w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Osteoporosis
in
primary
care:
an
opportunity
to
approach
risk
factors
Angra
Larissa
Durans
Costa
a,
Marcos
Antonio
Custódio
Neto
da
Silva
a,
Luciane
Maria
Oliveira
Brito
a,
Anna
Cyntia
Brandão
Nascimento
a,
Maria
do
Carmo
Lacerda
Barbosa
a,
José
Eduardo
Batista
a,
Geusa
Felipa
de
Barros
Bezerra
a,
Grac¸a
Maria
De
Castro
Viana
a,
Walbert
Edson
Muniz
Filho
a,
Flávia
Castello
Branco
Vidal
a,
Maria
do
Desterro
Soares
Brandão
Nascimento
a,b,∗aUniversidadeFederaldoMaranhão(UFMA),SãoLuís,MA,Brazil
bCentrodeEstudosSuperioresdeCaxias(CESC),Caxias,MA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28March2014 Accepted24March2015
Availableonline17November2015
Keywords:
Climacteric Osteoporosis Riskfactors
a
b
s
t
r
a
c
t
Introduction:Climactericwomenaresusceptibletoanumberofchanges,amongthem
osteo-porosis.Osteoporosisisa diseasecharacterizedbylowbonemassandsusceptibilityto fracture.Currently,thisdiseaseisapublichealthissue,beingnecessarytorecognizeits riskfactors.
Objectives: Identify risk factors related to osteoporosis in women attending PROPIS/
PROEX/UFMA,tracingasocio-demographiccharacterizationandconsideringcommunity lifestyles.
Materialandmethods:Thisisatransversalretrospectiveclinicalwithaquantitativeapproach
studyconductedbetweenMarchandJune2013inSãoLuís-MAwith107womentreatedat theProgramadePráticasdeIntegralidadeemSaúde(PROPIS–IntegralityHealthPractice Program).ThestudywasapprovedbytheUniversityHospitalEthicsCommitteeofUFMA underopinionno.362/07.DataweretabulatedandanalyzedintheepidemiologicalEpi-Info®
software,version3.4.1.
Results:Thebrowncolorwaspredominant,consensualrelationshipsprovedtobea
pro-tective factorand loweducationwasa riskfactor.The averageage ofthe groupwith menopausewas54.1yearsandwithoutmenopausewas31.3years(p<0.0001).The aver-ageageofmenopausewas43.7years.Theirregularmenstrualcyclewasaprotectivefactor. Theaveragenumberofpregnancieswas4.56forthegroupwithmenopauseand2.45for thegroupwithoutmenopause,withmostbirthsoccurringnormally(p<0.0001).Smoking, physicalinactivityandcaffeineintakewereriskfactors,whiletheabsenceofalcoholism andofsodaintakewereprotectivefactorsforthedisease.
∗ Correspondingauthor.
E-mail:[email protected](M.D.S.B.Nascimento).
http://dx.doi.org/10.1016/j.rbre.2015.07.014
Conclusion: ThepatientsfollowedthesocioeconomicanddemographicprofileofMaranhão. Mosthadmenarcheandmenopauseinappropriateperiods,showednopositivefamily his-toryofosteoporosis,didnotusuallydrinkalcohol,weresedentaryandthecaffeineintake washigh.
©2015ElsevierEditoraLtda.Allrightsreserved.
Osteoporose
na
atenc¸ão
primária:
uma
oportunidade
para
abordaros
fatores
de
risco
Palavras-chave:
Climatério Osteoporose Fatoresderisco
r
e
s
u
m
o
Introduc¸ão: Amulherclimatérica,estásusceptívelaumasériedealterac¸ões,dentreelas,a
osteoporose.Aosteoporoseéumadoenc¸acaracterizadapeladiminuic¸ãodamassaósseae susceptibilidadeafraturas.Atualmente,adoenc¸aéumproblemadesaúdepública,sendo necessárioreconhecerseusfatoresderisco.
Objetivos: Identificarfatoresderiscorelacionadosàosteoporoseemmulheresatendidas
peloPROPIS/PROEX/UFMA,caracterizandosócio-demograficamenteeoshábitosdevidada comunidade.
