SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Fresh
osteochondral
knee
allografts
in
Brazil
with
a
minimum
two-year
follow-up
夽
Luís
Eduardo
Passarelli
Tírico
∗,
Marco
Kawamura
Demange,
Luiz
Augusto
Ubirajara
Santos,
José
Ricardo
Pécora,
Alberto
Tesconi
Croci,
Gilberto
Luís
Camanho
UniversidadedeSãoPaulo(USP),FaculdadedeMedicina,DepartamentodeOrtopediaeTraumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28March2016 Accepted11April2016
Availableonline28December2016
Keywords:
Kneeinjuries Cartilage,articular
Transplantation,homologous Orthopedics
a
b
s
t
r
a
c
t
Objective:Thepresentstudyaimedtoreporttheresultsofthefirstseriesofcasesoffresh ostechondralallograftsinthekneejointinBrazilwithaminimumfollow-upoftwoyears.
Methods:A protocol of procurement, harvesting, processing, and utilization of fresh osteochondralallograftsinthekneejointwasestablished,beginningwithlegislation mod-ifications,graftharvestingtechniques,immediateprocessing,storageoffreshgrafts,and utilizationoftwosurgicaltechniquesofosteochondraltransplantation.Eightpatientswere treatedandfollowed-upforaminimumoftwoyears.
Results:PatientswereevaluatedwithsubjectiveIKDC,KOOS,andmodifiedMerleD’Aubigne andPostelquestionnaires.MeansubjectiveIKDCscorewas31.99±13.4preoperativeand 81.26±14.7atthelatestfollow-up;preoperativeKOOSscorewas46.8±20.9and postop-erativewas85.24±13.9,indicating asignificant improvementovertime (p<0.01).Mean modified Merle D’Aubigne-Postel score was 8.75±2.25, preoperatively, and 16.1±2.59 postoperatively. Friedman test fornon-parametric samples demonstrated a significant improvementinpostoperativescores(p<0.01).
Conclusion: TheuseoffreshosteochondralallograftsinBrazilisasafeprocedure,withgood clinicalresultsintheshort-andmedium-termforthetreatmentofosteochondrallesions greaterthan4cm2inthekneejoint.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,HospitaldasClínicas,SãoPaulo,SP,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](L.E.Tírico).
http://dx.doi.org/10.1016/j.rboe.2016.12.009
Ortopedia técnicasdecaptac¸ãodeenxertos,processamentoimediato,armazenamentoafrescodos enxertoseusodeduastécnicascirúrgicasdetransplanteosteocondral.Oitopacientesforam transplantadoseacompanhadoscommínimodedoisanosdeseguimento.
Resultados: OspacientesforamavaliadospormeiodosquestionáriosdoInternationalKnee DocumentationCommittee(IKDC)subjetivo,KneeInjuryandOsteoarthritisOutcomeScore(KOOS) eíndicedeMerleD’AubigneePostelmodificado.Amédiadapontuac¸ãodaescalaIKDC sub-jetivapré-operatóriafoide31,99±13,4ede81,26±14,7nopós-operatórioedaescalaKOOS pré-operatóriafoide46,8±20,9ede85,24±13,9nopós-operatório,commelhoria significa-tivaaolongodotempo(p<0,01).Amédiadapontuac¸ãopeloíndicedeMerleD’Aubigne ePostelmodificadofoide8,75±2,25nopré-operatórioede16,1±2,59nopós-operatório. OresultadodotestedeFriedmanparaamostrasnãoparamétricasdemonstroumelhoria significativaaolongodotempo(p<0,01).
Conclusões: OtransplanteosteocondralafresconoBrasiléumprocedimentoseguro,com bonsresultadosclínicosemcurtoemédioprazoparaotratamentodelesõesosteocondrais maioresdoque4cm2naarticulac¸ãodojoelho.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Chondral lesions in the knee joint affect approximately 900,000UScitizenseachyear,resultinginover200,000 sur-gicalproceduresfordiagnosisandtreatment.1Thereareno statisticsonthisdiseaseinBrazil.Thegoalinthetreatment oftraumaticchondralandosteochondrallesionsisto reestab-lishanatomyandfunctionofthe jointaswell aseliminate pain.
