w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
LASER
hemorrhoidal
dearterialization
Paulo
Boarini
∗,
Lucas
Rodrigues
Boarini,
Paulo
de
Azeredo
Passos
Candelaria,
Edgard
Mesquita
de
Lima,
Marcelo
Rodrigues
Boarini
HospitalMunicipaldoTatuapé,ResidênciadeCirurgiaGeral,Servic¸odeColoproctologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24August2016 Accepted4December2016 Availableonline28December2016
Keywords:
Hemorrhoids
HemorrhoidalLASERProcedure Hemorrhoidaldearterialization
a
b
s
t
r
a
c
t
Introduction:Hemorrhoidaldiseaseisassociatedwiththetheoryofarterialbloodhyperflow causingswellingsinhemorrhoidsand,consequently,hyperplasiaandvenouscongestion. Thetechniquehelpstopromotetheobliterationoftheterminalsofthesuperiorrectalartery brancheswithouttheneedforanesthesiabyelectrofulgurationwithdiodefiberLASER.The objectiveofthisstudyistodescribetheresultsof55patientswithhemorrhoidaldisease treatedbytheHemorrhoidalLASERProceduretechnique.
Method:Withouttheneedofanesthesia,terminalarteriolesoftheupperrectalarteryare identifiedbyaDopplertransducer(20MHzprobe3mm)placedonaspeciallydesigned proc-toscope.Afteridentification,itpromotesarteriolarelectrofulgurationat980nmfiberlaser diode,causinginterruptionofhemorrhoidalflow.Thisprocedureisrepeated circumferen-tially,followingtheclockwisepositions.
Results:Between2011and2014,55patientsunderwenttheHemorrhoidalLASERProcedure techniqueforhemorrhoidaldiseasegradesI,IIandIII.Therewasnoneedforanesthesia andonlytwopatientsrequiredsedationfortheprocedure.Theoverallsatisfactionratewas 89%,withsymptomresolutionin84%andadecreaseofatleastonegradeinhemorrhoidal diseasein80%ofcases.
Conclusion:HemorrhoidalLASERProcedureisapainlessoutpatienttechniquethatdoesnot requireanesthesia,inadditiontobeingsafeandeasytoperform.Itiseffectivein reduc-ingsymptomsandcomplicationsofthehemorrhoidaldiseasegradesIandII,withhigh satisfactionrates.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Desarterializac¸ão
hemorroidária
a
LASER
Palavras-chave:
Hemorroidas
HemorrhoidalLASERProcedure Desarterializac¸ãohemorroidária
r
e
s
u
m
o
Introduc¸ão:Adoenc¸ahemorroidáriaestáassociadaateoriavasculardehiperfluxoarterial causandodilatac¸õesnosplexoshemorroidáriose,consequentemente,hiperplasiae con-gestãovenosa.AtécnicaHeLPpromoveaobliterac¸ãodosramosterminaisdaartériaretal superior,semanecessidadedeanestesia,atravésdaeletrofulgurac¸ãocomfibradediiodo
∗ Correspondingauthor.
E-mail:[email protected](P.Boarini).
http://dx.doi.org/10.1016/j.jcol.2016.12.001
LASER.Oobjetivodestetrabalhoédescreverosresultados de55 pacientescomdoenc¸a hemorroidáriatratadospelatécnicaHeLP.
Método:Semanecessidadedeanestesia,asarteríolasterminaisdaartériaretalsuperiorsão identificadasatravésdeumtransdutordoppler(20mhzprobede3mm)locadoemum proc-toscópioespecialmentedesenhado.Apósaidentificac¸ão,promove-seaeletrofulgurac¸ão arteriolaratravésdeumafibrade980nmdediiodoLASER,ocasionandointerrupc¸ãodo hiperfluxohemorroidário.Esteprocedimentoérepetidocircunferencialmente,seguindo-se asposic¸õesdashorasdeumrelógio.
Resultados: Entre2011e2014,55pacientesforamsubmetidosatécnicaHeLPparadoenc¸a hemorroidáriadegrausI,IIeIII.Nenhumpacienteutilizouanestesiaeapenasdois neces-sitaramsedac¸ãoparaarealizac¸ãodoprocedimento.Oíndicedesatisfac¸ãoglobalatingiu 89%,houveresoluc¸ãodossintomasem84%ediminuic¸ãodeaomenosumgrau,nadoenc¸a hemorroidária,em80%doscasos.
