w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Anatomical
characteristics
of
anal
fistula
evaluated
by
three-dimensional
anorectal
ultrasonography:
is
there
a
correlation
with
Goodsall’s
theory?
Sthela
Maria
Murad-Regadas
a,∗,
Iris
Daiana
Dealcanfreitas
b,
Maura
Tarciany
Coutinho
Cajazeiras
de
Oliveira
c,
David
Pessoa
Morano
d,
Francisco
Sérgio
P.
Regadas
e,
Lusmar
V.
Rodrigues
f,
Graziela
Olivia
da
Silva
Fernandes
b,
Francisco
Sérgio
P.
Regadas
Filho
baDepartmentofSurgery,MedicineSchool,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
bUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
cUniversitySchoolofMedicineHospital,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
dSantaCasadeMisericórdia,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
eDepartmentofDigestiveSystem,MedicineSchool,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
fServiceofColoproctology,MedicineSchool,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received29December2014 Accepted20February2015 Availableonline20April2015
Keywords:
Transsphinctericfistula Goodsall’srule
Three-dimensionalanorectal ultrasonography
a
b
s
t
r
a
c
t
Purpose:Weaimedtocorrelatethecourseoftheanalfistulatract(T),locationoftheexternal opening(EO)andinternalopening(IO)inanterior(A)andposterior(P)circumferenceusing 3D-USaccordingtoGoodsall’srule.
Methods:151patientswithprimarycryptoglandularTranssphinctericfistulaswere exam-inedwith3D-USandcomparedwithsurgicalfinding.ThetypeoftheT(straightorcurved), EOandIOwereidentifiedanddividedinto3Groups:GI:EOandIOarelocatedina posi-tion;GII:EOandIOarelocatedinPpositionandGIII:OEandOIarelocatedintheopposite position.ThefindingswerecorrelatedwithGoodsall’srule.
Results:74/151(49%)wereincludedinGI,ofthem,41(55%)weremale(33/44%hadstraight tract and 8/11% curved) and 33 (45%) female (15/20%-straightand 18/25%-curved). GII included68(45%),ofthem,50(74%)weremale(39/57%-straightand11/15%-curved)and 18(26%)female(14/20%-straightand04/8%-curved).GIII=9(6%)andallofthemhadcurved tract.Theoverallconcordancebetween3D-USandsurgicalfindingwas98%fortractand 96%forIO.
∗ Correspondingauthor.
E-mail:[email protected](S.M.Murad-Regadas). http://dx.doi.org/10.1016/j.jcol.2015.02.006
Conclusion:The3D-USfindingscorrelatewiththeGoodsall’sruleintranssphinctericfistulas locatedintheanteriorcircumferencestraighttype,inmale,whileinfemalesthedistribution ofcurvedandstraightpathsissimilar.Intheposteriorcircumferencenocorrelationwas observedinboththesexes.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Características
anatômicas
da
fístula
anal
avaliadas
por
Ultrassonografia
Anorretal
Tridimensional:
Há
correlac¸ão
com
a
teoria
de
Goodsall?
Palavras-chave:
Fístulatransesfinctérica TeoriadeGoodsall Ultrassonografiaanorretal tridimensional
r
e
s
u
m
o
Objetivo: Correlacionarotrajeto(T)dafístulaanal,localizac¸ãodoorifícioexterno(OE)e orifíciointerno(OI)nahemicircunferênciaanterior(HCA)eposterior(HCP),utilizando 3D-US,comaleideGoodsall.
Método: 151pacientescomfístulastransesfinctéricascriptoglangularesforamexaminados comUS-3Dcorrelacionandocomosachadoscirúrgicos.Identificou-seotipodeT (retilí-neooucurvo),OEeOIedistribuiu-seospacientesem3grupos:GI:OEeOIlocalizadosem HCA;GII:OEeOIlocalizadosemHCPeGIII:OEeOIemposic¸õesopostas.Osachadosforam correlacionadoscomaleideGoodsall.