Materialemétodos: Trata-sedeumestudoclínicotransversalretrospectivocomabordagem
quantitativa,realizadoentremarc¸oejunhode2013emSãoLuís-MAcom107mulheres aten-didasnoProgramadePráticasdeIntegralidadeemSaúde(PROPIS).Apesquisafoiaprovada peloComitêdeÉticadoHospitalUniversitáriodaUFMAsobparecer362/07.Osdadosforam tabuladoseanalisadosnoprogramaepidemiológicoEpi-Info®versão3.4.1.
Resultados: Acorpardafoipredominante,auniãoconsensualmostrou-secomofatorde
protec¸ãoea baixaescolaridade foium fatorderisco.A médiadeidade dogrupocom menopausafoide54,1anosedogruposemmenopausa,31,3anos,comp<0,0001.Aidade médiadamenopausafoide43,7anos.Ociclomenstrualirregularfoiumfatordeprotec¸ão.O númeromédiodegestac¸õesfoide4,56paraogrupocommenopausaede2,45paraogrupo semmenopausa,tendoamaioriadospartosocorridodeformanatural,comp<0,0001.O tabagismo,sedentarismoeaingestãodecafeínaforamfatoresderisco,enquantoquea ausênciadeetilismoeaingestãoderefrigerantesconstituíramfatoresdeprotec¸ãoparaa doenc¸a.
Conclusão: AspacientesseguiramoperfilsocioeconômicoedemográficodoMaranhão.A
maioriatevemenarcaemenopausaemperíodoadequado,nãoapresentouhistóriafamiliar positivaparaosteoporose,nãocostumavaingerirbebidasalcoólicas,erasedentáriaeingeria cafeínademasiadamente.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Osteoporosis is a metabolic bone disease characterized by reduced bonemineral density (BMD),with deteriorationof bone microarchitecture, leading to an increase in skeletal fragilityandriskoffracture.1Thediagnosisofosteoporosisis
madebyevaluatingthelumbarspineinAP,proximalfemoral neckand/ortotalfemurandforearm,accordingtothecriteria proposedbytheWorldHealthOrganization(WHO).2
IntheUnitedStates,osteoporosisaffectsabout25million people,involvingmorethan1.3millionfracturesannually.3In
Brazil,theestimatedprojectionsforthenext10yearsreveal thatthenumberofhipfracturesduetoosteoporosis(currently 121,700annualfractures)willreach140,000hipfracturesper yearby2020.4,5
InBrazil,studiesinRecifeshowedaprevalenceof28.8% accordingtotheWHOcriteria.6ArecentstudyinSãoPaulo,
using WHO diagnostic criteria, revealed that 33% of post-menopausal womenhad osteoporosisinlumbarspine and femur.7
Theclinicalpresentationofthediseaseisoftenassociated withfracturesofthespine,hipandwrist;evenwithoutany significantreductioninbonemineraldensityorbone symp-tom,itisalsoconsideredasosteoporosis.8,9Fracturescaused
byosteoporosiscontributetobackpain,reducequalityoflife, andinterferewithactivitiesofdailyliving.9
Severalfactorsareinvolvedinthedevelopmentof osteo-porosis;someofthemcannotbechanged,whilemanyothers canbemodified,reducingthe incidenceofosteoporosis.8,10
Amongotherfactorsthatincreasethechanceofdeveloping osteoporosisthatcannotbechanged,themostrelevantare gender(especiallyfemale),increasingage,shortstature,white and Asian racesand heredity.11 Amongmodifiablefactors,
glucocorticoidsand anticonvulsants),sedentarism,smoking andalcoholabuse.10
Climacterichasastronginfluenceonbonelossinwomen duetothe imbalancebetweenboneformation and resorp-tionaswellasitbeingdeterminedbyadecreaseinestrogen production.12,13
Duetothishugeconcernforwomen’shealth,itisnecessary to recognize the risk factors related to osteoporosis, char-acterizingitsocio-demographicallyandtakinginto account communitylifestyles.
Material
and
methods
Thisisatransversalretrospectiveclinicalwithaquantitative approachstudyconductedbetweenMarchandJune2013in SãoLuís-MA.Thisworkrepresentsananalysisofsecondary datacollectedfromaprojectdatabaseentitled“Family Aggre-gation ofBreast Cancer in São Luís-Maranhão”, integrated withthe ProgramofPractices ofCompletenessand Health (PROPIS)/PROEX/UFMA,whichsupportedthedevelopmentof thisscientificresearch.
