Is age group a predictive factor for satisfaction among
patients undergoing sympathectomy to treat hyperhidrosis?
A idade é um fator preditivo de satisfação entre pacientes
submetidos à simpatectomia para o tratamento da hiper-hidrose?
José Ribas Milanez de Campos1, Nelson Wolosker2, Marco Antonio Soares Munia2, Guilherme Yazbek2, Paulo Kaufman2, Pedro Puech-Leão2, Fábio Biscegli Jatene3
Abstract
Objective: Video-assisted thoracic sympathectomy is currently the procedure of choice for the deinitive treatment of primary hyperhidrosis, because it is an efective, safe, and minimally invasive method. In the search for better quality of life indexes, all researchers look for predictive factors indicating better surgical outcomes. Failure in the primary treatment, postoperative compensatory hyperhidrosis, body mass index over 25, level of resection of the sympathetic chain, and extent of resection are some of the factors that may negatively inluence the results. he objective of this study was to compare, according to the age group, the quality of life after bilateral thoracic sympathectomy for treatment of primary hyperhidrosis in a cohort of 1,644 patients.
Methods: From February 2000 to October 2008, data were collected from 1,644 patients with palmar (71%) or axillary (29%) hyperhidrosis who underwent video-assisted thoracic sympathectomy. he patients were divided into three groups according to their ages. he irst group consisted of patients up to 17 years-old, the second from 18 to 30 years-old, and the third of over 30 years-old. All patients had a body mass index of less than 25.
Results: In the evaluation 30 days after surgery, improvement of the quality of life in the three groups was observed. here was no signiicant diference between the age groups. In the present study, 91.9% of the patients presented compensatory hyperhidrosis, with no diference between the age groups.
Conclusions: Patients with primary hyperhidrosis experience quality of life improvement after thoracic sympathectomy regardless of their age.
Keywords: hyperhidrosis; sympathectomy; quality of life; age.
Resumo
Objetivo: A simpatectomia torácica por videotoracoscopia é atualmente o procedimento de escolha para o tratamento deinitivo da hiper-hidrose palmar, pois é um método eicaz, seguro e minimamente invasivo. Na busca de melhores índices de qualidade de vida, os pesquisadores procuram por fatores preditivos de bom resultado cirúrgico. A falência do tratamento inicial, a hiper-hidrose compensatória, o índice de massa corpóreo acima de 25, o nível de ressecção ganglionar e a extensão da ressecção são alguns dos fatores que podem inluenciar negativamente os resultados. O objetivo deste estudo foi comparar a qualidade de vida dos pacientes submetidos à simpatectomia torácica, de acordo com a faixa etária, numa coorte com 1.644 pacientes.
Métodos: De fevereiro de 2000 a outubro de 2008, foram colhidos dados de 1.644 pacientes portadores de hiper-hidrose palmar (71%) ou axilar (29%), submetidos à simpatectomia torácica por videotoracoscopia. Os pacientes foram divididos em três grupos de acordo com a idade. O primeiro grupo foi de pacientes com até 17 anos, o segundo de 18 a 30 anos, e o terceiro com pacientes com mais de 30 anos de idade. Todos os pacientes tinham índice de massa corpóreo menor que 25.
Resultados: Numa avaliação 30 dias após o procedimento, a melhora da qualidade de vida foi obtida nos três grupos. Não houve diferença estatística entre as diferentes faixas etárias. Neste estudo, 91,9% dos pacientes apresentaram algum grau de hiper-hidrose compensatória, novamente sem diferença entre os grupos.
Conclusões: Pacientes portadores de hiper-hidrose primária apresentam melhora da qualidade de vida após o procedimento cirúrgico independentemente de sua idade.
Palavras-chave: hiper-hidrose; simpatectomia; qualidade de vida; idade.
Study carried out at the Ambulatório de Hiper-hidrose do Hospital das Clínicas da Faculdade de Medicina da USP.
1 Hospital das Clínicas, Heart Institute – Incor, University of São Paulo Medical School. 2 Department of Vascular Surgery, Hospital das Clínicas, University of São Paulo Medical School.
3 Department of horacic Surgery, Hospital das Clínicas, Heart Institute – Incor, University of São Paulo Medical School.
Financial support: none.
Conlict of interest: nothing to declare.
Introduction
Video-assisted thoracic sympathectomy (VATS) is currently the procedure of choice for the definitive treat-ment of primary hyperhidrosis, because it is an effective, safe, and minimally invasive method1. Since the
intro-duction of VATS in the 1990s, this therapeutic modal-ity has been used with increasing frequency, with good results regardless of the patient’s age2. The aim of the
treatment is to improve the quality of life, by reducing excessive sudoresis.
