Corresponding Author: 2011 Nov.-Dec.;19(6):1314-21
www.eerp.usp.br/rlae
Corresponding Author: Josefa Márquez Membrive
Universidad de Almería. Facultad Ciencias de la Salud. Carretera Sacramento s/n
04120, Almería, España E-mail: [email protected]
Quality of life in perimenopausal women working in the health and
educational system
Josefa Márquez Membrive
1José Granero-Molina
2Ma José Solvas Salmerón
3Cayetano Fernández-Sola
4Carmen Ma Rodríguez López
5Tesifón Parrón Carreño
6The objective of this study was to determine the association between the professional activity
and the perceived quality of life in climacteric women who work in Health and Education. A
descriptive and cross-sectional study was developed in a sample of 203 climacteric women,
together with a correlation analysis of labor factors’ influence on health-related quality
of life. Significant differences were found between working women’s quality of life and
some labor conditions. The perceived quality of life in perimenopausal women who work in
Education is higher than that of those working in Health (p=0.004). Nursing professionals
can develop health programs that deal with the work conditions that negatively influence
the perceived quality of life in climacteric women.
Descriptors: Quality of Life; Climacteric; Occupational Health; Job Satisfaction.
1 RN, M.Sc. in Nursing, Full Professor, Departamento de Enfermería y Fisioterapia, Universidad de Almería, Spain. E-mail: [email protected]. 2 RN, Ph.D. in Health Sciences, Professor, Departamento de Enfermería y Fisioterapia, Universidad de Almería, Spain. E-mail:
3 RN, Complejo Hospitalario Torrecárdenas, Almería, Spain. E-mail: [email protected].
4 RN, Ph.D. in Nursing, Professor, Departamento de Enfermería y Fisioterapia, Universidad de Almería, Spain. E-mail: [email protected]. 5 Physician, Ph.D. in Medicine, Full Professor, Departamento de Neurociencia y Ciencias de la Salud, Universidad de Almería, Spain.
E-mail: [email protected].
6 Physician, Ph.D. in Medicine, Associate Professor, Departamento de Neurociencia y Ciencias de la Salud, Universidad de Almería,
Qualidade de vida em mulheres climatéricas que trabalham no sistema sanitário e educativo
O objetivo deste estudo foi determinar a associação entre a atividade proissional e a
qualidade de vida percebida em mulheres climatéricas que trabalham nas áreas da saúde
e educação. Realizou-se estudo descritivo e transversal, numa amostra de 203 mulheres
climatéricas, juntamente com análise correlacional da inluência dos fatores de trabalho na qualidade de vida, relacionada à saúde. Encontraram-se diferenças signiicativas
entre a qualidade de vida das trabalhadoras e algumas variáveis laborais. A qualidade
de vida percebida pelas mulheres perimenopáusicas que trabalham na área da educação
é superior à daquelas que trabalham na área da saúde (p=0,004). Os proissionais
de enfermagem podem elaborar programas de saúde que abordem as condições de
trabalho que inluenciam negativamente a qualidade de vida percebida pelas mulheres
climatéricas.
Descritores: Qualidade de Vida; Climatério; Saúde Ocupacional; Satisfação no
Emprego.
Calidad de vida en mujeres climatéricas que trabajan en el sistema sanitario y educativo
El objetivo de este estudio fue determinar la asociación entre la actividad profesional y
la calidad de vida percibida en mujeres climatéricas que trabajan en las áreas sanitaria y
educativa. Se realizó un estudio descriptivo y transversal, en una muestra de 203 mujeres
climatéricas, junto al análisis correlacional de la inluencia de los factores laborales en la calidad de vida relacionada con la salud. Se encontraron diferencias signiicativas entre
la calidad de vida de las trabajadoras y algunas condiciones laborales. La calidad de vida
percibida por las mujeres perimenopáusicas que trabajan en educación es superior a la
de las que trabajan en salud (p=0,004). Los profesionales de Enfermería pueden elaborar
programas de salud, que aborden las condiciones de trabajo que inluyen negativamente
en la calidad de vida percibida por las mujeres climatéricas.
Descriptores: Calidad de Vida; Climaterio; Salud Ocupacional; Satisfacción en el
Trabajo.
Introduction
Quality of life has turned into a reference for the
so-called “state of wellbeing” in developed countries.
This broad concept receives the complex inluence of
multiple factors, including: psychological condition,
independence level, social relations, environmental
characteristics and physical health.
