w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Prevalence
of
Torque
teno
virus
in
healthy
donors
of
Paraná
State,
southern
Brazil
Jocimara
Costa
Mazzola
a,
Patrícia
Keiko
Saito
a,
Roger
Haruki
Yamakawa
a,
Maria
Angélica
Ehara
Watanabe
b,
Waldir
Veríssimo
da
Silva
Junior
a,
Alessandra
Cristina
Gobbi
Matta
a,
Sueli
Donizete
Borelli
a,∗aUniversidadeEstadualdeMaringá(UEM),Maringá,PR,Brazil
bUniversidadeEstadualdeLondrina(UEL),Londrina,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received21October2013 Accepted2July2015 Availableonline29July2015
Keywords:
Torquetenovirus Blooddonorspolymerase Chainreaction
Anellovirus Virology
a
b
s
t
r
a
c
t
Objective:TodeterminetheprevalenceoftheTorquetenovirusinhealthydonorsinthe
northernandnorthwesternregionsofthestateofParaná,southernBrazil.
Methods:TheTorquetenoviruswasdetectedbyanestedpolymerasechainreactionusing
asetofoligoprimersfortheN22region.
Results:Theprevalenceoftheviruswas69%in551healthyblooddonorsinsouthernBrazil.
Therewasnostatisticallysignificantdifferencebetweenthepresenceofthevirusandthe variablesgender,ethnicityandmaritalstatus.Therewassignificantdifferenceinthe preva-lenceofthevirusregardingtheageofthedonors(p-value=0.024)withahigherincidence (74.7%)in18-to24-year-olddonors.
Conclusion:AhighprevalenceofTorquetenoviruswasobservedinthepopulation
stud-ied.Furtherstudiesareneededtoelucidatetheroutesofcontaminationandtheclinical implicationsofthevirusinthehealthypopulation.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
TheTorquetenovirus(TTV)wasfirstdetectedin1997inthe bloodofJapanesepatientswithpost-transfusionhepatitis.1,2
Theviruswasalsodetectedintheliverandbloodofpeople withhepaticpathologiesofunknownetiology.2 The
associ-ation betweenTTVand liver diseases isstill controversial,
∗ Correspondingauthorat:LaboratóriodeImunogenética,UniversidadeEstadualdeMaringá(UEM),Av.Colombo,5790,Zona07,87020-900
Maringá,PR,Brazil.
E-mailaddresses:[email protected],[email protected](S.D.Borelli).
andseveralstudieshavebeenundertakentoidentifyinfection sources.3–5
Epidemiologicalstudieshaveevidencedtheprevalenceof TTVinotherpathologicalconditions,suchasinautoimmune diseases,4respiratoryconditions6andcancer.7However,
infor-mationisstilllackingonTTVinfectionandthedevelopmentof pathologies,aswellasthechangeinthecourseofaparticular disease.3,5
http://dx.doi.org/10.1016/j.bjhh.2015.07.005
Table1–PrevalenceofTorquetenovirusinhealthypopulationsofdifferentBrazilianstates.
Reference Yearofpublication State Samplestested TTVDNA
n (%)
Nieletal.17 1999 RiodeJaneiro 72 62.0
Bassitetal.18 2002 SãoPaulo 197 85.3
deCastroAmaranteetal.19 2007 SãoPaulo 270 50.5
Pintoetal.20 2007 Pará 186 60.0
Nasseretal.4 2009 Paraná 100 6.0
Costaetal.5 2012 MatoGrossodoSul 46 15.2
Massaúetal.21 2012 RioGrandedoSul 150 73.3
TTV:Torquetenovirus.
Bloodtransfusionwasinitiallyindicatedastheprincipal viaofviraltransmissionduetodirectcontactwith contam-inatedblood.Despite theprogressinpretransfusion safety, bloodrecipientsarenotfreefromriskofcontamination.8
TheserologicaltestsperformedonblooddonorsinBrazil are established bythe nationalhealth surveillance agency (ANVISA),andincludeserologyforHIV1andHIV2,HTLVIand HTLVII,hepatitisB(HBV),hepatitisC(HCV),Trypanosomacruzi
(Chagasdisease),Treponemapallidum(syphilis)andPlasmodium
inendemicareasofmalaria.9
Besidesthe serologicaltestsconductedaccordingtothe MinistryofHealthprotocol,thereisconcernaboutthe emerg-ing and re-emerging diseases that can affect transfusion safety.10
However,new routes oftransmission have been identi-fied,duetothepresenceofthevirus indifferentbiological excretionssuchasinfeces,11saliva12andalsoinriverwater
contaminatedbysewage.13
Currently,wide variabilityin theprevalenceofTTV has beenobservedinhealthypopulationsindifferentcountries, suchasinAlexandriainEgypt(48.4%),14UnitedArabEmirates
(75.0%)15 andIran(13.4%).16 InBraziltheprevalenceofTTV
variesfrom6to85%indifferentstates(Table1).