In search of better quality of life indexes, all research-ers look for predictive factors indicating better surgical outcomes. Failure in the primary treatment3, postoperative
compensatory hyperhidrosis4, body mass index over 255,
level of resection of the sympathetic chain, and extent of resection4,5 are some of the factors that may negatively
in-luence the results.
Treatment using VATS of children yields satisfactory results comparable to results obtained with adults6. Only
one article reports a greater postprocedure satisfaction in-dex in a group of young women, linking the result to a lower incidence of compensatory hyperhidrosis7. Speciically
re-garding age, there are no studies that compare objectively the postoperative quality of life of a large group of patients treated by the same surgical team.
he objective of this study was to compare, according to the age group, the quality of life ater bilateral thoracic sympathectomy for treatment of primary hyperhidrosis in a cohort of 1,644 patients.
Patients and Methods
From February 2000 to October 2008, data were col-lected from 1,644 patients with palmar (71%) or axillary (29%) hyperhidrosis who underwent VATS.
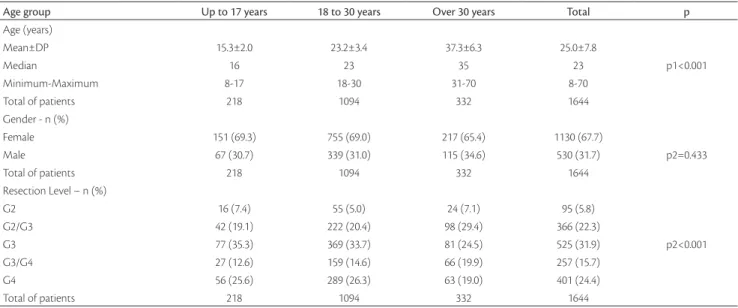
Patients were divided into three groups according to their ages. he irst group consisted of patients up to 17 years-old, the second from 18 to 30 years-old, and the third of over 30 years-old. All the patients had a body mass index of less than 255. he patients’ distribution, according to age
and gender, is presented in Table 1.
All the patients underwent two evaluations for the pur-pose of this study: before the surgery and one month ater it. In each visit, patients were given a clinical protocol to as-sess quality of life2. he incidence and intensity of
compen-satory hyperhidrosis were also studied in the postoperative evaluation.
he protocol for assessment of quality of life adminis-tered to all patients presented daily life situations in which hyperhidrosis might interfere. Quality of life was initially classiied into ive diferent satisfaction levels, which were obtained as the summed total score from the protocol (range from 20 to 100). When the total score was greater than 84, the quality of life was considered very poor; from 69 to 84, poor; from 52 to 68, good; from 36 to 51, very good; and from 20 to 35, excellent. he patients’ postoperative evolu-tions (one month) were classiied into ive diferent satisfac-tion levels, which were calculated as the summed total score from the questionnaire. When the total was greater than 84, the quality of life was considered much worse; from 69 to
Age group Up to 17 years 18 to 30 years Over 30 years Total p
Age (years)
Mean±DP 15.3±2.0 23.2±3.4 37.3±6.3 25.0±7.8
Median 16 23 35 23 p1<0.001
Minimum-Maximum 8-17 18-30 31-70 8-70
Total of patients 218 1094 332 1644
Gender - n (%)
Female 151 (69.3) 755 (69.0) 217 (65.4) 1130 (67.7)
Male 67 (30.7) 339 (31.0) 115 (34.6) 530 (31.7) p2=0.433
Total of patients 218 1094 332 1644
Resection Level – n (%)
G2 16 (7.4) 55 (5.0) 24 (7.1) 95 (5.8)
G2/G3 42 (19.1) 222 (20.4) 98 (29.4) 366 (22.3)
G3 77 (35.3) 369 (33.7) 81 (24.5) 525 (31.9) p2<0.001
G3/G4 27 (12.6) 159 (14.6) 66 (19.9) 257 (15.7)
G4 56 (25.6) 289 (26.3) 63 (19.0) 401 (24.4)
Total of patients 218 1094 332 1644
Table 1. A descriptive analysis of each age group.
84, a little worse; from 52 to 68, the same; from 36 to 51, a little better; and from 20 to 35, much better2.
he statistical test used to evaluate frequency data was the χ2 test. For continuous data (ages), we used ANOVA.
We considered a p≤0.05 to indicate a statistically signiicant diference between groups.
