to determine hemoglobin(Hb),ESRusingtheWestergrenmethod, rheuma-toid factor (RF) using nephelometric method and CRP by turbidimetricmethodinRAgroup.Theblood sampleswere centrifugedand the plasmasampleswere frozenat−20◦C untiltheanalysisofhomocysteine.Plasmahomocysteinewas measuredbyenzyme-linkedimmunoassayaccordingtothe manufacturer’sinstructions(AxisBiochemicals,ASANorway). Thehomocysteinelevelsamongpatientandcontrolgroups werecompared.Therelationshipbetweenhomocysteinelevel
and, disease characteristics and side effectswas also ana-lyzed.
Genomicstudies
GenomicDNAwaspreparedfromperipheralbloodofpatients andcontrols.The2Rand3RpolymorphismsoftheTSgene were analyzed by polymerase chain reaction amplification asdescribedpreviouslywithslightmodifications.23ThePCR
amplification program consisted ofan initialdenaturation stepat95◦Cfor15min,followedby30cyclesofdenaturationof 94◦Cfor1min,annealingat64◦Cfor1min,extensionat72◦C for1minandafinalextensionof72◦Cfor10min.PCRproducts were separated by 6%denaturing polyacrylamide gel elec-trophoresis(PAGE)for3hat300Vandvisualizedbyethidium bromide.Theallelicfrequenciesandgenotypedistributions amongpatientandcontrolgroupswerecompared.The distri-butionofgenotypesaccordingtodiseasecharacteristicsand sideeffectswasalsoanalyzed.
Statisticalanalysis
Descriptive statistics were performed and indicated as mean±standard deviation and median (maximum– minimum) for continuous variables. All qualitative data areexpressedasfrequenciesandpercentages.Thenormality ofthedistributionofcontinuousvariables wasanalyzedby Shapiro–Wilktest.Differencesingenotypedistributionwere testedwithtwosidedchi-squaretest.Theintergroup compar-isonsforcontinuousvariablesbetweenthetwogroups(with andwithoutpolymorphism)wereperformedbyStudentttest and Mann–WhitneyUtest. Spearman’scorrelationtestwas used to evaluate correlation between continuous variables and Pearson’schisquaretestorFisher’sexact outcomechi squaretestswereusedtodefinethecategoricalvariables.The level ofsignificancewas setto0.05.All statisticalanalyses weredoneusingSPSSforwindowsversion11.5.
Results
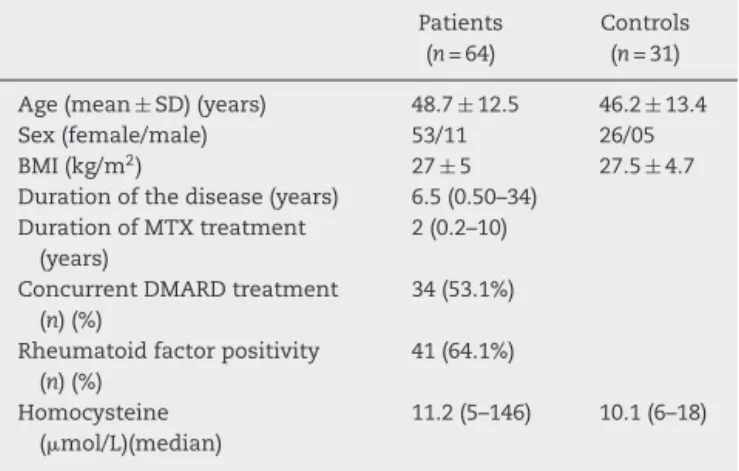
Atotalof64RApatientsand31controlsubjectswereincluded tothe study.DemographicdataofRApatientsand control subjectsarepresentedinTable1.Therewasnostatistical dif-ference betweenthemean age, sexand BMIofthe patient andcontrolgroups(p>0.05).MostpatientswerereceivingMTX atthetimeofrecruitmentbutsomehaddiscontinuedMTX treatmentduetoadverseeffects.Folicacidsupplementation withameandoseof5mgfolicacid/weeklywasrecordedinall patients.