Conclusão: HeLPéumatécnicaambulatorialeindolor,quenãoutilizaqualqueranestesia, éseguraefácildeserrealizada.Eficienteparareduzirsintomasecomplicac¸õesdadoenc¸a hemorroidáriagrausIeII,comíndicedesatisfac¸ãoelevada.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Hemorrhoidal disease affects a large part of the world’s population. Theprevalence inour country is notprecisely documented, but in the United States it is approximately 4.4%.1 The disease is associated with the vascular theory ofarterialblood hyperflow,causingdilationsinthe hemor-rhoidalplexusesand,consequently,venoushyperplasiaand congestion.2
In1995,Morinagaetal.proposedanewtherapeuticmethod based on the etiopathogenesis described above. A Doppler (Moricorn)was usedinthe assessmentand afterthe arte-rial flow identification, a high ligature was made inthese branches,reducingthe blood gradientreachingthe hemor-rhoidalplexus.3 Basedonthis principle,severaltechniques thatrequireanesthesiahavebeendeveloped,suchas mechan-icalanopexy4 and transanalhemorrhoidaldearterialization (THD).2,5
Insearchforasurgicaltechniqueforhemorrhoidaldisease withless postoperativepain, Salfiet al., in2009,described theHemorrhoidalLASERProcedure(HeLP)technique.Itisa minimally-invasivetechnique,whichdoesnotrequire anes-thesia, and consists in the identification of the terminal branches of the rectal artery through a Doppler located in a specially adapted proctoscope, followed by photoco-agulation of these branches using a 980nm LASER diode fiber.6,7
Thispublicationaimstodescribethefirst55casesinwhich theHeLPtechniquewasusedinBrazil.Athree-yearfollow-up wascarriedout,analyzingclinicalandfunctionalaspectsof patientsoperatedbythesamesurgicalteam,evaluating pre-andpostoperativesymptoms, characteristicsofthe studied population,descriptionofthetechniqueused,needfor anes-thesiafor the procedureand theoverall satisfactionindex relatedtothetechnique.
Materials
and
method
Between 2011and 2014,55 patientswere submittedto the HeLPtechnique,bythesamesurgeon,forhemorrhoidal dis-easegradesIandII,orgradeIIIwithlittlemucosalprolapse. GradeIVor gradeIIIhemorrhoids withlarge mucosal pro-lapse identified during outpatient proctologic examination were excludedfromthestudy.Data wereprospectively col-lectedandanalyzed.
Before undergoing the surgical procedure, the patients were submitted to colonoscopy or rectosigmoidoscopy to excludeotherpossiblecausesofbleeding.
Thepatientssignedthefreeandinformedconsent,which explainedabouttheproceduretobeperformed.Thepatients wereevaluatedondays7,30,90,120and180postoperatively. Thevisualanalogscale(VAS)ofpainwasappliedtwohours aftersurgeryinallpatientsandaretrogradequestionnairewas appliedontheday7postoperatively.Anoscopywasperformed to evaluate internal hemorrhoids after 30 days postopera-tively. Qualityof lifeassessment was questionedafter the thirdpostoperativemonth. ControlDopplerevaluationwas performedinallpatients,after120days,postoperatively.
HeLPtechnique
Thepatientisplacedinthelithotomyposition,withoutthe needforanytypeofanesthesia.Onlytwocasesrequired anal-gesia, perthepatient’s request.Antibioticprophylaxiswith cefazolinwasusedinallcases.
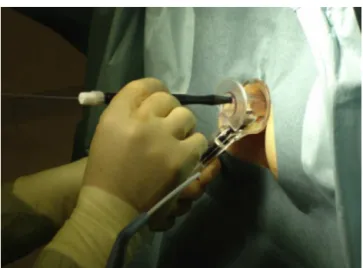
Fig.1–IdentificationofterminalarteriolesthroughDoppleruse.
Afteridentificationofthearterioles,theDoppleris with-drawnandthe980nmLASERopticalfiberisintroducedinthe samelocus(Fig.2).TheLeonardolaser–diodedeviceusedin ourstudywascalibratedwithapowerof13W.Interruption ofthearterysupplyingbloodflowisperformedbyactivating LASERenergythroughthe opticalfiber.First,two operator-controlledshotsareperformed,at2mmfromthemucosa,to promotescorchingofthelatter,followedbythreepresetshots forarterialobliteration(Fig.3).Eachshotlasts1.2s,witha0.6s intervalbetweenthem.
