PSYCHOCULTURAL MEANI NGS OF URI NARY I NCONTI NENCE I N W OMEN: A REVI EW
Rosân gela Higa1 Mar ia Helena Baena de Mor es Lopes2 Egber t o Ribeir o Tur at o3
Higa R, Lopes MHBM, Tu rat o ER. Psy ch ocu lt u ral m ean in gs of u r in ar y in con t in en ce in w om en : a r ev iew. Rev Lat ino- am Enfer m agem 2008 j ulho- agost o; 16( 4) : 779- 86.
The purpose of t he present st udy was t o ident ify and analyze st udies in healt h lit erat ure about t he psychocult ural m eanings report ed by w om en w ho experience urinary incont inence ( UI ) . A bibliographical search w as execut ed in t he follow ing dat abases: Lilacs, Medline, Pubm ed and Medscape. The pr esent r ev iew show ed t hat st udies not e sev er al m eanings. The ar t icles w er e gr ouped in t hr ee cat egor ies defined as significant : accor ding t o age ex per iences, cult ur al- r eligious ex per iences and ex per iences in self- car e. The st udies r ev ealed t hat t he degr ee of anguish and t he range of t he difficult ies experienced are relat ed bot h wit h age, et hnic group or religion and w it h t h e per cept ion each in div idu al h as of h er in con t in en ce, w h ich w ill lead t o differ en t lev els of em ot ion al disor der s and t o seeking ( or not seeking) t r eat m ent . Besides, bar r ier s r egar ding self- car e ar e per ceiv ed. I t is concluded t hat t he UI m ay cause suffer ing and incont inent w om en have difficult ies t o deal w it h t his pr oblem .
DESCRI PTORS: nur sing; w om en’s healt h; ur inar y incont inence; r ev iew lit er at ur e; psy chosocial im pact
SI GNI FI CADOS PSI CO-CULTURALES PARA LA I NCONTI NENCI A URI NARI A FEMENI NA:
UNA REVI SI ÓN
El obj et ivo del pr esent e t r abaj o fue ident ificar y analizar est udios en salud que t r at aban sobr e los significados psico- cult urales de m uj eres que pasaron por incont inencia urinaria ( I U) . Fue realizada una búsqueda bibliográfica en las bases de dat os: Lilacs, Medline, Pubm ed e Medscape. La present e revisión m ost ró est udios que present an plur alidad de significados. Los ar t ículos fuer on agr upados en t r es cat egor ías: v iv encias segun el gr upo et ár eo, v iv en cias cu lt u r ales- r elig iosas y v iv en cias sob r e el au t ocu id ad o. La in v est ig ación m ost r ó q u e, el g r ad o d e an gu st ia v iv ida y las dificu lt ades se en cu en t r an r elacion adas con la edad, et n ia o r eligión , así com o por la per cepción que cada indiv iduo t iene sobr e la incont inencia, lo cual lo llev ó a difer ent es gr ados de t r ast or no em ocional y a buscar ( o no) t rat am ient o. De la m ism a form a se perciben barreras en cuant o a su aut ocuidado. Se concluye que la I U puede causar sufrim ient o y que las m uj eres con incont inencia enfrent an dificult ades para m an ej ar est e pr oblem a.
DESCRI PTORES: enferm ería; salud de la m uj er; incont inencia urinaria; lit erat ura de revisión; im pact o psicosocial
SI GNI FI CADOS PSI COCULTURAI S DA I NCONTI NÊNCI A URI NÁRI A FEMI NI NA:
UMA REVI SÃO
O ob j et iv o d o p r esen t e t r ab alh o f oi id en t if icar e an alisar est u d os d a lit er at u r a em saú d e q u e ab or d assem sign if icados psicocu lt u r ais r elat ados por m u lh er es qu e v iv en ciam a in con t in ên cia u r in ár ia ( I U) . Realizou - se busca bibliográfica nas bases de dados Lilacs, Medline, Pubm ed e Medscape. A present e revisão ident ificou que est u d os ap on t am p olissem ia d e sig n if icad os. Os ar t ig os f or am ag r u p ad os em t r ês cat eg or ias eleit as com o r elev ant es: v iv ências segundo a faix a et ár ia, v iv ências cult ur al- r eligiosas e v iv ências quant o ao aut ocuidado. A pesquisa r ev elou que o gr au de angúst ia ex per im ent ado e a am plit ude das dificuldades est ão r elacionados t ant o com a idade, et nia ou r eligião, quant o com a per cepção que cada indivíduo t em de sua incont inência, o que levará aos diferent es níveis de t ranst orno em ocional e por procura ( ou não) de t rat am ent o. Além disso, há bar r eir as per cebidas n a m an u t en ção do au t ocu idado. Con clu i- se qu e a I U pode ger ar sof r im en t o e qu e as m ulher es incont inent es enfr ent am dificuldades par a lidar com esse pr oblem a.
DESCRI TORES: enferm agem ; saúde da m ulher; incont inência urinária; lit erat ura de revisão; im pact o psicossocial
1 RN, Cam pinas St at e Universit y, doct oral st udent , e- m ail: [email protected] .br; 2 RN, Free Lect ure, Associat e Professor, e- m ail: m hbaena@fcm .unicam p.br;
3 Physician, Free Lect urer, Facult y, e- m ail: ert urat [email protected] .br. School of Medical Sciences, Cam pinas St at e Universit y, Brazil.
I NTRODUCTI ON
U
r inar y incont inence ( UI ) affect s t he w or ldpopulat ion, especially t he fem ale populat ion: One out
of fiv e w om en has alr eady ex per ienced sy m pt om s of
t h i s d i s e a s e( 1 ). I n w o m e n , U I m a y o c c u r m o r e
f r eq u en t ly d u e t o: st r ess u r in ar y in con t in en ce, i. e.
exert ing pressure on t he abdom inal region, sneezing,
co u g h i n g , l a u g h i n g o r d o i n g sp o r t s; i n ca se s o f
ov eract iv e bladder, w it h ur ge- incont inence, it occur s
w it h a st r ong, incont r ollable ur ge t o ur inat e, w it h a
high chance of losing urine if a rest room is not found;
and m ix ed incont inence, w hen t her e is loss of ur ine
associat ed t o bot h sit u at ion s, i. e. it is pr eceded by
effor t s and sy m pt om s of ur gency( 2).