Results
All the patients underwent similar treatment before surgery following the same protocol except for the level of ganglion resection, which varied according to the location of the diaphoresis. he treatment was in accordance with the hospital’s ethical standards as set by the Ethics Committee for Analysis of Research Projects on Human Experimentation.
All participants underwent a bilateral VATS with two 5-mm incisions. he irst incision was made in the fourth submammary intercostal space to introduce the cam-era (30º), and the second was in the second mid-axillary intercostal space to allow for the insertion of surgical instruments8,9. Ablation, with the use of an electrical or
har-monic scalpel, was the chosen technique in all cases. he three groups were similar regarding distribution before surgery by gender, with a predominance of women. here was no signiicant diference regarding the type of surgery performed between patients younger than 17 years-old, and the group between 18 and 30 years-old. he group
of patients over 30 years-old underwent a greater number of G2/G3 and G3/G4 resections than the other two. No mor-tality or conversion to open surgery occurred in this series. he patients’ distribution, according to their postsurgi-cal compensatory hyperhidrosis, is presented in Table 2.
he ratios of compensatory hyperhidrosis occurrence were similar in the three age groups. he intensity of com-pensatory hyperhidrosis according to age is presented in Table 3. We observed that the older the patient, the greater the compensatory hyperhidrosis intensity. he distribution of quality of life in the three groups is presented in Table 4.
All the patients who underwent surgery presented low quality of life in the preoperative period and they were classi-ied in the categories poor or very poor, with predominance of the latter, regardless of the observed age group. here was no signiicant diference between the age groups (Table 4).
he distribution of the quality of life ater 30 days of the surgery is presented in Table 5.
In the evaluation that happened 30 days ater surgery, improvement of the quality of life in the three groups was observed. here was no signiicant diference between the age groups.
Discussion
Surgical treatment of hyperhidrosis with VATS provides a deinitive resolution of the disease and a low incidence of
Age Group Up to 17 years 18 to 30 years Over 30 years Total
Intensity of Compensatory Hyperhidrosis
Mild 57 (32.4%) 291 (31.9%) 73 (26.5%) 421 (30.9%)
Moderate 84 (47.7%) 377 (41.3%) 107 (38.9%) 568 (41.6%)
Severe 35 (19.9%) 245 (26.8%) 95 (34.5%) 375 (27.5%)
Total 176 913 275 1374
Table 3. Intensity of compensatory hyperhidrosis by age group.
p=0.011.
Age group Up to 17 years 18 to 30 years Over 30 years Total
Compensatory hyperhidrosis
Absent 22 (10.9%) 78 (7.7%) 23 (7.5%) 123 (8.1%)
Present 180 (89.1%) 929 (92.3%) 283 (92.5%) 1392 (91.9%)
Total 202 1007 306 1515
Table 2. Compensatory hyperhidrosis by age group.
p=0.299.
Quality of life Up to 17 years 18 to 30 years Over 30 years Total
Poor 48 (22.2%) 301 (27.5%) 85 (25.5%) 434 (26.4%)
Very poor 170 (77.8%) 793 (72.5%) 247 (74.5%) 1210 (73.6%)
Total of patients 218 1094 332 1644
Table 4. Quality of life before surgery, by age group.
compensatory hyperhidrosis, so more and more individuals are being treated at an earlier stage in life. Consequently, a great number of patients in diferent age groups has been treated10,11.
Most patients who seek treatment for hyperhidrosis are young because of the discomfort, discrimination, and social isolation they face due to their condition at this stage of life12.
Since clinical treatment is palliative and it might not gen-erate good results, sympathectomy can be regarded as the best therapeutic alternative. he fear of submitting a child or an adolescent to the surgical procedure, even though it is considered deinitive by the parents, is the reason why most patients undergo surgery only as young adults (between the 18th and 30th year of life).
All the patients in this study came from the same clinic and were treated by the same surgical team, with similar technical criteria being respected for all the groups13. he
level of resection used in each in case was considered the best when the surgeries were performed14, according to
worldwide literature8,11. For example, regarding treatment
for palmar hyperhidrosis, until 2002 it was treated with re-section of thoracic ganglias T2 and T3; in 2003, rere-section of T2 only; from 2004 to 2005, of T3; and as of 2006, of T4. Nevertheless, we were able to obtain good results in the treatment of the disease regardless of the age group, accord-ing to most of the published literature15,16. Among patients
under 30 years of age, there was no diference regarding the level of resection. However, in the patients older than 30, there was a greater prevalence of T2/T3 and T3/T4 resec-tions, which were used in the initial phase of our activity when only older individuals underwent surgery.
