www.jped.com.br
ORIGINAL
ARTICLE
Spirometry
and
volumetric
capnography
in
lung
function
assessment
of
obese
and
normal-weight
individuals
without
asthma
夽
Mariana
S.
Ferreira
a,∗,
Roberto
T.
Mendes
a,
Fernando
A.L.
Marson
a,b,
Mariana
P.
Zambon
a,
Maria
A.R.G.M.
Antonio
a,
Ilma
A.
Paschoal
c,
Adyléia
A.D.C.
Toro
a,
Silvana
D.
Severino
a,
Maria
A.G.O.
Ribeiro
a,
José
D.
Ribeiro
aaUniversidadeEstadualdeCampinas(UNICAMP),FaculdadedeCiênciasMédicas,DepartamentodePediatria,Campinas,SP,Brazil bUniversidadeEstadualdeCampinas(UNICAMP),FaculdadedeCiênciasMédicas,DepartamentodeGenéticaMédica,Campinas,
SP,Brazil
cUniversidadeEstadualdeCampinas(UNICAMP),FaculdadedeCiênciasMédicas,DepartamentodeClínicaMédica,Campinas,SP,
Brazil
Received22June2016;accepted3October2016 Availableonline19April2017
KEYWORDS
Capnography; Spirometry; Obesity
Abstract
Objective: Toanalyzeandcomparelungfunctionofobeseandhealthy,normal-weightchildren andadolescents,withoutasthma,throughspirometryandvolumetriccapnography.
Methods: Cross-sectionalstudyincluding77subjects(38obese)aged5---17years.Allsubjects underwentspirometryandvolumetriccapnography.Theevaluationswererepeatedinobese subjectsaftertheuseofabronchodilator.
Results: Atthespirometry assessment, obese individuals,when compared with thecontrol group,showed lowervalues offorcedexpiratoryvolume inthefirst second byforced vital capacity(FEV1/FVC)andexpiratoryflowsat75%andbetween25and75%oftheFVC(p<0.05). Volumetriccapnographyshowedthatobeseindividualshadahighervolumeofproducedcarbon dioxideandalveolartidalvolume(p<0.05).Additionally,theassociationsbetweendeadspace volumeandtidalvolume,aswellasphase-3slopenormalizedbytidalvolume,werelowerin healthysubjects(p<0.05).Thesedatasuggestthatobesitydoesnotalterventilation homo-geneity,butflowhomogeneity.Aftersubdividingthegroupsbyage,agreaterdifferenceinlung functionwasobservedinobeseandhealthyindividualsaged>11years(p<0.05).
夽
Pleasecitethisarticleas:FerreiraMS,MendesRT,MarsonFA,ZambonMP,AntonioMA,PaschoalIA,etal.Spirometryandvolumetric capnographyinlungfunctionassessmentofobeseandnormal-weightindividualswithoutasthma.JPediatr(RioJ).2017;93:398---405.
∗Correspondingauthor.
E-mail:[email protected](M.S.Ferreira).
http://dx.doi.org/10.1016/j.jped.2016.10.007
Lungfunctioninobeseandhealthyindividualswithoutasthma 399
Conclusion: Evenwithoutthediagnosisofasthmabyclinicalcriteriaandwithoutresponseto bronchodilatoruse,obeseindividualsshowedlowerFEV1/FVCvaluesandforcedexpiratoryflow, indicatingthepresenceofanobstructiveprocess.Volumetriccapnographyshowedthatobese individualshadhigheralveolartidalvolume,withnoalterationsinventilationhomogeneity, suggestingflowalterations,withoutaffectinglungvolumes.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
PALAVRAS-CHAVE
Capnografia; Espirometria; Obesidade
Espirometriaecapnografiavolumétricanaavaliac¸ãodafunc¸ãopulmonar deindivíduosobesoseeutróficossemasma
Resumo
Objetivo: Analisarecompararafunc¸ãopulmonardecrianc¸aseadolescentesobesoseeutróficos saudáveis,semasma,pelaespirometriaecapnografiavolumétrica.
Métodos: Estudotransversalincluindo77indivíduos (38obesos)comidadeentrecincoa17 anos.Todososindivíduosrealizaramespirometriaecapnografiavolumétrica.Osobesos repe-tiramasavaliac¸õesapósousodebroncodilatador.
Resultados: Naavaliac¸ãodaespirometria,osindivíduosobesos,quandocomparadosaogrupo controle,apresentaram menoresvaloresnovolumeexpiratórioforc¸adonoprimeirosegundo pela capacidadevitalforc¸ada(VEF1/CVF)enosfluxosexpiratóriosa75%daCVFeentre 25-75% damesma(p<0,05). A capnografiavolumétricademonstrou que osobesos apresentam maiorvolume produzido dedióxido decarbonoe volumecorrente alveolar(p<0,05). Além disso,arelac¸ãoentreovolumeespac¸omortoevolumecorrente,bemcomooslopedafase 3normalizadopelovolumecorrenteforammenoresnosindivíduossaudáveis(p<0,05).Esses dadossugeremqueaobesidadenãoalteraahomogeneidadedaventilac¸ão,massimdosfluxos. Ao subdividir osgruposporidade, foiobservadamaiordiferenc¸anafunc¸ão pulmonarentre indivíduosobesosesaudáveisnafaixaetáriaacimade11anos(p<0,05).