Th e o c c u r r e n c e o f u r i n a r y l o s s i n t h e s e
sit uat ions im plies psychosocial consequences t hat are
m ore devast at ing t han physical healt h sequelae, w it h
m u lt ip le an d w id esp r ead ef f ect s t h at r est r ict d aily
act ivit ies, social int eract ion, t he self- percept ion of t he
st at e of healt h and qualit y of life for t he incont inent
wom an, when com pared wit h a cont inent . Considering
people over 60 years old, according t o t he evaluat ion
of qualit y of life m easured by t he I ncont inence I m pact Qu est ion n air e ( I I Q) , em ot ion al f act or s w er e sh ow n
t o b e t h e m o st a f f ect ed . Nea r l y o n e t h i r d o f t h e
r e s p o n d e n t s m e n t i o n e d n e r v o u s n e s s , s h a m e o r
fr ust r at ion because of t heir UI ; t he social dom inance
and fear of t he odor scored as highest im pac( 3), since
u r in ar y loss r est r ict s con t act w it h co- w or k er s( 4 ) an d
phy sical pr ox im it y w it h people in gener al( 5).
I n c o n t i n e n c e a f f e c t s p e o p l e o f a l l a g e s ,
r egar dless of socioeconom ic and cult ur al condit ions,
a n d i t f r e q u e n t l y a f f e c t s t h e g r o u p s w i t h m o r e
lim it at ions in t he search for help m ore int ensely, such
as elder ly or ph y sically disabled people. Sin ce it is
on e of t h e so- called silen t p r ob lem s in Ger iat r ics,
cau sed b y t h e p h y siolog ical d eclin e of t h e eld er ly
per son, it can influence a cer t ain lack of int er est by
healt hcar e pr ofessionals( 6 ), par t icular ly nur ses, w ho,
i n t u r n , b a s e t h e m s e l v e s o n o l d m y t h s a n d
st ereot ypes, such as t he belief t hat t he elderly accept
UI as a nat ural consequence of t heir advancing age( 7).
Con seq u en t ly, it can also in f lu en ce t h e v alid it y of
invest ing in UI t reat m ent for people in t his age range( 6).
S u c h f a c t o r s m a y l e a d t h e n u r s e t o a n
incorrect evaluat ion of t he care for incont inent elders,
b o t h i n t h e i d e n t i f i ca t i o n o f t h e p r o b l e m a n d i t s
handling. The conflict of est ablishing clinical priorit ies
for t he nur sing t eam , as w ell as educat ional deficit s
f o r U I , i s m e n t i o n e d a s a b a r r i e r t o p r o m o t e
con t in en ce. Th er ef or e, t h e pr of ession al t eam n eeds
t o be aw ar e of t he im pact of not t r eat ing UI for t he
e l d e r l y, a n d s h o u l d t h e n p r o m o t e t h e s t a t e o f
cont inence and develop st rat egies for t he cont ainm ent
of ur inar y loss( 7).
Since t his is a delicat e problem , oft en hidden
becau se t h e sy m pt om s ar e disr egar ded du e t o lack
of knowledge or sham e, t he fact suggest s t hat t his is
a “ h i d d en ” p r o b l em , u n d er est i m a t ed b o t h b y t h e
c a r r i e r a n d b y n u r s e s a n d o t h e r h e a l t h c a r e
pr ofession als. Kn ow ledge abou t t h e im pact of UI in
t he populat ion, it s t ypes and causes, are fundam ent al
aspect s t o be considered when evaluat ing t he problem
a n d , co n se q u e n t l y, w h e n d i a g n o si n g a p p r o p r i a t e
act ions( 6 ).
I n v i e w o f w h a t w a s e x p o se d a b o u t t h i s
u r i n a r y d y sf u n ct i o n , t h e n e e d t o a n a l y ze st u d i e s
inv olv ing nar r at iv es of w om en w it h UI is consider ed
a p r i o r i t y a n d r e l e v a n t t o u n d e r s t a n d t h e i r
experiences, as well as em ot ional react ions associat ed
t o episodes of ur inar y loss and t he m eanings r elat ed
t o t he phenom enon. Thus, im port ant cont ribut ions will
b e g at h er ed so t h at h eal t h car e p r o f essi o n al s can
im pr ov e t heir psy chological focus and t he int er est in
Th e a u t h o r s u n d e r s t a n d t h a t s t u d i e s
perform ed wit h wom en suffering from UI are t ools t o
ev id en ce v iew s an d f eelin g s of in con t in en t p eop le
about t heir problem and t heir at t it udes in t he face of
urinary loss. Therefore, t he goal of t he present st udy
w a s t o i d en t i f y a n d a n a l y ze h ea l t h ca r e l i t er a t u r e
st udies about t he psy chocult ur al m eanings r epor t ed
by w om en ex per iencing UI .
METHOD
This is a lit er at ur e r ev iew , aim ing t o gat her
and synt hesize exist ing knowledge about t he proposed
t opic: t h e m ean in gs of UI f or w om en . Th e r ev iew s
were carefully developed, since t he am ount of st udies
about t he t opic consider ed her e is not lar ge.
To support t he discussion, a lit erat ure review
was perform ed in t he following dat abases: Lilacs ( Lat
in-Am er i ca n a n d Ca r i b b ea n Li t er a t u r e i n Hea l t h ca r e
S e r v i c e s ) , Me d l i n e ( I n t e r n a t i o n a l Li t e r a t u r e i n
Healt hcare Sciences) , Pubm ed and Medscape. Art icles
w e r e s e l e c t e d b y u s i n g t h e k e y w o r d s u r i n a r y , incont inence, fem ale, qualit at ive st udy and qualit y of life accor ding t o t he aut hor s’ m et hodological opt ion. Regar ding t he obj ect s of st udy, t he ar t icles select ed
should hav e been w r it t en in Por t uguese, Spanish or
English, and published aft er 1990.