We currently know that regardless of the resection level most patients present some degree of compensatory hyper-hidrosis17. In this study, 91.9% of the patients presented any
degree of compensatory hyperhidrosis, with no diference between the age groups.
he intensity of compensatory hyperhidrosis was more severe in the group of individuals over 30 years of age, possibly because of the resection of two thoracic ganglia (T2/T3 and T3/T4), which was done more frequently than in the other groups.
In all the age groups, we observed a female predomi-nance, which can be explained by the greater aesthetic-so-cial concern shown by these patients.
It is well-established in the literature that patients with hyperhidrosis experience a poor quality of life and the surgical outcome depends on the resolution of the symp-toms and severity of compensatory hyperhidrosis, as well as on how the patients adapt to this new condition of life. Although some individuals with mild compensatory hy-perhidrosis may report a very poor quality of life, others, with even a severe case of hyperhidrosis, may report a bet-ter level of quality of life (adapted patients). Herein, we only performed the surgery on patients whose quality of life was classiied as poor or very poor, therefore, any improvement in primary symptoms leads to an increase in quality of life.
In the postoperative period, if no technical complica-tions occurred, there was a substantial improvement in the patients’ daily lives, as indicated not only by the therapeutic success, but also by the satisfaction of the individuals and the improvement in the quality of life in all the age groups, even with the occurrence of compensatory hyperhidrosis18-20.
Generic methods of assessing the quality of life, such as the SF-36, are unable to evaluate changes in the quality of life in the case of certain diseases. he quality of life proto-col that we chose has been validated and used in several re-ported studies, which speciically focused on the symptoms of hyperhidrosis in diferent daily life situations and on how they afected patients’ global quality of life2,10,21,22.
he only factors that are currently associated with worsened quality of life ater surgery are compensatory hy-perhidrosis, when severely manifested, and surgical failure. In this study, we observed that the group over 30 years of age presented greater severity of compensatory hyperhidro-sis but, nevertheless, it did not report a worsened quality of life. his is probably because these patients are in a psycho-logically more stable phase in life, and for this same reason are able to better understand the possible complication and endure it better.
In an attempt to search for new prognostic factors, we analyzed the response to the procedure by different age groups and found no significant differences. The
Quality of life Up to 17 years 18 to 30 years Over 30 years Total
Much better 147 (67.3%) 634 (57.9%) 241 (72.7%) 1022 (68.8%)
Slightly better 57 (26.2%) 414 (37.8%) 71 (21.3%) 542 (26.3%)
he same 10 (4.6%) 28 (2.6%) 16 (4.8%) 54 (3.3%)
Slightly worse 3 (1.4%) 13 (1.2%) 4 (1.2%) 20 (1.2%)
Much worse 1 (0.5%) 5 (0.5%) 0 (0.0%) 6 (0.4%)
Total of patients 218 1094 332 1644
p=0.395.
same levels of quality of life (far better) in the postopera-tive period were verified in all groups of patients, regard-less of their age. In most cases, this surgery immediately eliminates the patient’s distress very safely21, generating
a high level of satisfaction for most patients regardless of their ages.
Conclusion
Patients with primary hyperhidrosis experience quality of life improvement ater thoracic sympathectomy regard-less of their ages.
References
1. Alric P, Branchereau P, Berthet JP, Leger P, Mary H, Mary-Ane C. Video-assisted thoracoscopic sympathectomy for palmar hyper-hidrosis: results in 102 cases. Ann Vasc Surg. 2002;16:708-13.
2. De Campos JRM, Kaufman P, Werebe E de C, Andrade Filho LO, Wolosker N. Quality of life, before and after thoracic sym-pathectomy: report on 378 operated patients. Ann horac Surg. 2003;76:886-91.
3. Sugimura H, Spratt EH, Compeau CG, Kattail D, Shargall Y. horacoscopic sympathetic clipping for hyperhidrosis: long-term results and reversibility. J horac Cardiovasc Surg. 2009;137:1370-6.
4. Neumayer CH, Bischof G, Függer R, Imhof M, Jakesz R, Plas EG, et al. Eicacy and safety of thoracoscopic sympathectomy for hyper-hidrosis of the upper limb. Results of 734 sympathectomies. Ann Chir Gynaecol. 2001;90:2000-2.
5. de Campos JR, Wolosker N, Takeda FR, Kaufman P, Kuzniec S, Jatene FB, et al. he body mass index and level of resection: predic-tive factors for compensatory sweating after sympathectomy.Clin Auton Res. 2005;15:116-20.