Thirty-four (53%) patients were using MTX and other DMARDs.38(59.4%)patientswereusingoralMTX,while26 (40.6%) patients were on subcutaneous MTX therapy. The meandurationanddoseoftheMTXwere2years(0.2–10)and 15mg/week(10–20)respectively.
Table1–Demographicandclinicalcharacteristicsof patientsandcontrols.
Patients (n=64)
Controls (n=31)
Age(mean±SD)(years) 48.7±12.5 46.2±13.4
Sex(female/male) 53/11 26/05
BMI(kg/m2) 27±5 27.5±4.7
Durationofthedisease(years) 6.5(0.50–34) DurationofMTXtreatment
(years)
2(0.2–10)
ConcurrentDMARDtreatment (n)(%)
34(53.1%)
Rheumatoidfactorpositivity (n)(%)
41(64.1%)
Homocysteine (mol/L)(median)
11.2(5–146) 10.1(6–18)
BMI, body mass index; MTX, methotrexate; DMARD, disease-modifyingantirheumaticdrugs.
andclinicalfeaturesbetweenthepatientswithandwithout adverseeffectsduringMTXtreatment(p>0.05).
ThefrequenciesofTS2R/TS3Rpolymorphismswere
deter-minedinallsubjectsandwerefoundtobestatisticallysimilar betweenpatientand controlgroups (Table2).The distribu-tionofallelepolymorphismsinregardtoMTX-relatedadverse eventswascarriedout.TS2R/TS3Rgenepolymorphismswere foundtobesimilarinpatientswithandwithoutMTX-related adverseevents(Table3).Inordertodefinethe relationship betweenMTX-relatedsideeffectsandpolymorphismsinTS gene,wehaveanalyzedthepatientsreceivingonlyMTX treat-ment.Thedistribution ofTS 2R and 3R polymorphisms in patientswithandwithout adverseeffectswas againfound tobesimilar(p>0.05)(Table4).
Table4–Thegenotypicdistributionaccordingto adverseeventsinpatientsreceivingonlymethotrexate treatment.
Variables Adverseeffect(−) (n=13)
Adverseeffect(+) (n=17)
p
TS2R2R 3(23.1%) 7(41.2%)
TS2R3R 5(38.5%) 7(41.2%)
TS3R3R 5(38.5%) 3(17.6%)
2R3R+3R3R 10(76.9%) 10(58.8%) 0.440
TS,thymidylatesynthase.
Thedistributionofdisease activityparametersinregard toallelepolymorphismswasalsodetermined.Nostatistical differenceamongESR,CRP,HAQandDAS28valuesinregard
toTS2Rand3Rpolymorphismswasobservedinthepatient
group(Table5).
Themeanplasmahomocysteinelevelswerestatistically similarinpatientandcontrolsubjects.Inthepatientgroup, the mean homocysteinelevel wascorrelated withESR lev-els (p<0.05, r=30) and found to be significantly higher in patientswithMTX-relatedsideeffectsthaninpatients with-outsideeffects(Table6).Thehomocysteinevalueswerealso similarinpatientswithandwithoutTSgenepolymorphism (Table7).
Discussion
The most studied polymorphisms in the TS gene was described byHorieetal.24 TheTSgene containsatandem
repeatfoundinthe5′untranslatedregionandsubjectswere observedwithtwotandemrepeats,threetandemrepeatsor heterozygousgenotype.Thistandemrepeatregionactsasan
Table2–Thedistributionofgenotypes(TSpolymorphisms)inpatientandcontrolgroups.
Control(n=31) n(%)
RA(n=64) n(%)
p Oddsratio(%CI)
TS2R2R 6(19.4%) 14(21.9%) – 1.000a
TS2R3R 20(64.5%) 33(51.6%) 0.539 0.707(0.234–2.137)
TS3R3R 5(16.1%) 17(26.6%) 0.593 1.457(0.366–5.801)
2R3R+3R3R 25(80.6%) 50(78.1%) 0.778 0.857(0.294–2.499)
TS,thymidylatesynthase;CI,confidenceinterval. a Referencecategory.