Th e r esu lt s of t h e elect r on ic sear ch es w er e
evaluat ed and select ed t o ret rieve art icles considered
r e l e v a n t a n d e x c l u d e t h o s e o f l e s s e r a c a d e m i c
im p or t an ce in t h e au t h or s’ v iew . Fou r st ag es w er e
t h en per f or m ed: ( a) select ion of t h e ar t icles in t h e
chosen dat abases and, based on t heir t it les, inclusion
and analysis of t he t ext s t hat referred t o UI in wom en,
ex cluding t hose focusing on UI in childr en and m en;
( b) select ion of t he ar t icles by car efully r eading t he
a b st r a ct s, w i t h t h e st u d i e s b e i n g d o n e u n d e r a
qualit at iv e m et hodological focus, i. e. t hose cov er ing
t he r epor t ed ex per iences and r est r ict ions caused by
u r in ar y loss. Ar t icles w it h an epidem iological f ocu s,
inst rum ent validat ion and evaluat ion of qualit y of life
u sin g scales w er e ex clu d ed . ( c) Wh en look in g f or
in t egr al ar t icles for t h e locat ion of t h e pu blicat ion s,
t he follow ing r esour ces w er e used: t he bibliogr aphic
com m ut ing ser v ice and t he ar chiv es of t he libr ar y of
t he Facult y of Medical Sciences at t he Univer sit y of
Cam p in as ( UNI CAMP) , sear ch es in Cap es’ Por t al of
Jour nals t hr ough t he sear ch engine of t he Elect r onic
Library of Unicam p and t he Scient ific Elect ronic Library On lin e ( SciELO) ; an d ( d ) cr it ical ev alu at ion of t h e ar t i cl es, af t er r ead i n g t h em i n t eg r al l y. Sev en t een
st u d ies w er e t h er ef or e in clu d ed in a f in al an aly sis,
p er f or m ed w it h a q u alit at iv e f ocu s, as w ell as t w o
r ecen t Br azilian j ou r n als, w h ose f u n d am en t als an d
a r g u m en t a t i o n m a t ch ed t h e p r o p o sed t h em e a n d
com plem ent ed t he r elevant t hem es of t he qualit at ive
ap p r oach . Fin ally, 1 9 b ib liog r ap h ic r ef er en ces w er e
consider ed per t inent for t his ar t icle.
Af t er r e- r eadin g t h e cor pu s ( t h e f u ll set of collect ed m at er ial) , st u dies w er e obser v ed t o poin t
out a variet y of m eanings, as expect ed from research
r e s u l t s i n H u m a n i t i e s . Th e d a t a w e r e a n a l y z e d
according t o t he result s t hat em erged in t he published
st u dies an d gr ou ped in cat egor ies/ t opics. Aim in g t o
u n d er st an d t h e m ean in g s t h e w om en at t r ib u t ed in
issues r elat ed t o t heir ex per ience w it h ur inar y loss,
t h e d a t a a n a l y s i s w a s b a s e d o n p s y c h o s o c i a l
r ef er en ces.
The cat egorizat ion of t he st udies consist ed in
t he definit ion of t he infor m at ion, t ak ing int o account
t h e ex per ien ces r epor t ed in t h e qu alit at iv e st u dies,
gr ou ped by t h em at ic r elev an ce; occasion ally in t h e
repet it ion of t he addressed t opic, as well as t he clinical
ex per ience of t he r esear ch pr ofessionals’ t heor et ical
k n ow led g e. Th e st u d ies g at h er ed w er e g r ou p ed in
t hree cat egories, seen as prom inent : ( 1) Experiences
a c c o r d i n g t o a g e r a n g e ; ( 2 ) Cu l t u r a l - r e l i g i o u s
e l c i t r a e h t f o e l t i
T Method Approach Journal Year
y r a n i r u f o e c n e i r e p x e s ' n e m o w r e d l o g n i r e v o c s i D . 1 e c n e n it n o c n i t n e t n o c ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q s i s y l a n a e g n a r e g
A ResearchNursing
h tl a e H
& 1991
e r a c -fl e S y d u t s e v it a t il a u q a : e c n e n it n o c n i f o g n i n a e m e h T . 2 s r e f f u s e c n e n it n o c n i y r a n i r u c i r t a i r e g -n o n f o ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q s i s y l a n a l a c i g o l o h c y s p e g n a r e g
A Journalof
g n i s r u N d e c n a v d
A 1993
s u o i g il e r -l a r u tl u C y r a n i r u h t i w n e m o w d n a s r e n o it it c a r p l a r e n e G . 3 e c n e n it n o c n i ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . g n il p m a s l u f e s o p r u p ; s i s y l a n a c it a m e h
t Sefl-care
f o l a n r u o J h s it i r B e c it c a r P l a r e n e
G 1998
r e d l o y b e c n e n it n o c n i y r a n i r u o t e s n o p s e R . 4 y t i n u m m o c e h t n i g n i v il s n o s r e p ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . e r a w t f o s c i h p a r g o n h t e ; s i s y l a n a c it a m e h
t Sefl-care
d n u o W f o l a n r u o J d n a y m o t s O e c n e n it n o C g n i s r u N 8 9 9 1 y r a n i r u h t i w e l p o e p n i g n i k e e s p l e h o t s r e i r r a B . 5 s m o t p m y s ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . e l p m a s m o d n a r ; s i s y l a n a c it a m e h t e g n a r e g A e c it c a r P y li m a
F 2001
s u o i g il e r -l a r u tl u C e r a c -fl e S s e c n e i r e p x e d n a s n o it p e c r e p s ' n e m o w i n a t s i k a P . 6 e c n e n it n o c n i f o t n e t n o c ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q s i s y l a n a s u o i g il e r -l a r u tl u C d r a d n a t S g n i s r u
N 2001
