Braz. Dent. J. vol.25 número3
Texto
Imagem
Documentos relacionados
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
However, if we take into consideration the different properties of weak hysteresis (hysteresis at the micro level) and strong hysteresis (hysteresis at the macro level),
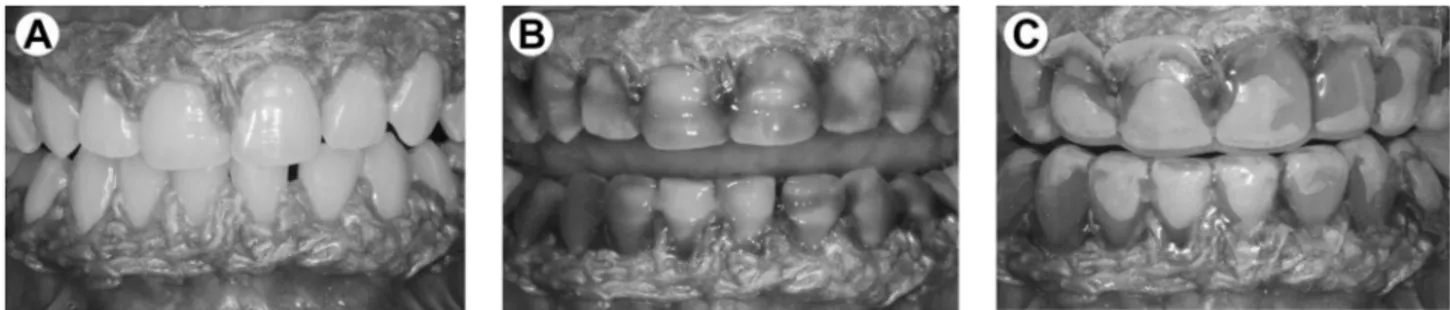
This study evaluated the effects of tooth bleaching with high-concentration of hydrogen peroxide on alterations of translucency parameter (TP) and color of dentin and enamel..
Capítulo 6 - Resultados 128 Considerando a mesma sub-rede de citações entre países, porém aplicando- se um filtro para países europeus, é possível identificar quais
As expected, combined technique resulted in improved bleaching effect since no additional bleaching procedure was performed when only in-office technique was used. Thus, the aim
aimed to evaluate the effects of different desensitizing protocols on the efficacy of in-office bleaching agent and microhardness and chemical composition of human enamel
4611-7/00 Representantes comerciais e agentes do comércio de matérias-primas agrícolas e animais vivos 3 4612-5/00 Representantes comerciais e agentes do comércio de
Assim como no caso de estabilização, a condição de síntese do Teorema 3.1 foi cons- truída de tal forma a conter algumas condições disponíveis na literatura (consideradas as