Table3–ThegenotypicdistributionofRApatientsaccordingtopresenceofadverseevents.
Adverseevents(−) (n=28)
Adverseevents(+) (n=36)
p Oddsratio(95%CI)
TS2R2R 4(14.3%) 10(27.8%) – 1.000a
TS2R3R 14(50.0%) 19(52.8%) 0.375 0.543(0.141–2.093)
TS3R3R 10(35.7%) 7(19.4%) 0.098 0.280(0.062–1.266)
2R3R+3R3R 24(85.7%) 26(72.2%) 0.195 0.433(0.120–1.567)
Table5–Thedistributionofdiseaseactivityparametersaccordingtothepolymorphismsinthymidylatesynthasegene.
Variables 2R2R
(n=14)
2R3R (n=33)
3R3R (n=17)
p
HAQ(median) 0.8(0–3) 0.6(0–3) 0.75(0–2.5) 0.695
DAS28(median) 4.0(2.1–7.5) 4.0(1.7–7.8) 4.5(1.9–6.9) 0.909
ESR(median) 29.0(10.0–120.0) 30.0(2.0–82.0) 25.0(7.0–65.0) 0.695
CRP(median) 0.7(0.3–10.0) 0.7(0.1–10.5) 0.8(0.2–4.8) 0.409
HAQ,healthassessmentquestionnaire;DAS,diseaseactivityscore;ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein.
enhancertotheTSpromoterandleadstoanincreaseinTS activity.ThepromoterenhancerregionofTSgenecontains adouble(2R)oratriple(3R)28-base-pair(bp)tandemrepeat polymorphismwhere3Rgenotypeisassociatedwithahigher TSgeneexpression.24,25
Ourstudyshowed thatthefrequencyofTS2Rand TS3R polymorphisms was similar in Turkish RA patients and healthycontrolsubjects.Theratesofpolymorphisminthe tandem repeat of 5′ UTR region were significantly lower fromthe previousstudieswhich couldberelatedtoethnic differences.26
Previousauthors reported that genotyping for TS poly-morphism may become auseful indicator for determining theappropriatedosageofMTXandformonitoringMTX tox-icity inRA patients.2,6,9,11 There have been confusingdata
regardingtheimpactofTSpolymorphismonMTXtreatment responseinRApatients,asTSisoneoftheenzymesinthe folatemetabolicpathwaythatisdirectlyinhibitedbyMTX.A lowerdiseaseactivityandanimprovedresponsetolowdose MTX were reported in patients having TS polymorphism.2
Kumagai et al.9 and Inoue et al.11 evaluated the
relation-ship between the response to MTX and TS genotype in Japanese patients and reported a better response to MTX in patients with 6bp alleles in TS 3′ UTR region. But the regardedpatientsintheirstudywereonlowdose(6mg/week) MTX therapy. On the other hand,the 3R/3R genotype was associatedwithpoorresponsetoMTXtherapyinsome pre-vious studies.6,13 Regarding MTX toxicity, polymorphism of
TSgenewasassociatedwithoccurrenceofalopecia18while
no relation between polymorphism of TS gene and MTX toxicity was reported in other previous studies.6 Contrary
to some previous studies, the present study also showed that genetic polymorphisms in the TS gene didnot influ-ence the disease activity or toxicity of MTX treatment in RApatientsreceivingfolatesupplementation.Grabaretal.8
studied a group of gene polymorphism including TS and reported no relationship betweenpolymorphisms and dis-ease activity parameters including ESR, CRP and DAS 28
Table6–Homocysteinlevelsaccordingtothepresence ofadverseeffectsofmethotrexateinpatientswithAR.