The treatment of chondral lesions greater than 4cm2 bydebridement or microfracture techniquesdoes not pro-mote good results, asit does notaddress the subchondral boneinjuryandpromotesrepairwithfibrocartilaginoustissue insteadofhyalinecartilage,thereforenotbeingrecommended forthetreatmentoftheseinjuries.2,3Autologous osteochon-draltransplantationisagoodtreatmentoption,asitpromotes repairwithhyalinecartilageandgraftspossibledefectsofthe subchondralbone.However,itislimitedbythemorbidityof thedonorsite;itcanbeideallyusedininjuriesofupto2.5cm indiameterandupto10mmdeep.4–6
Currently,treatmentoptionsforchondraland osteochon-dralkneelesionslargerthan4cm2areautologouschondrocyte implantationandfreshosteochondralallografts(FOA). Autolo-gouschondrocytetransplantationisacomplextechniquethat requirestwooperationsforbiopsyand celltransplantation, andhasaveryhighcost.7TheuseofFOAforthetreatmentof largeosteochondrallesionsofthekneeisabiologicaloptionin youngpatients;itsmainadvantageisthatitisatissuewithlive hyalinecartilage,featuringchondrocytesinachondralmatrix withpreservedcollagenfiberarchitecture.8,9
Inothercountries, FOAhavebeenusedfordecades.10–14 Thistechniquewas firstintroducedtotreatpost-traumatic bonedefects.15,16However,itisnowusedforthetreatmentof variousdisordersoftheknee,suchasosteochondritis disse-cans(OD),secondaryosteonecrosis,anddegenerativedisease oftheknee,aswellasinfracturesequelae.17–20Theprinciple ofFOAistorestorethebiologicalstructureofthejoint,rebuild thearticularhyalinecartilagesurface,andprovidean osteo-chondraltissuecapableofsupportingthemechanicalloadof theindividual.21,22
Tothebestoftheauthors’knowledge,thereareno stud-iesorcasereportsontheuseoftheFOAtechniqueinBrazil, becauseuntil2009the lawsregulatingtissuebanksdidnot allowfreshtissuestobeusedfortransplantationintimefor thereleaseofcultures;itwasnecessarytowaitfortheresults ofthesetestsbeforeuse.23
Thisstudyaimedtoreporttheresultsofthefirstcasesof FOAtransplantationinthekneejointinBrazil,witha mini-mumfollow-upoftwoyears.
Methods
This study was conducted at the Institute of Orthopedics and Traumatology of this institution and was approved by the Ethics Committee for Research Project Analysis (CAPPesq).
Fig.1–(A)Osteotomyofthefemur10cmabovethejointlinewithoutviolationofthejointcapsule;(B)Tibialosteotomy 2cmbelowtheATT;(C)FinalresultofthepiecebeforetransportationtotheTissueBank.
larger than 4cm2, and whose chondral or osteochondral lesionsfailedprevioustreatmentforarticularcartilagerepair. Patientswithinflammatoryarthropathy,withactive infec-tioninthekneeorelsewhereinthebody,andsmokerswere excluded.
Fordonorselection,theinclusionandexclusioncriteriafor musculoskeletaltissuessetforthbytheBrazilianAssociation of Organ Transplantation (Associac¸ão Brasileira de Trans-plantedeÓrgãos[ABTO])wasused,andindividualsbetween 15and45yearswereselected.
Thesampleconsistedoffiveorgandonorsandeight recipi-ents(eightknees),whichwereoperatedfromMarchtoOctober 2012.