Conclusão: Mesmosemodiagnósticodeasmaporcritériosclínicosesemrespostaaousode broncodilatador,osindivíduosobesosapresentarammenoresvaloresnoVEF1/CVFenosfluxos expiratóriosforc¸ados,indicandoapresenc¸adeprocessoobstrutivo.Acapnografiavolumétrica indicou nos indivíduos obesos maior volume corrente alveolar, sem alterac¸ões na homo-geneidadedaventilac¸ão,sugerindoalterac¸ãonosfluxos,semcomprometimentodosvolumes pulmonares.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Childhoodandadolescentobesityhascurrentlyreached epi-demic proportions and is considered one of the greatest challenges for publichealth in the 21st century.1 Consid-ering thisrisingprevalence, thereisaspecialconcern,as dysfunctionsresultingfromexcessfatmassshowan increas-ingly earlier onset, which affect the well-being of these individualssincechildhood.2,3
One of the deleterious effects of obesity is lung func-tionimpairment.Amongobeseindividualsinadulthood,this impairmentis alreadyevidentin literature.4---7 Itis known thatthedepositionofadiposetissueontheribcageleadsto animpairmentinitscomplianceand,consequently,tothe decreasein itsexpandability. The mechanical impairment triggerschangesinthelungelasticproperties,resultingin reducedfunctionalresidualcapacity,tidalvolume(TV),and expiratory reserve volume (ERV). Additionally, there is a reductioninforcedvitalcapacity(FVC)and,consequently, ofthetotallungcapacity.4---7
However,themechanismthroughwhichobesityimpairs lungfunctionappearstobedifferentintheyoung popula-tion.The results shown in the literatureare divergent in relationtothelungfunctionofobesechildrenand adoles-cents.Discrepanciesregardingfindingsmightbeinfluenced bychangesinbodystructureduringthisperiod.Moreover, studiesincludedifferentageandethnicgroups.8---15
Spirometryisthemostusedtoolfortheanalysisoflung function.Itsusehasbeendescribedinincreasinglyyounger populations.16 However,itisaneffort-dependenttestthat requiresunderstandingandcooperationoftheassessed indi-vidual,whichcangeneratedifficultiesinyoungersubjects. Therefore,thesearchfornewevaluationmethodsthatcan beusedinthispopulationhasbeenencouraged.
is divided into three phases: phase 1, which is compati-ble with air in the conduction airways and dead space; phase2 encompasses the proximal airways; and phase3, knownasthealveolarplateau,isrelatedtotheperipheral airways.
The advantageof VCis thatit does notrequireforced maneuvers,beingeasytoperform,eveninyounger individ-uals.VCwasfirstdevelopedforuseinindividualsundergoing mechanical ventilation,17---23 and its use in spontaneously breathingindividualsisrecent,withfewpublishedstudies, especiallyin children.24---29 There is nostandardization for dataanalysisinVCintheliterature.
Therefore,thestudyaimedtoevaluatelungfunctionin obesechildren andadolescents (without asthma) through spirometryandVC,andtocomparetheresultswithacontrol groupofhealthy,normal-weightindividualsinthesameage group.
Methods
Studysubjects
Thestudyincluded 38obesesubjects(20boys)aged5---17 yearsand 39 healthy subjects (17 boys) in the same age group.Thesample sizecalculationwasbasedon spirome-trymarkers, obtainedin apilot study,andconsidering an
˛errorof0.05 andaˇerror of0.20.Withthese assump-tions,theachievedsamplevalue comprised31individuals ineachgroup(obeseandhealthycontrols)for FVCand17 formeanforcedexpiratoryflowbetween25%and75%ofFVC (FEF25---75%)---thevariablesthatshowedgreatervariability.In
thiscontext,thestudysamplepowerwashigherthan80%. Theobeseindividualsincludedinthepresent studyare regularly followed-up at the Multidisciplinary Outpatient ClinicforObeseChildrenandAdolescents.Todefineobesity, theCenterforDiseaseControlandPrevention(CDC)criteria wereusedforindividualsaged2---20years.Individualswho wereabovethe95thpercentilefor bodymassindex(BMI) wereconsideredobese.Thestudyincludedonlyindividuals withexogenousobesity.
Healthy,normal-weightindividuals withBMI withinthe normalrange (BMIbetween the5th and85th percentile), whocomprisethedatabaseoftheLungPhysiology Labora-toryoftheCenterforPediatricResearchatUnicampwere includedinthecontrolgroup.
To be included in the study, participants’ parents or guardianssignedthe freeand informedconsentformand noneoftheincludedpatientsweresmokersand/orhadany currentrespiratorydiseases,suchascolds.