Resultados: 74/151(49%) incluídos no GI, destes, 41(55%) homens(33/44% com trajeto retilíneo e 8/11% curvo) e 33(45%) mulheres(15/20%-retilíneo e 18/25%-curvo). No GII incluídos 68(45%), destes, 50(74%) homens(39/57%-retilíneo e 11/15%-curvo) e 18(26%) mulheres(14/20%-retilíneoe04/8%-curvo).GIII=9(6%)todosostrajetoscurvos.A concordân-ciaentreoUS-3Deosachadoscirúrgicosfoide98%paratrajetose96%paraoOI. Conclusão: Osachadosultrassonográficospermitiramcorrelacionarfístulas transesfinc-téricascomtrajetos retilíneoslocalizadasnahemicircunferênciaanterior,em homens, enquantoemmulheresadistribuic¸ãodostrajetosemcurvoeretilíneoforamsimilares. Nahemicircunferênciaposteriornãohouvecorrelac¸ãoemambosossexos.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Aperianal,oranal,orperanus,fistulaisdefinedasan anoma-louspathwaylinkingtwoepitheliafromdifferentorigins.This defectischaracterizedbythreebasiccomponents: internal opening(IO),fistuloustract(FT)andexternalopening(EO).1
Moreoften,theperianalfistularesultsfromaninfectiousand inflammatoryprocesswithitsorigininthecryptoglandular area.1,2 Thisconditiondependsonamedicaltreatmentthat
aimstopreventrecurrence and damagetosphincter mus-cles.Thus,ananatomicalknowledgeoftheperianalregion, anunderstandingofthepathophysiologyofthediseaseand anaccurateandappropriatesurgicalplanningareessential.
Theextentofthefistulouspathisvariableandcan com-promiseseveralanatomicalstructuresintheanorectalregion. Themostoftenusedclassificationforfistulaewasproposed byParksetal.,3relatingtheextentofthefistulouspathwith
sphinctericmusclesinvolved,andthedefectisclassifiedinto four maintypes: intersphincteric, transsphincteric, supras-phinctericand extrasphincteric. Proctologic examination is thefirstpropaedeuticmeasure,butthismaynotallowa cor-rectclassificationoffistulaeandcanmissdeepfistulaeandthe visualizationoftheinternalopening.4DavidHenryGoodsall’s
clinicalobservations,aimingtodefinethecourseofanal fistu-lae,ledtotheformulationofarulethatcametobearhisname (Goodsall’srule),indicatingthatOEssituatedposteriorlytoa transverselinedrawnacrossthecenteroftheanalcanaldrain towardanIOlocatedat6h(i.e.,formacurved-pathtype).On theotherhand,OEssituatedanteriorlytothislinedrainforan IOradiallylocated(i.e.,formastraight-typepath).5Goodsall’s
originalobservationswerelistedatthemeetingoftheWest London’sMedicalandChirurgicalSocietyonMay6,1887by Edwards6andafterwardswereuniversallyacceptedand
pub-lishedintheformofGoodsall’s“rule”or“law”.Althoughthis ruleisuseful,somestudieshaveshownvariableresultsfor primaryfistulae.7,8
Recent technological advances have allowed a careful complementaryevaluation,usingimagingmethodssuchas anorectalultrasonography,especiallythethree-dimensional mode, and magnetic resonance imaging.9–15 The 3D mode
detailsofthedistributionoffistulous pathsandtherateof muscleinvolvementineachhemicircumferenceandinboth genders.14,15
Therefore,thisstudyaimstoevaluatetheanatomic charac-teristicsofthefistulouspathandoftheexternalandinternal openingsinpatientswithtranssphinctericanalfistulausing thethree-dimensionalanorectalultrasound(US-3D),and cor-relatethefindingswithGoodsall’stheory,withacomparison betweengenders.