Satisfaction with health is one of the fundamental
components of perceived quality of life, which is why
a term was proposed to adapt its denomination to the
contents of the quality of life concept: Health-Related
Quality of Life (HRQoL).
This concept includes, among other factors, the
work-related quality of life(1) and the possible inluence
the endocrine modiications of ovarian failure may exert
on women’s perceived quality of life(2-4). Therefore,
from the HRQoL perspective, the consequences of the
climacterium should be considered as a speciic aspect
of health-related quality of life. The increased life
expectancy of the general population and of women in
particular (there will be more than ten million climacteric
women in Spain during this century) has turned women’s
health care in this phase of life into a priority; the way
this should be accomplished, however, represents one
of the main sources of public health debate. Although
agreement exists that the approach of the climacterium
able to develop it unavoidably implies knowledge about
symptom-related factors and the determination of its
inluence on quality of life. Various publications on both
issues(7-9) evidence socio-demographic factors, including
the number of children, social class, culture or work(10-13)
that have demonstrated their role as relevant variables
in the clinical vivacity about the climacterium and
menopause.
Most papers published speciically analyze labor activities, but a review about their inluence on
menopausal women’s quality of life reveals contradictory
results. While some studies found no relation between
work, menopause and quality of life(2,14-15), others
show that working women experience less speciically
menopausal symptoms than housewives(16-17). Some
authors(18) appoint that the satisfaction level of
menopausal women with work is positively related to a
lesser display of somatic and psychological symptoms.
This same relation is also present in another study that
also considers(19) the need to incorporate the range of
work-related variables in research on quality of life in
the climacterium.
The goal of this study is to describe and analyze
the association between labor conditions and quality
of life among climacteric women working in health and
education.
Method
This descriptive and cross-sectional study
incorporates a correlation analysis of the variables
involved, searching for associations among them.
Data were collected in 2007-2008, in a reference
population of climacteric women, between 45 and 65
years old, who worked in the health and educative
sectors in the province of Almería (Spain). This age
range, previously used in construction and validation
process of speciic menopause scales among Spanish
women(20), collects information on the variable nature of
the start, continuation and disappearance of climacteric
symptoms, also coinciding with the inal phase of the
professional life of women which, in Spain, extends
until the age of 65 years. Group-1. Nurses who work in
hospitals (Complejo Hospitalario Torrecárdenas) and in
Primary Health Care services (Zonas Básicas de Salud in
the Almería-Centro Health District). Group-2. Teachers
at Secondary Education Institutions and the Universidad
de Almería. Both areas were chosen because most
workers are women, their nature is clearly social and
their labor conditions are clearly distinctive.
In a reference population of 429 women who
attended to the inclusion criteria, the sample size was
estimated using QUESTA software, with a 95% conidence
level. The inclusion criteria were: being a woman, age
between 45 and 65 years, who were working in health
or education in the province of Almería (Spain) at the
time of data collection. The deinitive sample comprised
203 active women: 86 nurses working in health and 117
teachers, selected from the original list through simple
random sampling. After obtaining permission to develop
the research, the primary investigator contacted the
boards of the job centers, which provided the data needed
to select and contact the participants from the Secondary
Education Institutions, University Departments, Health
Centers and the Hospital Complex. Three investigators
made appointments by telephone with all participating
workers, with a view to data collection at the different
job centers. Data were collected during the rest hours of
the Secondary Education and University teachers, as well
as the Hospital and Health Center workers. In speciic
meeting rooms at the job centers, the investigator
presented and explained the study aims to the women
and, after showing a data conidentiality commitment,
invited them to participate, handed over the survey and
gave them time to answer it, demonstrating availability
to clarify any kind of doubt. None of the women invited
refused to participate. Data were collected during
approximately ten months, between September 2007
and June 2008. The self-administered questionnaire
contained 73 questions, distributed in three parts:
1st Part: collects data on socio-demographic
characteristics and the climacteric proile, measured
through closed questions and distinguishing among
three subgroups: premenopause (>45 years and normal
menstruation), climacterium (>45 years, irregular
menstruation in number or quantity) and postmenopause
(>45 years, as from 12 months without menstruation).