Several factors may contribute to the variability of the resultsofTTVprevalencestudies,suchasthegeographical distributionofthepopulationunderanalysis,thediagnostic methodused,thesizeofthestudygroupandthedifficultyof makingasinglesetofprimersabletoidentifythemajorityof viralgenotypes.10,15
TTVinfectioniscommoninhealthydonorsworldwide.15,19
KnowledgeoftheprevalenceoftheTTvirusinspecificregions, servesasaresourcetoelucidatethetransmissionroutesand thepossiblecause ofdisease,and mayassistindeveloping guidelinesforactionstocontrolvirustransmissionin popula-tions.Theaimofthisstudywastodeterminetheprevalence ofTTVinhealthydonorsinthenorthernandnorthwestern regionsofParanástate,asthereisalackofstudiesshowing theprevalenceoftheTTVvirusinhealthydonorsinsouthern Brazil.
Methods
Thistransverse quantitativeanalysis involves humanDNA samplesobtainedfromhealthydonorsin2010.Thepopulation comprised551volunteers,agedbetween18and55years.The samplesweregroupedaccordingtothegeographiclocationof
thesource,inoneofthesevenmesoregionsofParanáState, accordingtotheBrazilianInstituteofGeographyandStatistics (IBGE)(Northwest,Central-West,North-Central,theregionof NortePioneiro,Central-Eastern,Mid-SouthandMetropolitan regionofCuritiba)andotherstates.
Anestedpolymerasechainreaction(nestedPCR)with spe-cificprimersfortheN22codifyingregion(ORF1OpenReading Frame1)wasemployedtodetectTTVDNA.Asenseprimer (RD037)followedbyoligonucleotideprimers5′GCAGCAGCA
TATGGATATGT3′andRD038(5′TGACTGTGCTAAGGCCTC
TA3′)wereemployedinthefirstamplification.Theproduct
ofthefirstamplificationandtheantisenseprimersRD0515′
CATACACATGAATGCCAGGC3′andRD0525′GTACTTCTT
GCTGGTGAAAT3′wereusedinthesecondamplification.All
reagentswereidenticalinbothreactionswithafinalvolume of25.0Lcomprisedof2.5LPCRbuffer,0.75L50mM
mag-nesiumchloride(MgCl2),2.0L1.25mMdeoxyribonucleotide
phosphate(dNTP),1.0Lofeachsense(2.5M)andantisense
(2.5M)primer,2.5LTaqDNApolymerase(InvitrogenLife
TechnologiesBrazil),and12.75LsterileMilliQwater.A
fur-ther2.5LgenomicDNAwasusedforthefirstamplification,
and2.5Loftheproductfromthefirstamplificationwasused
forthesecondamplification.Bothreactionsoccurredina ther-mocycler(AppliedBiosystems)devicewithdenaturingat94◦C
for30s,followedby35cyclesat53◦Cfor30sforprimer
anneal-ing,72◦Cfor45sforprimerextension,withafinalextension
at72◦Cfor10min.TheamplifiedDNA productswere
ana-lyzedby2%agarosegelelectrophoresis,stainedwithSYBR®
Safe(1L/10mLgel),andphotographedunderUVlight.The
DNALadder(Invitrogen)consistedof50basepairs(bp)andthe amplifiedDNAproductsof197bp.Alltestsincluded a pos-itive control(TTV genomic DNA).Data were analyzedwith theStatistic7.0computerprogramusingthechi-squaredtest, Yates’scontinuitycorrectionandFisher’sexacttestwith sig-nificance set atalevel of5%.The assaycomplied with all ethicalguidelinesandwasapprovedbytheResearchEthics CommitteeoftheUniversidade EstadualdeMaringá(UEM), Paraná,Brazil(Process271/2011).
Results
Table2–DemographiccharacteristicsandprevalenceofTorquetenovirusamonghealthyblooddonors.