Harvesting
Inthepresentstudy,alltissuesforFOAwereobtainedfrom organdonors,harvestedinanoperatingroomwithlaminar airflowaftertheheart,liverandkidneyhadbeenharvested. Thekneeswereharvestedasablock;onlytheskinand sub-cutaneoustissuewere dissected,andthejoint capsulewas keptintact. Osteotomywas performedon the distalfemur 10cmabovethejointlineandontheproximaltibiaandfibula, 2cmbelowthedistalpartoftheanteriortibialtuberosity(ATT) (Fig.1A–C).
Thepieces, asa block, were placed inlactated Ringer’s solutionandtransportedatatemperatureof2◦–8◦C.After
har-vesting,tissuesweresenttotheTissueBankforprocessing within12hoftheharvestprocedure.
Processing
Theprocessingstagewas performedin aproperoperating room,classifiedasclass100orISO5,and equippedwitha laminarflowmodule.Thearticularcapsuleofthekneewas opened through the medial parapatellar access route and structuresweremeasuredwithacalipertopairwiththe recip-ientsintheFOAlist.Atthisstage,thearticularcartilagewas analyzedandonlypiecesinwhichthisstructurewasintact wereused.
Pairingwasperformedbycomparingtheactualsizeofthe proximaltibiaoftheaffected kneeatthe levelofthejoint inthe donorand inthe recipient. Thismeasurement was obtainedby assessing this receptor segment through digi-talradiographsoftheaffectedkneeinanteroposteriorview,
discountingthemagnification(Fig.2).Inthedonor,this mea-surementwasmadeusingacaliper.Forlesionsoftheproximal portion ofthe tibia, patella, femoraltrochlea, and massive lesionsofthefemoralcondyles,adifferenceofatmost5mm betweenthedonorandrecipientwasusedasaparameterfor matching.Forfocallesionsofthefemoralcondyle,apositive pairingwasmadewhenthe donorcondylewasequaltoor largerthanthatofthereceiver.
Oncedonorandrecipientwerematched,allanalysisexams were performed.Theselectedtissueswerepackedintriple vacuum-sealedpackages,containingapreservationmedium withnutrients.Ittookameanof14daysforthetissuecultures tobereleased;duringthisperiod,thereceiverwasprepared
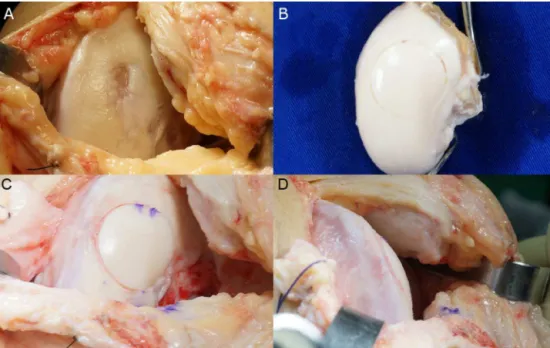
Fig.3–(A)Macroscopicappearanceofosteochondritisdissecanslesionintheleftmedialfemoralcondyle;(B)Donorleft medialfemoralcondylewithacylinderpreparedinthesameanatomicalsiteoftherecipient’sdefect;(C)FOArestoringthe articularsurfaceofthemedialfemoralcondyle;(D)Macroscopiclateralviewofthetransplant,theperfectcongruenceofthe articularsurfaceofthemedialfemoralcondylecanbeobserved.
andthesurgicalprocedurewasscheduledtobeperformedas closeaspossibletothedateofculturerelease.
Storageandpreservation
Themediumusedfortissuepreservationwasthe commer-cialHamF-12– GIBCOwithglutamaxmedium(Invitrogen, Life Technologies, USA), whichcontains aminoacids, vita-mins, and minerals. To the medium, amphotericin B (12.5mg/500mL), streptomycin (50mg/500mL), gentamicin (25mg/500mL), and penicillin G (5,000,000UI/500mL) were addedasprophylaxisagainstmicroorganisms.Tissueswere stored in a refrigerator below 4◦C while awaiting culture
results.
