I NFLUENCE OF NONI NVASI VE VENTI LATI ON BY BI PAP
®ON EXERCI SE
TOLERANCE AND RESPI RATORY MUSCLE STRENGTH I N CHRONI C
OBSTRUCTI VE PULMONARY DI SEASE PATI ENTS ( COPD)
Dir ceu Cost a1 An d r eza Toled o2 Audr ey Bor ghi e Silv a3
Luciana Mar ia Malosá Sam paio4
Cost a D, Toledo A, Silva AB, Sam paio LMM. I nfluence of noninvasive vent ilat ion by BiPAP® on exercise t olerance an d r esp ir at or y m u scle st r en g t h in ch r on ic ob st r u ct iv e p u lm on ar y d isease p at ien t s ( COPD) . Rev Lat in o- am En fer m agem 2 0 0 6 m aio- j u n h o; 1 4 ( 3 ) : 3 7 8 - 8 2 .
This st udy aim ed t o assess t he effect of BiPAP®, by nasal m ask, on ex er cise t oler ance and r espir at or y m uscle st r engt h in pat ient s w it h a clinical and spir om et r ic diagnosis of m oder at e/ sever e COPD ( FEV1 < 60% of pr edict ed) . Ten pat ient s of 59.4± 8.9 y ear s old, w it h FEV1/ FVC < 70% of pr edict ed lev el, w er e t r eat ed w it h 30 m inut es of BiPAP® ( I PAP: 10 and 15 cm H2O; EPAP: 4 cm H2O) , t hr ee days per w eek, dur ing t w o m ont hs. Befor e
and aft er t he t r eat m ent , spir om et r y , inspir at or y ( MI P) and ex pir at or y ( MEP) m uscle st r engt h and t he dist ance w alk ed in six m inut es ( 6MWT) w er e m easur ed. We obser v ed a significant incr ease ( Wilcox on, p< 0. 05) in t he m ean v alues of MI P ( fr om - 55± 17 t o - 77± 19, r espect iv ely ) , MEP ( fr om 75± 20 t o 109± 36, r espect iv ely ) and w alk in g d ist an ce ( f r om 3 4 9 ± 6 7 t o 4 4 8 ± 7 5 ) . Based on t h ese r esu lt s, w e con clu d ed t h at BiPAP® im p r ov es r espir at or y m uscle st r engt h and ex er cise t oler ance in t hese COPD pat ient s.
DESCRI PTORS: pu lm on ar y disease, ch r on ic obst r u ct iv e; pu lm on ar y v en t ilat ion ; ex er cise t oler an ce
I N FLUEN CI A DE LA VEN TI LACI ÓN N O EVASI VA MEDI AN TE EL BI PAP
®SOBRE
LA TOLERANCI A AL EJERCI CI O FÍ SI CO Y FUERZA MUSCULAR RESPI RATORI A
EN PACI ENTES CON ENFERMEDAD PULMONAR OBSTRUTI VA CRÓNI CA ( EPOC)
El obj et iv o de est o est udio fue ev aluar el efect o del BiPAP®, por m edio de la m áscar a nasal, sobr e la t o l er an ci a al ej er ci ci o f ísi co y el d esem p eñ o m u scu l ar r esp i r at o r i o en p aci en t es co n d i ag n o si s cl ín i co y espir om ét r ico de EPOC m oder ada/ gr av e ( VEF1 < 6 0 % del pr ev isible) . Con VEF1/ CVF < 7 0 % del pr ev isible y edad pr om edia de 5 9 , 4 ± 8 , 9 añ os, diez pacien t es fu er on t r at ados con 3 0 m in u t os de BiPAP® ( I PAP= 1 0 - 1 5 e EPAP= 4 cm H2O) , en t r es sesiones sem anales, dur ant e dos m eses. Ant es y después del t r at am ient o, fue m edida la espir om et r ía, la fuer za m uscular inspir at or ia ( PI m ax ) y ex pir at or ia ( PEm ax ) y la dist ancia cubier t a en seis m inut os ( TC6 ) . Fuer on ev idenciados aum ent os significat iv os ( Wilcox on, p< 0 , 0 5 ) en el pr om edio de la PI m ax ( de - 55± 17 a - 77± 19 cm H2O) , de la PEm ax ( de 75± 20 a 109± 36 cm H2O) y de la dist ancia cubier t a ( de 349± 67
a 447± 75 m et r os) . Con base en est os r esult ados, se concluy e que el BiPAP® m ej or ó el desem peño m uscular r espir at or io y la t oler ancia al ej er cicio físico en est os pacient es con EPOC.