ThemethodefficacyisevaluatedagainbyDopplershortly afterthelastLASERshotand,iftheflowpersists,anewshotis carriedoutatthesamesite.Theremaybepersistenceofthe arterialflow,andinthiscase,webelieveittoberesonanceof thelargerperi-rectalarteries.
Aclockwiserotationoftherectoscopeallowsthe identifi-cationofallbranchesofthesuperiorrectalartery.Inthisway, thepositionoftheclockhoursisfollowed,checkingat1,2,3 o’clockandsoon.Amaximumof12branchescanbetreated atthesamesurgicalprocedure.
Results
TheHeLPtechniquewasappliedto55patients,28womenand 27men,withameanageof45years(22–67years).Mostthe populationsubmittedtosurgery(44patients)wasclassifiedas havinghemorrhoidsgradesIandIIand20%ofthesamplehad gradeIIIhemorrhoidsatdiagnosis(Table1).
Eleven patients had previous surgeries fortreatment of hemorrhoids(8rubberbandligations,2PPHsand1THD).No patientshowedcomplicationsduetothepreviousprocedure, onlyhemorrhoidaldiseaserecurrence(Table1).
Regardingthesurgicalindication,40patientshad hema-tocheziaasthemaincomplaint,6patientshadepisodesof hemorrhoidalthrombosis(acutepainandanallumps)treated clinicallyin other services, 5 patientshad anal discomfort secondarytoprolapseduringevacuationand4patients com-plainedofanalpruritus(Table2).
Table1–Patientcharacteristics.
Characteristics Patients
(n=55)
Meanage(years) 45.5(22–67)
Gender(%)
Male 49%
Female 51%
Hemorrhoidgrade(%)
GradesIandII 80%
GradeIII 20%
Previoussurgeries(%)
Rubberbandligation 14%
PPH 4%
THD 2%
Mainsymptom(%)
Bleeding 73%
Previousacuteepisodes(thrombosis) 11%
Analdiscomfort 9%
Pruritus 7%
PPH,procedureforprolapseandhemorrhoids(PPH);THD,transanal hemorrhoidaldearterialization.
Table2–Perioperativeandfollow-upperiod.
Characteristics Patients
(n=55)
Timeofsurgery(min) 9.9(7–19)
Perioperativebleeding(%) 5%
PostoperativepainVAS(mean) 1.4(0–3)
Intraoperativeanesthesia 0
Intraoperativesedation(%) 4%
Postoperativetenesmus(%) 15%
Evaluationat6months(%)
Symptomdisappearance 84%
Overallsatisfactionindex 89%
Nipplevolumereduction(1grade) 80%
Fig.2–Identificationofarterioles.
Noneofthesurgeriesrequiredtheuseofanesthesia.The meansurgicaltimewas9.9min,rangingfrom7to19min.The meannumberofbranchesofthesuperiorrectalarterythat were obliterated was 10.1 arterioles(7–12). Only2patients were anxious in the preoperative period and we chose to
Fig.3–Arterialobliterationusing980nmLASERfiber
optics.
performsedationwithmidazolamandfentanylforthesafety of the procedure. Bleeding during the surgical procedure occurred inthreepatients, butall weretreatedwithLASER fiber,requiringnomoreinvasivemaneuversforhemostasis. No procedure was performed on the external components (Table2).
Themeanvisualanalogpainscaleinthefirst2hwas1.4 (0–3).Themeantimebetweensurgeryandhospitaldischarge was4h.
Atthere-evaluationonday7postoperatively,11patients complained of self-limited bleeding and 8 patients com-plained of tenesmus, which showed complete resolution during follow-up. On day 30 postoperatively, 44 of the 55 patientshadareductionofatleastonegradeinthe classi-ficationofhemorrhoidaldisease.
All patients were assessed with Doppler after day 120 postoperatively.Weverifiedthatsomepatientshadflowat some of the previously photocoagulated points, albeit not necessarilyaccompaniedbysymptomreturn. Thebleeding decreasedinallcasesforwhichitwasthemaincomplaint. At180days,postoperatively,46of55patientsreported symp-tomdisappearance.Theoverallsatisfactionwiththesurgical and postoperativeproceduresreached89%,and 80%ofthe patients showedreductionofatleast onegradeof hemor-rhoidaldisease(Table2).