e r a c -fl e S g n i k e e s m o r f e l p o e p r e d l o s t n e v e r p t a h W . 7 e v it a t il a u q A ? e c n e n it n o c n i y r a n i r u r o f t n e m t a e r t y t i n u m m o c f o e s u e h t o t s r e i r r a b f o n o it a r o l p x e . s e c i v r e s e c n e n it n o c t n e t n o c ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . g n il p m a s l u f e s o p r u p ; s i s y l a n
a Sefl-care FamliyPracitce 2004
e l a m e f m r e t -g n o l r o f l e d o m l a r u tl u c a g n i p o l e v e D . 8 e c n e n it n o c n i y r a n i r u l a r u tl u c ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q s i s y l a n a l e d o m e g n a r e g A & e c n e i c S l a i c o S e n i c i d e
M 2006
s u o i g il e r -l a r u tl u C e r a c -fl e S n i e c n e n it n o c y r a n i r u e t o m o r p s e s r u n o D . 9 y d u t s y r o t a r o l p x e n A ? e l p o e p r e d l o d e z il a t i p s o h ; s i s y l a n a t n e t n o c ; p u o r g s u c o f ; y d u t s e v it a t il a u Q . g n il p m a s l u f e s o p r u
p Cutlural-reilgious
l a c i n il C f o l a n r u o J g n i s r u
N 2006
: a n i h C n i e c n e n it n o c n i y r a n i r u e l a m e F . 0 1 s e v it c e p s r e p d n a s e c n e i r e p x e ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . s i s y l a n a l a c i g o l o n e m o n e h p e v it a t e r p r e t n i s u o i g il e r -l a r u tl u
C HeatlhCarefor
n e m o W l a n o it a n r e t n I 6 0 0 2 e r a c -fl e S e f il s ' n e m o w n i s n o it c i r t s e r e c n e n it n o c n i y r a n i r U . 1
1 Quanittaitvestudy;structuredinterview;descripitve
. s i s y l a n a e g n a r e g
A RevistadaEscola
m e g a m r e f n E e d P S U a d 6 0 0 2 e r a c -fl e S h s i k r u T d n a n a c c o r o M n i e c n e n it n o c n i y r a n i r U . 2 1 d n a t c a p m i n o y d u t s e v it a t il a u q a : n e m o w t n e m t a e r t r o f s e c n e r e f e r p ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . n o it a r u t a s y b g n il p m a s ; s i s y l a n a c it a m e h t s u o i g il e r -l a r u tl u
C BriitshJournalof
e c it c a r P l a r e n e
G 2006
e r a c -fl e S h t i w g n i p o c n i s e c n e i r e p x e s ' n e m o w e s e n i h C . 3 1 e c n e n it n o c n i y r a n i r u t n e t n o c ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . g n il p m a s l u f e s o p r u p ; s i s y l a n
a Cutlural-reilgious
l a c i n il C f o l a n r u o J g n i s r u
N 2007
s ' n e m o w : e c n e n it n o c n i s s e r t s h t i w g n i p o C . 4 1 s e c n e n it n o c n i y a d y r e v e f o s e c n e i r e p x e t n e t n o c ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q . g n il p m a s l u f e s o p r u p ; s i s y l a n
a Sefl-care
l a n o it a n r e t n I f o l a n r u o J g n i s r u N l a c i g o l o r U 7 0 0 2 a : e r a c e c n e n it n o c e v it i s n e s y ll a r u tl u C . 5 1 n e m o w n a i d n I n a i s A h t u o S g n o m a y d u t s e v it a t il a u q . r e t s e c i e L n i d n a c it a m e t s y s ; p u o r g s u c o f ; y d u t s e v it a t il a u Q . g n il p m a s l u f e s o p r u p ; s i s y l a n a e v it a r e t i s u o i g il e r -l a r u tl u C e c it c a r P y li m a
F 2007
e r a c -fl e S -e r a c s ' n e m o w s t i b i h n i n o it a il i m u h f o r a e F . 6 1 e c n e n it n o c n i y r a n i r u m r e t -g n o l r o f r o i v a h e b g n i k e e s ; s c it u e n e m r e h l a c i g o l o n e m o n e h p : y d u t s e v it a t il a u Q ; s y s il a n a l a i c o s o h c y s p ; w e i v r e t n i d e r u t c u r t s -i m e s . g n il p m a s l u f e s o p r u p e g n a r e g
A Scandinavian
g n i r a C l a n r u o J e c n e i c S 7 0 0 2 e r a c -fl e S e v il f o s e i r o t s s ' n e m o w y l r e d l e : e r o m o n t n e li S . 7 1 e r a c m r e t -g n o l n i e c n e n it n o c n i y r a n i r u h t i w ; w e i v r e t n i d e r u t c u r t s -i m e s ; y d u t s e v it a t il a u Q ; s i s y l a n a c it a m e h
t Sefl-care
l a n r u o J y g o l o t n o r e G g n i s r u N 7 0 0 2 e l a m e f n o e c n e n it n o c n i y r a n i r u f o t c a p m i e h T . 8 1 l e n n o s r e p g n i s r u n e v it p i r c s e d ; w e i v r e t n i d e r u t c u r t s ; y d u t s e v it a t it n a u Q . g n il p m a s l u f e s o p r u p ; s i s y l a n a e g n a r e g
A RevistaBraslieira
m e g a m r e f n E e
d 2007
e r a c -fl e S g n i v il f o e c n e i r e p x e s ' n e m o w f o g n i n a e m e h T . 9 1 s i e c n e n it n o c n i y r a n i r u m r e t -g n o l h t i w . s s e n s s e l r e w o p ; s c it u e n e m r e h l a c i g o l o n e m o n e h p : y d u t s e v it a t il a u Q ; s y s il a n a l a i c o s o h c y s p ; w e i v r e t n i d e r u t c u r t s -i m e s . g n il p m a s l u f e s o p r u p s u o i g il e r -l a r u tl u
C JournalofCilnical
g n i s r u
N 2007
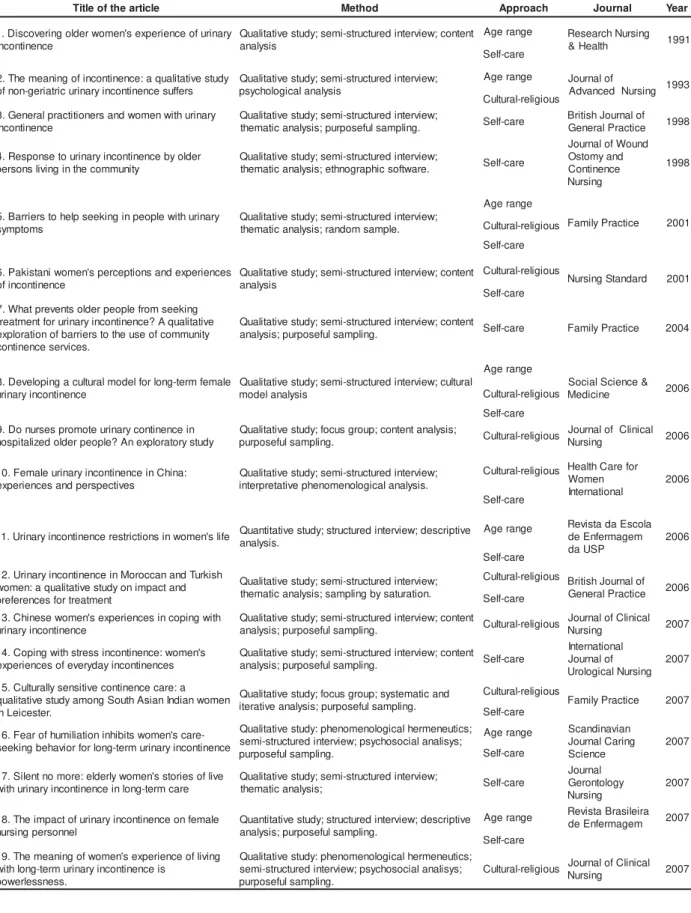
Table 1 – Publicat ions according t o t he t it le of t he art icle, t he m et hod used, t hem es addressed, j ournal and year
of publicat ion, 2007
EXPERI ENCES ACCORDI NG TO AGE RANGE
Nowadays, t he UI experiences of older wom en
are invest igat ed m ore oft en, probably due t o it s high
prevalence aft er t he m enopause, alt hough psychosocial
alt er at ions seem t o be ex pr essiv e in all age r anges.