DESCRI PTORES: en fer m edad pu lm on ar obst r u ct iv a cr ón ica; v en t ilación pu lm on ar ; t oler an cia al ej er cicio
I NFLUÊNCI A DA VENTI LAÇÃO NÃO I NVASI VA POR MEI O DO BI PAP
®SOBRE
A TOLERÂN CI A AO EXERCÍ CI O FÍ SI CO E FORÇA MUSCULAR RESPI RATÓRI A
EM PACI ENTES COM DOENÇA PULMONAR OBSTRUTI VA CRÔNI CA ( DPOC)
O obj et iv o dest e est u do f oi av aliar o ef eit o do BiPAP®, at r av és de m áscar a n asal, n a t oler ân cia ao ex er cício físico e no desem penho m uscular r espir at ór io em pacient es com diagnóst ico clínico e espir om ét r ico de DPOC, m oder ado/ gr av e ( VEF1 < 6 0 % do pr ev ist o) . Com VEF1/ CVF < 7 0 % do pr ev ist o e idade m édia de 59,4± 8,9 anos, dez pacient es com doença pulm onar obst r ut iva cr ônica ( DPOC) for am t r at ados com 30 m inut os de BiPAP® ( I PAP= 1 0 - 1 5 e EPAP= 4 cm H2O) , em t r ês sessões sem an ais, du r an t e dois m eses. An t es e após o t r at am ent o m ediu- se a espir om et r ia, a for ça m uscular inspir at ór ia ( PI m ax ) e ex pir at ór ia ( PEm ax ) e a dist ância per cor r ida em seis m inut os ( TC6) . For am const at ados aum ent os significat ivos ( Wilcox on, p< 0,05) na m édia da PI m ax ( de - 55± 17 par a - 77± 19 cm H2O) , da PEm ax ( de 75± 20 par a 109± 36 cm H2O) e da dist ância per cor r ida ( de 349± 67 par a 448± 75 m et r os) . Com base nesses r esult ados conclui- se que o BiPAP® m elhor ou o desem penho m uscular r espir at ór io e a t oler ância ao ex er cício físico nesses pacient es com DPOC.
DESCRI TORES: doen ça pu lm on ar obst r u t iv a cr ôn ica; v en t ilação pu lm on ar ; t oler ân cia ao ex er cício
D ispon ív e l e m lín gu a por t u gu e sa n a SciELO Br a sil w w w .scie lo.br / r la e
1
I NTRODUCTI ON
N
oninvasive vent ilat ion ( NI V) has been used successfully for t r eat ing r espir at or y insufficiency duet o d if f er en t cau ses, in clu d in g sleep ap n ea, ch r on ic
obst r uct ive pulm onar y disease ( COPD) and pulm onar y
edem a( 1 ). Th e applicat ion of bi- lev el posit iv e air w ay
pr essur e ( BiPAP®) , w hich associat es t he pr essur e of
v ent ilat or y suppor t w it h posit iv e final pr essur e, aim s
t o increase alveolar recruit m ent during inspirat ion and
pr ev en t alv eolar collapse du r in g ex pir at ion( 2 ).
Som e st u d ies( 3 ) h av e at t em p t ed t o an aly ze
t h e in f lu en ce of BiPAP® on t h e r esp ir at or y m u scles
an d ex er cise t oler an ce in pat ien t s w it h COPD. Th eir
r esu lt s sh ow ed t h at p at ien t s w h o ar e t r eat ed w it h
BiPAP® t w o h ou r s p er d ay, d u r in g f iv e con secu t iv e
d a y s , p r e s e n t g r e a t e r r e s p i r a t o r y m u s c l e r e s t ,
i m p r o v ed t o l er an ce an d r ed u ced d y sp n ea. Si m i l ar
r esu lt s h av e b een f ou n d in ot h er st u d ies( 4 ), w h ich
at t r ibut ed t he incr ease in r espir at or y m uscle st r engt h
t o t he m uscle r est pr om ot ed by NI V. How ev er, ot her
r e se a r ch( 5 ) h a s n o t d e m o n st r a t e d a n y si g n i f i ca n t
gr ow t h in r espir at or y m uscle st r engt h.
A s CO PD p a t i e n t s p r e s e n t v e n t i l a t o r y
l i m i t at i o n s t h at l ead t o p r o g r essi v e i n t o l er an ce t o
e f f o r t s( 6 ), d u e t o d y s p n e a , w e a k n e s s a n d
d e c o n d i t i o n i n g o f r e s p i r a t o r y a n d p e r i p h e r a l
m uscles( 7), m aking t hem vulner able t o hospit alizat ion,
t his st udy aim s t o assess t he effect s of bi- level NI V in
COPD pat ient s on ex er cise t oler ance and r espir at or y
m u scle st r en gt h .