Aresponsetotheuseofbronchodilator(BD)greaterthan 10%forforcedexpiratoryvolumeinthefirstsecondofthe FVC(FEV1)wasconsideredasanexclusioncriterion,asitis
indicativeofasthma.However,noneofindividualshadtobe excludedforthatreason.
Individuals witha clinical history of anyother respira-torydiseases,suchaschronicobstructivepulmonarydisease andsleepapnea, werealsoexcluded.This evaluationwas performed throughtheanalysisof the outpatientmedical recordsof thestudy subjects.The studywasapprovedby theEthicsCommitteeoftheUniversity(#1165/2009).
Studydesign
Thiswasacross-sectionalandanalyticalstudywithacontrol groupcomparinglungfunctioninobeseandhealthychildren andadolescentsthroughspirometryandVC.
BMI
Regardingobesity,theCDCcriteriawereusedforthe inclu-sionofindividualsinthestudy(girls:http://www.cdc.gov/
growthcharts/data/set1/chart16.pdf and boys: http://
www.cdc.gov/growthcharts/data/set1/chart15.pdf).
Sub-sequently, for the statistical purposes of the study, the dataweretransformedintoz-scores,accordingtotheWorld HealthOrganizationcriteria.
Lungfunctionassessments
Prior to the evaluations, all subjects rested for at least 10min.First,theVCwasperformed,asitisapassive evalua-tion;subsequently,thespirometrywasperformed,because it is effort-dependent. Obesesubjects repeatedthe eval-uations20minaftertheuse ofaBD.Albuterol(C13H21NO3
[400mg])wasadministeredforbronchodilation.
Spirometry
Spirometry was performed according to the standards of the European Respiratory Society and American Thoracic Society. The acceptance criterion for the spirometry test comprisedatleast threeacceptable andtworeproducible standard curves. All study subjects met the criteria for acceptance.
ACPFS/Dspirometer(MedicalGraphicsCorp.,MN,USA) wasusedwiththesoftwareBREEZEPFWindowsversion3.8 (MedicalGraphicsCorp.,MN,USA).Thedatawereconverted toz-scores accordingtothenormalitycriteriaestablished by Quanjeretal. (2012)usingthe GLI2012software, pro-duced bythe GlobalLung Initiative(GLI), a Task Forceof theEuropeanRespiratorySociety.16
The z-scores of thefollowing variables were analyzed: FVC,FEV1,FEV1/FVC,forcedexpiratoryflowat75%ofFVC (FEF75%),andFEF25---75%.TheERVwasalsoevaluatedbythe percentageofthepredictedvalue.
Volumetriccapnography
The VC analysis was performed using the non-invasive CO2SMOmonitor(Dixtal,SãoPaulo,Brazil),usingthe
Analy-sisPlus® software,Windowsversion.Participantsperformed thetestinthesittingposition,usinganasalclipandnovisual contactwiththemonitor,topreventvisualinfluenceonthe respiratorypattern.Theywereinstructedtobreathecalmly, for 5min, intothe mouthpiece connectedtothemonitor. Respiratorycycleswerecorrectedsothattherewasno vari-ationgreaterthan25%ofexpiredvolume(EV)and5%ofCO2
attheend ofexpiration(EtCO2),accordingtothepattern
ofpreviousstudies.25,27
Lungfunctioninobeseandhealthyindividualswithoutasthma 401
of phases 2 and 3 (Slp2 and Slp3), which are numeri-calrepresentationsofCO2exhalationcurve;normalization of slopes by TV, to equalize the differences in height and weight (Slp2/VC and Slp3/VC)27; and the capnogra-phy index, proposed by Fuchs etal. (Slp3/Slp2)×100) to quantifyventilationhomogeneity.26
Analysisofresults
The SPSS 21.0 software (SPSS Inc., IL, USA) was usedfor statisticalanalysis.Thecomparisonsbetweenthestudy cat-egorical variables were performed using the chi-squared test.Thecomparisonsofnumericalvariablesbetweentwo groupswasperformedusingtheMann---Whitneytest.Linear regressionwasusedtoquantifytheassociationbetweenlung functionvariablesandBMIz-score.Alldatawerecorrected by theBonferroni test, considering an ˛<0.05/numberof testsperformedwitheachvariable.
Results
Studysubjects
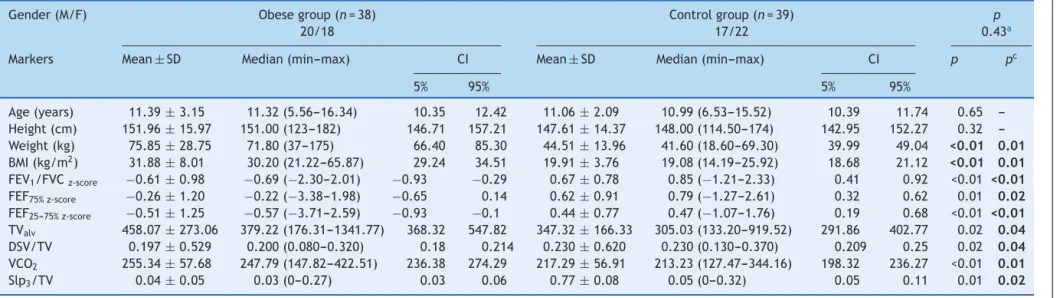
The study comprised 38 obese (20 boys) and 39 healthy (17boys)individuals,whoseagerangedfrom5.56to16.54 years.The descriptiveanalysisoftheanthropometricdata of the participants is shown in Table 1. Body weight and BMIweredifferentbetweenthegroups, andtherewasno differencebetween thegroupsregardingage,gender, and height.