Thestudywasconductedbyinterviewingusinga question-naire,inasampleconsistingof107women(between17and 75years),healthy,somewithclinicalsignsofclimacteric (neu-rovegetative,neuropsychiatricorgenital),inwhichriskfactors relatedtoosteoporosiswereobserved.
Theselectionofthesepatientsoccurredbyspontaneous demandamongpeopleassistedbytheProgramofPracticesof CompletenessandHealth(PROPIS)oftheFederalUniversity ofMaranhão(UFMA).
Thecriterionfortheinclusionofpatientsinthestudywas womenlivinginSãoLuís-MAassistedbytheprogramandthe criterionusedfornon-inclusionwaswomenwhodonotlive inSãoLuís-MAbuthadbeenassistedbyPROPIS/UFMA.
Women who met the inclusion criteria were informed aboutthe researchand,afterconsentingto takepart init, signedtheFreeInformedConsentpreviouslyapprovedbythe Ethics Committeeofthe UniversityHospital ofthe Federal UniversityofMaranhão(UFMA)undertheopinionno.362/07. Dataweretabulatedandanalyzedintheepidemiological Epi-Info® software,version3.4.1.Toinvestigatethe
associa-tionamongvariables,theratioofproportionswasused.In continuousvariables,theANOVAtestwasusedandtheresults wereexpressedasmeansandstandarddeviation.Theresults wereexpressed withwholenumbers andpercentages. The variablesthatwereconsideredsignificantpresentedvalueof
p<0.05.
Results
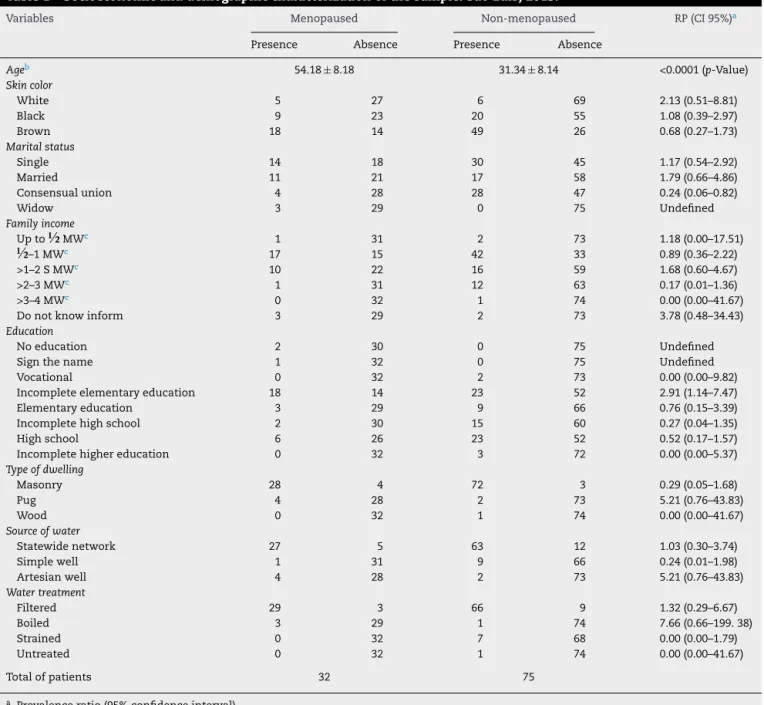
Theanalysisofsocioeconomicanddemographicprofiles of the groups with and without menopause showed no sig-nificantdifference. Thegroups were homogeneous, with a predominanceofbrownskincolor,consensualrelationship proved to be a protective factor and the average monthly incomewasof2–3minimumwages(Table1).
The low level of education proved to be a risk factor; mostpatientslivedinbrickhouses,whosewatersupplywas
providedbythestatewatersupplyandthewaterwasfiltered (Table1).
Considering average age, the people of the group with menopausehad54.1yearsandwithoutmenopausehad31.3 years asaverage,provingit tobeasignificantdatum,with
p<0.0001(Table1).