MATERI ALS AND METHODS
I n div idu a ls: We st udied t en individuals, five
m en and fiv e w om en, w it h a m ean age of 65. 3 ± 9. 6
y ear s, ex - sm ok er s, w hose phy sicians had pr escr ibed
p u l m o n a r y r e h a b i l i t a t i o n a t t h e Sp e ci a l Un i t f o r
Re s p i r a t o r y Ph y s i o t h e r a p y , w i t h a c l i n i c a l a n d
spir om et r ic diagnosis of m oder at e/ sever e COPD ( FEV1
< 6 0 % o f p r e d i c t e d ) , w i t h FEV1/ FV C < 7 0 % o f
pr edict ed, an d clin ically st able. Th ese pat ien t s, w h o
w e r e r e c e i v i n g b r o n c h o d i l a t o r s ( b e r o t e c a n d / o r
a t r o v e n t ) f o r c a s e s o f i n t e n s e d y s p n e a , w e r e
subm it t ed t o a gener al and specific ev aluat ion of t he
r esp i r a t o r y sy st em a n d si g n ed a co n sen t t er m t o
par t icipat e in t he pr oposed pr ogr am , as r ecom m ended
by Br azilian legislat ion for r esear ch inv olv ing hum an
b e i n g s . Th i s s t u d y w a s a p p r o v e d b y t h e e t h i c s
com m it t ee f or r esear ch in v olv in g h u m an b ein g s at
t he inst it ut ion w her e t he st udy w as car r ied out .
I n c l u s i o n c r i t e r i a w e r e t h e a b s e n c e o f
a s s o c i a t e d c a r d i o v a s c u l a r d i s e a s e s , o r t h o p e d i c
d i seases, h y p er r esp o n si v en ess an d n eu r o m u scu l ar
d i s o r d e r s t h a t w o u l d i m p e d e t h e r e a l i z a t i o n o f
ex per im ent al pr ocedur es pr oposed in t his st udy.
Ex p e r im e n t a l p r oce d u r e : Befor e and aft er
t r eat m en t , pat ien t s w er e su bm it t ed t o t h e follow in g
assessm en t s:
- Spir om et r y : car r ied out by m eans of a Vit alogr aph
s p i r o m e t e r, m o d e l 2 0 2 1 , a c c o r d i n g t o Am e r i c a n
Th o r a ci c So ci et y( 8 ) st a n d a r d s, t o ch a r a ct er i ze t h e
degr ee of obst r u ct iv e pu lm on ar y disor der.
- Respir at or y Mu scle St r en gt h : obt ain ed by u sin g a
Ge r - A r m a n o - v a c u u m m e t e r s c a l e d i n c m H2O.
Max im u m in spir at or y pr essu r e ( MI P) an d m ax im u m
ex pir at or y pr essur e ( MEP) w er e m easur ed accor ding
t o earlier st udies( 9), w it h t he individual in t he ort host at ic
posit ion and w it h a nose clip. MI P w as m easured close
t o t he r esidual volum e aft er m axim um expir at ion. MEP
w as m easur ed close t o t ot al pulm onar y capacit y ( TPC)
aft er m ax im um inspir at ion. I ndiv iduals w er e or ient ed
t o sust ain pr essur e for m or e t han a second and each
m aneuv er w as r ealized at least t hr ee t im es. For t he
sak e of an aly sis, t h e h ig h est r esu lt w as t ak en in t o
accou n t ;
- S i x - Mi n u t e Wa l k i n g Te s t ( 6 MW T) : t o e v a l u a t e
exer cise t oler ance, pat ient s w er e subm it t ed t o a 6MWT
in a f lat lev el cor r idor of 3 0 m et er s len gt h an d 1 . 5
m et er s w idt h, dem ar cat ed ev er y 2 m et er s.
Pat ien t s w er e ad v ised t o t ak e a lig h t m eal
about t w o hour s befor e t he t est and not t o per for m
an y in t en se p h y sical ex er cise, n or t ak e m ed icat ion
dur ing t he 24 hour s befor e t he ex am inat ion, besides
u sin g com for t able clot h in g an d sh oes for t ak in g t h e
t est .
