www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Prevalence
of
depressive
symptoms
in
patients
with
cleft
lip
and
palate
夽
,
夽夽
Leonardo
Santos
Lima
a,
Gustavo
Silveira
Ribeiro
b,
Sibele
Nascimento
de
Aquino
a,
Fernando
Madalena
Volpe
c,
Daniella
Reis
Barbosa
Martelli
a,
Mário
Sérgio
Oliveira
Swerts
b,d,
Lívia
Maris
Ribeiro
Paranaíba
a,
Hercílio
Martelli
Júnior
a,d,∗aHospitalUniversitárioClementedeFarias,UniversidadeEstadualdeMontesClaros(UNIMONTES),MontesClaros,MG,Brazil bUniversidadeJosédoRosárioVellano(UNIFENAS),Alfenas,MG,Brazil
cFundac¸ãoHospitalardoEstadodeMinasGerais(FHEMIG),BeloHorizonte,MG,Brazil dCentroPró-Sorriso,Alfenas,MG,Brazil
Received29November2013;accepted6July2014 Availableonline7February2015
KEYWORDS
Cleftlip; Cleftpalate; Depression; Child; Adolescent
Abstract
Introduction:Cleftlipand/orpalate(CL/P)representthemostcommoncongenitalanomalies oftheface.
Objective: Toevaluatetheprevalenceofdepressivesymptomsinchildrenandadolescentswith nonsyndromiccleftlipand/orpalate(nsCL/P).
Methods:Weconductedanobservational,case-controlstudy,withacasestudygroupcomposed of61patientswithnsCL/P,aged7---17years,andacontrolgroupof61clinicallynormalpatients. Bothgroupswereselectedatthesameinstitution.
Results:Depressivesymptomswereobservedinthecasegroup(nsCL/P),buttherewereno statisticallysignificantdifferencescomparedtothecontrolgroup.Noassociationwasfound betweenthetwogroups(caseandcontrol)inrelationtosociodemographicvariables:gender, ageandeducation.
Conclusions: Thisstudyidentifiedtheprevalenceofdepressivesymptomsinchildrenand ado-lescents withnsCL/Pfromalocalizedgeographicpopulation, althoughtheresultswere not
夽 Pleasecitethisarticleas:LimaLS,RibeiroGS,deAquinoSN,VolpeFM,MartelliDR,SwertsMS,etal.Prevalenceofdepressivesymptoms inpatientswithcleftlipandpalate.BrazJOtorhinolaryngol.2015;81:177---83.
夽夽
Institution:PostgraduatePrograminHealthSciences,CentrodeCiênciasBiológicasedaSaúde,UniversidadeEstadualdeMontesClaros (UNIMONTES),MontesClaros,MG,Brazil.
∗Correspondingauthor.
E-mail:[email protected](H.MartelliJúnior). http://dx.doi.org/10.1016/j.bjorl.2015.01.004
statisticallysignificantwhencomparedtothecontrolgroup,notjustifyingtheuseofCDI(Child Depression Inventory) asa screening instrument for depressive symptomsin the examined population.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Fissurapalatina; Fendalabial; Depressão; Crianc¸a; Adolescente
Prevalênciadesintomasdepressivosempacientescomfissuraslabiopalatinas
Resumo
Introduc¸ão:Fissuraslabiaise/oupalatinas(FL/Ps)representamasanomaliascraniofaciaismais comuns.
Objetivos: Avaliaraprevalênciadesintomasdepressivosemcrianc¸aseadolescentesnão sin-drômicoscomFL/P(FL/PNS).
Método: Foirealizadoumestudoobservacionaldecaso-controlecomumaamostrapopulacional deconveniência,comumgrupocaso(61pacientescomFL/PNS,tendoidadesentre7a17anos) eumgrupocontrole(61pacientesclinicamentenormais).Ambososgruposforamselecionados namesmaInstituic¸ão.
Resultados: Sintomasdepressivosforamobservadosnogrupocaso(FL/PNS),mas nãohouve diferenc¸as estatisticamentesignificantes quandocomparado como grupo controle. Nãofoi encontradaassociac¸ãoentreosdoisgrupos(casoecontrole)emrelac¸ãoàsvariáveis sociode-mográficas:gênero,idadeeeducac¸ão.