Regarding sample’s premenopausal characteristics, menarcheinthegroupwithmenopausewas13.6yearsand 13.2yearsinthegroupwithoutmenopause,adifferencenot statisticallysignificant(Table2).
The average age of menopause in the group with menopausewas43.7years,andthemajority(62.5%)occurred naturallyandwithouthormonereplacementtherapy(93.8%). Astomenstrualcycle,theirregulartypeprovedtobea pro-tectivefactor(Table2).
Inbothstudygroups,withandwithoutmenopause,family historyofosteoporosiswasnotasignificantfactor.The major-ityhadanegativefamilyhistoryofosteoporosis(Table2).
Consideringgestationalsamplecharacterization,the aver-age number of pregnancies was 4.56 for the group with menopauseand2.45forthegroupwithoutmenopause,and mostbirthsoccurred naturally.Thisisasignificant datum, withp<0.0001(Table3).
Theanalysisoflifestyleandnutritionalstatusofthe sam-pleshowedthatsmoking,lackofphysicalexerciseandintake ofcaffeineareriskfactorsforosteoporosis,whiletheabsence ofalcoholabuse,aswellastheintakeofsoftdrinksandcanned foodareprotectivefactorsforthedisease(Table4).
Discussion
AccordingtoepidemiologicaldataofEuropeUnionmember states, therewillbechangesinage structure,withamore acuteconcentrationinthe groupwith80 yearsormore.In this group,therewillbeahigherincidenceofosteoporotic fractures.Thispopulationgroupwillincreasefrom8.9million womenand4.5millionmenin1995to26.4millionwomenand 17.4millionmenin2050.14
Literaturedatastatethatosteoporosisisabone-metabolic disease that especially affects women after menopause. According to the World Health Organization, one-third of whitewomenabovetheageof65haveosteoporosis.15
In Brazil,it is noticedthat thereare fewstudies in the literaturethatanalyzetheepidemiologyprofileof osteoporo-sis.AstudyconductedinRecifebyBandeiraetal.6,witha
sample of627women, found anaverage age of63.9 years and a menopause period of 16.2 years. Martini et al. 16,
analyzingpremenopausalwomen,foundaprevalenceof6% of osteoporosisand 33% of postmenopausalwomen. Clark etal.4foundaprevalenceof33.8%ofosteoporosisin
post-menopausalwomen.Theprevalenceofosteoporosisishigher in women with a family income lower than 10 minimum wages.17
Inthisstudy,theprevalenceofosteoporosiswas40%,a sim-ilarresulttothedataofastudywith600patientsevaluated inDetroit,USA,inwhichaprevalenceofosteoporosisof52% wasobserved.17 Thisshowsthattheproblemof
Table1–Socioeconomicanddemographiccharacterizationofthesample.SãoLuís,2013.
Variables Menopaused Non-menopaused RP(CI95%)a
Presence Absence Presence Absence
Ageb 54.18±8.18 31.34±8.14 <0.0001(p-Value)
Skincolor
White 5 27 6 69 2.13(0.51–8.81)
Black 9 23 20 55 1.08(0.39–2.97)
Brown 18 14 49 26 0.68(0.27–1.73)
Maritalstatus
Single 14 18 30 45 1.17(0.54–2.92)
Married 11 21 17 58 1.79(0.66–4.86)
Consensualunion 4 28 28 47 0.24(0.06–0.82)
Widow 3 29 0 75 Undefined
Familyincome
Upto
½
MWc 1 31 2 73 1.18(0.00–17.51)½
–1MWc 17 15 42 33 0.89(0.36–2.22)>1–2SMWc 10 22 16 59 1.68(0.60–4.67)
>2–3MWc 1 31 12 63 0.17(0.01–1.36)
>3–4MWc 0 32 1 74 0.00(0.00–41.67)
Donotknowinform 3 29 2 73 3.78(0.48–34.43)
Education
Noeducation 2 30 0 75 Undefined
Signthename 1 32 0 75 Undefined
Vocational 0 32 2 73 0.00(0.00–9.82)
Incompleteelementaryeducation 18 14 23 52 2.91(1.14–7.47)
Elementaryeducation 3 29 9 66 0.76(0.15–3.39)
Incompletehighschool 2 30 15 60 0.27(0.04–1.35)
Highschool 6 26 23 52 0.52(0.17–1.57)
Incompletehighereducation 0 32 3 72 0.00(0.00–5.37)
Typeofdwelling
Masonry 28 4 72 3 0.29(0.05–1.68)
Pug 4 28 2 73 5.21(0.76–43.83)
Wood 0 32 1 74 0.00(0.00–41.67)
Sourceofwater
Statewidenetwork 27 5 63 12 1.03(0.30–3.74)
Simplewell 1 31 9 66 0.24(0.01–1.98)
Artesianwell 4 28 2 73 5.21(0.76–43.83)
Watertreatment
Filtered 29 3 66 9 1.32(0.29–6.67)
Boiled 3 29 1 74 7.66(0.66–199.38)
Strained 0 32 7 68 0.00(0.00–1.79)
Untreated 0 32 1 74 0.00(0.00–41.67)
Totalofpatients 32 75
a Prevalenceratio(95%confidenceinterval). b Mean±standarddeviation.