Lungfunction
Studyparticipantsunderwentlungfunctiontestingthrough spirometryandVC.Table 1shows thevariablesthat were different between the groups at the lung function analy-sis.FEV1/FVC,FEF75%,andFEF25---75%werelowerintheobese group,evenaftertheBonferronicorrection.Inthesample, 36.8% ofobese individualshad FEF25---75% below70% of the predictedvalue,characterizingobstructiveflowdisorders. Therewerenoalterationsinsubjectsfromthecontrolgroup at this evaluation. There was no differencebetween the groupsregardingFVC,FEV1,andERV.
RegardingtheVC,adifferencewasobservedbetweenthe groupsforDSV/TVandSlp3/TV,whichwerelowerinobese patients,andinTValvandVCO2,whichwerehigher.There wasnodifferenceregardingthecapnographyindexbetween thegroups.
When analyzing the response of obese individuals to the use of BD, it was verified that none of the partici-pantsshowedaresponsehigherthan10%inFEV1,disproving thediagnosisofasthma.RegardingFVC(p=0.05),a reduc-tionafter medication wasobserved, and consequently an increase in FEV1/FVC (p=0.02). In the VC, the use of BD resulted in a reduction in MVt(p=0.01), MValv (p=0.01), andVCO2 (p=0.02), andan increase inDSV(p<0.01) and DSV/TV(p<0.01).Therefore,theobeseindividualsdidnot showapositiveresponsetotheuseofBD.
Lungfunctionandbodymass
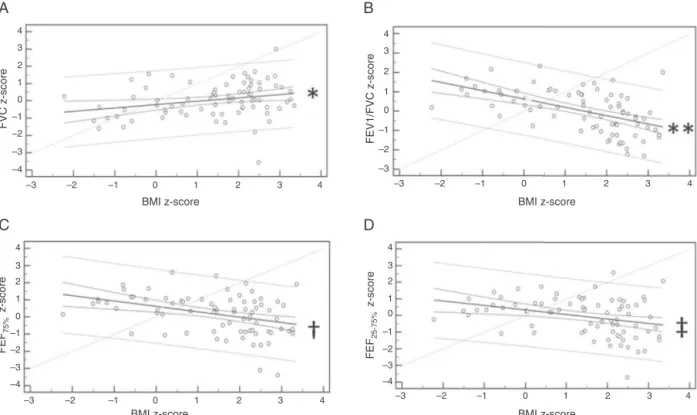
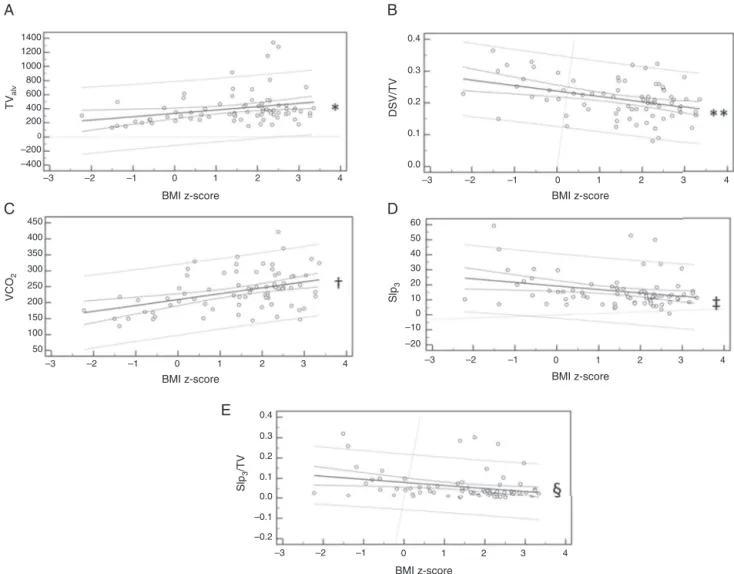
Figs.1and2show,respectively,thespirometryandVC
varia-blesthatwereinfluencedbytheBMIz-score.Intheanalysis oflinearregression,itwasverifiedthatBMIinfluencesFVC, FEV1/FVC, FEF75%, and FEF25---75%. In the VC, the variables TValv,DSV/TV,VCO2,Slp3,andSlp3/TVwereinfluencedby BMI.
Analysisoflungfunctionaccordingtoagegroup
Thestudyparticipantsweresubdividedintotwosubgroups accordingtotheagerange(ages5---11andage>11years), toverifywhetherdifferencesinlungfunctionoccurredeven attheyoungest agegroupsor startedwhentheindividual wasalreadyintheprocessofpubertalmaturation.