Surgicaltechnique
Surgerywasscheduledforthedayafterculturesrelease,in ordertominimizethetimebetweencollectionand transplan-tation.
Theknees were approachedbymedialor lateral parap-atellararthrotomydependingonthesiteofthelesiontobe transplanted.Forcasesofmultiplelesions,alargearthrotomy wasmade,similartotheincisionfortotalkneearthroplasty, whichfacilitatedtheaccesstoallstructuresandpreservedthe meniscalinsertionsduringtheaccessroute.Inlesionsofthe posteriorcondyle,inwhichtheapproachisdifficult,the ante-riorhornofthemeniscuswascutradially;themeniscuswas shiftedforbetteraccesstoinjury,withsubsequentsuture.
TwotypesofsurgicaltechniquesforFAO wereused:the osteochondralcylindertechnique,inwhichaspecific instru-mentwasusedtopreparetherecipient bedandthe donor graft(BiotechnologyOrtopediaImportac¸ãoeExportac¸ãoLtd.;
Fig.3);andthesurfacetechnique,inwhichboththereceiver andthedonorwerepreparedmanuallywiththeaidofchisels, curettes,andabonesaw(Fig.4).
Thedonorgraftwastakenfromthesameanatomical loca-tionasthelesionintherecipient.Forthis,thetissuebankwas askedforadonorgraftthatcorrespondedtothelesionofthe recipient.
Functionalassessment
Patientswereevaluatedpreoperatively,intraoperatively,and postoperatively through the International Knee Documen-tation Committee (IKDC) 2000 Subjective Knee Evaluation Form,24 the KneeInjury and Osteoarthritis Outcome Score (KOOS),25andtheMerleD’AubigneandPostelScore,modified fortheknee26,27foradetailedassessmentofthelesionandof limbfunction.
Statisticalanalysis
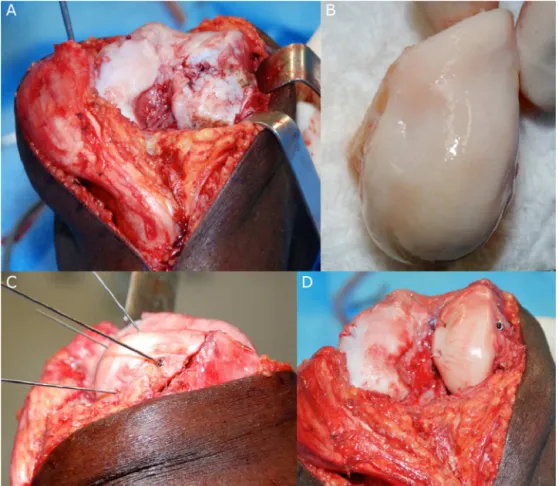
Fig.4–(A)Osteonecrosissequelaeinthelateralfemoralcondyle(LFC)withlateralparapatellaraccessrouteandmedial patellarluxation;(B)LFCofthedonorduringsurgery;(C)Aspectoftheprovisionalfixationofthegraftshowingthe congruenceofthearticularsurface;(D)FinalfixationoftheLFCthatrestorestheanatomyofthejoint.
Forstatisticallysignificantdifferences,atypeIerrorequal toorlowerthan5%wasadopted.SPSSv.20.0softwareforMac wasusedindataanalysis.
Results
EightFOAwereconductedfromMarch2012toOctober2012, from five donors and eight operated knees. Patients were followed-upforatleasttwoyearsaftersurgery(30–37months). FivepatientshadaninitialdiagnosisofOD,onepatienthad post-chemotherapyfemoralcondyle necrosis,and two had post-traumaticsequelae.Themean ageofthetransplanted patientswas 30.1years (17–44)and themean transplanted area was 10.6cm2 (4.6–22.4cm2). Mean number of days betweenharvestingandtransplantationwas15.3(14–16)and meannumberofsurgeriespriortoFOAwastwo(0–4)(Table1). Sixtransplantswereperformedinthefemoralcondyle,onein thetibialplateauwiththemeniscus,andoneinthepatella.