c Minimumwage.
riskfactorsinourpopulation.InAsiancountries,the preva-lencewas39.1%,alsosimilartothatfoundinthisstudy.18,19
Astoskincolor,moststudieshavereportedthatthe preva-lenceofosteoporosisandfractureincidencevariesaccording togenderand race.Whitewomenaftermenopause havea higherincidenceoffractures.1,8,15However,astudyconducted
inBaltimore,USA,foundaprevalenceof22%ofosteoporosis inAfrican-Americans,avaluehigherthanexpectedforthis population.20
In relation tomarital status, this study founda higher prevalence of women in stable relationships. Most of the patientshadloweducationanditsdirectrelationtothe preva-lenceofosteoporosiswasnotdefinedinpapers.Thereason probablyistheeffectofeducationonlifestyle,nutritionand economicstatus.21
The influence of hypoestrogenism in the development of osteoporosis is well documented. Thus, studies show that early menopause and delayed menarchehave a dele-terious effect on the development ofthis disease, leading to decreased bone mass in early life, when bone mineral content would be expected to be increased or stabilized. This earlyloss, if sustained forfuture years and not diag-nosed and treated, may lead to osteoporosis and then to an increase of the risk of fractures, which would add greater morbidity and mortality to the underlying disease.22,23
Table2–Characterizationofreproductiveageofthesample.SãoLuís,2013.
Variables Menopaused Non-menopaused RP(CI95%)a
Presence Absence Presence Absence
Menarcheb 13.61±1.45 13.28±1.50 0.2974(p-Value)
Menopauseb 43.71±7.64 – Undefined
Menstrualcycle
Regular 22 10 36 39 2.38(0.92–6.28)
Irregular 9 23 39 36 0.36(0.13–0.96)
Typeofmenopause
Natural 20(62.5%) – Undefined
Surgical 12(37.5%) – Undefined
TRH
Yes 2(6.3%) – Undefined
Not 30(93.8%) – Undefined
Familyhistoryofosteoporosis 5 27 21 54 0.48(0.14–1.54)
Totaldepacients 32 75
TRH,thyrotropin-releasinghormone.
a Prevalenceratio(95%confidenceinterval). b Mean±StandardDeviation.
Table3–Sample’sgestationalcharacterization.SãoLuís,2013.
Variables Menopauseda Non-menopauseda p-Value
Pregnancies 4.56±3.25 2.45±2.12 0.0001
Standarddeliveries 3.62±3.03 1.53±1.79 <0.0001
Cesareanbirths 0.25±0.67 0.36±0.76 0.4820
Spontaneousabortions 0.59±1.10 0.28±0.72 0.0850
Triggeredabortions 0.09±0.39 0.21±0.57 0.2862
Stillbirths 0.06±0.35 0.10±0.45 0.6241
Totalofpatients 32 75
a Prevalenceratio(95%confidenceinterval).
premenopausalwomenconsistofmenstrualdisorders and lowbodyweight.20
Regarding family history of fractures and osteoporosis, mostofthestudiesreportapositiveassociationbetweenthe two,althoughthisstudydidnotshowsignificantdata.8,15,17
Interestingly,thereare noconvincing datainthe litera-ture establishing a direct relation between parity or years
of breastfeeding and osteoporosis.24 In a study conducted
inSaudiArabiatheyfoundasignificantcorrelationbetween havingosteoporosisandincreasingage,fertilityperiod, par-ity, menopausalduration andgynecologicalage(timesince menarcheinyears).25
Withregardtolifestyle,studiesareemphaticwhen stat-ing thatadietlowincalcium andvitaminDisharmfulto
Table4–Characterizationoflifehabitsandnutritionalstatusofthesample.SãoLuís,2013.