Conclusões:Esteestudoobservouaprevalênciadesintomasdepressivosemcrianc¸ase adoles-centescomFL/PNSdeumapopulac¸ãogeográficalocalizada,emboraosresultadosnãotenham sidoestatisticamentesignificantesquandocomparadocomogrupocontrole,nãojustificando assimautilizac¸ãodoInventáriodeDepressão Infantil(IDI),comoinstrumentorastreadorde sintomasdepressivosnapopulac¸ãoanalisada.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Nonsyndromiclipand/orpalatecleft(NSCL/P)isthemost prevalentcongenitalgeneticdefectofcraniofacialareaand results in anatomical complications and in psychological andbehavioraldisorders.1The incidenceofNSCL/P varies
accordingtogeographiclocation,race andsocioeconomic status,2,3andhasameandistributionofabout1caseper700
livebirths.4TheetiologyofNSCL/Pismultifactorial,
involv-ingseveralgenesandcomplexmoleculareventsthatoccur duringembryogenesis,thatarealsoinfluencedby environ-mentalfactors.5,6
Some studies have suggested an increased risk for the development of psychiatric disorders in children and adolescents with NSCL/P, and have noted abnormal lev-els of depressive symptoms.7---12 The literature contains
population-basedstudiesthatidentifydepressivedisorders inthegeneralpopulation, thatreachaprevalence of10% and an incidence of 2%.13 It is estimated that
approxi-mately5%ofpeopleworldwidehavedepression,andabout 10---25%ofthemmayshowsomedepressiveepisodeduring life.14,15
Theprevalenceofdepressioninchildhoodincreaseswith age, and is approximately 2% overall; it increases pro-gressivelyandat adolescent ages,reaches levelsclose to
adulthood.16 In different regions of the world, including
Brazil, these values range from0.4 to 3.0% for children, and 3.3 to 12.4% for teenagers. These variations can be explained by methodologicaldifferences in sample selec-tionstrategy,aswellasbyculturaldifferences,depending onwherethestudieshavebeenconducted.15---17
Earlydetection of depressive symptomscould indicate social, school or family environment damage,7,8,18 and,
therefore, several methods are used for screening and diagnosis.19,20The ChildDepressionInventory(CDI)isused
toassessdepressivesymptomsinchildrenandadolescents indifferentclinicalandresearchcontexts.19---21Thus,some
studies have shown anassociation between occurrence of this malformation and psychosocial adjustment, suggest-ing greater attention to patients with NSCL/P, including their overall development andintegration withthe social environment.21---24
In addition, psychiatric and psychological support of patientswithNSCL/Pthroughout growthanddevelopment and also throughout the entire periodof rehabilitation is necessary,inordertounderstandtheneedsofpatientsand oftheirparentswhoarefeelingandlivingwitha craniofa-cialmalformation.10,11,23,24 Thus,theaimofthisstudywas
Methods
Weconductedacase---controlobservationalstudy.All par-ticipants wereselectedfrom thesame institution(Centro deReferênciaparaReabilitac¸ãodeAnomaliasCraniofaciais eClínicasOdontológicaseMédicas),inMinasGerais,Brazil. Thecasestudygroupconsistedof61patientswithNSCL/P,
allofthemchildren andteenagersbetween theagesof7 and17;thecontrolgroupconsistedof61clinicallyhealthy individuals(withnegativepersonalorfamilyhistoryfor cra-niofacialchanges or syndromes), in thesame case group. Bothgroupswereselectedbychance,enrollinganadequate numberofsubjectstoequaltheprevioussampling calcula-tionsusedtodeterminethenumberofsubjectsneededfor
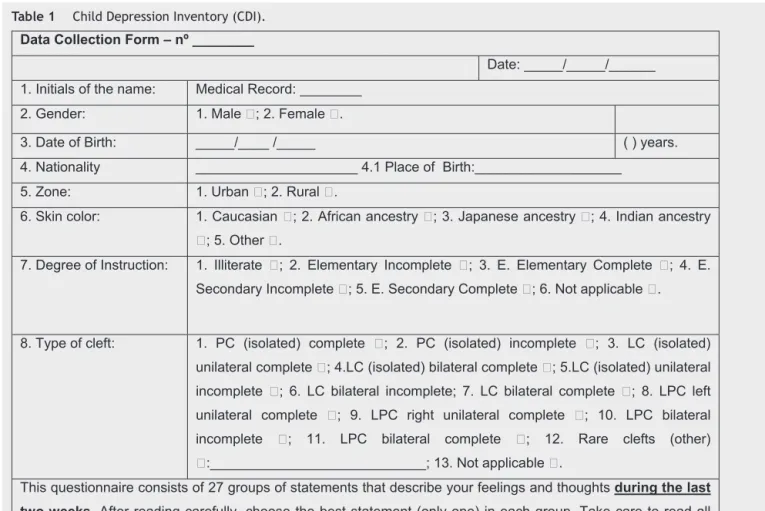
Table1 ChildDepressionInventory(CDI).