Onepatientwaslosttofollow-upatsixmonths(patient5); inthiscase,alldataofthescoreswerereplacedbytheworst valueamongallpatients,whichcharacterizedtheuseofthe worstcasescenarioandanalysisbyintentiontotreatbynot excludingthispatientfromthestudy.
MeanpreoperativeIKDCsubjectivescorewas31.99±13.4 and 81.26±14.7 postoperatively. Mean preoperative KOOS was 46.8±20.9 and 85.24±13.9 postoperatively. ANOVA
indicatedthatpatientsshowedsignificantimprovementover time,whencomparingpreoperativeandpostoperativeresults (p<0.01).
ThemeanmodifiedMerleD’AubigneandPostelScorefor thekneewas8.75±2.25preoperativelyand16.1±2.59 post-operatively. The Friedman test fornonparametric samples indicatedthatthepatientsshowedsignificantimprovement over time,whencomparing preoperativeand postoperative results(p<0.01).
Discussion
FOAtransplantationinthekneejointwerenotperformeduntil 2009inBrazil,asthelegislationinthecountrydidnotallow thestorageoffreshtissueslongenoughfortheprocedureto beperformedsafely.28Thisstudyisthefirstreporteduseof FOAinSouthAmerica.
AsthefirststudyofFOAinBrazil,onlypatientsbetween15 and45yearsoldwithahistoryoftraumaticoracquiredlesions ofthekneegreater than4cm2 wereincluded, andpatients withdegenerativelesionswereexcluded.
6 LFC 5.2 15 Cylinder 17 OD 2
7 MFC 4.8 16 Cylinder 18 OD 2
8 MFC 13 16 Cylinder 38 OD 2
Har,harvest; LFC, lateralfemoralcondyle; MFC,medial femoral condyle;Fx, fracture; OD, osteochondritisdissecans;post-chem, post-chemotherapy;Tx,transplantation.
ormortuaries.Todate,harvestinginthesefacilitiesinBrazil isnotpossibleduetolegalaspects,whichlimitsthenumber ofgraftsavailablefortransplantation.
Afterbeingharvested,graftsweresentimmediatelytothe tissuebankforprocessing,whichoccurredwithin12hofthe procedure. This agility between harvesting and processing allowedfor a short interval between collection and trans-plantation (15.3 days), a fact that contributes to increased cell viability of the transplanted chondrocytes in cartilage graftswhencomparedwithgraftsstoredforlongerperiods.30 Anotherfactorthatcontributedtotheshorttimebetween har-vestingandtransplantationwasthefactthatallgraftswere harvestedwithina100kmradiusfromthecityofSãoPaulo, withnoneedforairtransportation,whichdecreasedthetime intervalbetweenharvestingandtransplantation.
Transplantswereperformedusingtwosurgicaltechniques: osteochondralcylinderandsurface.Thespecificinstruments fortheosteochondralcylindertechniquewerenotavailable inBrazilatthebeginningofthisstudy;therefore,an instru-mentalsetwasmanufacturedbyanationalcompanyforthe surgicalprocedurewiththistechnique.Inthistechnique,the diameter ofthe osteochondralcylinder ofthe donor must beequalto or 1mm smaller than the recipient bed. How-ever,intheinstrumentsetused,thisdifferencewasslightly greaterthantheoptimum;therefore,itwasnecessaryto fix-atesomegraftswith3-mmcannulatedcompressionscrews, whichwereremovedbyarthroscopy12weeksafter transplan-tation.