The sym bolic aspect s, however, are shown to be different
For wom en over 60 years old, t he feelings of
ur inar y loss com e about built and “ negot iat ed” as a
r esu lt of in div idu al an d sh ar ed ex per ien ces( 8 ); t h ey
are associat ed wit h t he idea t hat t his is an inevit able
ph en om en on , a con sequ en ce of adv an cin g age an d
an im plicat ion of t he am ount of children delivered. The
w o m en d escr i b e i n co n t i n en ce as a d eg en er a t i v e
process(9), and a condition inherent to their life history(8).
A m o n g y o u n g a n d m i d d l e - a g e d w o m e n
( under 50 y ear s old) , t he pr oblem is per ceiv ed as a
p e r so n a l d y sf u n ct i o n , w i t h a l o ss o f t h e h e a l t h y p r o p e r t i e s o f t h e b o d y, t h u s f a ci n g a si g n i f i ca n t
d if f icu lt y in cop in g w it h t h e d isease. Becau se t h ey
con sider UI a t aboo, t h ey see t h is ph en om en on as
unaccept able for social life and feel socially despised
a n d g u i l t y i n t h e f a ce o f a co n se q u e n t r e p u l si v e
r eact ion fr om t he gr oup and abandonm ent by a par t
of societ y( 10).
Eld er ly w om en ex p lain ed t h at accid en t s or
ot her pr oblem s r elat ed t o UI w er e a t hr eat t o t heir
self - est eem , w it h t h is t h r eat en cou r ag in g t h em t o
develop efficient syst em s of care for cont inence, which
helped t o prot ect t heir self- est eem . I f t hey succeeded,
t h ey cou ld p ossib ly accep t UI an d lead a “ n or m al”
lifest y le( 11).
S o m e o f t h e y o u n g e r w o m e n r e p o r t e d
experiencing t he charact erist ic feelings of t he urinary
sym pt om s w it h indiffer ence, or even under est im at ing
t h em . I t is r em ar k ab le t h at t h ey ar e ab le t o k eep
norm alit y, since t here seem t o be negat ive defensive r esponses, because it inv olv es a lar ge adj ust m ent of
e f f o r t s w i t h b e h a v i o r s t h a t a r e ch a r a ct e r i st i c o f
con t in en t people, an d t h ey fr equ en t ly do n ot follow
t he rat ional pat hways t o cope wit h t he problem( 10).
Th e l a ck o f co n t r o l o v e r UI d u r i n g so ci a l
act iv it ies is sh ow n t o b e p r esen t , w it h ev id en ce of
psy chological im plicat ions in leisur e, pr ofessional and
f am ily lif e. Wom en m en t ion t h e f ear of losin g t h eir
j obs or changing t heir work funct ions because of labor
r e st r i ct i o n s, ca u si n g l i m i t a t i o n s i n a ct i v i t i e s t h a t
dem and physical effort , and const ant int errupt ions t o
g o t o t h e r est r o o m b ecau se o f h i g h er m i ct u r i t i o n
frequency( 4- 5). For elderly wom en, t he fear of t he odor
was shown t o have a high im pact on social rest rict ions,
wit h t he m ost affect ed pract ices being going t o places
where t here is no rest room and t aking longer t rips( 5).
A m o n g t h e y o u n g e r w o m e n , b e s i d e s t h e
afor em ent ioned com plaint s, t hey r epor t sham e w hen
t his “ disgr ace” happens in public, especially in social
event s w it h fr iends and dur ing spor t s pr act ice( 4- 5).
Since beaut y car e is applied t o t he body in
t he frequent idolat ry of physical shape, added t o t he
fact t hat wom en usually t end t o desire wit h t heir whole b od ies, w it h sex u alit y d ist r ib u t ed acr oss t h e w h ole body and not cent er ed only in t he genit al or gans( 12),
u r in ar y loss r est r ict s sex u al in t er act ion , sin ce t h ey
i m a g i n e t h e m s e l v e s a s u n a t t r a c t i v e . Fo r y o u n g
wom en, t his would point t o an “ early old age”, which
t hey norm ally t end t o abhor, feeling sham e in t he face
of clear ev idence of loss of self- est eem , highlight ed
b y t h e f ear o f r ej ect i o n i n sex u al act i v i t y d u e t o
incont inence, guilt about not feeling desire or pleasure
and about losing urine during t he orgasm( 5). The im pact
of UI w as f elt in in t im at e r elat ion sh ip s: sex u al lif e
w as inhibit ed due t o it s lack of spont aneit y, needing
t o be planned, int erfering in t he sexualit y of t he wom en
and t heir par t ner s( 13).
The several aspect s m ent ioned by t he wom en
a r e r e l a t e d t o t h e p s y c h o d y n a m i c a n d c u l t u r a l
m e a n i n g s a t t r i b u t e d t o t h e b o d y. B o d y - r e l a t e d
m eanings change w it h age, since elderly w om en saw
UI as a nat ural condit ion of aging. Am ong t he younger
w om en , it seem s t o m ean loss of con t r ol ov er t h e b o d y. Fe e l i n g s , s t a t e m e n t s a n d p r a c t i c e s w e r e
obser v ed t o be associat ed t o t he body, em bedded in
int erpersonal relat ions t hat alt er t he em ot ional aspect s
of incont inent w om en.
CULTURAL-RELI GI OUS EXPERI ENCES
Lit er at ur e point s m or e fr equent ly t o st udies
p er f o r m ed w i t h w est er n w o m en , esp eci al l y i n t h e
Unit ed St at es and Eur ope. Am ong t hose w ho st udied
w om en f r om Mor occo, Tu r k ey, Pak ist an an d I n d ia,
t he populat ion w as const it ut ed by im m igr ant s liv ing
i n Eu r o p e a n c o u n t r i e s ( 1 4 - 1 6 ). Th e r e s e e m t o b e
sim ilar it ies in t h e psy ch ological m ean in gs of UI f or
w om en living in differ ent cult ur es, et hnic gr oups and
s o c i a l c o n d i t i o n s ; h o w e v e r, r e g a r d i n g r e l i g i o u s
pr act ices, t he ex per iences of incont inent w om en can
int er fer e w it h follow ing som e r eligions( 15- 16).