Data Collection Form – nº ________
Date: _____/_____/______
1. Initials of the name: Medical Record: ________
. s r a e y ) ( _
_ _ _ _ / _ _ _ _ / _ _ _ _ _ :
h t r i B f o e t a D . 3
4. Nationality _____________________ 4.1 Place of Birth:___________________
7. Degree of Instruction: 1. Illit
This questionnaire consists of 27 groups of statements that describe your feelings and thoughtsduring the last
two weeks. After reading carefully, choose the best statement (only one) in each group. Take care to read all
the statements in each group before making your choice.
1. ( ) I get sad from time to time; ( ) I am sad many times; ( ) I am sad all the time
2. ( ) Nothing will ever work out for me; ( ) I'm not sure if things will work out for me;
( ) All will be fine for me
3. ( ) I do almost everything right; ( ) Many things I do are wrong; ( ) I do everything wrong
4. ( ) I have fun with many things; ( ) I have fun with a few things; ( ) I have no fun with anything
5. ( ) I am bad all the time; ( ) Many times I am bad; ( ) I am bad at one time or another
6. ( ) I think that bad things might happen to me one time or another; ( ) I am worried that bad things would
happen to me; ( ) I am sure that terrible things will happen to me
7. ( ) I hate myself; ( ) I do not like myself; ( ) I like myself
8. ( ) All bad things happen by my fault; ( ) Many bad things happen by my fault; ( ) The bad things usually do not
Table1(Continued)
9. ( ) I do not think about killing myself; ( ) I think about killing myself, but would not do it; ( ) I want to kill myself
10. ( ) I want to cry every day; ( ) Many days I feel like crying; ( ) I want to cry at one time or another
11. ( ) Always there is something bothering me; ( ) Often there is something bothering me; ( ) Once in a while
there's something bothering me
12. ( ) I like being with other people; ( ) I often do not like being with other people; ( ) I have no desire to be with
anyone
13. ( ) I cannot decide on anything; () It is difficult to me to make decisions; ()
I decide myself about things easily
14. ( ) My looks are cool; ( ) There are some things I do not like about my appearance; ( ) I am ugly
15. ( ) I always have to force myself to do my homework; ( ) I often have to force myself to do my homework; ( ) I
have no trouble doing schoolwork
16. ( ) I have trouble sleeping every night; ( ) I often have trouble sleeping; ( ) I sleep well
17. ( ) I get tired once in a while; ( ) In many days I get tired; ( ) I'm always tired
18. ( ) On most days I'm not about to eat; ( ) In many days I'm not about to eat; ( )
I eat well
19. ( ) I do not worry about pain; ( ) I often worry about pain; ( ) I always worry about pain
20 ( ) I do not feel alone; ( ) Many times I feel alone; ( ) I always feel alone
21. ( ) I never have fun at school; ( ) I just have fun at school one time or another;
( ) Many times I have fun at school
22. ( ) I have many friends; ( ) I have many friends, but want more; ( ) I have no friends
23. ( ) My performance in school is good; ( ) My performance in school is not as good as before; ( ) I am going
wrong in matters on which I was good
24. ( ) I will never be as good as others; ( ) If I want I can be as good as others; ( )
I am as good as others
25. ( ) Nobody really loves me; ( ) I am not sure if anybody loves me; () I am sure that somebody loves me
26. ( ) I generally do what they tell me to do; ( ) I generally do not do what they tell me to do; ( ) I never do what
they tell me to do
27. ( ) I get along with people; ( ) Often I get myself into fights; ( ) I get myself into fights all the time
Sum (Total Score): _______
statisticalpurposes.PatientswithCL/Pasonemanifestation ofaclinicalsyndromeandthosewithafamilyhistoryof con-sanguinitywereexcludedfromthestudy.Wecomparedthe prevalence andseverity of depressivesymptoms between groupsbyapplyingCDI,aself-directedandself-explanatory questionnaire.19
This instrument(CDI)(Table1) wasdevelopedin order to detect the presence and severity of depressive symp-tomsinchildrenandadolescentssoastoidentifychangesin mood,selfworth,vegetativefunctionsandself-evaluative andinterpersonalbehaviors.The27itemsofthis question-nairearesummedtoobtainascorethatcanbevalidatedand specificallyreflectthenationalityofthequestionnaire.19,25
Duringtheapplicationofthequestionnaire,eachitemofCDI
wasreadinthepresenceofthepatients toensure under-standingandremoveuncertainties.Thealphavaluewasset at0.5%.Acutoffpoint(score)of17pointshadbeen pre-viously established for statistical significance. The results were comparedusing thechi-squared test and by logistic regressionanalysis.Thisstudywasapprovedbythe Institu-tionalEthicsCommittee(N◦.56/2010).