Homocystein p
Adverseeffects 0.024
Absent 10.7(5.0–33.0)
Present 12.45(6.8–146.0)
values.RegardingtheadverseeffectsduetoMTXtreatment,
TS2R/3Rpolymorphismswerefoundtodecreasebonemarrow
toxicityintheirstudygroup.8 Inthepresenceofrisk
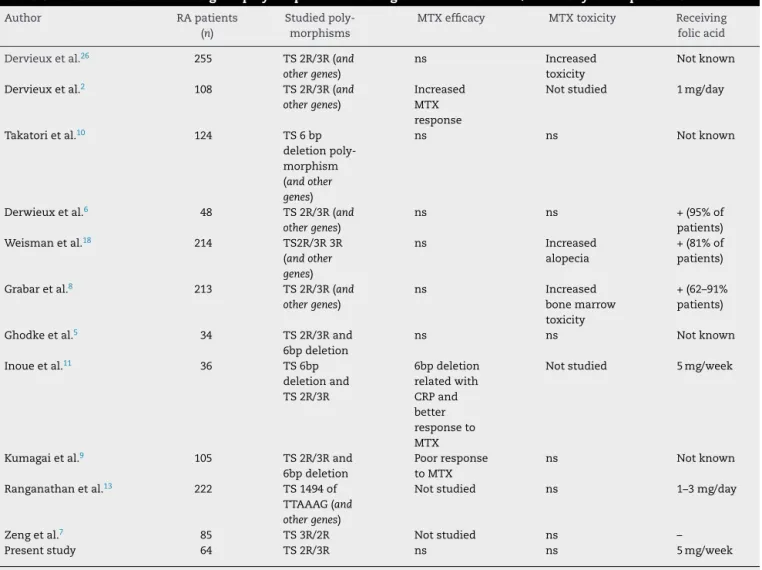
geno-typecombinationsamongvariantsinTSandothergenes,a higherlikelihoodtoexhibittoxicitieswasreported.27Table8
representsareviewofpublishedliteratureonTSgene poly-morphisms affectingMTX treatment and/or toxicity inRA patients.
MTXinhibitstheenzymedihydrofolatereductase,thereby depletingthepoolofreducedfolatesandproducingastateof effectivefolatedeficiency.1FolicacidimprovesMTX
tolerabil-ityrateswithoutcompromisingefficacy.1,25mg/dayfolicacid
hasbeenproposedtobegiveninallpatientsreceivingMTX therapy.28,29Inourstudyallofthepatientswereon
concomi-tantfolicacidsupplementation,whichmightbealimitationof ourstudy.Itwouldbevaluabletostudythesegeneexpressions accordingtosideeffectsofMTX,inbothpatientsonfolate supplementationand inpatientsnotreceivingthis supple-mentation.Ourstudyalsoincludedarelativelysmallnumber ofpatientsandnotallofthepolymorphicgenesinvolvedin theMTXmetabolismweretested.Thereforeadditionaldata mightbeneededtodemonstratemoreconclusiveresults.But ourstudywasnotbiasedbygeneticheterogeneity,asallthe patientsweremembersofanethnicallyhomogeneous popu-lation.WehavepreviouslystudiedpolymorphismsinMTHFR A1298CandC677Tgenesbutfailedtoshowanyrelationship withtoxicityofMTXinthesamegroupofRApatients.30The
discrepanciesbetweenpreviousstudiesandthepresentstudy mightbeduetothedifferencesinthefrequenciesofTS2R/3R homozygoticpolymorphisms,sinceourstudygrouphaslower frequenciesofthispolymorphisms(5%and6%)thanin previ-ousstudies.5,18
Table7–Thelevelsofhomocysteinaccordingtothe polymorphismofThymidylatesynthasegene.
Homocystein p
0.893a TS2R2R 11.3(5.2–146.0)
TS2R3R 11.0(5.2–50.0) TS3R3R 11.0(5.0–42.0)
2R3R+3R3R 11.0(5.0–50.0) 0.655b
TS,thymidylatesynthase.
a Varianceanalysisamonggenotypes.
b Comparisonbetweengenotypeswithriskyalleleandreference
Table8–LiteraturereviewonTSgenepolymorphismsaffectingMTXtreatmentand/ortoxicityinRApatients.