Clinicalevaluationsmadethroughobjectiveandsubjective questionnaires(IKDC,KOOS,andmodifiedMerle D’Aubigne andPostel)demonstratedasignificantimprovementbetween thepreoperativeperiodandlastfollow-up(p<0.01).Onlyone patienthadapostoperativecomplicationatfollow-up. This patienthad a historyofmedialtibial plateaufracture that developedacuteinfectionafterfracturefixation;itwastreated withserialsurgicaldebridementandremovalofanyhardware material. Thispatient had a recurrence ofthe prior infec-tion three months after the osteochondral transplantation (threeyearsafterthefracture),withgraftfailure.Radiographic imagesofallotherpatientsshowedincorporationofthegrafts, withoutsubchondralcystformationorgraftcollapse.Patients returnedtotheirdailyactivitiesofworkandleisure,aswellas tolow-impactsports.Thelevelofpatientsatisfactionwiththe procedurewasconsideredhighbyalltransplantrecipients.
Thepresentstudyhasseverallimitations.Ithadasmall sampleofpatients,withashortfollow-upperiod,andwithout acontrolgroupforcomparisonofresults.Anotherlimitationis thefactthattwosurgicaltechniqueswereevaluatedtogether, whichmaypresentdifferentresultsduetothedifferencein thesizeofthegraftsandsurgicaltechnicaldifficulties.
Conclusion
InBrazil,FOAisasafeprocedurewithgoodclinicalresultsin theshortandmediumtermforthetreatmentofosteochondral lesionsofthekneejointlargerthan4cm2.Thisisacomplex procedurethatreliesonadatabaseofspecializedtissuesanda surgicalteamtrainedinharvestingandprocessingthetissue.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TotheteamsoftheTissueBankandtheKneeGroupofthis institutionfortheircooperationwiththepresentstudy.
r
e
f
e
r
e
n
c
e
s
1.ColeB,FrederickRW,LevyAS,ZaslavKR.Managementofa 37-year-oldmanwithrecurrentkneepain.JClinOutcomes Manag.1999;6(6):46–57.
2.AsikM,CiftciF,SenC,ErdilM,AtalarA.Themicrofracture techniqueforthetreatmentoffull-thicknessarticular cartilagelesionsoftheknee:midtermresults.Arthroscopy. 2008;24(11):1214–20.
3.MinasT,NehrerS.Currentconceptsinthetreatmentof articularcartilagedefects.Orthopedics.1997;20(6):525–38.
4.BarthaL,VajdaA,DuskaZ,RahmehH,HangodyL. Autologousosteochondralmosaicplastygrafting.JOrthop SportsPhysTher.2006;36(10):739–50.
5.HangodyL,DobosJ,BaloE,PanicsG,HangodyLR,BerkesI. Clinicalexperienceswithautologousosteochondral
6. MaHL,HungSC,WangST,ChangMC,ChenTH. Osteochondralautograftstransferforpost-traumatic osteochondraldefectoftheknee-2–5yearsfollow-up.Injury. 2004;35(12):1286–92.
7. NiemeyerP,PestkaJM,KreuzPC,ErggeletC,SchmalH, SuedkampNP,etal.Characteristiccomplicationsafter autologouschondrocyteimplantationforcartilagedefectsof thekneejoint.AmJSportsMed.2008;36(11):2091–9.
8. ShermanSL,GarrityJ,BauerK,CookJ,StannardJ,BugbeeW. Freshosteochondralallografttransplantationfortheknee: currentconcepts.JAmAcadOrthopSurg.2014;22(2):121–33.
9. WilliamsRJ3rd,RanawatAS,PotterHG,CarterT,WarrenRF. Freshstoredallograftsforthetreatmentofosteochondral defectsoftheknee.JBoneJointSurgAm.2007;89(4):718–26.
10.AubinPP,CheahHK,DavisAM,GrossAE.Long-termfollowup offreshfemoralosteochondralallograftsforposttraumatic kneedefects.ClinOrthopRelatRes.2001;391Suppl.:S318–27.
11.BugbeeWD.Freshosteochondralallografts.JKneeSurg. 2002;15(3):191–5.
12.GrossAE,ShashaN,AubinP.Long-termfollowupoftheuseof freshosteochondralallograftsforposttraumatickneedefects. ClinOrthopRelatRes.2005;435:79–87.