TTV TTV Total p-Value
Positive n(%)
Negative n(%)
Gender 0.785
Male 144(70.0) 62(30.0) 206
Female 236(68.4) 109(31.6) 315
Age(years) 0.024
18–24 124(74.7) 42(25.3) 166
25–38 154(70.3) 65(29.7) 219
39–53 97(63.0) 57(37.0) 154
54–55 5(41.7) 7(58.3) 12
Ethnicbackground 0.999
Caucasian 316(69.0) 142(31.0) 458
Africandescent 64(68.8) 29(31.2) 93
Maritalstatus 0.916
Married 183(68.0) 86(32.0) 269
Single 170(69.7) 74(30.3) 244
Othersa 27(71.1) 11(28.9) 38
TTV:Torquetenovirus.
a Widowed,separated,divorcedorcohabiting.
sociodemographic variables,the proportionofTTV-positive individualsdifferedinrespecttoage(Fisher’sexact test:p -value=0.024),withtheratebeinghigherinthe18–24yearolds. Therewasnostatisticallysignificantdifferenceinthe preva-lence of the virus between gender and ethnic background (p-value>0.05).
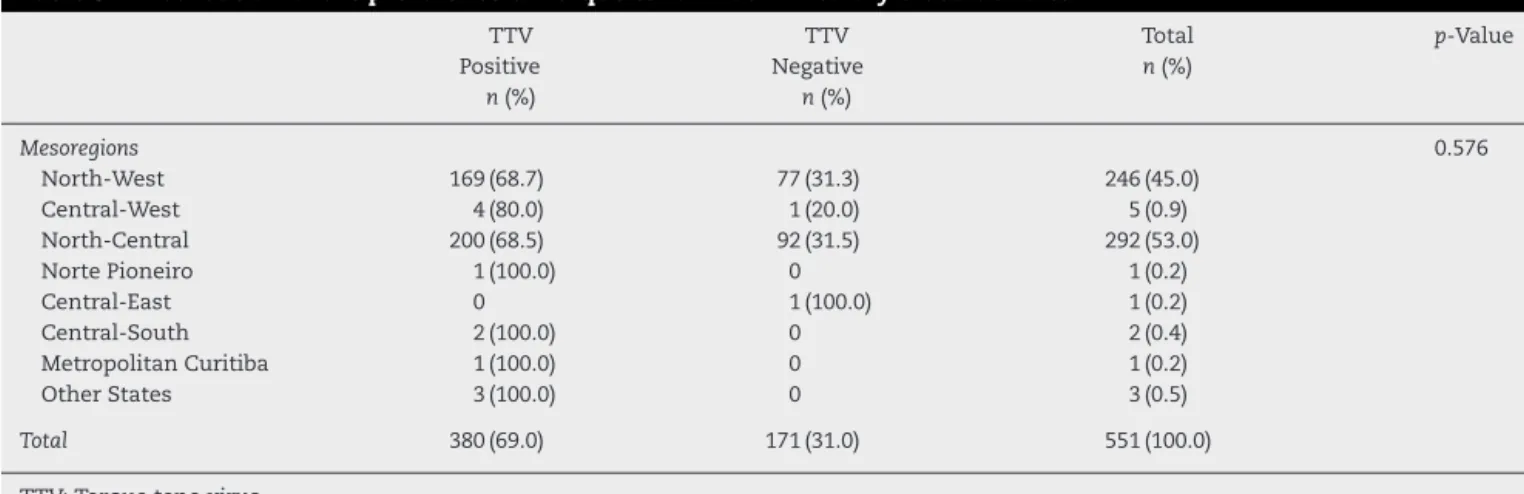
The prevalence of TTV in healthy blood donors was assessedbymesoregionofthestateofParaná,southernBrazil (Table3).Thestatisticstest(ChisquaredwithYatescorrection) indicatednosignificantdifferencesinthepresenceofthevirus andthedifferentmesoregions(p-value=0.576).
Discussion
TheprevalenceofTTVinblooddonorsinthemesoregionsof thestateofParanáinsouthernBrazilwas69%.Other stud-iesinBrazilianpopulationsshowed60%prevalenceinBelém, Pará20and50.5%inthesoutheasternregionofthestateofSão
Paulo.18InsouthernBrazil,studiesshowedahighprevalence
ofthevirusinhealthydonors(73.3%)inthemunicipalityof Pelotas,RS21andalsothepresenceofthevirusinsamplesof
drinkingwaterandsewagewater.13,22
TTVtransmissionbybloodtransfusionhasbeena recur-ringconcernsincethe1990s.1InBrazil,astudyconductedat
auniversityhospitalshowedconcernabouttheriskofviral transmissionbybloodtransfusion,23theserologicalscreening
ofdonorscannotprovidecompleteprotectionfromthe trans-missionofinfectiousagents.