6. Sugimura H, Spratt EH, Compeau CG, Kattail D, Shargall Y. horacoscopic sympathetic clipping for hyperhidrosis: long-term results and reversibility. J horac Cardiovasc Surg. 2009;137:1370-6
7. Araújo CA, Azevedo IM, Ferreira MA, Ferreira HP, Dantas JL, Medeiros AC. Compensatory sweating after thoracoscopic sym-pathectomy: characteristics, prevalence and inluence on patient satisfaction J Bras Pneumol. 2009;35:213-20.
8. Munia MA, Wolosker N, Kaufman P, de Campos JRM, Puech-Leão P. A randomized Trial of T3-T4 versus T4 sympathectomy for iso-lated axillary hyperhidrosis. J Vasc Surg. 2007;45:130-3.
9. de Campos JRM, Kaufman P, Wolosker N, Munia MA, de Campos Werebe E, Andrade Filho LO, et al. Axillary hyperhidrosis: T3/ T4 versus T4 thoracic sympathectomy in a series of 276 cases. J Laparoendosc Adv Surg Tech A. 2006;16:598-603.
10. Munia MA, Wolosker N, Kaufmann P, de Campos JR, Puech-Leão P. Sustained beneit lasting one year from T4 instead of T3-T4 sympathectomy for isolated axillary hyperhidrosis. Clinics. 2008;63:771-4.
11. Wolosker N, Yazbek G, Ishy A, de Campos JR, Kaufman P, Puech-Leão P. Is sympathectomy at T4 level better than at T3 level for treating palmar hyperhidrosis?J Laparoendosc Adv Surg Tech A. 2008;18:102-6.
12. Drott C, Gothberg G, Claes G. Endoscopic transthoracic sympath-ectomy: an eicient and safe method for the treatment of hyper-hidrosis. J Am Acad Dermatol. 1995;33:78-81.
13. Shachor D, Jedeikin R, Olsfanger D, Bendahan J, Sivak G, Freund U. Endoscopic transthoracic sympathectomy in the treatment of pri-mary hyperhidrosis. A review of 290 sympathectomies. Arch Surg. 1994;129:241-4.
14. Lin CC, Wu HH. Lin-Telaranta classiication: the importance of dif-ferent procedures for didif-ferent indications in sympathetic surgery. Ann Chir Gynaecol. 2001;90:161-6.
15. Jafer U, Weedon K, Cameron AEP. Factors afecting outcome following endoscopic thoracic sympathectomy. Br J Surg. 2007;94:1108-12.
16. Leseche G, Castier Y, habut G, Petit MD, Combes M, Cerceau O, et al. Endoscopic transthoracic sympathectomy for upper limb hy-perhidrosis: limited sympathectomy does not reduce postopera-tive compensatory sweating. J Vasc Surg. 2003;37:124-8.
17. Yazbek G, Wolosker N, de Campos JR, Kaufman P, Ishy A, Puech-Leão P. Palmar hyperhidrosis--which is the best level of denerva-tion using video-assisted thoracoscopic sympathectomy: T2 or T3 ganglion? J Vasc Surg. 2005;42:281-5.
18. O’riordain DS, Maher M, Waldron DJ, O’donovan B, Brady MP. Limiting the anatomic extent of upper thoracic sympathec-tomy for primary palmar hyperhidrosis. Surg Gynecol Obstet. 1993;176:151-4.
19. Doblas M, Gutierrez R, Fontcuberta J, Orgaz A, Lopez P, Criado E. horacodorsal sympathectomy for severe hyperhydrosis: posterior bilateral versus unilateral staged sympathectomy. Ann Vasc Surg. 2003;17:97-102.
20. Yazbek G, Wolosker N, Kaufman P, de Campos JR, Puech-Leão P, Jatene FB. Twenty Months of Evolution Following Sympathectomy on Patients with Palmar Hyperhidrosis: Sympathectomy at the T3 Level is Better than at the T2 Level. Clinics (Sao Paulo). 2009;64:743-9.
21. Wolosker N, Yazbek G, Milanez de Campos JR, Kaufman P, Ishy A, Puech-Leão P. Evaluation of plantar hyperhidrosis in patients undergoing video-assisted thoracoscopic sympathectomy. Clin Auton Res. 2007;17:172-6.
22. Amir M, Arish A, Weinstein Y. Impairment in quality of life among patients seeking surgery for hyperhidrosis (excessive sweating). Preliminary results. Isr Psychiatry Relat Sci. 2000;37:25-31.
Correspondence Marco Antonio Munia Rua Joaquim Floriano, 820 – cj 193/194 – Itaim Bibi CEP 04534-000 – São Paulo (SP), Brasil E-mail: [email protected]