13.LattermannC,RomineSE.Osteochondralallografts:stateof theart.ClinSportsMed.2009;28(2):285–301.
14.ShashaN,AubinPP,CheahHK,DavisAM,AgnidisZ,Gross AE.Long-termclinicalexperiencewithfreshosteochondral allograftsforarticularkneedefectsinhighdemandpatients. CellTissueBank.2002;3(3):175–82.
15.VolkovM.Allotransplantationofjoints.JBoneJointSurgBr. 1970;52(1):49–53.
16.CzitromAA,LangerF,McKeeN,GrossAE.Boneandcartilage allotransplantation.Areviewof14yearsofresearchand clinicalstudies.ClinOrthopRelatRes.1986;208:141–5.
17.GörtzS,DeYoungAJ,BugbeeWD.Freshosteochondral allograftingforosteochondrallesionsofthetalus.FootAnkle Int.2010;31(4):283–90.
18.GortzS,DeYoungAJ,BugbeeWD.Freshosteochondral allograftingforsteroid-associatedosteonecrosisofthe femoralcondyles.ClinOrthopRelatRes.2010;(468):1269–78.
19.HarrisJD,BrophyRH,SistonRA,FlaniganDC.Treatmentof chondraldefectsintheathlete’sknee.Arthroscopy. 2010;26(6):841–52.
20.GomollAH,FilardoG,AlmqvistFK,BugbeeWD,JelicM, MonllauJC,etal.Surgicaltreatmentforearlyosteoarthritis. PartII:allograftsandconcurrentprocedures.KneeSurg SportsTraumatolArthrosc.2012;20(3):468–86.
21.OssendorfC,SteinwachsMR,KreuzPC,OsterhoffG,LahmA, DucommunPP,etal.Autologouschondrocyteimplantation (ACI)forthetreatmentoflargeandcomplexcartilagelesions oftheknee.SportsMedArthroscRehabilTherTechnol. 2011;3:11.
22.GörtzS,BugbeeWD.Allograftsinarticularcartilagerepair.J BoneJointSurgAm.2006;88(6):1374–84.
23.TiricoLDMK.Ousodotransplanteosteocondralafrescono tratamentodaslesõesosteocondraisdojoelho.RevBras Ortop.2012;47(6):694–700.
24.IrrgangJJ,AndersonAF,BolandAL,HarnerCD,KurosakaM, NeyretP,etal.Developmentandvalidationofthe
internationalkneedocumentationcommitteesubjective kneeform.AmJSportsMed.2001;29(5):600–13.
25.BekkersJE,deWindtTS,RaijmakersNJ,DhertWJ,SarisDB. ValidationoftheKneeInjuryandOsteoarthritisOutcome Score(KOOS)forthetreatmentoffocalcartilagelesions. OsteoarthrCartil.2009;17(11):1434–9.
26.ChuCR,ConveryFR,AkesonWH,MeyersM,AmielD. Articularcartilagetransplantation.Clinicalresultsinthe knee.ClinOrthopRelatRes.1999;(360):159–68.
27.D’AubigneRM,PostelM.Functionalresultsofhip arthroplastywithacrylicprosthesis.JBoneJointSurgAm. 1954;36(3):451–75.
28.Brasil.MinistériodaSaúdeAgênciaNacionaldeVigilância Sanitária.RDCN◦220,27dedezembrode2006.Resoluc¸ãoda DiretoriaColegiada.RDC/ANVISA.2006.Availablefrom:
http://www.saude.mg.gov.br/atos normativos/legislacao- sanitaria/estabelecimentos-de-saude/banco-de-leite-de-sangue-de-celulas-de-cordao-umbilical-e-outros-orgaos. 29.VangsnessCTJr,TriffonMJ,JoyceMJ,MooreTM.Softtissue
forallograftreconstructionofthehumanknee:asurveyof theAmericanAssociationofTissueBanks.AmJSportsMed. 1996;24(2):230–4.