Method
FromJanuary2010toJune2013,151patientswith transsphinc-teric anal fistulae from the Coloproctology Clinic, Hospital UniversitárioWalterCantídio,UniversidadeFederaldoCeará (HUWC-UFC)andfromtheoutpatientclinic,Coloproctology Center,HospitalSãoCarloswereprospectivelyevaluated.The study was approvedby the Ethics Committee on Research oftheHospitalUniversitárioWalterCantídio.Thesepatients weresubmittedtoUS-3DintheColoproctologyCenter, Hos-pital São Carlos, and those patients with transsphincteric analfistulaofcryptoglandular origin,withidentification of allitscomponents,externalopening,primaryandsecondary fistulous path, and internalopening, were included. Those patientswithotherbenignormalignantanorectaldiseases, sphinctermuscle injury diagnosed byUS-3D,previous col-orectal/proctologicsurgery,morethanoneinternalopening, recurrentfistulae,andwithintersphincteric,extrasphincteric andsuprasphinctericfistulawereexcluded.
Patientsweredividedinto3groupsaccordingtothe posi-tionofEOandIOwithrespecttoanalcircumference,using positionsof3and9hours(h),drawingalinethroughtheanal canal,asproposedbyGoodsall,withitsdivisioninan ante-riorhemicircumference(AHC)correspondingtotheinterval between9and3h(anusinthelithotomyposition)anda pos-teriorhemicircumference(PHC)correspondingtotheinterval between3and9h:GroupI(EOandIOinAHC);GroupII(EO andIOinPHC)andGroupIII(EOandIOinopposite hemicir-cumference–OHC).Thedatawereevaluatedfortheposition ofEOandIO,pathtypes(straightandcurved)ineachgroup, comparinggenders(male–Mandfemale–F),andcorrelating ourfindingswiththeTheoryofGoodsall.
Allpatientsunderwentsurgery,andUS-3Dfindingswere comparedwithintraoperativefindings:typeofpath,location oftheinternalorifice,andidentificationofthesecondarypath. Theconcordanceratewascalculated.
Three-dimensionalanorectalultrasound
A Pro-Focus BK Medical (Herley, Denmark) ultrasound machine witha type2052,360-grade rotational transducer withfrequencyof9–16MHzandfocallengthrangingfrom2.8 to6.2cmwasused.Thistransducerprovidesautomaticimage acquisitioninaproximal-distaldirectionina6.0-cmsegment during50s.Itisnotnecessarytomovethetransducerinside therectumand/oranal canal.Acquisitionofasequence of numeroustransaxialparallel images(0.25mm)isobtained, resultinginacube-shapeddigitalizedvolumetricimagewith greatmobility,enablingitsanalysisinmultipleplanesandin
realtime.Thus,afterwardstheexaminerhastheopportunity toreviewthetest,asmanytimesasnecessary,whichresults inmoreinformation.
Ourpatientsunderwentrectalenema2hbeforetheexam, withtheprocedure notrequiring anestheticsedation.They wereinitiallyplacedinleftlateraldecubitus(Simsposition). After a static inspection and identification of the external fistulousopening,digitalrectalexaminationwasheldto eval-uate the retrograde preparation. Then the transducer was introducedtothelowerrectum.Twoscanswereacquiredto evaluatetheanatomyofthefullanalcanal,identifyingpath(s), internal orifice(s) and/or the presenceof adjacent cavities, allowingtheidentificationoftranssphinctericfistulae, accord-ingtoParksetal.3
Thefirstscanwasdonewithoutapplicationofhydrogen peroxide.Atthisstage,thefistulouspathwasecographically representedbyahypoechoicimagesituatedlaterallytothe sphincter muscle and crossingthe external anal sphincter (EAS)andtheinternalanalsphincter(IAS)intranssphincteric fistulae.Secondarypathscouldbeidentifiedbyproximalor distalextensionsofthemainpath.Theinternalfistulous ori-ficecorrespondedtoaruptureimageinIAS(intheabsence ofpriorsphincterotomy)andtoahypoechoicimagein subep-ithelialtissue.