2nd Part: explores the labor conditions through 24
closed questions, distributed in two blocks. The irst 18
items are part of the Quality of Life at Work Survey (QLWS)
(21), which the Spanish Ministry of Labor and Social Affairs
periodically applies. The instrument explores workers’
quality of life through objective information about the
actual situations in which activities are accomplished in the
work environment, together with subjective information
about the workers’ personal perceptions about their
labor conditions and relations. The six remaining items,
addressing work conditions and the women’s type of
occupational exposure, were obtained from the Spanish
Márquez Membrive J, Granero Molina J, Solvas Salmerón MJ, Fernández Sola C, Rodríguez López CM, Parrón Carreño T.
3rd Part: contains 31 items and collects information
about quality of life and menopause through the use of
the Cervantes Scale(20). This questionnaire, validated
for menopause research in Spanish women, measures
the global quality of life score, as well as scores in
different areas or domains (psychic, partner relation,
vasomotor symptoms, aging). Short, practical to apply
and easy to correct, this scale uses a score range from
0 to 5 to measure the presence of symptoms, in which
0 represents the absence of the symptom and 5 the
presence of a very severe symptom. Therefore, lower
scores correspond to a better quality of life.
Calculations were elaborated in SPSS 17.0
software. First, data were subject to descriptive analysis:
determination of means and standard deviations
(quantitative variables) and percentages (categorical
variables). Next, the relation between quality of life and
work conditions was analyzed: Pearson’s correlation
test, Spearman’s test and Kendal’s Tau-b test were used;
Student’s t-test was used to compare means
(Mann-Whitney for those variables in which n<30); the
chi-square test was used to compare qualitative variables.
Table 1 – Climacteric condition of women in the simple
according to professional activity (Health-Education)
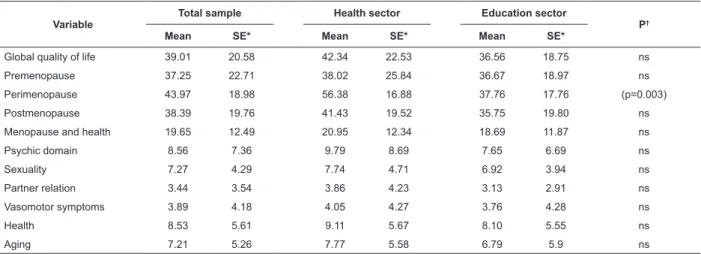
Table 2 – HRQoL in climacteric women
Results
The mean age of the women in the simple was 50.61
years and similar in both sectors. About 69% were married
or had a ixed partner. The mean number of children was
1.92. In general, the collected data show homogeneous
climacteric patterns in both groups (Table 1).
Variable Total sample (n)
Health sector (n)
Education sector (n)
Premenopausal 80 34 46
Perimenopausal 39 13 26
Postmenopausal 84 39 45
The global quality of life score was lower among
women who worked in the Education System (36.56)
tan in the Health System (42.34), which means a
higher perceived quality of life, although differences
were only signiicant in the group of perimenopausal
women (Table 2).
Variable
Total sample Health sector Education sector
P†
Mean SE* Mean SE* Mean SE*
Global quality of life 39.01 20.58 42.34 22.53 36.56 18.75 ns
Premenopause 37.25 22.71 38.02 25.84 36.67 18.97 ns
Perimenopause 43.97 18.98 56.38 16.88 37.76 17.76 (p=0.003)
Postmenopause 38.39 19.76 41.43 19.52 35.75 19.80 ns