It was observed that the obese individuals had lower FEV1/FVCvalues,evenattheyoungeragegroups.However,
thechangesinFEFandincreaseinlungvolumes,analyzed byVC,weresignificantonlyintheoldergroup.Table2shows thep-valuesthatweresignificantinlungfunctionanalysis accordingtotheagegroup.
Discussion
The complexity of obesity and its close association with otherdiseasesencouragesthesearchforanunderstandingof themechanismsinvolvedinthechainofdeleteriouseffects causedbyexcessbodyweight.Whenanalyzingtheeffects ofobesity during childhoodandadolescence, theanalysis shouldbeeven morecareful,as thisperiodis marked by changesinbodystructure.28
Theinteractionbetweensuchdynamicandintense pro-cessesmaybethereasonforthedivergenceintheliterature thataddressestheinfluenceofobesity onlungfunctionin childrenand adolescents.Inaddition tothesubject com-plexity, the studies differ in relation to age group and populationcharacteristics.
Among the adult population, the literature is clear in establishing that obesity affects lung function through a restrictiveprocess.5,7Inyoungindividuals,studieshighlight theassociationbetweenobesityandasthma,butthereare fewconclusionsregardingthesubjectinindividualswithout asthma.
Inthepresentstudy,itwasobservedthattheobese indi-vidualshad lower FEV1/FVC and FEF values. The findings regardingtheexpiratoryflowsshouldbeanalyzedwith cau-tionduetothevariabilityofthetechniqueandthemethod used.Itwasalsoobservedthatobeseindividualshadhigher FVCvalues;however,aftertheBonferroni correction,this differencedidnotremainsignificant.
Amongthefindings,whatismorefrequentlyobservedin theliteratureandthatisconsistentwiththepresentstudy, isthelowerFEV1/FVCvalue amongtheobeseindividuals. RegardingFVCandFEV1,thefindingsarecontradictory,with studiesshowingpositive,negative,ornoassociationinthe comparison of obese and healthy individuals. The incon-sistency of the findings is maintained for the analysis of expiratoryflowsandERV.8---15
Ferreira
MS
et
al.
Table1 Comparisonbetweenthegroups’anthropometricdatawithspirometryandvolumetriccapnographyvariablesthatshowedapositiveassociation.
Gender(M/F) Obesegroup(n=38) Controlgroup(n=39) p
20/18 17/22 0.43a
Markers Mean±SD Median(min---max) CI Mean±SD Median(min---max) CI p pc
5% 95% 5% 95%
Age(years) 11.39±3.15 11.32(5.56---16.34) 10.35 12.42 11.06±2.09 10.99(6.53---15.52) 10.39 11.74 0.65
---Height(cm) 151.96±15.97 151.00(123---182) 146.71 157.21 147.61±14.37 148.00(114.50---174) 142.95 152.27 0.32
---Weight(kg) 75.85±28.75 71.80(37---175) 66.40 85.30 44.51±13.96 41.60(18.60---69.30) 39.99 49.04 <0.01 0.01
BMI(kg/m2) 31.88±8.01 30.20(21.22---65.87) 29.24 34.51 19.91±3.76 19.08(14.19---25.92) 18.68 21.12 <0.01 0.01
FEV1/FVCz-score −0.61±0.98 −0.69(−2.30---2.01) −0.93 −0.29 0.67±0.78 0.85(−1.21---2.33) 0.41 0.92 <0.01 <0.01
FEF75%z-score −0.26±1.20 −0.22(−3.38---1.98) −0.65 0.14 0.62±0.91 0.79(−1.27---2.61) 0.32 0.62 0.01 0.02
FEF25---75%z-score −0.51±1.25 −0.57(−3.71---2.59) −0.93 −0.1 0.44±0.77 0.47(−1.07---1.76) 0.19 0.68 <0.01 <0.01
TValv 458.07±273.06 379.22(176.31---1341.77) 368.32 547.82 347.32±166.33 305.03(133.20---919.52) 291.86 402.77 0.02 0.04
DSV/TV 0.197±0.529 0.200(0.080---0.320) 0.18 0.214 0.230±0.620 0.230(0.130---0.370) 0.209 0.25 0.02 0.04
VCO2 255.34±57.68 247.79(147.82---422.51) 236.38 274.29 217.29±56.91 213.23(127.47---344.16) 198.32 236.27 <0.01 0.01
Slp3/TV 0.04±0.05 0.03(0---0.27) 0.03 0.06 0.77±0.08 0.05(0---0.32) 0.05 0.11 0.01 0.02
n,numberofpatients;p,p-value;pc,p-valuecorrectedbytheBonferronitest;M,male;F,female;CI,confidenceinterval;SD,standarddeviation;min,minimum;max,maximum;
BMI,bodymassindex;kg/m2,kilogramspersquaremeter;FEV
1,forcedexpiratoryvolumeinthefirstsecond;FVC,forcedvitalcapacity;FEF75%,forcedexpiratoryflowat75%ofFVC;
FEF25---75%,forcedexpiratoryflowbetween25%and75%ofFVC;TValv,alveolartidalvolume;DSV,deadspacevolume;TV,tidalvolume;VCO2,exhaledcarbondioxidevolume;Slp3/TV,
phase-3slopecorrectedbyTV. Boldmeans‘‘StatisticallySignificant’’.