ThesecondscanwasobtainedafterEOcatheterismwith avascularcatheter(intracath)andaninjectionof0.3–1.0mL of10%hydrogenperoxide(H2O2)inallcases.Thepresenceof
H2O2incontactwiththeinflamedtissueproducesairbubbles,
andthehypoechoicultrasoundimagesbecomehyperechoic images, with more enhancement.9,10,14,15 All examinations
were performedbyasinglecoloproctologistexperiencedin thismethod.
Statisticalanalysis
StatisticalanalyseswereperformedusingSPSSversion17for Windows®.Evaluationofdataincludeddescriptivestatistics
(mean,standarddeviation,interquartilerange).Theanalytical methodsappliedwereStudent’st-testandFisher’sexacttest. Thelevelofstatisticalsignificancewassetatp<0.05.
Results
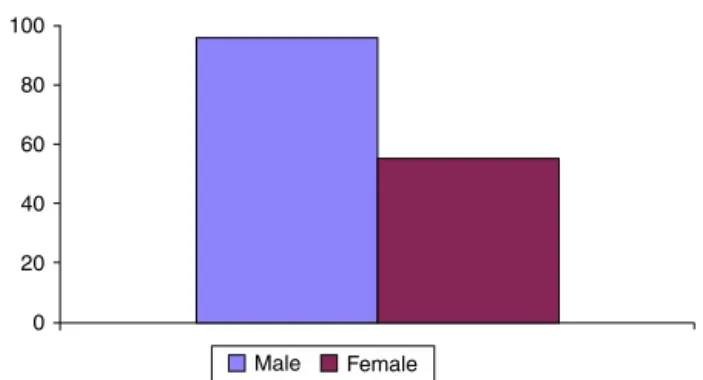
151patientswithtranssphinctericanalfistulaof cryptoglan-dularorigin,agedfrom 18to74 years,withamean ageof 40.3(±11.6)years,wereevaluated.Ofthistotal,55(36%)were womenand96(64%)men(Fig.1).Seventy-four(49%)patients (M:41,F:33)wereincludedinGI;68(45%)(M:50,F:18)were includedinG2;and9(6%)(M:5,F:4)were includedinGIII (Table1).
Thefistulouspathwasstraightin103(68%)(M:74,F:29) andcurvedin48(32%)(M:22,F:26)patients,withno statis-ticaldifferencewhencomparedtothetypeofpathineach hemicircumference(p=0.090).However,ahigherincidenceof straightpathswasevidencedinmalepatients(p=0.006),and asimilardistributionbetweenstraightandcurvedpathswas observedinfemalepatients(Table2).
Male 100
80
60
40 20
0
Female
Fig.1–Prevalenceoftranssphinctericanalfistulaebetween genders.
Table1–Distributionofpatientsbetweengenders accordingtothepositionofexternalandinternal fistulousorificesinanteriorandposterior hemicircumferences.
Groups Gender
Female Male
GROUP1 15(20%) 33(44%)
GROUP2 04(8%) 11(15%)
GROUP3 04(%) 05(%)
Table2–Distributionofpatientsbetweengenders accordingtofistulapathtype.
Gender Typeofpath
Straight Curve
Female 29(19%) 26(17%)
Male 74(49%) 22(15%)
Table3–Distributionofpatientsamonggroups accordingtofistulapathtype.
Total=151 Straight–103(68%) Curve–48(32%)
Male Female Male Female
Pathtype
GroupI(74) 33(44%) 15(20%) 8(11%) 18(25%) GroupII(68) 39(57%) 14(20%) 11(15%) 04(8%) GroupIII(09) 02(22%) – 03(33%) 04(45%)
F:18/25%)hadcurvedpaths(Table3),andahigherincidence ofstraight pathsinmalepatients wasobserved,compared tofemalepatients(p=0.003).However,inwomenthe distri-butionofcurved(seeFig.3)andstraight pathswassimilar. Secondarypathswereseenin18(24%)patients,ofwhom50% werewomen.