Menopause and health 19.65 12.49 20.95 12.34 18.69 11.87 ns
Psychic domain 8.56 7.36 9.79 8.69 7.65 6.69 ns
Sexuality 7.27 4.29 7.74 4.71 6.92 3.94 ns
Partner relation 3.44 3.54 3.86 4.23 3.13 2.91 ns
Vasomotor symptoms 3.89 4.18 4.05 4.27 3.76 4.28 ns
Health 8.53 5.61 9.11 5.67 8.10 5.55 ns
Aging 7.21 5.26 7.77 5.58 6.79 5.9 ns
*SE = standard error
†Comparison between health and education sector ns = not signiicant
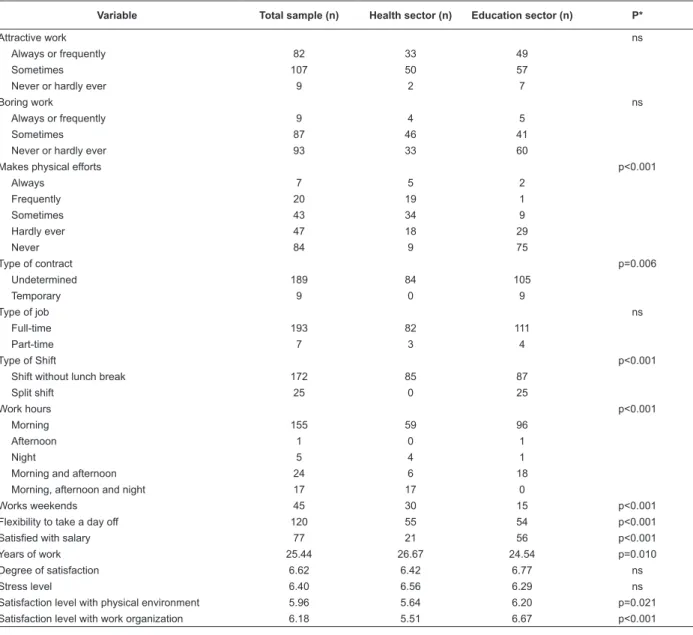
The scores obtained for climacteric women’s
work-related quality of life (Table 3) highlighted that both
stress levels and degrees of satisfaction with their
work were very similar between health and education
sectors (“liking the job” and “job stability” are the most
expressed motives). Signiicant differences were found,
though, with regard to satisfaction levels related to
physical environment and work organization variables.
In both cases, expressed satisfaction levels were higher
among women in the education sector. In comparison
with women working in health institutions, about 90%
of women working in education never made physical
efforts, with signiicant differences.
With regard to the work conditions in both sectors
under analysis (Table 4), higher levels of exposure to
biological (61.6%) and chemical (54.7%) contaminating
agents, vibrations (31.4%) and radiations (25.6%)
Table 3 – Perceived work-related quality of life among climacteric women
Table 4 – Work conditions according to job sector
Variable Total sample (n) Health sector (n) Education sector (n) P*
Attractive work ns
Always or frequently 82 33 49
Sometimes 107 50 57
Never or hardly ever 9 2 7
Boring work ns
Always or frequently 9 4 5
Sometimes 87 46 41
Never or hardly ever 93 33 60
Makes physical efforts p<0.001
Always 7 5 2
Frequently 20 19 1
Sometimes 43 34 9
Hardly ever 47 18 29
Never 84 9 75
Type of contract p=0.006
Undetermined 189 84 105
Temporary 9 0 9
Type of job ns
Full-time 193 82 111
Part-time 7 3 4
Type of Shift p<0.001
Shift without lunch break 172 85 87
Split shift 25 0 25
Work hours p<0.001
Morning 155 59 96
Afternoon 1 0 1
Night 5 4 1
Morning and afternoon 24 6 18
Morning, afternoon and night 17 17 0
Works weekends 45 30 15 p<0.001
Flexibility to take a day off 120 55 54 p<0.001
Satisfied with salary 77 21 56 p<0.001
Years of work 25.44 26.67 24.54 p=0.010
Degree of satisfaction 6.62 6.42 6.77 ns
Stress level 6.40 6.56 6.29 ns
Satisfaction level with physical environment 5.96 5.64 6.20 p=0.021 Satisfaction level with work organization 6.18 5.51 6.67 p<0.001
*Comparison between health and education sector
ns = not signiicant
Variables Total sample (n) Health sector (n) Education sector (n) p*-value
Exposure to biological contaminants 72 53 19 p<0.001
Exposure to noise ns
Very low 57 20 37
Not very high but annoying 81 34 47
High 57 29 28
Comfortable temperature 49 25 24 ns
Exposure to vibrations 34 27 7 p<0.001
Exposure to radiations 25 22 3 p<0.001
Exposure to chemical contaminants 54 47 7 p<0.001
*Comparison between health and education sector
Márquez Membrive J, Granero Molina J, Solvas Salmerón MJ, Fernández Sola C, Rodríguez López CM, Parrón Carreño T.