Vit al signs w er e m easur ed befor e and at t he
end of t he t est :
- Sy st olic ( SBP) and diast olic blood pr essur e ( DBP) ,
u s i n g a D i a s i s t s t e t h o s c o p e a n d B D
sph y gm om an om et er, t h r ou gh in dir ect au scu lt at ion ;
- Ca r d i a c f r e q u e n cy ( CF) a n d p e r i p h e r a l o x y g e n
sat ur at ion ( SpO2) , using a Nonin 8500A por t able pulse
o x i m et er ;
- subj ect ive feeling of dyspnea, using Bor g’s per ceived
ex er t ion scale, r anging fr om “ zer o” for no lack of air
t o “ t en” for a m axim um feeling of lack of air.
The six - m inut e w alk ing t est inv olv ed a w alk
possible dist ance, during a six- m ont h per iod, r eceiving
a st a n d a r d i ze d e n co u r a g e m e n t e v e r y m i n u t e( 1 0 ).
Pat ien t s w er e accom pan ied by t h e ev alu at or du r in g
t he six m inut es and cont inuously m onit or ing t hr ough
t he pulse oxim et er. For t he sake of analysis, CF, SpO2
a n d su b j e ct i v e f e e l i n g o f d y sp n e a w e r e r e co r d e d
befor e and aft er t he t est . Wit h a v iew t o m inim izing
lear n in g ef f ect s, each p at ien t car r ied ou t t w o t est s
befor e t h e t r eat m en t , an d t h e lon gest dist an ce w as
calcu lat ed .
Non in vasiv e Ven t ilat ion ( NI V)
Pat ient s w er e subm it t ed t o NI V by m eans of
BiPAP®, u sin g a n asal m ask , f or 3 0 m in u t es, t h r ee
t im es per w eek, on alt er nat e days, dur ing six w eeks.
B i PA P® l e v e l s w e r e a d j u s t e d a c c o r d i n g t o e a c h
p at ien t ’s t oler an ce. Pat ien t s r em ain ed com f or t ab ly
seat ed t hr oughout t he NI V applicat ion ( w it h I PAP set
bet w een 1 0 an d 1 5 cm H2O an d EPAP at 4 cm H2O) ,
and w er e asked t o adopt diaphr agm at ic br eat hing ( 11)
dur ing t he applicat ion.
STATI STI CAL ANALYSI S
For t h e st at ist ical an aly sis of p h y siolog ical
v a r i a b l e s a n d d i s t a n c e w a l k e d b e f o r e a n d a f t e r
t r e a t m e n t w i t h N I V, w e u s e d W i l c o x o n ’ s n o n
-par am et r ical t est , as dat a did n ot pr esen t a n or m al
dist r ibut ion. A p< 0.05 significance level w as adopt ed.
RESULTS
Table 1 pr esen t s t h e par t icipan t s’ in div idu al
ant hropom et ric and dem ographic charact erist ics relat ed
t o age, gender, weight , height , body m ass index ( BMI ) ,
w it h m ean v alues and st andar d dev iat ions.
Table 1 - I ndiv idual ant hr opom et r ic and dem ographic
c h a r a c t e r i s t i c s w i t h m e a n v a l u e s a n d s t a n d a r d
d ev iat ion s
s t c e j b u
S Age(years) Gender Weight(kg) Height(m) BMI(kg/m2)
1 72 M 78.5 1.63 29.5 2 68 M 68.5 1.66 24.9
3 66 M 89 1.76 28.7
4 78 M 66.5 1.68 23.6
5 64 M 72 1.61 27.8
6 64 F 70 1.65 25.7
7 70 F 51 1.5 22.7
8 43 F 109 1.53 46.6
9 63 F 72 1.52 31.2
0
1 43 F 63 1.55 26.2
D S / n a e
M 65.3±9.6 74±15.7 1.61±0.1 28.7±6.8 BMI : body m ass index; SD: st andar d deviat ion.
Ta b l e 2 s h o w s t h e s p i r o m e t r i c r e s u l t s
obt ain ed w h en ev alu at in g an d r eev alu at in g pat ien t s
w h o r e c e i v e d B i PA P® a p p l i c a t i o n . N o s i g n i f i c a n t
changes w er e found bet w een t he spir om et r ic indices
obt ained befor e and aft er NI V t r eat m ent .
Tab l e 2 - Sp i r o m et r i c m easu r em en t s i n l i t er s an d
p e r c e n t a g e s o f p r e d i c t e d b e f o r e a n d a f t e r
BiPAP®t r eat m en t
FVC: for ced vit al capacit y; FEV
1: for ced expir at or y volum e in one second; MVV: m axim um volunt ar y vent ilat ion; FEF
25- 75%: for ced expir at or y flow 25-75; NS: not significant .