InGroupII,15(22%)patients(M:11/15%F:4/8%)hadcurved paths,and53(78%)patients(M:39/57%;F:14/20%)hadstraight paths(Table3andFig.4).Therewasnostatisticaldifference, regardingthepresenceofcurvedandstraight paths,inthe comparisonbetweenmenandwomen.Secondarypathswere seenin17(25%)patients,ofwhom9weremen.
InGroupIII,allits9patientshadcurvedpaths(M:5,F:4) (Table3).Secondarypathswereobservedin4(44%)patients, allofthemfemales.
TheconcordancedegreeamongUS-3Dandintraoperative findingswas:primarypath=99%,secondarypath=98%,and internalopening=98%.
Discussion
Thetreatment ofanal fistulae isamajorchallenge forthe coloproctologist.Studiesshowhighinjuryratesforfecal con-tinence (18–82%)in patientsundergoing surgicaltreatment
a
EAS
IAS
IAS
Superior
Middle
Inferior OI
EAS
EAS IAS
b
a
b
EAS
IAS
IAS Superior
Middle
Inferior
Inferior OI
EAS
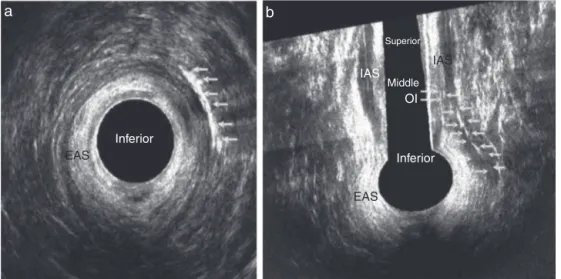
Fig.3–Transsphinctericfistulainafemalepatientafterapplicationofhydrogenperoxide.Curvedpathlocatedinanterior hemicircumference.EAS–externalanalsphincter;IAS–internalanalsphincter.(a)Axialplaneand(b)coronalplane.
resultinginsectionofsphinctermuscle.14,16Therefore,afull
assessmentisnecessaryforatherapeuticconducttobe cor-rectlychosen.Technologicaladvanceswithcomplementary imagingmethodshavecontributedtothe understandingof thecorrelationbetweenthefistulouscomplexandanalcanal anatomy.14,15
The evaluation of any fistula starts with a proctologic exam,withthe positionof theexternaland internal fistu-lousopeningsrelativetoanalcircumference.The“Goodsall’s rule”remains in use bya number ofsurgeons during the evaluationofanalfistulaeinpre-andtransoperativephases, oftenwithoutevidenceofconcordancebetweenruleand sur-gicalfindings,inanattempttopredictthetypeofpath, as wellastheinternalopeninglocalization,beginningfromthe locationoftheperianalexternalopening.Therefore,the eval-uationwitha complementaryimagingmethod wouldhelp inchoosingthe therapeuticapproach. Studies haveshown thatevenfistulaedescribedassimple,thatis,witha superfi-cial,subcutaneousorlowtranssphinctericpath(representing approximately95%ofthetreatedfistulae),maypresent,after thefistulotomy,highcomplicationratesduetothepresence ofsecondarypathsorflawsintheidentificationoftheprimary internalopening.17,18Theattentiononidentifyingthepaths
andtheirrelationshiptotheanalsphincterimprovethe out-comeofasubsequentsurgicalapproach,andmayresultin lesstraumatothesphinctericapparatusand,consequently, inlowermorbidityforthepatient.19
Theaimofthisstudywastoevaluatetheanatomical char-acteristics of anal fistulae (of transsphincteric type) using US-3D and correlating its findings of EO and IO position and thetypeofpath withGoodsall’stheory, with the con-firmationbysurgicalfindings.Theselectionofpatientswith transsphinctericfistulaeforinclusioninthisstudyisdueto thehigherprevalenceofthistypeofdefectinthestudyperiod, andtheincidenceofanalfistulaeisgreaterinmenbyaratio of2:1andinyoungadultswithanoverallmeanageof40years –datasimilartootherstudiesintheliterature.20
TheGoodsall’srulepostulatesthatanteriorfistulaehave radial(straight)paths,whichisconsistentwiththeresultsof
thisstudywhenassessingmales–themajorityofour sam-ple. However,forwomenasimilarity betweenstraight and curvedpathswas found.CiroccoandRielly evaluatedtheir intraoperativefindingsandcorrelatedtheirresultswiththe Goodsall’srule,showingassociationinonly49%ofanterior fis-tulaewithradialpaths,while71%ofthisgroupoffistulaewere presentedwithaninternalopeninginthemiddleline,with nostraightpaths,andincluding4casesofhorseshoefistulae. Therefore,eveninfistulaeoftheanteriorsegment,whichmay seemsimpleconditionsonphysicalexamination,the preop-erativeultrasonographicdefinitioncanavoidsurprisesforthe surgeon.Inthepresentstudy,ahighercorrelationwith ante-riorfistulaewasnoted,and65%ofpathswereofstraighttype; ofthese,44%affectedmenandonly20%,women.