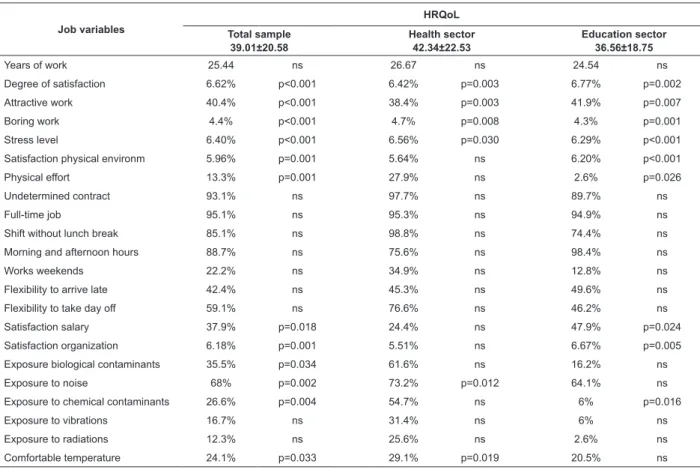
The results of the relation between work variables
and the global HRQoL score in both sectors (Table 5)
show that the nurses who were most satisied with their
work displayed a better quality of life (p=0.003), similar
to those who considered their work attractive (p=0.003),
against worse scores for those who considered it boring
(p=0.008). Both the stress level (p=0.030) and exposure
to noise (p=0.012) determined a worse quality of life, as
opposed to exposure to comfortable temperature at the
workplace, which is related with an increase in these
workers’ perceived quality of life (p=0.019).
As for educational workers, the teachers who
were most satisied with their work (p=0.002) and its
organization (p=0.002) showed better quality of life
scores; the same is true for professionals who considered
their work attractive (p=0.007), against worse scores for
Table 5 – Relation between job variables and global HRQoL scores
those who considered their work was boring (p=0.001).
The teachers who obtained better quality of life scores
indicate lower stress levels and greater satisfaction with
the physical environment of their workplace (p<0.001).
Likewise, signiicant differences in perceived quality of
life were found between teachers who made physical
efforts during their work shift and those who did not
(p=0.026), with lower scores for the former; this extends
to exposure to physical contaminants at the workplace,
which reduces these workers’ perceived quality of life
(p=0.016). The degree of satisfaction with the salary
was also identiied as a determinant of perceived HRQoL (p=0.024), without statistically signiicant differences
when comparing the global score of women working in
health and in education.
Job variables
HRQoL
Total sample 39.01±20.58
Health sector 42.34±22.53
Education sector 36.56±18.75
Years of work 25.44 ns 26.67 ns 24.54 ns
Degree of satisfaction 6.62% p<0.001 6.42% p=0.003 6.77% p=0.002
Attractive work 40.4% p<0.001 38.4% p=0.003 41.9% p=0.007
Boring work 4.4% p<0.001 4.7% p=0.008 4.3% p=0.001
Stress level 6.40% p<0.001 6.56% p=0.030 6.29% p<0.001
Satisfaction physical environm 5.96% p=0.001 5.64% ns 6.20% p<0.001
Physical effort 13.3% p=0.001 27.9% ns 2.6% p=0.026
Undetermined contract 93.1% ns 97.7% ns 89.7% ns
Full-time job 95.1% ns 95.3% ns 94.9% ns
Shift without lunch break 85.1% ns 98.8% ns 74.4% ns
Morning and afternoon hours 88.7% ns 75.6% ns 98.4% ns
Works weekends 22.2% ns 34.9% ns 12.8% ns
Flexibility to arrive late 42.4% ns 45.3% ns 49.6% ns
Flexibility to take day off 59.1% ns 76.6% ns 46.2% ns
Satisfaction salary 37.9% p=0.018 24.4% ns 47.9% p=0.024
Satisfaction organization 6.18% p=0.001 5.51% ns 6.67% p=0.005
Exposure biological contaminants 35.5% p=0.034 61.6% ns 16.2% ns
Exposure to noise 68% p=0.002 73.2% p=0.012 64.1% ns
Exposure to chemical contaminants 26.6% p=0.004 54.7% ns 6% p=0.016
Exposure to vibrations 16.7% ns 31.4% ns 6% ns
Exposure to radiations 12.3% ns 25.6% ns 2.6% ns
Comfortable temperature 24.1% p=0.033 29.1% p=0.019 20.5% ns
ns = not signiicant.