Discussion
Thedearterializationoftheterminalbranchesofthesuperior rectalarteryundoubtedlyconstitutesanefficientwaytotreat hemorrhoidaldisease.2–15
Severaltechniquesusedforthetreatmentofhemorrhoidal diseaseseektobalanceefficiencyandlesspostoperativepain. Theconventionaltechniquesbringfeartomanypatients,16,17 whorefrainfrombeingadequatelytreated,eitherdueto pre-viousexperience,orfromreportsoffriendsandrelatives.
to the so-calledexcisional or conventional techniques.16,17 Theimportanceinchoosingthetechniqueisparamountto thesuccessineachcase.
TheHeLPtechniqueiswell-establishedforthetreatment ofgradesIand IIhemorrhoidaldiseaseand somegradeIII cases,wherethesmallprolapseisnotpartofthecomplaint. IthasbeensuccessfullydisseminatedintheUnitedKingdom, Italy,CzechRepublic,Spain,andTurkey,aswellasinMexico, Argentinaandothers.6,7,21–23Despiteourexperiencedescribed inthisstudy,newpublicationswithlargersamplesandlonger follow-up are necessary, always aimingat achieving excel-lenceinthetreatmentofthesecases.
Giamundoetal.,inacomparativestudywithrubberband ligationfor gradesII and III hemorrhoidal disease showed lesspostoperativepain(p<0.001),greatersymptomresolution (p<0.001),greaternumberofpatientswithaone-grade reduc-tionofhemorrhoidaldisease(p<0.001)andbetterqualityof life(p=0.002). Therefore, although it isa higher-cost tech-nique,ithasverysatisfactoryshort-andlong-termresults.21 Itisnoteworthythe factthatitisatechniquethatdoes notrequireanesthesiaandcanberepeatedseveraltimes,as manyasnecessary,withoutcausingdamagetothe anorec-talanatomyandphysiology.Thefactthatitdoesnotrequire anesthesiadoesnotpreventitsperformancewiththeaidof sedation or even compound analgesia.It is anadvance in theoutpatienttreatmentofhemorrhoidaldisease,aswellas atechnological-scientificadvanceintheuse ofa specially-designed proctoscope for the precise identification of the terminalarteriolesthroughDoppler,anditsphotocoagulation throughLASERuse.6,7,21–23
OurstudywaslimitedtohemorrhoidsgradesIandII,as wellasgradeIIIhemorrhoidswithsmallprolapse,but new studies have demonstrated good results ofHeLP use with associatedmucopexywhenthepatienthasalargemucosal prolapse.22
Therearealsosomeeconomicbarriers,mainlybecauseitis arelativelynewandlessdisseminatedtechniqueinour coun-try,butcomparativestudies withotherexisting techniques havereporteda higherindexofpatient satisfaction.6,7,21–23 Thisproceduredecreasesthecostsofthehospitalstay,which representsanimportantpartoftheamountspentwith treat-ment.
Weconcludethatthisisanefficient,painless,ambulatory, andeasy-to-performtechnique,inwhichthelearningcurve becomessmall,giventhenumberoftimesthesameprocedure ofidentificationandphotocoagulationisperformedinasingle patient.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. LoderPB,KammMA,NichollsRJ,PhillipsRKS.Haemorrhoids pathology,pathophysiologyandaetiology.BrJSurg. 1994;81:946–54.
2.RattoC,DonisiL,ParelloA,LittaF,DogliettoGB.Evaluationof transanalhemorrhoidaldearterializationasaminimally invasivetherapeuticapproachtohemorrhoids.DisColon Rectum.2010;53:803–11.
3.MorinagaK,HasudaK,IkedaT.Anoveltherapyforinternal hemorrhoids:ligationofthehemorrhoidalarterywitha newlydevisedinstrument(Moricorn)inconjunctionwitha Dopplerflowmeter.AmJGastroenterol.1995;90:610–3.
4.LongoA.Treatmentofhaemorrhoidsdiseasebyreductionof mucosaandhaemorrhoidalprolapsewithacircularsuturing device:anewprocedure.In:ProceedingsoftheSixthWorld CongressofEndoscopicSurgery,Monduzzi.1998.p.777–84.
5.RattoC,GiordanoP,DonisiL,ParelloA,LittaF,DogliettoGB. Transanalhaemorrhoidaldearterialization(THD)forselected fourth-degreehaemorrhoids.TechColoproctol.2011;15:191–7.
6.SalfiR.Anewtechniqueforambulatoryhemorrhoidal treatment.Coloproctology.2009;31:99–103.