In this series, there was no evidence of correlation of posteriorpathswithGoodsall’sruleinbothgenders,with pre-dominanceofstraightpaths;CiroccoandReillyshowedthat Goodsall’srulewasaccurateindescribingthepathofanal fis-tulaewithposteriorexternalopening,bothinmaleandfemale subjects(90%of124patients;87%ofmenand97%ofwomen withposteriorexternalopeninghadtheirpathtoward poste-riormidline).
Theresultsofthisstudydidrevealneitheracomplete cor-relationwithGoodsall’srulenorwiththeresultspresentedby CiroccoandReilly,comparingpatientswithanalfistulawith thisrule.Thisisduetothecomplexityoffistulae,makingit difficulttocharacterizethesedefectsassimpleorcomplex, accordingtothepositionoftheirorificeswiththeanal cir-cumference.Therefore, ourdatasuggest theeliminationof thedistinctionbetweenanteriorandposteriorfistulaeasof thetypeofpathpresented.Eachfistulashowsthedistribution ofitscomponents(OE,OIandFT)differently,notfollowinga singlerule.
a
EAS
EAS IAS
OI
IAS
b
EAS
IAS
IAS
PR EAS
Inferior Middle Superior
OI
c
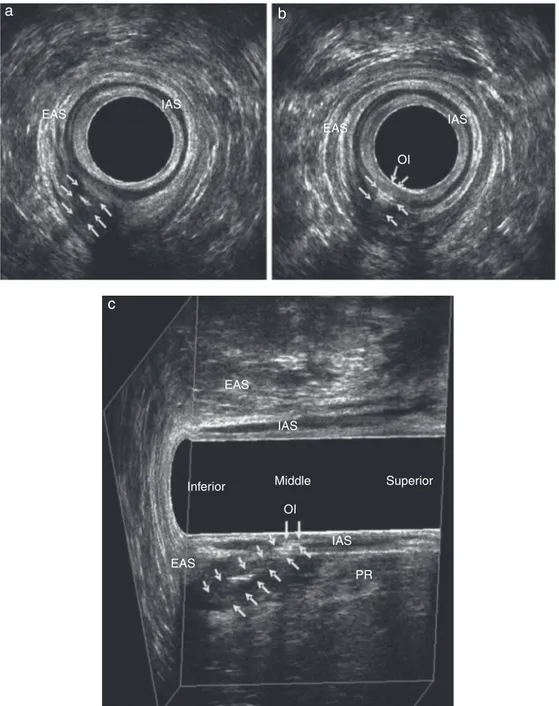
Fig.4–Transsphinctericfistulainamalepatientafterapplicationofhydrogenperoxide.Straightpathlocatedinposterior hemicircumference.EAS–externalanalsphincter;IAS–internalanalsphincter;PR–puborectal.(a)Axialplane–path,(b) axialplane–internalopeningand(C)paramediansagittalplane.