When sear ching for st udies about r epor t s of
east er n w o m en ex p er i en ci n g UI , t h e p sy ch o so ci al
asp ect s i n d i cat ed t h at cu l t u r al d i f f er en ces d o n o t
change t he m eanings of urinary loss, since t here were
sim ilarit ies bet ween narrat ives of west ern and east ern
w om en . Lik e w om en f r om Am er ican an d Eu r op ean
cou n t r ies( 7 - 1 1 ), t h e b od y w as ex p er ien ced as b ein g
w er e exper ienced w hen t he w om en could not cont r ol t he accident s, leading t o feelings of helplessness and
anguish( 17).
Ch in ese w om en r ep or t ed f eelin g s of g u ilt ,
l o n el i n ess an d em o t i o n al i so l at i o n( 1 8 ), d escr i b ed a p e r so n a l l o ss o f co n t r o l e v e r y t i m e t h e y w e t t e d
t hem selves w it h urine, felt st ressed w hen it occurred in public, and in front of friends. The feeling of sham e
and hum iliat ion was higher t han fear( 19). For t he I ndian wom en living in Leicest er, UK, it is possible t hat social
st igm as from t he sout hern Asian populat ion cont ribut e t o t he difficult y t hey m ay have t o discuss cont
inence-r elat ed cainence-r e w it h ot heinence-r people( 14).
I n t he subgr oup w her e t he r eligious ident it y was analyzed, such as I slam ic or Jewish, urinary loss
b e co m e s a p r o b l e m i n t h e f o l l o w i n g o f r e l i g i o u s p r ecep t s( 1 5 ). For som e Mu slim w om en , b ein g a UI
su ffer er m ean s h av in g t o be r eser v ed, isolat ed an d w it h feelin gs of low self- est eem( 1 6 ). Sim ilar t o w h at
h a p p e n s t o Je w i sh w o m e n , i n co n t i n e n ce f o r t h e
Muslim w om en led t o t he lim it at ion of r eligious life, r elat ed t o t he need of cleanliness for t he pr act ice of
pr ay er( 15- 16).
However, Muslim wom en resort t o prayers t o
m inim ize t heir anguish, but t his com fort m ay be denied d u e t o b e i n g u n cl e a n , t h e r e f o r e i n cr e a si n g t h e i r
st r ess( 16). Losing ur ine w ould r epr esent a sinful and u n c l e a n p h e n o m e n o n , e x p e r i e n c i n g p e r s o n a l
c l e a n l i n e s s a s a h e a v y b u r d e n , s i n c e t h e y f e e l physically dirt y when urinary loss occurs, and t he rit ual
of clean in g is n eeded m or e f r equ en t ly so t h at t h ey
c a n k e e p t h e m s e l v e s c l e a n( 1 5 ). Ex p e r i e n c i n g in con t in en ce du r in g t h e clean sin g cer em on y m ak es
t hem feel filt hy and im pur e because, aft er t he body cleaning, it becom es indispensable t o r epeat pr ay er s
befor e r est ar t ing t he cleansing r it uals( 15- 16).
EXPERI ENCES REGARDI NG SELF-CARE
Wom en frequent ly disregard sym pt om s when
t h e dist u r ban ces cau sed by in con t in en ce ar e sm all;
t h ey f eel ash am ed w h en t h ey h av e t o r ep or t t h eir problem t o a professional, om it t he fact in fam ily life
and gener ally suffer in silence( 4).
For som e w om en, t he m eaning of v aluat ing
a body t hat is st r ong and healt hy induces a cer t ain r e si st a n ce t o p a i n , a n d i t f r e q u e n t l y b e co m e s a
d e t e r m i n i n g f a c t o r f o r n o t s e e k i n g a m e d i c a l
appoint m ent . Oft en, t hey expect t he disease t o reach
such an int ensit y t hat it would im pede t he norm al use
o f t h e b o d y, t o t h e e x t e n t t h a t t h e p r o b l e m i s
disregarded due to the difficulties that they face when
exposing and describing the sym ptom s to the physician(20).
Em barrassm ent and sham e, associat ed t o t he
l a c k o f k n o w l e d g e a n d u n d e r s t a n d i n g a b o u t
incont inence as a disease, and ex per iencing differ ent
m ean in gs or u r in ar y loss f or each per son gen er at e
m ult iple ways of self- care, disregarding t he help of a
h ealt h car e pr of ession al. Elder ly people, ev en t h ose
w h o r eg u lar ly see h ealt h car e p r of ession als, r ar ely
speak about t heir urinary loss, probably due t o sham e
or t o t he erroneous concept ion t hat it is not a healt h
problem ( 8,18). Am ong t hose who believe t hat UI is an
i r r ev er si b l e p r ob l em an d a con seq u en ce of ag i n g ,
t h e r e s e e m s t o b e a b e t t e r a c c e p t a n c e o f t h e
sym pt om s. Alt hough t here are social and psychological
cost s, som et im es ev en for t heir ow n phy sical healt h,
success in st rat egies ut ilized t o m inim ize incont inence
also cont ribut es t o m ake t hem not reveal t he problem
t o ot hers( 21).
The int er fer ences of UI in t he r est r ict ion of
younger w om en’s ever yday act ivit ies do not seem t o
h av e an ex pr essiv e m ean in g in t h e sear ch for
self-car e t o solv e t he pr oblem( 13), w it h t he psy chological
fact or s dr aw ing at t ent ion w hen t hey r eact t o ur inar y
loss wit h apat hy or when t hey abst ain from rect ifying
act ions( 9). Ot her s exper ience ur inar y loss as a t aboo,
t r y t o m a n i p u l a t e i n co n t i n en ce i n d i f f er en t w a y s,
r ecov er t he pow er ov er t heir uncont r olled body and
cont inue liv ing nor m ally( 17).