Author RApatients
(n)
Studied poly-morphisms
MTXefficacy MTXtoxicity Receiving
folicacid
Dervieuxetal.26 255 TS2R/3R(and
othergenes)
ns Increased
toxicity
Notknown
Dervieuxetal.2 108 TS2R/3R(and othergenes)
Increased MTX response
Notstudied 1mg/day
Takatorietal.10 124 TS6bp deletion poly-morphism (andother genes)
ns ns Notknown
Derwieuxetal.6 48 TS2R/3R(and othergenes)
ns ns +(95%of
patients) Weismanetal.18 214 TS2R/3R3R
(andother genes)
ns Increased
alopecia
+(81%of patients)
Grabaretal.8 213 TS2R/3R(and othergenes)
ns Increased
bonemarrow toxicity
+(62–91% patients)
Ghodkeetal.5 34 TS2R/3Rand
6bpdeletion
ns ns Notknown
Inoueetal.11 36 TS6bp
deletionand TS2R/3R
6bpdeletion relatedwith CRPand better responseto MTX
Notstudied 5mg/week
Kumagaietal.9 105 TS2R/3Rand 6bpdeletion
Poorresponse toMTX
ns Notknown
Ranganathanetal.13 222 TS1494of TTAAAG(and othergenes)
Notstudied ns 1–3mg/day
Zengetal.7 85 TS3R/2R Notstudied ns –
Presentstudy 64 TS2R/3R ns ns 5mg/week
TS,thymidylatesynthase;MTX,methotrexate;ns,non-significant.
Plasmahomocysteinelevels were reportedtoberelated withinflammatorymarkersinsomeRApatients16,17in
accor-dancewithourdataindicatingarelationshipbetweenESRand homocysteinelevelsinourstudygroup.
Previousstudies onthe effect ofMTX on homocysteine concentrations in patients with RA showed a substantial riseinhomocysteineconcentrationsduringMTXtreatment, aneffectthatwasdiminishedbyfolate supplementation.31
Plasmahomocysteinelevelsweremeasuredin105RApatients and patients receiving MTX showed a persistent greater increaseinplasmahomocysteinewhichwasexplainedby fur-therenhancementofMTHFRpolymorphism.Theseauthors concluded that plasma homocysteine may be important in mediating the gastrointestinal side effects of MTX.15
Some previous authors speculated that impeded homo-cysteine metabolismintroducedbyintracellularconversion of folate was the mechanism of the increased frequency of toxicities in patients with the mutant allele at C677T polymorphism.4,29Inourstudythehomocysteinelevelswere
similarbetweenpatientsandhealthycontrolsubjectswhich may be due to the regular receiving of folate supplemen-tation in all patients. Previous studies, in agreement with our study, indicated that MTX doses with adjuvant folic
acid did notincrease homocysteinelevels.28 But
homocys-teinelevelswerefoundtobehigherinpatientswithadverse effectsduetoMTXthaninpatientswithoutadverseeffects. This may be explained by the active disease in patients who have to decrease or stop MTX treatment due to side effects.
Methotrexate metabolism is complex and involves the interaction ofa numberofgenes inthe folate pathway.In ourstudy,2Rand3RpolymorphismsintheTSgenewerenot relatedwithMTXefficacyortoxicityinRApatientsreceiving folatesupplementation.Wespeculatethattheeffectsofother geneticpolymorphismsonthesensitivitytoMTXtoxicitymay bestrongerthanthoseofTS2Rand3Rgenepolymorphisms. However,homocysteinelevelswerecorrelatedwithESR lev-els,andfoundtobehigherinpatientswithadverseeffects thaninpatientswithouttheseeffects,whichmightindicate the effect ofhomocysteineondisease activity and/or MTX toxicity.
polymorphismsinotherenzymesthatmightberesponsible fromclinicaltoxicityofMTXinpatientssufferingfromRA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RanganathanP,McLeodHL.Methotrexatepharmacogenetics: thefirststeptowardindividualizedtherapyinrheumatoid arthritis.ArthritisRheum.2006;54:1366–77.