Lungfunctioninobeseandhealthyindividualswithoutasthma 403
A
4
3
2
1
0
–1
–2
–3
–4
4
3
2
1
0
–1
–2
–3
4
3
2
1
0
–1
–2
–3
–4 4
3
2
1
0
–1
–2
–3
–4
–3 –2 –1 0
BMI z-score BMI z-score
BMI z-score BMI z-score
FVC z-score
FEV1/FVC z-score
FEF
25-75%
z-score
FEF
75%
z-score
2
1 3 4 –3 –2 –1 0 1 2 3 4
–3 –2 –1 0 1 2 3 4
–3 –2 –1 0 1 2 3 4
B
D
C
Figure1 Linearregressionofspirometry variablesinfluenced by z-scoreofbodymassindex(BMI).(A) Forcedvitalcapacity
(FVC)z-score:y=−0.21+0.20x;*p=0.020;(B)ratiobetweenforcedexpiratoryvolumeinthefirstsecondandFVC(FEV
1/FVC)z -score:y=0.64−0.43x;**p<0.001;(C)forcedexpiratoryflowat75%ofFVC(FEF
75%)z-score:y=0.63−0.31x;†p=0.001;(D)forced expiratoryflowbetween25%and75%ofFVC(FEF25---75%)z-score:y=0.34−0.27x;‡p=0.005.
Table2 Differencesbetweenobeseandhealthypatients
inlungfunctionevaluationaccordingtoagerange.
Variables 5---11years >11years
p pc p pc
FEV1/FVCz-score <0.01 <0.01 <0.01 <0.01 FEF25---75%z-score <0.01 <0.01 <0.01 <0.01
MValv 0.46 1 0.04 0.16
TValv 0.30 1 0.03 0.11
VCO2 0.27 0.01 0.05
p,p-value;pc,p-valuecorrectedbytheBonferronitest;FEV1,
forcedexpiratoryvolumeinthefirstsecond;FVC,forcedvital capacity;FEF25---75%,forcedexpiratoryflowbetween25%and75%
ofFVC;MValv,alveolarminutevolume;TValv,alveolartidal
vol-ume;VCO2,exhaledcarbondioxidevolume.TheMann---Whitney
testwasusedforstatisticalanalysis,consideringanalpha=0.05. Boldmeans‘‘StatisticallySignificant’’.
body. Thus, both body growth and pubertal development mayinfluencelungfunction.Astherearedifferencesinthe onsetanddurationofeachindividual’sgrowthandpuberty periods,theanalysisoflungfunction,subdividingthegroups by pubertal development, could provide a better under-standingof how growth influencesthe alterations in lung function.Thiswasalimitationofthepresentstudy.28,29
Therefore,theauthors soughttoimprovetheaccuracy and reliability of the study by using twodifferent mech-anisms of pulmonary function assessment. In addition to spirometry,whichiscurrentlythemostoftenusedtoolfor thisanalysis,individualswereassessedthroughVC.
The use of VC in clinical practicestarted in the 1980s withFletcheretal.17 However,itwasmainlyusedin intu-batedindividualssubmittedtomechanicalventilation.18---21 Theuse of VCfor theanalysis oflung function in sponta-neouslybreathingindividualsis evenmorerecentandhas beenappliedinseveralclinicalconditions.22---27Inthe pedi-atricagegroup,theliteratureisevenscarcer,andstudies were found only in individuals with asthma, cystic fibro-sis,andbronchopulmonarydysplasia.24---27Tothebestofthe authors’knowledge,thisisthefirststudytoevaluateobese childrenandadolescentsinspontaneousbreathingthrough spirometryandVC,simultaneously.
Despitethescarceliterature,VCisanoptionforthe anal-ysisoflungfunctioninchildrenandadolescents,asitisan easy-to-understand test, with noneed for forced maneu-vers,being inexpensiveand notrequiring theuse ofinert gases.Additionally,itprovidesinformationonlungvolume andDSV,aswellasventilationhomogeneitythroughtheCO2 exhalationslopes.
In the present study,it wasobserved that obese indi-vidualshavegreaterlungvolumesthanhealthyindividuals (TValvandVCO2)andlowervaluesofDSV/TVandSlp3/TV.