Results
Table2 Generalcharacteristicsofpatientswithnonsyndromiclipandpalateclefts(casegroup)andwithoutlipandpalate clefts(controlgroup).
Variables Cases Controls Total ORadjusted OR CI95% p
n % n % n %
Gender
Male 29 47.5 27 44.3 56 45.9 1.14 1.13 0.56---2.32 0.716
Female 32 52.5 34 55.7 66 54.1
Age(years)
7---9 23 37.7 21 34.4 44 36.1 1.40 1.38 0.68---2.85 0.364
10---13 20 32.8 26 42.6 46 37.7
14---17 18 29.5 14 23.0 32 26.2
Skincolor
Leukoderma 35 57.4 24 39.3 59 48.3 2.07 2.0 1.00---4.27 0.048
Melanoderma 26 42.6 37 60.7 63 51.7
Depressivesymptoms
Yes 13 21.3 08 13.1 21 17.2 1.80 1.77 0.68---4.70 0.234
No 48 78.7 53 86.9 101 82.8
Total 61 100 61 100 122 100
When the classification of NSCL/P was evaluated for the case group, we found a higher frequency of cleft palate (n=33), with equal distribution for isolated cleft lip and palate(n=14;correspondingto23%foreachinthegroup). Whenthetwogroupswerecompared,thelogisticregression analysisidentifiednoassociation amongsociodemographic variables: gender (p=0.716; OR 1.14; CI 95% 0.56---2.32), age (p=0.364; OR 1.40; CI 95% 0.68---2.85) and schooling (p=0.082;OR3.34;CI95%0.86---13.0).An associationwas detectedforskincolor(p=0.048;OR3.34;CI95%1.0---4.27), meaningthatindividualswithNSCL/P are3.34timesmore likelytobeCaucasians(Table2).
We detected the presence of depressive symptoms in 21.3%, n=13 of the case group (NSCL/P); however, there wasnostatisticalsignificancecomparedtothecontrolgroup (p=0.234,OR1.80,95%CI0.68---4.70)(Table2).Theanalysis ofeachofthe27itemsofCDIidentifiedahomogeneous dis-tributionforthefrequencyofdepressivesymptomsinboth groups.Anassociationforthreeitemswasobserved,when wecomparedthemeanofscores,byCDIsub-items(Table3). Concerningtheitemrelatedtosuicide,itwasobservedthat 8.4%(n=5)ofsubjectsinthecasegroup(nsL/PC)reported somesuicidalthoughtscomparedtoonly1.6%(n=1)inthe controlgroup.
Discussion
Somestudieshavereportedanincreasedriskforthe devel-opmentofpsychiatricdisordersinchildrenandadolescents with NSCL/P, citing abnormally high levels of depressive symptoms.10,11,26---28Ameta-analysisthatincluded340
stud-iesidentifiedhighlevelsofdepressivesymptomsinseveral chronic diseases or conditions, in comparison with nor-malindividuals.28Markeddifferenceswerefoundinchronic
fatiguesyndrome, fibromyalgia, migraine, epilepsyandin CL/P.Thepresenceofthesesymptomswasmoreprevalent in female patients and in individuals living in developing
Table 3 Comparison of mean scores by sub-item ofCDI (p-value,comparisonofmediansbyKruskal---Wallistest)of patientswithnonsyndromiclipandpalatecleft(casegroup) andcontrolpatients(n=122).