7.GiamundoP,CecchettiW,EsercizioL,FantinoG,GeraciM, LombezziR,etal.Doppler-guidedHemorrhoidalLASER Procedureforthetreatmentofsymptomatichemorrhoids: experimentalbackgroundandshort-termclinicalresultsofa newmini-invasivetreatment.SurgEndosc.2011;25:1369–75.
8.TohEL,NgKH,EuKW.Thefourthbranchofthesuperior rectalarteryanditssignificanceintransanalhaemorrhoidal dearterialisation.TechColoproctol.2010;14:345–8.
9.SohnN,AronoffJS,CohenFS,WeinsteinMA.Transanal hemorrhoidaldearterializationisanalternativetooperative hemorrhoidectomy.AmJSurg.2001;182:515–9.
10.SobradoCWJr,HoraJAB.TratamentoCirúrgicodaDoenc¸a HemorroidáriaporDesarterializac¸ãoTransanalGuiadapor DopplerassociadaaoReparoAnorretal:ATécnicadoTHD. Atualizac¸ãoemCirurgiadoAparelhoDigestivoeem Coloproctologia,2012.SãoPaulo:Departamentode
GastroenterologiadaFaculdadedeMedicinadaUSP;2012.p. 319–26.
11.RamírezJM,AguilellaV,ElíaM,GraciaJA,MartínezM. Doppler-guidedhemorrhoidalarteryligationinthe managementofsymptomatichemorrhoids.RevEspEnferm Dig.2005;97:97–103.
12.QinPP,HuangB,CaiHJ,GeQ,WangZL.Aprospective controlledcomparativestudyofDoppler-guided
hemorrhoidalarteryligationversusoperativeproceduresfor prolapseandhemorrhoids.ZhonghuaYiXueZaZhi. 2010;90:3131–4.
13.PolRA,vanderZwetWC,HoornenborgD,MakkingaB,Kaijser M,EeftinckSM,etal.Resultsof244consecutivepatientswith hemorrhoidstreatedwithDoppler-guidedhemorrhoidal arteryligation.DigSurg.2010;27:279–84.
14.JeongWJ,ChoSW,NohKT,ChungSS.Oneyearfollow-up resultofDoppler-guidedhemorrhoidalarteryligationand recto-analrepairin97consecutivepatients.JKoreanSoc Coloproctol.2011;27:298–302.
15.HoraJAB,KlajnerS,KruglenskyD,SobradoCWJr.Tratamento CirúrgicodaDoenc¸aHemorroidáriaporDesarterializac¸ão TransanalGuiadaporDopplerassociadaaoReparoAnorretal (ATécnicadoTHD):ExperiênciaInicial.In:1◦Congresso
PaulistadeColoproctologia.SãoPaulo8e9dejunhode. 2012.
16.FergusonJA,MazierWP,GanchrowMI,FriendWG.Theclosed techniqueofhemorrhoidectomy.Surgery.1971;70:480–4.
17.MilliganETC,MorganC,NaughtonJLF,OfficeRR.Surgical anatomyoftheanalcanalandtheoperativetreatmentof haemorrhoids.Lancet.1937;II:1119–24.
18.InfantinoA,AltomareDF,BottiniC,BonannoM,ManciniS. Prospectiverandomizedmulticentrestudycomparingstapler haemorrhoidopexywithDoppler-guidedtransanal
19.GreenbergR,KarinE,AvitalS,SkornickY,WerbinN.First100 caseswithDoppler-guidedhemorrhoidalarteryligation.Dis ColonRectum.2006;49:485–9.
20.GiordanoP,OvertonJ,MadedduF,ZamanS,GravanteG. Transanalhemorrhoidaldearterialization:asystematic review.DisColonRectum.2009;52:1665–71.
21.GiamundoP,SalfiR,GeraciM,TibaldiL,MurruL,ValenteM. Thehemorrhoidlaserproceduretechniquevsrubberband ligation:arandomizedtrialcomparing2mini-invasive treatmentsforsecond-andthird-degreehemorrhoids.Dis ColonRectum.2011;54:693–8.
22.GiamundoP,GeraciM,TibaldiL,EsercizioL,AgostiniS, TestoreP,etal.Laserhaemorrhoidalarterialclosure(HeLP) withrecto-anal-repair(RAR):anovelprocedureforthe treatmentofadvancedhaemorrhoidaldisease(Abstract). ColorectalDis.2014;16Suppl.3:21–36.