HRQoL = health-related quality of life
Discussion
Quality of life is a dificult concept, in view of its
subjective, complex and multidimensional nature,
involving several factors. The nurses’ work conditions,
whether they are teachers or caregivers, are perceived
as determinants of HRQoL(1), in addition to the possible
inluence deriving from physiological changes inherent
in women, like in the case of the climacterium. The
perceived global HRQoL in the study population is higher
than the Spanish means found in other studies that used
the same scale(20). This could be due to the fact that
these studies were developed in the general population
a higher education degree, a factor that is widely related
with quality of life in climacteric women. The results of
our study signal that HRQoL is similar among nurses
and teachers, except in the group of perimenopausal
women, where workers in the education sector score
higher; this derives from the latter’s lower prevalence
of exposure to certain work conditions that negatively
interfere in the perceived quality of life. These data
are in line with other studies(23), in which factors in the
so-called “physical domain”, including the conciliation
between family-professional life, night or shift work
receive the worst scores among health workers. These
scores relect clinical nurses’ lesser satisfaction with the
work organization, perceived salary, physical efforts and
exposure to contaminants; all of these aspects, together
with their hierarchical submission and emotional
exhaustion deriving from patient care, are valued worse
as determinants of HRQoL in more recent studies(24). The
fact that the quality of life in both groups was worse in
the perimenopausal period coincides with other studies
accomplished in the general population(25), given that
this period covers women with irregular menstruation,
in terms of quantity as well as number, and when the
irst symptoms of the climacterium start to appear.
One of the labor factors related with a better
HRQoL in both groups was the consideration of work
as attractive “always or frequently”. Nevertheless, the
igures found are lower than those published in the
Survey of the Ministry of Labor and Social Affairs(21),
which already concluded that a higher percentage of
college graduates consider work more attractive than in
the rest of the population. Similarly, the percentage of
women that never or hardly ever considered work boring
was higher than that published in the same survey(21).
The degree of satisfaction with the work performed was
clearly related with a better perceived HRQoL in both
groups, a fact that has already been appointed in other
publications(18).
The stress developed in the workplace is also
related with a lower perceived HRQoL, among teachers
as well as clinical nurses, although the differences
between the date collected for both groups are smaller
than those informed in other studies(21). The group of
women who worked in health mentioned making more
physical efforts at work. This result is probably related
with the greater mental and psychological effort clinical
nursing make; nevertheless, the association with the
nurses’ referred quality of life was not signiicant.
The present study data constitute an important
source of research hypotheses to continue investigating
the relation between work and quality of life in the
climacterium. The results point towards the need
to inform referral institutions, so that Occupational
Nursing professionals at Occupational Risk Prevention
Services can elaborate speciic health programs for this
population.
Conclusions
The HRQoL of the study population decreases in
the perimenopausal period, but is nevertheless higher
than that of the Spanish general population. Although
the climacteric patterns found among women working in
the health and education sectors are homogeneous, the
HRQoL is higher among women working in education than
in health, with differences that were only signiicant in
the group of perimenopausal women. Working in health
is associated with a lower perceived quality of life, and
job satisfaction is associated with variables related to
the physical environment and work organization. Work
times, conciliation between family and professional life,
physical efforts and exposure to contaminants receive
the worst assessments.
Limitations
These study results need to be interpreted with
caution because, although the sample follows strictly
probabilistic criteria, the reference population was
elected through convenience sampling, which needs
to be taken into account before making any inference.
The Cervantes Scale is a speciic HRQoL measure for
the menopause in Spanish women, whose original was
developed in Spanish and is adapted to the research
context. Any adaption needs to be validated for use in
other contexts.
References
1. Rocha SSL, Felli VEA. Qualidade de vida no trabalho
docente em enfermagem. Rev. Latino-Am. Enfermagem.
2004;12(1):28-35.
2. Blumel JE, Castelo-Branco C, Binfa L, Gramegna G, Tacla
X, Aracena B, et al. Quality of life after the menopause:
a population study. Maturitas. 2000;34(1):17-23.
3. Nisar N, Sohoo NA. Frequency of menopausal
symptoms and their impact on the quality of life of
women: a hospital based survey. Pak J Med Assoc.
2009;59(11):752-6.
4. Yangin Hb, Kukulu K, Sözer Ga. The perception of
menopause among women Turkish. J Women J Aging.
Márquez Membrive J, Granero Molina J, Solvas Salmerón MJ, Fernández Sola C, Rodríguez López CM, Parrón Carreño T.
5. Olozábal JC, Pastor F, Montero J, García R. Adscripción
a los diversos modelos de concebir la menopausia del
personal sanitario de Salamanca. Cuad Med Psicosom
Psiq Enlace. 2000;53:16-26.