Sub-item Cases Controls p
1 0.312 0.213 0.443
2 0.410 0.525 0.223
3 0.267 0.361 0.167
4 0.328 0.360 0.710
5 0.082 0.213 0.065
6 0.738 0.836 0.344
7 0.066 0.131 0.301
8 0.262 0.328 0.278
9 0.393 0.426 0.429
10 0.213 0.213 0.845
11 0.574 0.705 0.356
12 0.262 0.410 0.155
13 0.508 0.508 1.000
14 0.328 0.426 0.278
15 0.951 0.574 0.021a
16 0.148 0.344 0.052
17 0.426 0.492 0.735
18 0.328 0.230 0.671
19 0.820 0.951 0.393
20 0.328 0.262 0.519
21 0.312 0.312 0.656
22 0.295 0.262 0.802
23 0.312 0.377 0.958
24 0.508 0.787 0.044a
25 0.131 0.295 0.039a
26 0.377 0.180 0.094
27 0.164 0.098 0.519
countries.28 In thepresent study,despite thepresence of
depressivesymptomsinthecasegroupwithNSCL/P(21.3%,
n=13), no positive statistical significance was observed, whencomparedwithcontrol group(p=0.234;OR1.80;CI 95%0.68---4.70).Astratifiedanalysisshowednoassociation ofdepressivesymptomsinbothgroups(caseversuscontrol) inthecombinationofvariables,suchasgender(p=0.145) andage(p=0.165).
Itisknownthattheearlydetectionofdepressive symp-tomsisimportantforidentifyinginadvanceanyill-effects on the family, social and school environments7,8,26---28 so
that the application of screening and diagnotic meth-ods can guide the treatment of these patients.19,29 In an
Irish case---control study, the authors compared the pres-enceoffunctional,psychologicaldisorders,suchasanxiety anddepression, andalsobehavioral disorders,among160 children and adolescents with NSCL/P and in 113 normal individuals.30Animportantassociationofchangesin
behav-ior and depressive symptoms in the presence of NSCL/P (p<0.001)wasobserved.Inourstudy,ascoreof17wasused, basedontheadaptationandstandardizationofthis instru-mentinBrazil.26Theanalysisofeachofthe27itemsofCDI
identifiedahomogeneousdistributionof thefrequency of depressivesymptomsinbothgroups,thuswithnopositive association.IntheIrishstudy,withrespecttofacial appear-anceanddifficultywithspeech,patientsweremoreunhappy thancontrols,andhigh suiciderateswereobserved,asin ourstudy,with8.4%(n=5)oftherespondentsin thecase group(NSCL/P),comparedwith1.6% (n=1) inthecontrol group.30 Anotherstudy found a high incidenceof
psycho-logical disordersand difficulties withsocial interactionin patientswithCL/P.10
Withrespecttoclefttype,wefoundhigherratesof prob-lemsrelatedtoanxiety,depression,andlearningandspeech difficultiesinchildrenwithisolatedpalatecleft,compared tochildrenwithbothlipandpalatecleft.31 Inthepresent
study,whencomparingthepresenceofdepressivesymptoms amongpatientsin thecase group(NSCL/P) versuscontrol group,wefoundsimilaritieswiththoseresults,butwithno positivestatistical correlation.Other studiesalsopoint to anassociationbetweentheoccurrenceofthismalformation andpsychosocialadjustment,suggesting greaterattention topatientswithNSCL/P,includingtheiroveralldevelopment andintegrationintothesocialenvironment.29,32---35Although
thisstudywasconductedinareferralcenterfor rehabilita-tionofcraniofacialanomalies,ithassomelimitations,such asthelimitedgeographicarea,i.e.,restrictedtoaportion ofasingleBrazilianstate.Forallanalyzes,alphawas0.05. The sample sizewas sufficientfor the detectionof a dif-ference of twopoints between groups in CDI instrument, consideringacoefficientofvariationof0.5andastatistical powerof0.8.