Variables Menopaused Non-menopaused RP(CI95%)a
Presence Absence Presence Absence
Smoking 2 30 4 71 1.18(0.14–8.14)
Alcoholism 4 28 32 43 0.19(0.05–0.66)
Exercise 9 23 14 61 1.70(0.58–4.95)
Intakeof:
Milkanddairyproducts 29 3 69 6 0.84(0.17–4.60)
Refrigerantandcanned 18 14 63 12 0.24(0.09–0.68)
Caffeine 21 11 40 35 1.67(0.65–4.32)
Greens 31 1 72 3 1.29(0.11–33.56)
Greenleaves 30 2 68 7 1.54(0.27–11.48)
Meats 31 1 73 2 0.85(0.06–24.62)
Totalofpatients 32 75
thebones,aswellasproteinexcess,fiber(especiallyoatsand spinach)andsodium,aswellasexcessiveintakeofcaffeine andcarbonatedbeverages,whichmayreducecalcium absorp-tionorevenincreaserenalexcretion.8,12,14Onanalyzingthe
soda intakeas aprotector,theseresults maybe explained bythe factthatthepost-menopausalgroupconsumedless refrigerantthanwithoutmenopausegroup.
Furthermore,consumptionofalcoholandsmokingarerisk factorsforosteoporosistotheextentthattheylowerestrogen levelsandfavorboneloss.8,15,17
As for physical exercise, most studies indicate that it is beneficial in that it increases the strength and bone density.8,15,17,23
Althoughthedatainthisstudywerenotstatistically signif-icant,theyfollowthesamepatternpresentedbylargerstudies inscientificliterature.
Thepatientsanalyzed inthis study followed thesocial, economicanddemographicprofileofthestateofMaranhão, thatis,thepatternshowninothernationalandinternational studieswasnotobservedinthisparticularstudy.Thisshows thatosteoporosisisamultifactorialdiseasewithan increas-ingprevalence.Ithasagreatimportancetopublichealthand studieswithalargersamplearenecessarysothatmore sig-nificantcomparisonsaremade.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TotheProgramofPracticesofCompletenessand Healthof theFederalUniversityofMaranhão–PROPIS/UFMAfortheir supportandpartnershipnecessaryfortheimplementationof thisproject.
r
e
f
e
r
e
n
c
e
s
1. PintoNetoAM,SoaresA,UrbanetzAA,SouzaACA,Ferrari AEM,AmaralB,etal.ConsensoBrasileirodeOsteoporose.Rev BrasReumatol.2002;42:343–54.
2. Assessmentoffractureriskanditsapplicationtoscreening forpostmenopausalosteoporosis.WHOtechnicalreport series843,Geneva;1994.
3. FernandesCE,BaracatEC,LimaGR.ClimatérioManualde Orientac¸ãodaFederac¸ãoBrasileiradasAssociac¸õesde GinecologiaeObstetrícia–FEBRASGO.1sted.SãoPaulo: Ponto;2004.
4. ClarkP,Cons-MolinaF,DelezéM,Ragi-EisS,HaddockL, ZanchettaJR,etal.Theprevalenceofvertebralfracturesin LatinAmericancountries:theLatin-AmericanVertebral OsteoporosisStudy(LAVOS).OsteoporosInt.2009;20:275–82.
5. KomatsuRS,RamosLR,SzejnfeldVL.Incidenceofproximal femurfracturesinMarilia,Brazil.JNutrHealthAging. 2004;8:362–7.
6. BandeiraF,CarvalhoEF.Prevalênciadeosteoporoseefraturas vertebraisemmulheresnapós-menopausaatendidasem servic¸osdereferência.RevBrasEpidemiol.2007;10:86–98.