A
1400 0.4
0.3
0.2
0.1
0.0
–3 –2 –1 0 1 2 3 4 1200
1000 800 600 400 200
0
–200 –400
450 60
50 40 30 20 10 0 –10 –20
0.4 0.3 0.2 0.1 0.0 –0.1 –0.2 400
350 300 250 200 150 100 50
–3 –2 –1 0 1 2 3 4 –3 –2 –1 0 1 2 3 4
–3 –2 –1 0 1 2 3 4 –3 –2 –1 0
BMI z-score
BMI z-score
BMI z-score
BMI z-score
BMI z-score
TV
alv
VCO
2
DSV/TV
Slp
3
Slp
3
/TV
2
1 3 4
B
D
C
E
Figure2 Linearregressionofthevolumetriccapnographyvariablesinfluencedbythebodymassindex(BMI)z-score.(A)
Alve-olartidal volume (TValv): y=335.26+47.45x; *p=0.050;(B)ratio between thedead spacevolume andtidal volume (DSV/TV):
y=0.24−0.02x;**p=0.003;(C)exhaledcarbondioxide volume(VCO
2):y=209.98+18.51x;†p=0.003);(D)phase3-slope (Slp3):
y=19.32−2.32x;‡p=0.041;(E)phase-3slopecorrectedbytidalvolume(Slp
3/TV):y=0.08−0.01x;§p=0.044.
The explanation for lower values in Slp3/TV in obese individuals is consistent withthe findings of Ream etal., whoevaluatedchildrenandadolescentswhowereintubated andsubmitted tominor surgeries and found lower values ofSlp3 in individualswithhigher TVanda negative asso-ciationbetweenSlp3and bodyweightandsurfacearea.19 Therefore,obeseindividuals,whohavehigherweight,body surfacearea,andTVthanthecontrolgroup,showedlower Slp3/TVvalues.
The DSV/TV ratio is used to monitor respiratory dis-easeseverityinmechanicallyventilatedpatients.18,21Inthe presentstudy,lowervalueswereobservedinobesepatients thaninhealthyindividuals,indicatingabsenceofpulmonary disease.Thelowervaluesfound inobeseindividualswere influencedbythehigherTVs.
VC was shown to be a complementary tool to the spirometry, as it detected increased lung volumes during spontaneousbreathingwithoutforcedmaneuvers,afinding thatwasnotdetectedbythespirometry.However,thistool isnotcapableofdetectingchangesinrespiratoryflows.For thisreason,oneevaluationdoesnotreplacetheother,but
thecomplementaryuseofbothmayimprovetheknowledge aboutthepulmonarystatusoftheassessedindividuals.
Lungvolumeanalysiswasrelevant,mainlyafterthe sub-division of the individuals by age groups. FEV1/FVC and forcedexpiratoryflowswerealteredinthegroupaged5---11 years,aswellasinthoseolderthan11years.However,VCO2 wasdifferentonlyintheoldergroup.
The increase in lung volume may be a response to increased cardiorespiratory demand in obese individuals, especially during pubertal development, which is charac-terized by changesin body structure.28,30 However,obese patientsmayhavesmaller-caliberairwaysduetothe impair-ment of respiratory mechanics by adipose tissue. Thus, increasingvolumeinasmaller-caliberunitresultsinreduced respiratoryflows.
Lungfunctioninobeseandhealthyindividualswithoutasthma 405
whichwasmoresignificantinindividualsolderthan11years. No changes were observed in Slp3, Slp3/TV, and in the capnographyindex.Thus,thestudysuggeststhatobese indi-vidualsshowalterationsinlungflow,evenattheyoungerage groups,withoutcompromisinglungvolumesandventilation homogeneity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
MSF would like to thank the support from CAPES (Coordenac¸ãodeAperfeic¸oamentodePessoaldeNível Supe-rior). FALM would like to thank the supportfrom FAPESP (Fundac¸ão de Apoio a Pesquisa do Estado de São Paulo) [2011/12939-4];[2015/12858-5];[2015/12183-8]andFundo de Apoioà Pesquisa, ao Ensino e à Extensão da Universi-dadedeCampinas[648/2015].JDRwouldliketothankthe supportfromFAPESP[2011/18845-1];[2015/12183-8].
References
1.Obesity:preventingandmanagingtheglobalepidemic.Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i---xii,1---253.
2.EbblingCB,PawlakDB,LudwigDS.Childhoodobesity: public-healthcrisis,commonsensecure.Lancet.2002;360:473---82. 3.HuangJS,BarlowSE,Quiros-TejeiraRE,ScheimannA,
Skele-tonJ,SuskindD,etal.Consensusstatement:childhoodobesity forpediatricgastroenterologists.JPediatrGastroenterolNutr. 2012;56:99---109.
4.ShoreSA.Obesityandasthma:possiblemechanisms.JAllergy ClinImmunol.2008;121:1087---93.
5.KingGG,Brown NJ,DibaC,ThorpeCW,Mu˜nozP,MarksGB, etal.Theeffectsofbodyweightonairwaycaliber.EurRespir J.2005;25:896---901.
6.ChapmanDG,BerendN,King GG,SalomeCM.Increased air-wayclosureis a determinantofairway hyperresponsiveness. EurRespirJ.2008;32:1563---9.
7.PereiraCA.Espirometria.JPneumol.2002;28:s2---82.
8.ChenY,RennieD,CormierY,DosmanJA.Waistcircumference associatedwithpulmonary function in children. Pediatr Pul-monol.2009;44:216---21.