Although ourresults donotconfirm the findings inthe literature,thisstudysuggeststhatpsychologicaland psychi-atricsupportisneededforpatientswithNSCL/Pthroughout theirgrowthanddevelopment,andthroughoutthe rehabil-itationperiod,inordertounderstandtheneedsofpatients andoftheirfamilieswhoareexperiencingfirsthanda cra-niofacialmalformation.7,8,18,35 We alsoneed toemphasize
that in a limited geographic area and with the method-ologyand tool chosen, the use of ascreening instrument fordepressivesymptomsfor thisgroupofindividuals with
NSCL/P wasnot justifiable.10,11,23,24 Thus, the aim of this
studywastoassesstheprevalenceofdepressivesymptoms inchildrenandadolescentswithNSCL/P.
Conclusion
Theauthorsofthisstudyidentifiedtheprevalenceof depres-sive symptoms in children and adolescents with nsCL/P fromalocalizedgeographicpopulation,althoughtheresults werenotstatisticallysignificantcomparedwiththecontrol group. There was no association of depressive symptoms withsociodemographic variables (gender, age and school-ing). CDI is an instrumentused in variouschronic clinical andgeneticconditions,aimedtoidentifypatientswiththe potentialortheriskofdevelopingdepressivesymptoms.But inthespecificpopulationofthepresent study,wedidnot feelitnecessarytoadoptCDIasascreeninginstrumentfor suchcraniofacialabnormalities.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ThisstudywassupportedbyFundac¸ãodeAmparoàPesquisa do Estado de Minas Gerais --- FAPEMIG; Conselho Nacional deDesenvolvimento Científico eTecnológico --- CNPq; Pro-cad/Casadinho---CNPq/Capes.
References
1.FinnellRH,GreerKA,BarberRC,PiedrahitaJA.Neuraltubeand craniofacialdefectswithspecialemphasisonfolatepathway genes.CritRevOralBiolMed.1998;9:38---53.
2.CobourneMT.Thecomplexgeneticsofcleftlipandpalate.Eur JOrthod.2004;26:7---16.
3.MartelliJúniorH,OrsiJúniorJ,ChavesMR,BarrosLM,BonanPR, FreitasJA.Estudoepidemiológicodasfissuraslabiaisepalatais emAlfenas-MinasGerais-de1986a1998.RPGRevPosGrad. 2006;13:31---5.
4.MosseyPA,LittleJ,MungerRG,DixonMJ,ShawWC.Cleftlip andpalate.Lancet.2009;374:1773---85.
5.Marazita ML. The evolution of human genetic studies of cleft lip and cleft palate. Annu Rev Genomics Hum Genet. 2012;13:263---83.
6.Paranaíba LMR, Bufalino A, Martelli-Júnior H, de Barros LM, Graner E, Coletta RD. Lack of association between polymorphisms (rs2235371 and rs642961) and non-syndromic cleft lip and/or palate in a Brazilian population. Oral Dis. 2010;16:193---7.
7.OkkerseJM,BeemerFA,Cordia-deHaanM,Heineman-deBoer JA, Mellenbergh GJ, Wolters WH. Facial attractiveness and facialimpairmentratingsinchildrenwithcraniofacial malfor-mations.CleftPalateCraniofacJ.2001;38:386---92.
8.SchusterM,KummerP,EysholdtU,RosanowskiF.Social orien-tationofparentsofchildrenwithcleftlipandpalate. HNO. 2003;51:507---12.
9.Hunt O, Burden D, Hepper P, Johnston C. The psychosocial effectsofcleftlipandpalate:asystematicreview.EurJOrthod. 2005;27:274---85.
11.SnyderH,PopeAW. Psychosocialadjustment inchildrenand adolescentswithacraniofacialanomaly:diagnosis-specific pat-terns.CleftPalateCraniofacJ.2010;47:264---72.
12.DemirT,KaracetinG,BaghakiS,AydinY.Psychiatricassessment ofchildren withnonsyndromic cleft lipand palate. General HospitalPsychiatry.2011;33:594---603.
13.RombaldiAJ, SilvaMCD,GazalleFK,AzevedoMR,HallalPC. Prevalênciae fatores associados a sintomas depressivos em adultosdosuldoBrasil:estudotransversaldebasepopulacional [Prevalence of depressive symptoms and associated factors among southern Brazilianadults: cross-sectional population-basedstudy].RevBrasEpidemiol.2010;13:620---9.