2. DervieuxT,FurstD,LeinDO,CappsR,SmithK,WalshM, etal.Polyglutamationofmethotrexatewithcommon polymorphismsinreducedfolatecarrieraminoimidazole carboxamidribonucleotidetransformylaseandthymidylate synthaseareassociatedwithmethotrexateeffectsin rheumatoidarthritis.ArthritisRheum.2004;50: 2766–74.
3. KremerJM,GalivanJ,StreckfussA,KamenB.Methotrexate metabolismanalysisinbloodandliverofrheumatoid arthritispatients:associationwithhepaticfolatedeficiency andformationofpolyglutamates.ArthritisRheum.1986;29: 832–5.
4. TaniguchiA,KamataniN.Pharmacogeneticapproachesto rheumatoidarthritis.PharmacogenomicsJ.2004;4: 350–3.
5. GhodkeY,ChopraA,JoshiK,PatwardhanB.Arethymidilate synthaseandmethylenetetrahydrofolatereductasegenes linkedwithmethotrextaeresponse(efficacy,toxicity)in Indian(Asian)rheumatoidarthritispatients?ClinRheumatol. 2008;27:787–9.
6. DervieuxT,GreensteinN,KremerJ.Pharmacogenomicand metabolicbiomarkersinthefolatepathwayandtheir associationwithmethotrexateeffectsduringdosage escalationinrheumatoidarthritis.ArthritisRheum. 2006;54:3095–103.
7. ZengQY,WangYK,XiaoZY,ChenSB.Pharmacogeneticstudy of5,10MTHFRC677Tandthymidylatesyntase3R/2Rgene polymorphismsandmethotrexate-relatedtoxicityinChinese Hanpatientswithinflammatoryarthritis.AnnRheumDis. 2008;67:1193–4.
8. GrabarBP,LogarD,LestanB,DolzanV.Geneticdeterminants ofmethotrexatetoxicityinrheumatoidarthritispatients:a studyofpolymorphismsaffectingmethotrexatetransport andfolatemetabolism.EurJClinPharmacol.2008;64: 1057–68.
9. KumagaiK,HiyamaK,OyamaT,MaedaH,KohnoN. Polymorphismsinthethymidylatesynthaseand
methylenetetrahydrofolatereductasegenesandsensitivityto thelow-dosemethotrexatetherapyinpatientswith
rheumatoidarthritis.IntJMolMed.2003;11: 593–600.
10.TakatoriR,TakahushiK,TokunagaD,HojoT,FujiokaM, AsanoT,etal.ABCB1,C3435Tpolymorphisminfluences methotrexatesensitivityinrheumatoidarthritispatients. ClinExpRheumatol.2006;24:546–54.
11.InoueS,HashiguchiM,TakagiK,KawaiS,MochizukiM. Preliminarystudytoidentifythepredictivefactorsforthe responsetomethotrexatetherapyinpatientswith rheumatoidarthritis.JPharmSocJpn.2009;129: 843–9.
12.WesselsJA,DeVries-BaustraJK,HeijmansBT,SlagboomPE, Goekoop-RuitermanYP,AllaartCF,etal.Efficacyandtoxicity ofmethotrexateinearlyrheumatoidarthritisareassociated
withsinglenucleotidepolymorphismingenescodingfor folatepathwayenzymes.ArthritisRheum.2006;54:1087–95. 13.RanganathanP,CulverhouseR,MarshS.Methotrexategene
polymorphismsandtheireffectsonMTXtoxicityin CaucasianandAfricanAmericanpatientswithrheumatoid arthritis.JRheumatol.2008;5:559–69.
14.MarshS.Thymidylatesynthasepharmacogenetics.Invest NewDrugs.2005;23:533–7.
15.HaagsmaCJ,BlomHJ,VanRielPL,Van’tHofMA,Giesendorf BA,VanOppenraaij-EmmerzaalD,etal.Influenceof sulphasalazine,methotrexate,andthecombinationofboth onplasmahomocysteineconcentrationsinpatientswith rheumatoidarthritis.AnnRheumDis.1999;58:79–84. 16.FujimakiC,HayashiH,TsuboiS,MatsuyamaT,KosugeK,
YamadaH,etal.Plasmatotalhomocysteineleveland methylenetetrahydrofolatereductase677C>Tgenetic polymorphisminJapanesepatientswithrheumatoid arthritis.Biomarkers.2009;14:49–54.