For t h e im m ig r an t Mu slim w om en liv in g in
Eu r o p ean co u n t r i es, i n h i b i t i o n s an d l i m i t at i o n s o f
lan gu age pr ev en t t h em f r om clear ly r epor t in g t h eir
c o n d i t i o n t o t h e h e a l t h c a r e p r o f e s s i o n a l s a n d
c o m p l e t e l y u n d e r s t a n d i n g t h e o r i e n t a t i o n s t h e y
receive, which suggest s t hat inadequat e care m ay be
adopt ed( 14- 16). The inhibit ions m ay be r educed w hen
t r eat ed by a f em ale h ealt h car e pr of ession al. Th ese
wom en cope wit h urinary loss by sharing t he problem
wit h ot her wom en, and t hen develop st rat egies t o live
w i t h i n co n t i n e n ce , su ch a s t r y i n g t o r e d u ce t h e
incidence by m anaging t he episodes( 16,18). Deficiencies
in seek ing help also seem t o be r elat ed t o a lack of
k now ledge about t heir ow n anat om y, phy siology and
av ailable t r eat m ent s( 15).
On t h e o t h e r h a n d , t h e a t t i t u d e o f so m e
h ealt h car e p r of ession als m ay cau se in h ib it ion an d
pr ev ent t he w om an fr om ex pr essing her com plaint s
du r in g an appoin t m en t , in t h e sam e w ay t h at it is
ident it ies of t he populat ion receiving care. The at t it udes
a n d p r a ct i ce s o f t h e se p r o f e ssi o n a l s a r e st r o n g
bar r ier s for people t o seek counseling or help. I f t he
pr of ession als ask ed t h e w om en abou t t h eir u r in ar y
sy m p t om s r eg u lar ly, t h ey w ou ld p r ob ab ly v er b alize
t hem and seek help m ore oft en( 21- 22).
Elderly wom en wit h UI living in long- t erm st ay
i n s t i t u t i o n s r e p o r t e d c o m m o n c o n c e r n s i n t h e i r
ex per ien ces w it h u r in ar y loss, an d t h ey r epor t t h at
t h e i n st i t u t i o n a l cu l t u r e ca n i n f l u en ce ch a n g es i n
nursing pract ice relat ed t o individual care, suggest ing
oppor t u n it ies t o pr ov ide h ealt h edu cat ion m easu r es
relat ed t o qualit y of life( 23).
Pe o p l e w h o se e k t h e h e l p o f h e a l t h ca r e
p r o f e ssi o n a l s d e si r e m o r e i n f o r m a t i o n a b o u t t h e
causes, t reat m ent s and m echanism s t o deal w it h t he
problem . Wom en request bet t er int eract ion wit h t hese
professionals, and t he need for discussion and furt her
knowledge about t he t opic was ident ified( 24). The w ay
of p er f or m in g t h is com m u n icat ion is r ep or t ed as a
pr ior it y for t he diagnosis and est ablishm ent of bonds
a n d e m p a t h y t o s e e k a n d d e t e r m i n e t h e m o s t
a p p r o p r i a t e e d u c a t i o n a l m e t h o d t o f a c i l i t a t e
c o m p r e h e n s i o n , a n d t h u s c o m p l i a n c e w i t h t h e
t r eat m ent( 25).
I t i s n e ce ssa r y, e sp e ci a l l y f o r h e a l t h ca r e
professionals, t o m ake m ore effort s in order t o know
what each person feels about her condit ion, how she
deals w it h t h e pr oblem in h er day - t o- day act iv it ies
an d h ow sh e is r u led by t h e sy m bolic m ean in gs of
t h is ph en om en on .
Th e p er son al an d h ealt h car e p r of ession als’
b a r r i e r s w o m e n f a c e d w h e n t h e y s o u g h t h e l p
e n c o u r a g e t h e i m p r o v i s a t i o n o f m e a n s f o r t h e
adapt at ion of ur inar y loss, oft en inadequat e or ev en
inefficient . Wom en adopt self- care m easures as a way
t o m inim ize ur inar y loss, alt hough t hey ack now ledge
t h at m an y ar e h ar m fu l t o t h eir h ealt h , su ch as t h e
co n t i n u o u s u sa g e o f a b so r b e n t p a d s a n d h y d r i c
r est r ict ion, w hich m ay t r igger der m at ologic pr oblem s
and ur inar y infect ions( 4,5,21).
FI NAL CONSI DERATI ONS
An im p or t an t r esu lt in t h e h ealt h car e an d
b iom ed ical lit er at u r e r ev iew w as t h e ev id en ce t h at
t he st udies published about ur inar y incont inence, in
general, offer few references t o report s collect ed wit h
w om en about how dist ressing t his disease is and t he
m a n y c o n s e q u e n t p s y c h o s o c i a l p r o b l e m s , s i n c e
w et t in g on eself w it h u r in e is a v er y em b ar r assin g
p er son al ex p er ien ce.
The st udies consider ed her e r ev eal t hat t he
d e g r e e o f d i st r e ss e x p e r i e n ce d a n d t h e r a n g e o f
dif f icu lt ies ar e n ot on ly r elat ed t o age, et h n icit y or
r eligion, but also w it h t he r esponses of each per son
and how each indiv idual per ceiv es her incont inence, si n ce t h e m ean i n g s g i v en t o h eal t h car e p r o b l em s
st r uct ur e our liv es. I t is k now n t hat r esponses w it h
differ ent degr ees of em ot ional disor der s in t he face
of t h is u r in ar y p r ob lem can sh at t er t h e con f id en ce
an d r espect on e h as f or on eself, an d pr ev en t t h em
fr om seek ing help.
Re g a r d i n g t h e i m p l i c a t i o n s f o r n u r s i n g
pract ice, t hese result s can be used as a guideline for
pr ocedu r es t h at w ill low er or elim in at e t h e bar r ier s
p er cei v ed i n sel f - ca r e m a i n t en a n ce, f a ci l i t a t e t h e
execut ion of int er vent ions t o r educe ur inar y loss and
pr om ot e cont inence, w it h t he necessar y educat ional
focus that favors open discussions, during which wom en
can report and share their experiences and feelings.
REFERENCES
1 . Ag en cy f or Healt h Car e Policy an d Resear ch ( AHCPR) . Ov er v i ew : u r i n ar y i n con t i n en ce i n ad u l t s cl i n i cal p r act i ce g u id elin e u p d at e, Rock v ille, MD. Mar ch 1 9 9 6 . [ Acesso em 02 agost o 2003] . Disponível em : ht t p: / / w w w.ahcpr.gov/ clinic/ uiov er v w . ht m .