9.HeQQ,WongTW,DuL,JiangZQ,QiuH,GaoY,etal. Respira-toryhealthinoverweightandobeseChinesechildren.Pediatr Plmonol.2009;44:997---1002.
10.LazarusR, ColditzG, BerkeyCS, SpeizerFE. Effectsofbody fatonventilatorfunctioninchildren:cross-sectionalfindings fromarandompopulationsampleofschoolchildren.Pediatr Pulmonol.1997;24:187---94.
11.PekkarinenE,VanninenE,LãnsimiesE,KokkarinenJ,Timonen KL.Relationbetweenbodycomposition,abdominalobesityand lungfunction.ClinPhysiolFunctImaging.2012;32:83---8. 12.ÜlguerZ,DemirE,Tanac¸R,GöskenD,GülenF,DarcanS,etal.
Theeffectofchildhoodobesityonrespiratoryfunctionstests andairwayhyperresponsiveness.TurkJPediatr.2006;48:43---50. 13.SpathopoulosD,ParaskakisE,TrypsianisG,TsalkidisA, Arvaniti-douV,EmporiadouM,etal.Theeffectofobesityonpulmonary
lungfunctionofschoolaged childreninGreece.Pediatr Pul-monol.2009;44:273---80.
14.EisenmannJC,ArnallDA,KanuhoV,InterpretterC,CoastJR. Obesityandpulmonaryfunction inNavajoandHopichildren. EthDis.2007;17:14---8.
15.Boran P, Tocuk G, Pisgin B, Oktem S, Yegin Z, Bostan O. Impact ofobesity on ventilatoryfunction.J Pediatr (Rio J). 2007;83:171---6.
16.QuanjerPH,StanojevicS,ColeTJ,BaurX,HallGL,CulverBH, etal.Multi-ethnicreferencevaluesforspirometryfor3---95yr agerange:thegloballungfunction2012equations.EurRespir J.2012;40:1324---43.
17.FletcherR,JonsonB,CummingG,BrewJ.Theconceptof dead-spacewithspecialreferencetothesinglebreathtestforcarbon dioxide.BrJAnaesth.1981;53:77---88.
18.RomeroPV,LucangeloU,LopezAguilarJ,FernandezR,Blanch L. Physiologically based indices of volumetric capnography in patients receiving mechanical ventilation. Eur Respir J. 1997;10:1309---15.
19.Ream RJ, Schreiner MS, Neff JD, Mc Rae KM, Jawad AF, SchererPW,etal.Volumetriccapnographyinchildren. Influ-enceofgrowthonthealveolarplateauslope.Anesthesiology. 1995;82:64---73.
20.BöhmSH,MeischS,vonSanderslebenA,ThammO,PassoniI, ArcaJM,etal.Theeffectsoflungrecruitmentonthephase IIIslopeofvolumetriccapnographyinmorbidlyobesepatients. AnesthAnalg.2009;109:151---9.
21.Blanch L, Romero PV, Lucangelo U. Volumetric capnogra-phy inmechanically ventilatedpatient. MinervaAnesthesiol. 2006;76:577---85.
22.VeronezL, PereiraMC, daSilvaSM,Barcaui LA,De Capitani EM,MoreiraMM,etal.Volumetriccapnographyforthe evalua-tionofchronicairwaydisease.IntJChronObstructPulmonDis. 2014;23:983---9.
23.Qi GS, GuWC,Yang WL,XiF,Wu H, Liu Jm.The abilityof volumetriccapnograhytodistinguishbetweenchronic obstruc-tive pulmonary disease patients and normal subjects. Lung. 2014;192:661---8.
24.FouzasS,HäckiC,LatzinP,ProiettiE,SchulzkeS,FreyU,etal. Volumetriccapnographyininfantswithbronchopulmonary dys-plasia.JPediatr.2014;164:283---8.
25.Ribeiro MA, Silva MT, Ribeiro JD, Moreira MM, Almeida CC, Almeida-Junior AA, et al. Volumetric capnography as a tool to detect early peripheric lungobstruction in cysticfibrosis patients.JPediatr(RioJ).2012;88:509---17.
26.FuchsSI, JungeS,EllemunterH, BallmannM,GappaM. Cal-culationofthecapnographicindexbasedonexpiratorymolar mass-volume-curves---asuitabletooltoscreenforcysticfibrosis lungdisease.JCystFibros.2013;12:277---83.
27.Almeida CC, Almeida-Junior AA, Ribeiro MA, Silva MT, Ribeiro JD. Volumetric capnography to detect ventilation inhomogeneityinchildrenandadolescentswithcontrolled per-sistentasthma.JPediatr(RioJ).2011;87:163---8.
28.BiroFM,KhouryP,MorrisonJA.Influenceofobesityontiming ofpuberty.IntJAndrol.2006;29:272---7.
29.Bar-OrO,RowlandTW.Physiologicalandperceptualresponses toexerciseinthehealthchild.In:Pediatricexercisemedicine ---fromphysiologicalprinciplestohealthcareapplication.Human Kinetics;2004.p.03---58.