sphinctermuscle.Thisenablesthe classificationoffistulae accordingtoParksetal.3andtheidentificationofsecondary
paths(inthisstudy,secondarypathswereidentifiedin14% ofpatients).Thiscomplementaryassessmentalsoallowsan evaluationoftheportionofmusculatureinvolvedbythe fis-tulouspath,andthequantificationofmuscletissuethatwill beseveredduringsurgery.14Takentogether,allthesedatawill
characterizethefistulaascomplexorsimple,andwillserve asguidanceinthechoiceoftreatment,inordertoprevent recurrenceandtopreservesphincterfunction.Likewise,the positionofthefistula(anteriororposterior)couldhavegreater importancerelativetosphinctericmuscledistribution,which showsdifferenceswhencomparinganteriorversusposterior hemicircumference.20,21 Instudiesevaluatingtheanalcanal
ofnormalpatientsofbothgenders,thedistributionof sphinc-tericmusculaturewasstudied,andthesmallerlengthofthe analsphincterinwomenwasevidenced,whichcharacterizes morecomplexfistulae,especiallythoselocatedintheanterior quadrant.14,21
theresultsrangedfrom65to100%and,withtheuseof hydro-genperoxide,from71to99%.Forinternalopening,theresults rangedfrom64to96%and,withtheuseofhydrogen perox-ide,from77–98%to54–97%.22–24Theresultsofthestudywere
similartothoseintheliterature,withhighcorrelationwith transoperativefindings.
ThechoiceofUS-3Disduetotheeaseofcarryingoutthe procedurebyacolorectalsurgeon,asallpatientswithananal fistulaareevaluatedpreoperativelywiththisimagingmethod inthisinstitution.Anotheroption,magneticresonance imag-ing,isamorecostlymethod,andisperformedbyaradiologist. Thismethodshouldbeusedindoubtfulcases.13Thisisthe
firststudytocorrelateanalfistulacomponentswithGoodsall’s ruleusingUS-3Dandintraoperatoryfindings.
Thenumberofpatientsincludedinthisstudyisclinically relevant,andhereweemphasizetheimportanceofafull eval-uationwithUS-3Dbyasingleevaluatorwithexperienceinthis methodandtheuniquenessofpatientsoperatedbyateamof threetrainedcolorectalsurgeons.However,thesearepatients withonlyonetypeoffistula(transsphincteric).Further stud-iesareneeded,withinclusionofintersphinctericfistulae,or still,withthestudyofpatientswithanotherimagingmethod, suchasmagneticresonanceimaging.
Conclusion
Inconclusion,ourultrasoundfindings correlatewith Good-sall’s theory for anterior hemicircumference, straight-type, fistulaeinmen,whileinwomenthedistributionofcurvedand straightpathsissimilar.Ontheotherhand,inposterior hemi-circumferencenocorrelationwasobservedinbothgenders. US-3Dshowedhighcorrelationwithintraoperativefindings.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CormanML.Colonandrectalsurgery.2nded.Philadelphia: J.B.Lippincott;1989.p.137.
2. HamalainenKP,SainioAP.Incidenceoffistulasafterdrainage ofacuteanorectalabscesses.DisColonRectum.
1998;41:1357–61.
3. ParksAG,GordonPH,HardcastleJD.Aclassificationof fistula-in-ano.BrJSurg.1976;63:1–12.
4. BuchananGN,HalliganS,BartramCI,WilliamsAB,TarroniD,
CohenCR.Clinicalexamination,endosonographyandMR
imaginginpreoperativeassessmentoffistulainano: comparisonwithoutcome-basedreferencestandard. Radiology.2004;233:674–81.
5. GoodsallDH,MilesWE.Ano-rectalfistula.In:GoodsallDH, MilesWE,editors.Diseasesoftheanusandrectum.London: Longmans,Green&Co.;1990.p.92–137.