17.VanEdeAE,LaanRF,BlomHJ,BoersGH,HaagsmaCJ,Thomas CM,etal.Homocysteineandfolatestatusin
methotrexate-treatedpatientswithrheumatoidarthritis. Rheumatology(Oxf).2002;41:658–65.
18.WeismanMH,FurstDE,ParkGS,KremerJM,SmithKM, WallaceDJ,etal.Riskgenotypesinfolate-dependentenzymes andtheirassociationwithmethotrexate-relatedsideeffects inrheumatoidarthritis.ArthritisRheum.2006;54:607–12. 19.ArnettFC,EdworthySM,BlochDA,McShaneDJ,FriesJF,
CooperNS,etal.TheAmericanRheumatismAssociation 1987revisedcriteriafortheclassificationofrheumatoid arthritis.ArthritisRheum.1988;31:315–24.
20.VanderHeijdeDM,Van’tHofMA,VanRielPL,TheunisseLA, LubbertsEW,VanLeeuwenMA,etal.Judgingdiseaseactivity inclinicalpracticeinrheumatoidarthritis:firststepinthe developmentofadiseaseactivityscore.AnnRheumDis. 1990;49:916–20.
21.BruceB,FriesJF.TheHealthAssessmentQuestionnaire (HAQ).ClinExpRheumatol.2005;23Suppl.39:14–8. 22.SenerdemN,GulA,KoniceM,AralO,OcalL,InancM,etal.
Theuseoftwodifferenthealthassessmentquestionnairesin Turkishrheumatoidarthritispopulationandassessmentof theassociationwithdisability.ClinRheumatol.1999;18: 33–7.
23.EtienneMC,ChazalM,Laurent-PuigP,MagnéN,RostyC, FormentoJL,etal.Prognosticvalueoftumoralthymidylate synthaseandp53inmetastaticcolorectalcancerpatients receivingfluorouracil-basedchemotherapy:phenotypicand genotypicanalyses.JClinOncol.2002;20:2832–43.
24.HorieN,AibaH,OguroK,HojoH,TakeishiK.Functional analysisandDNApolymorphismofthetandemlyrepeated sequencesinthe5′terminalregulatoryregionofthehuman
geneforthymidylatesynthase.CellStructFunct. 1995;20:191–7.
25.InoueS,HashiguchiM,ChiyadoT,SunamiY,TanakaT, MochizukiM,etal.Pharmacogeneticstudyof
methylentetrahydrofolateandthymidylatesynthasein Japaneseandassessmentofethnicandgenderdifferences. Pharmacogenomics.2007;8:41–7.
26.KawakamiK,OmuraK,KanehiraE,WatanabeY.Polymorphic tandemrepeatsintheTSgeneisassociatedwithitsprotein expressioninhumangastrointestinalcancers.Anticancer Res.1999;19:3249–52.
27.DerwieuxT,WesselsJA,VanderStraatenT,PenrodT,Moore JH,GuchelaarHJ,etal.Gene-geneinteractionsinfolateand adenosinebiosynthesispathwaysaffectmethotrexate efficacyandtolerabilityinrheumatoidarthritis. PharmacogenetGenomics.2009;19812:935–44. 28.WhittleSL,HughesRA.Folatesupplementationand
29.MorganSL,BaggottJE.Folatesupplementationduring methotrexatetherapyforrheumatoidarthritis.ClinExp Rheumatol.2010;28Suppl.61:102–9.
30.TasbasO,BormanP,GurkanKarabulutH,TukunA, Yorgancıo ˘gluR.ThefrequencyofA1298CandC677T polymorphismsofthemethylenetetrahydrofolategenein
Turkishpatientswithrheumatoidarthritis:relationshipto methotrexatetoxicity.OpenRheumatolJ.2011;5:30–5. 31.HoekstraM,HaagsmaCJ,DoelmanCJA,VandeLaarMAFJ.