2. Abram s P, Cardoso L, Fall M, Griffit hs D, Rosier P, Ulm st en U, et al. The st andar dizat ion of t er m inology of low er ur inar y tract function: repot from the standardization sub- com m ittee of t he int ernat ional cont inence societ y. Urology 2003; 61: 37- 49. 3. Teunissen D, Van den Bosh W, Van Weel C, Lagro-Janssen TA. I t can always happen: t he im pact of urinary incont inence on elderly m en and w om en. Scand J Prim Healt h Care 2006; 2 4 ( 3 ) : 1 6 6 - 7 3 .
4. Higa R, Lopes MHBM. The im pact of ur inar y incont inence o n f e m a l e n u r s i n g p e r s o n n e l . Re v B r a s En f e r m 2 0 0 7 ; 6 0 ( 2 ) : 2 1 3 - 6 .
5 . Lo p e s M H B M , H i g a R. Re s t r i ç õ e s c a u s a d a s p e l a incont inência urinária à vida da m ulher. Rev Esc Enferm USP 2 0 0 6 ; 4 0 ( 1 ) : 3 4 - 4 1 .
6 . Rodr igu es RAP, Men des MMR. I n con t in ên cia u r in ár ia em idosos: pr opost a par a a condut a da enfer m eira. Rev. Lat ino-Am . Enfer m agem . [ per iódico na I nt er net ] . 1 9 9 4 Jul [ cit ado 2 0 0 7 Ju l 3 0 ] ; 2 ( 2 ) : 5 - 2 0 . D i s p o n ív e l e m : h t t p : / / w w w. scielo. br / pdf / r lae/ v 2 n 2 / v 2 n 2 a0 2 . pdf.
7 . D i n g w a l l L, McLa f f er t y E. D o n u r ses p r o m o t e u r i n a r y cont inence in hospit alized older people? An explorat ory st udy. J Clin Nu r s 2 0 0 6 Oct ; 1 5 ( 1 0 ) : 1 2 7 6 - 8 6 .
long-t e r m f e m a l e u r i n a r y i n co n long-t i n e n ce . So c Sci Me d . 2 0 0 6 ; 6 3 ( 1 2 ) : 3 1 5 0 - 6 1 .
9. Shaw C, Tansey R, Jackson C, Hyde C, Allan R. Barriers t o h elp seek in g in people w it h u r in ar y sy m pt om s. Fam Pr act . 2 0 0 1 Feb r u ar y ; 1 8 9 ( 1 ) : 4 8 - 5 2 .
10. Ashw ort h PD, Hagan MT. The m eaning of incont inence: a qualit at ive st udy of non- geriat ric urinary incont inence suffers. J Ad v Nu r s 1 9 9 3 ; 1 8 ( 9 ) : 1 4 1 5 - 2 3 .
11. Dow d TT. Discovering older w om en’s experience of urinary in con t in en ce. Res Nu r s Healt h . 1 9 9 1 Ju n e; 1 4 ( 3 ) : 1 7 9 - 8 6 . 1 2 . Mu r ar o RM. Sex u alidade da m u lh er br asileir a: cor po e classe social d a m u lh er b r asileir a. 5 . ed . Rio d e Jan eir o: Edit ora Rosa dos Tem pos; 1 9 9 6 .
1 3 . Hägglu n d D, Waden st en B. Fear of h u m iliat ion in h ibit s w o m e n ’ s c a r e - s e e k i n g b e h a v i o r f o r l o n g - t e r m u r i n a r y in con t in en ce. Scan d J Car in g Sci 2 0 0 7 ; 2 1 : 3 0 5 – 1 2 . 14. Doshani A, Pit chfor t h E, Mayne CJ, Tincello D. Cult ur ally sensit iv e cont inence car e: a qualit at iv e st udy am ong Sout h Asian I ndian w om en in Leicest er. Fam Pract . 2007; 24: 585-9 3 .
1 5 . Van d en Mu i j sen b er g ME, Lag r o - Jan ssen TA. Ur i n ar y incont inence in Mor occan and Tur k ish w om en: a qualit at ive st udy on im pact and preferences for t reat m ent . Br J Gen Pract . 2 0 0 6 D ecem b er ; 5 6 ( 5 3 3 ) : 9 4 5 - 9 .
1 6 . W i l k i n s o n K . Pa k i s t a n i w o m e n ’ s p e r c e p t i o n s a n d ex per iences of incont inence. Nur s St and. 2001 Oct ober 17-2 3 ; 1 6 ( 5 ) : 3 3 - 9 .
Recebido em : 23.9.2007 Aprovado em : 16.6.2008
1 7 . Hä g g l u n d D , Ah l st r ö m G. Th e m e a n i n g o f w o m e n ’ s ex per ien ce of liv in g w it h lon g- t er m u r in ar y in con t in en ce is pow erlessness. J Clin Nurs. 2007 Oct ober; 16( 10) : 1946- 54. 1 8 . Kom or ow sk i L, Ch en B. Fem ale u r in ar y in con t in en ce in Ch in a: ex p er ien ces an d p er sp ect iv es. Healt h Car e Wom en I n t 2 0 0 6 Feb r u ar y ; 2 7 ( 2 ) : 1 6 9 - 8 1 .
19. Li FLW, Low LPL, Lee DTF. Chinese w om en’s ex per iences in coping w it h urinary incont inence. J Clin Nurs. 2007 March; 1 6 ( 3 ) : 6 1 0 - 2 .
2 0 . Bo l t an sk i L. As cl asses so ci ai s e o co r p o . 3 ed . São Paulo: Edit ora Paz e Ter ra; 2004.
2 1 . Hor r och s S, Som er set M, St oddar t H, Pet er s TJ. Wh at p r ev en t s old er p eop le f r om seek in g t r eat m en t f or u r in ar y incont inence? A qualit at ive explor at ion of bar r ier s t o t he use o f c o m m u n i t y c o n t i n e n c e s e r v i c e s . Fa r m Pr a c t 2 0 0 4 Decem b er ; 2 1 ( 6 ) : 6 8 9 - 9 6 .
22. Grealish M. General pract it ioners and w om en w it h urinary in con t in en ce. Br J Gen Pr act 1 9 9 8 Febr u ar y ; 4 8 : 9 7 5 - 8 . 23. MacDonald CD, But ler L. Silent no m ore: elderly w om en’s st or ies of liv e w it h ur inar y incont inence in long- t er m car e. J Ger on t ol Nu r s 2 0 0 7 Jan u ar y ; 3 3 ( 1 ) : 1 4 - 2 0 .