SimilartoTTV, othervirusesrelatedtoliverdamageare overlooked inblood donors,including thehepatitisGvirus (HGV).Somestudies haveshownthe prevalenceofHGVin healthypopulationsofJapan(0.9%)andSouthAfrica(18.9%).24
InBrazilaprevalenceof7.1%wasalsoshowninthestateof Goias25and9.7%inSãoPaulo.26
AlthoughTTVcontamination can occur from both con-taminated blood and blood products,2 there is no specific
legislationthatrequirestestingofblooddonorsforthevirus. Therefore, little isknownabout the routesoftransmission anddiseasesoriginatingfromthepresenceofthevirusinthe humanpopulation.
Based on the results presented, the association of the virus withthestudy variables canbedetermined(Table2). The prevalence of TTVinfection was (380/69%) in healthy donorsfromthenorthernandnorthwesternregionsofParaná, slightlybelowthatfoundinRioGrandedoSul(73.3%)21and
the regionofSãoPaulo(85.3%).18However,oneshouldalso
notethattheprevalenceofthevirusinothercountriesranged from2.7to79.5%.10Thevariablesofgender,race(Caucasian
orAfricandescent),andmaritalstatusshowednostatistical associationwiththepresenceofthevirus.Theresultsofthis studyareinagreementwithotherstudiesthathavesuggested thatTTVinfectionisrelativelycommonindifferent popula-tionsandindifferentregionsoftheworld.1,2
Withrespecttoagegroups,thestudyincludedindividuals between18and55 yearsandrevealedahighprevalenceof infectedyoungpeoplebetween18and24(74.7%).However, it was found thatthe prevalencedeclined inover 24-year-old individuals, especiallythose of 54 and 55 (41.7%).This contrasts with previous studies that showed a cumulative prevalencewithincreasingage,orthepresenceofthevirus independentlyofage.27
Several studies conducted in different countries and individuals in different age groups demonstrated varying prevalencesforTTV.18,28Thediscussionofotheragegroups
islimitedbytheparticularpopulationselectedforthisstudy. The results of this study indicated that the presence of TTVwassignificantlyassociatedwithage(p-value=0.024),in agreementwithastudyinPelotas,southernBrazil.21
Table3–DistributionoftheprevalenceofTorquetenovirusinhealthyblooddonors.
TTV TTV Total p-Value
Positive n(%)
Negative n(%)
n(%)
Mesoregions 0.576
North-West 169(68.7) 77(31.3) 246(45.0)
Central-West 4(80.0) 1(20.0) 5(0.9)
North-Central 200(68.5) 92(31.5) 292(53.0)
NortePioneiro 1(100.0) 0 1(0.2)
Central-East 0 1(100.0) 1(0.2)
Central-South 2(100.0) 0 2(0.4)
MetropolitanCuritiba 1(100.0) 0 1(0.2)
OtherStates 3(100.0) 0 3(0.5)
Total 380(69.0) 171(31.0) 551(100.0)
TTV:Torquetenovirus.
Mostofthedonorswere fromthenorth-centraland
north-westParanámesoregions(98%)withprevalencesof68.5%and 68.7%,respectively.Theseregionsbelongtothe15thRegional HealthDistrictofParanáandreferthecityofMaringa,Parana, Brazil.Abeetal.demonstratedthattheTTVvirusiswidely distributedindifferentregionsoftheplanet,andwithhigh prevalencerates.29
Asisapparentfromtheliterature,severalfactorsmay influ-encethevariabilityofresultsforTTVprevalence,amongthem thegeographicaldistributionofthepopulationsstudied,the diagnosticmethodsofdetection,thesizeofstudygroupsand thesetofprimersusedinthestudy.3,15,28
Thehighratesofviralprevalencemaybedirectlyrelated totheformsofcontamination.Astudyofsamplesofblood andsalivafrom thesame individualsshowedthe presence ofthevirusinthesameproportionsregardlessofthe biolog-icalsampleused.30 Thepresenceofthevirus inwaterhas
beeninvestigatedovertime,andalthoughthepurposeofthe presentstudywasnottodemonstratethepresenceofvirus inenvironmentalsamples,theimportanceofthisanalysisfor studyingtheviralprevalenceinagivenregionisimportant.