6. Forouhari S, Khajehei M, Moattari M, Mohit M, Rad
Ms, Ghaem H. The effect of education and Awareness on
the quality-of-life in postmenopausal women. Indian J
Commun Med. 2010;35(1):109-14.
7. Jiménez de Luque P, Mejías Jiménez A, Avis Alvarado
M, Biota Jiménez P, Sánchez Inchausti F. Altercaciones
en la menopausia. ROL Enferm. 2006;29(4):64-6.
8. Lindh-Astrand L, Forman M, Hammar M, Kjelldren
KI. Women’s conception of the menopausal transition a
qualitative study. J Clin Nurs. 2007;16(3):509-17.
9. Goncalves R, Merighi M. Reflexoes sobre a sexualidade
durante a vivência do climatério. Rev. Latino-Am.
Enfermagem. 2009;17(2):160-6.
10. Gambacciani M, Ciapone M, Cappagli B, Monteleone
P, Benussi C, Bevilacqua G, et al. Effects of low-dose,
continuous combined estradiol and norestisterone acetate
on menopausal quality of life in early postmenopausal
women. Maturitas. 2003;44(2):157-63.
11. Delgado A, Sánchez MC, Galindo I, Pérez C, Duque MJ.
Actitudes de las mujeres ante la menopausia y variables
predictoras. Atención Primaria. 2001;27(1):27-41.
12. Rossella E, Nappi, Esme A, Nijland. Women’s
perception of sexuality the menopause: Outcomes of
a European telephone survey. Eur J Obstet Gynecol
Reproduct Biol. 2008;137(1):10-6.
13. Kowalcek I, Rotte D, Banz C, Diedrich K. Women’s
attitude and perceptions towards menopause in different
cultures: Cross-cultural and intra-cultural comparison of
pre-menopausal and post-menopausal women in Germany
and in Papua New. Maturitas. 2005;51(3):227-35.
14. Dueñas JL, Durán M, Abad P. Calidad de vida en las mujeres
españolas sintomáticas. En Dueñas Díez JL. Climaterio y
calidad de vida. Madrid: Masson; 2001. p. 97-102.
15. Salazar MA, Paravic KT. Desempeño laboral y
climaterio en trabajadoras de instituciones públicas. Rev
Med Chil. 2005;133(3):315-22.
16. Olaolorun FM, Lawoyin A. Experience of menopausal
symptoms by women in an urban community in Ibadan,
Nigeria. Menopause. 2009;16(4):822-30.
17. Lee MS, Kim JH, Park MS, Yang YH, Ko SD, Joe SH.
Factors influencing the severity of menopause symptoms
in Korean post-menopausal women. J Korean Med Sci.
2010;25(5):758-65.
18. Dennerstein L, Dudley L, Guthrie E, Barrett-Connor
J. Life satisfaction, symptoms, and the menopausal
transition. Medscape Women’s Health. 2000;5(4):E4.
19. Im EO, Meleis AI. Women’s work and symptoms
during midlife: Korean immigrant women. Women’s
Health. 2001;33(1-2):83-103.
20. Palacios S, Ferrer Barriendos J, Parrilla JJ,
Castelo-Branco C, Manubens M, Alberich X, et al. Calidad de vida
relacionada con la salud en la mujer española durante la
perimenopausia y posmenopausia. Desarrollo y validación
de la Escala Cervantes. Med Clin. 2004;122(6):205-11.
21. Ministerio de Trabajo y Asuntos Sociales (ES).
Encuesta sobre calidad de vida en el trabajo. Madrid:
Ministerio de Trabajo y Asuntos Sociales; 2004.
22. Instituto Nacional de Seguridad e Higiene en el
trabajo. V encuesta nacional de condiciones de trabajo.
Madrid: Instituto Nacional de Seguridad e Higiene en el
trabajo; 2004.
23. Andrades Barrientos L, Valenzuela Suazo S.
Fatores associados a qualidade de vida de enfermeiras
hospitalares chilenas. Rev. Latino-Am. Enfermagem.
2007;15(3):480-6.
24. Ríos Assalvi K, Barbosa DA, Gonçalves A, Belasco
S. Avaliação de qualidade de vida e depressão de
técnicos e auxiliares de enfermagem. Rev. Latino-Am.
Enfermagem. 2010;18(3):413-20.
25. Mishra GD, Brown WJ, Dobson AJ. Physical and
mental health: changes during menopause transition.
Qual Life Res. 2003;12(4):405-12.
Received: Dec. 29th 2010