14.Mattos Souza LD, Silva RS, Godoy RV, Cruzeiro ALS, Faria AD, Pinheiro RT. Sintomatologia depressiva em adoles-centesiniciais---estudodebasepopulacional.JBrasPsiquiatr. 2008;57:261---6.
15.BahlsSC.Depressivesymptomsinadolescentsofapublicschool. RevBrasPsiquiatr.2002;24:63---7.
16.ÁlvaresADM,LobatoGR.Umestudoexploratóriodaincidência desintomasdepressivosemcrianc¸aseadolescentesem acolhi-mentoinstitucional.TemasemPsicologia.2013;21:151---64. 17.Adewuya AO, Ologum YA. Factors associated with
depres-sive symptoms in Nigerian adolescents. J Adolesc Health. 2006;39:105---10.
18.JohanssonB,RingsbergKC. Parents’experiencesofhavinga childwithcleftlipandpalate.JAdvNur.2004;47:165---73. 19.Kovacs M. The Children’s Depression Inventory (CDI).
Psy-chopharmacolBull.1985;21:995---8.
20.TurnerSR,RumseyN,SandyJR.Psychologicalaspectsofcleft lipandpalate.EurJOrthod.1998;20:407---15.
21.RiveraCL,BernalG,RossellóJ.TheChildrenDepression Inven-tory(CDI)andtheBeckDepressionInventory(BDI):theirvalidity asscreeningmeasuresformajordepressioninagroupofPuerto Ricanadolescents.IntJClinHealthPsychol.2005;5:485---98. 22.GoresteinC,AndradeL.InventáriodedepressãodeBeck:
pro-priedadespsicométricasdaversãoemportuguês.RevPsiqClin. 1998;25:245---50.
23.ChristensenK,JuelK,HerskindAM,MurrayJC.Longtermfollow upofsurvivalassociatedwithcleftlipandpalatebirth.BMJ. 2004;328:1405.
24.MillarK,BellA,BowmanA,BrownD,LoTW,SiebertP,etal. Psychologicalstatusasafunctionofresidualscarringandfacial asymmetryaftersurgicalrepair ofcleftlipandpalate. Cleft PalateCraniofacJ.2011;50:150---7.
25.Gouveia V, Barbosa G, Almeida H, Gaião A. Inventário de DepressãoInfantil---CDI:Estudodeadaptac¸ãocomescolares deJoãoPessoa.JBrasPsiquiatr.1995;44:345---9.
26.LeiteGIC,PaumgartenRJF,KoifmanS.Oralcleftsinthe new-born and medical intakes and maternal health conditions: a case-controlstudyinthecityofRiodeJaneiro,Brasil.RevBras SaúdeMaternInfant.2005;5:35---43.
27.BoesAD,MurkoV,WoodJL,LangbehnDR,CanadyJ,Richman L,etal.Socialfunctioninboyswithcleftlipandpalate: rela-tionshiptoventralfrontalcortexmorphology.BehavBrainRes. 2007;181:224---31.
28.PinquartM,ShenY.Depressivesymptomsinchildrenand adoles-centswithchronicphysicalillness:anupdatedmeta-analysis.J PediatrPsychol.2011;36:375---84.
29.Thurber S, SnowM,Honts CR. The ZungSelf-Rating Depres-sionScale: convergentvalidityanddiagnostic discrimination. Assessment.2002;9:401---5.
30.HuntO,BurdenD,HepperP,StevensonM,JohnstonC. Self-reportsofpsychosocialfunctioningamongchildrenandyoung adults with cleft lip and palate. Cleft Palate Craniofac J. 2006;43:598---605.
31.MillardT,RichmanLC.Differentcleftconditions,facial appear-ance,andspeech:relationshiptopsychologicalvariables.Cleft PalateCraniofacJ.2001;38:68---75.
32.ChristensenK,MortensenPB.Facialcleftingandpsychiatric dis-eases:afollow-upoftheDanish1936-1987FacialCleftcohort. CleftPalateCraniofacJ.2002;39:392---6.
33.LockhartE.Thementalhealthneedsofchildrenand adoles-centswithcleftlipand/orpalate.ClinChildPsycholPsychiatry. 2003;8:7---16.
34.Kapp-SimonKA.Psychologicalissuesincleftlipandpalate.Clin PlastSurg.2004;31:347---52.