StudieshavedetectedTTVin97%ofwatersamples col-lectedinJapan31and inBrazil,in92%ofsamplescollected
fromriversandstreamsinManaus.32Theviralgenomewas
alsoreportedinsamplesofdrinkingwaterinRioGrandedo Sul.13ThepresenceofTTVinthewaterofrivers,lakes,and
treatmentplantsandespeciallyindrinkingwaterhashada majorimpactinspreadingthevirus.Thismayberelatedto thehighprevalenceofthevirusinhealthyindividuals.
Conclusion
ThisstudyfoundahighprevalenceofTTVinhealthyblood donors,inagreementwithotherstudiesintheBrazilian pop-ulation.Theclinicalsignificanceofthepresenceofthevirus inthesedonorscannotbeevaluatedbasedonthisstudy,but canserveasabasisforfuturestudies.Inviewofthe differ-enttransmissionroutesandthelackofcompleteinformation about the pathogenesis ofTTV, it is important to develop measurestominimizethe riskoftransmissionofthis and othervirusesamonghealthcareproviders.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NishizawaT,OkamotoH,KonishiK,YoshizawaH,Miyakawa Y,MayumiM.AnovelDNAvirus(TTV)associatedwith elevatedtransaminaselevelsinposttranfusionhepatitisof unknownetiology.BiochemBiophysResCommun. 1997;241(1):92–7.
2.OkamotoH,NishizawaT,KatoN,UkitaM,IkedaH,IizukaH, etal.MolecularcloningandcharacterizationofanovelDNA virus(TTV)associatedwithposttransfusionhepatitisof unknownetiology.HepatolRes.1998;10(1):1–16.
3.WatanabeMA,MirandaHC,OliveiraKB,OliveiraCE,Tristão FS,DuarteLM,etal.Aspectospatológicos,imunológicose propriedadesmolecularesdoTTvírus.JBrasPatolMedLab. 2005;41(4):223–8.
4.NasserTF,BrajãodeOliveiraK,ReicheEM,AmaranteMK, PelegrinelliFungaroMH,WatanabeMA.DetectionofTTvirus inHIV-1exposedbutuninfectedindividualsandinHIV-1 infectedpatientsanditsinfluenceonCD4+lymphocytesand viralload.MicrobPathog.2009;47(1):33–7.
5.CostaMR,CostaIP,DevalleS,CastroARCM,FreitasSZ. Prevalenceandgeneticdiversityoftorquetenovirusin patientswithsystemiclupuserythematosusinareference serviceinMatoGrossodoSul.RevBrasReumatol.
2012;52(1):49–54.
6.MaggiF,PifferiM,FornaiC,AndreoliE,TempestiniE, VatteroniM,etal.TTvirusinthenasalsecretionofchildren withacuterespiratorydiseases:relationstoviremiaand diseaseseverity.JVirol.2003;77(4):2418–25.
7.GirardC,OttomaniL,DucosJ,DereureO,CarlesMJ,GuillotB. HighprevalenceofTorqueTeno(TT)virusinclassical Kaposi’ssarcoma.ActaDermVenereol.2007;87(1):14–7.
8.CarrazzoneCF,BritoAM,GomesYM.Importânciada avaliac¸ãosorológicapré-transfusionalemreceptoresde sangue.RevBrasHematolHemoter.2004;26(2):93–8.
9.MinistériodaSaúde.AgênciaNacionaldeVigilância Sanitária.Resoluc¸ãodaDiretoriaColegiada(RDC)No153de 14dejulhode2004.Brasília:ANVISA;2004.
11.OkamotoH,AkahaneY,UkitaM,FukudaM,TsudaF, MiyakawaY,etal.FecalexcretionofanonenvelopedDNA virus(TTV)associatedwithposttransfusionnon-A-G hepatitis.JMedVirol.1998;56(2):128–32.
12.NaganumaM,TominagaN,MiyamuraT,SodaA,MoriuchiM, MoriuchiH.TTvirusprevalence,viralloadsandgenotypic variabilityinsalivafromhealthyJapanesechildren.Acta Paediatr.2008;97(12):1686–90.
13.VecchiaAD,FleckJD,ComerlatoJ,KlugeM,BergamaschiB,Da SilvaJV,etal.FirstdescriptionofAdenovirus,Enterovirus, RotavirusandTorquetenovirusinwatersamplescollected fromtheArroioDilúvio,PortoAlegre,Brazil.BrazJBiol. 2012;72(2):323–9.