6.EdwardsFS.Someoftherarerformsofrectalfistulae.Lancet. 1887;1:1089.
7.CiroccoWC,ReillyJC.Challengingthepredictiveaccuracyof Goodsall’sruleforanalfistulas.DisColonRectum.
1992;35:537–42.
8.GunawardhanaPA,DeenKI.Comparisonofhydrogen
peroxideinstillationwithGoodsall’sruleforfistula-in-ano. ANZJSurg.2001;71:472–4.
9.Navarro-LunaA,García-DomingoMI,Rius-MacíasJ, Marco-MolinaC.Ultrasoundstudyofanalfistulaswith
hydrogenperoxideenhancement.DisColonRectum.
2004;47:108–14.
10.Sudol-SzopinskaI,SzczepkowskiM,PanorskaAK,Szopinski T,JakubowskiW.Comparisonofcontrast-enhancedwith noncontrastendosonographyinthediagnosticsofanal fistulas.EurRadiol.2004;14:2236–41.
11.WestRL,DwarkasingS,Felt-BersmaRJ,etal.Hydrogen
peroxide-enhancedthree-dimensionalendoanal
ultrasonographyandendoanalmagneticresonanceimaging
inevaluatingperianalfistulas:agreementandpatient preference.EurJGastroenterolHepatol.2004;16:1319–24. 12.RattoC,GrilloE,ParelloA,CostamagnaG,DogliettoGB.
Endoanalultrasound-guidedsurgeryforanalfistula. Endoscopy.2005;37:722–8.
13.SunMR,SmithMP,KaneRA.Currenttechniquesinimaging offistulainano:three-dimensionalendoanalultrasoundand magneticresonanceimaging.SeminUltrasoundCTMRI. 2008;29:454–71.
14.Murad-RegadasSM,RegadasFSP,RodriguesLV,HolandaEC, BarretoRGL,LetíciaO.Roleofthree-dimensionalanorectal ultrasonographyintheassessmentofanterior
transsphinctericfistula.DisColonRectum.2010;53:1035–40. 15.Murad-RegadasSM,RegadasFSP,RodriguesLV,etal.
Anatomiccharacteristicsofanalfistulaonthree-dimensional anorectalultrasonography(3-DAUS).DisColonRectum. 2011;54:460–6.
16.OmmerA,WengerFA,RolfsT,WalzMK.Continencedisorders afteranalsurgery:arelevantproblem?IntJColorectalDis. 2008;23:1023–31.
17.SangwanYP,RosenL,RietherRD,StasikJJ,SheetsJA, KhubchandaniIT.Issimplefistula-in-anosimple?DisColon Rectum.1994;37:885–9.
18.AhmedA,Abou-Zeid.Analfistula:intraoperativedifficulties andunexpectedfindings.WorldJGastroenterol.
2011;17:3272–6.
19.Garcia-AguilarJ,BelmonteC,WongWD,GoldbergSM,Madoff RD.Analfistulasurgery:factorsassociatedwithrecurrence andincontinence.DisColonRectum.1996;39:723–9.
20.WilliamsAB,BartramCI,HalliganS,MarshallMM,NichollsRJ, KmiotWA.Multiplanaranalendosonography–normalanal canalanatomy.ColorectalDis.2001;3:169–74.
21.RegadasFS,Murad-RegadasSM,LimaDM,etal.Analcanal
anatomyshowedbythree-dimensionalanorectal
ultrasonography.SurgEndosc.2007;21:2207–11.
22.GustafssonUM,KahveciogluB,AstromG,etal.Endoanal ultrasoundormagneticresonanceimagingforpreoperative assessmentofanalfistula:acomparativestudy.Colorectal Dis.2001;3:189–97.
23.NavarroA,RiusJ,ColleraP,etal.Analfistulas:resultsof ultrasonographicstudies.DisColonRectum.1998;41:A57. 24.DeenKI,WilliamsJG,HutchinsonR.Fistulasinano:endoanal