7.PinheiroMM,dosReisNetoET,MachadoFS,OmuraF,Yang JHK,SzejnfeldJ,etal.Riskfactorsforosteoporoticfractures andlowbonedensityinpreandpostmenopausalwomen. RevSaúdePública.2010;44:479–85.
8.FernandesCE.Menopausa:diagnósticoetratamento.1sted. SãoPaulo:Segmento;2003.
9.SatoM,VietriJ,FlynnJA,FujiwaraS.Bonefracturesand feelingatriskforosteoporosisamongwomeninJapan: patientcharacteristicsandoutcomesintheNationalHealth andWellnessSurvey.ArchOsteoporos.2014;9:199.
10.MontillaRNG,MarucciMFN,AldrighiJM.Avaliac¸ãodoestado nutricionaledoconsumoalimentardemulheresno climatério.RevAssocMedBras.2003;49:91–5.
11.Nationalconsensus,proposal.Osteoporosis1995–basic diagnosisandtherapeutic,elements.SãoPauloMedJ. 1995;113:7–18.
12.MontillaRNG,AldrighiJM,MarucciMFN.Relac¸ão
cálcio/proteínadadietademulheresnoclimatério.RevAssoc MedBras.2004;50:52–4.
13.RiggsBL,MeltonLJIII.Involutionalosteoporosis.NEnglJ Med.1986;314:1676–86.
14.LanzilottiHS,LanzilottiRS,TrotteAPR,DiasAS,BornandB, CostaEAMM.Osteoporoseemmulheresnapós-menopausa, cálciodietéticoeoutrosfatoresderisco.RevNutrCampinas. 2003;16:181–93.
15.GaliJC.Osteoporose.ActaOrtopBras.2001;9:53–62.
16.MartiniLA,MouraEC,SantosLC,MaltaDC,PinheiroMM. Prevalênciadediagnósticoautorreferidodeosteoporose, Brasil,2006.RevSaudePublica.2009;43Suppl.2:107–16.
17.FariasFAB.Prevalênciadeosteoporose,fraturasvertebrais, ingestãodecálcioedeficiênciadevitaminaDemmulheres napós-menopausa,vol.189.RiodeJaneiro:EscolaNacional deSaúdePública/CentrodePesquisasAggeu
Magalhães/Fundac¸ãoInstitutoOswaldoCruz(Fiocruz);2003. p.6–7[Tesededoutorado].
18.KimKH,LeeK,KoYJ,KimSJ,OhSI,DurranceDY,etal. Prevalence,awareness,andtreatmentofosteoporosisamong Koreanwomen:theFourthKoreaNationalHealthand NutritionExaminationSurvey.Bone.2012;50:1039–44.
19.SungjoonL,ChunKC,SoHO,SungBaeP.Correlationbetween bonemineraldensitymeasuredbydual-energyX-ray absorptiometryandhounsfieldunitsmeasuredbydiagnostic CTinlumbarspine.JKoreanNeurosurgSoc.2013;54: 384–9.
20.KhanA.Managementoflowbonemineraldensityin premenopausalwomen.JObstetGynaecol.2005;27:345–9.
21.KeramatA,PatwardhanB,LarijaniB,ChopraA,MithalA, ChakravartyD,etal.Theassessmentofosteoporosisrisk factorsinIranianwomencomparedwithIndianwomen.BMC MusculoskeletDisord.2008;9:28.
22.PaivaLC,HorovitzAP,SantosAV,CarvasanGAF,PintoNeto AM.Prevalênciadeosteoporoseemmulheresna
pós-menopausaeassociac¸ãocomfatoresclínicose reprodutivos.RevBrasGinecolObstet.2003;25:507–12.
23.LopesIBF.Reduc¸ãodadensidademineralósseaemmulheres namenarcacomprolactinoma,vol.80.RiodeJaneiro: FaculdadedeMedicina/ProgramadePós-Graduac¸ãoem Endocrinologia/UniversidadeFederaldoRiodeJaneiro;2007. p.1–6[Dissertac¸ão].
24.RochaFAC,JúniorFSS.Osteoporoseegravidez.RevBras Reumatol.2005;45:141–5.