14.HashishMH,El-BarrawyMA,MahmoudOA,AbdelRahman NW.TTvirusamongblooddonorsinAlexandria.JEgypt PublicHealth.2005;80(5–6):651–64.
15.AlfaresiMS,ElnazerAM,AlzaabiAS,ElkoushAA,IslamAA. TransfusiontransmittedvirusinscreenedUnitedArab Emiratesblooddonors.SaudiMedJ.2006;27(1):58–62.
16.SaraA,SolhjooK,JahromiAR,YaghobiR.Studythe prevalenceofTTvirusinfectioninSouthIranianvolunteer blooddonors.AfrJMicrobiolRes.2012;6(23):5077–81.
17.NielC,deOliveiraJM,RossRS,GomesSA,RoggendorfM, ViazovS.HighprevalenceofTTvirusinfectioninBrazilian blooddonors.JMedVirol.1999;57(3):259–63.
18.BassitL,TakeiK,Hoshino-ShimizuS,NishiyaAS,SabinoEC, BassitRP,etal.NewPrevalenceEstimateofTTvirus(TTV) infectioninlow-andhigh-riskpopulationfromSãoPaulo, Brazil.RevInstMedTropSaoPaulo.2002;44(4):233–4.
19.deCastroAmaranteMF,KashimaS,CovasDT.TTvirus(TTV) genotypinginblooddonorsandmultipletransfusedpatients inBrazil.VirusGenes.2007;35(3):503–9.
20.PintoWV,AssisMF,LemosJA.PrevalênciadoTTVem doadoresdesangue,naregiãometropolitanadeBelém-Pará. CadernoSaúdeColetiva.2007;15(3):349–56.
21.MassaúA,MartinsC,NachtigalGC,AraujoAB,RossettiML, NielC,etal.ThehighprevalenceofTorqueTenoVirusDNAin blooddonorsandhaemodialysispatientsinsouthernBrazil. MemInstOswaldoCruz.2012;107(5):684–6.
22.VecchiaAD,KlugeM,dosSantosdaSilvaJV,ComerlatoJ, RodriguesMT,FleckJD,etal.PresenceofTorquetenovirus (TTV)intapwaterinpublicschoolsfromSouthernBrazil. FoodEnvironVirol.2013;5(1):41–5.
23.SchöningerN,DuroCL.Atuac¸ãodoenfermeiroemservic¸ode hemoterapia.CiêncCuidSaúde.2010;9(2):317–24.
24.SatharMA,SoniPN,YorkD.GBVirusC/HepatitisGVirus (GBV-C/HGV):stilllookingforadisease.IntJExpPathol. 2000;81(5):305–22.
25.OliveiraLA,MartinsRM,CarneiroMA,TelesAS,SilvaAS, CardosoDD,etal.PrevalenceandgenotypesofGBVirus C/HepatitisGvirusamongblooddonorsinCentralBrazil. MemInstOswaldoCruz.2002;97(7):953–7.
26.LeviJE,ContriDG,LimaLP,TakaokaDT,GarriniRH,SantosW, etal.HighprevalenceofGBVirusC/HepatitisGVirusRNA amongBrazilianblooddonors.RevInstMedTropSaoPaulo. 2003;45(2):75–8.
27.HsiehSY,WuYH,HoYP,TsaoKC,YehCT,LianYF.High prevalenceofTTvirusinfectioninhealthychildrenand adultsandinpatientswithliverdiseaseinTaiwan.JClin Microbiol.1999;37(6):1829–31.
28.VasconcelosHC,MenezesME,NielC.TTvirusinfectionin childrenandadultswhovisitedageneralhospitalinthe southofBrazilforroutineprocedure.MemInstOswaldoCruz. 2001;96(4):519–22.
29.AbeK,InamiT,AsanoK,MiyoshiC,MasakiN,HayashiS, etal.TTvirusinfectioniswidespreadinthegeneral populationsfromdifferentgeographicregions.JClin Microbiol.1999;37(8):2703–5.
30.SpandoleS,CimponeriuD,TomaM,RaduI,IonD.Rapid detectionofhumantorquetenovirusesusinghigh-resolution meltinganalysis.BalkanJMedGenet.2013;16(1):55–62.
31.HaramotoE,KatayamaH,OgumaK,YamashitaH,Nakajima E,OhgakiS.One-yearmonthlymonitoringofTorqueTeno Virus(TTV)inwastewatertreatmentplantsinJapan.Water Res.2005;39(10):2008–13.