Tab le 3 p r esen t s t h e m ean r esu lt s f or t h e
follow ing phy siological answ er s: CF, SpO2, subj ect iv e
f e e l i n g o f d y sp n e a , MI P a n d MEP, a s w e l l a s t h e
d ist an ce w alk ed d u r in g t h e 6 MWT. We d id n ot f in d
st at ist ically sign if ican t dif f er en ces bet w een t h e pr
e-a n d p o s t - t r e e-a t m e n t s i t u e-a t i o n s f o r CF, Sp O2 a n d
su b j ect iv e f eelin g of d y sp n ea. How ev er, d if f er en ces
f or dist an ce w alk ed, MI P an d MEP w er e st at ist ically
sign if ican t .
Ta b l e 3 - Co m p a r i s o n b e t w e e n m e a n v a l u e s o n
d y sp n e a sca l e f o r 6 MW T, MI P, MEP a n d d i st a n ce
w alk ed, befor e and aft er t r eat m ent w it h BiPAP®
SpO2: per ipher aloxygen sat ur at ion; CF: car diac fr equency; MI P: m axim um inspir at or y pr essur e; MEP: m axim um expir at or y pr essur e.
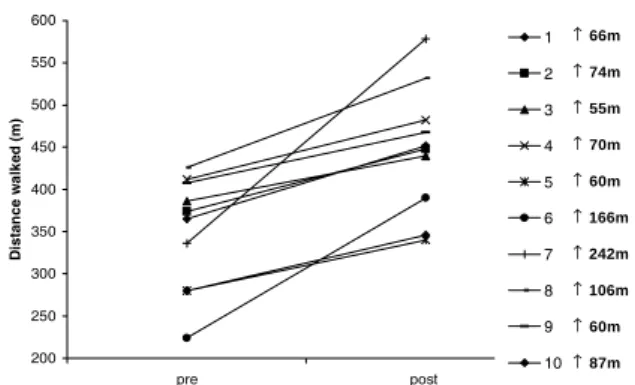
Fi g u r e 1 i l l u st r a t e s i n d i v i d u a l r e su l t s f o r
dist ance w alk ed in m et er s, obt ained befor e and aft er
t r eat m ent w it h NI V.
P A P i B -e r
P ® Post-BiPAP®
) % ( C V
F 60.98±11.98 57.35±11.76(NS)
) l ( C V
F 1.78±0.56 1.65±0.55(NS)
V E
F 1(%) 43.25±8.92 45.09±8.18 ) S N ( V E
F 1(l) 1.06±0.21 1.05±0.28(NS)
V E
F 1/FVC(%) 58.4±17 61.8±11(NS)
) % ( V V
M 42.80±8.91 44.02±6.71(NS)
) l ( V V
M 37.83±8.51 39.62±10.63(NS)
F E
F 25-75%(%) 17.52±10.03 19.82±9.64 ) S N ( 2 F E
F 5-75%(l) 0.51±0.28 0.58±0.29(NS)
® P A P i B -e r
P Post-BiPAP® P-value
O p
S 2(%) 85.4±3.7 92.8±1.6 0.10
) 0 1 -0 ( a e n p s y
D 2.9±1.5 0.7±0.8 0.10 ) m p b ( F
C 115.8±10.1 117.7±11.1 0.10 H m c ( P I
M 2O) -54.50±17.07 -76.66±18.87 0.007* H m c ( P E
M 2O) 74.70±70 109.44±35.74 0.007* ) m ( d e k l a w e c n a t s i
RTG RQUV
&
KU
VC
P
E
G
Y
C
NM
G
F
O
↑ 66m
↑ 74m
↑ 55m
↑ 70m
↑ 60m
↑ 166m
↑ 242m
↑ 106m
↑ 60m
↑ 87m
Figur e 1 - I ndividual values for dist ance w alked dur ing
6 MWT, obt ained dur ing evaluat ion and r eevaluat ion
DI SCUSSI ON
No n i n v a si v e v e n t i l a t i o n h a s b e e n u se d i n
differ ent st udies t o pr ovide gr eat er r espir at or y m uscle
r est( 4). NI V is able t o “ alleviat e” t he inspirat ory m uscles’
w o r k l o a d , p r o m o t i n g a t e m p o r a r y r e st a n d t h u s
allow in g for bet t er con dit ion s t o dev elop r espir at or y
m u scle st r en gt h .
Our r esult s show ed t hat NI V t hr ough a nasal
m ask by m eans of BiPAP®, dur ing a six- w eek per iod,
si g n i f i ca n t l y i n cr e a se d m u scl e st r e n g t h i n COPD
p a t i e n t s , i n l i n e w i t h l i t e r a t u r e( 1 2 ), w h i c h h a s
d em o n st r at ed i n cr eases i n MI P an d MEP af t er t h e
ch r o n i c a p p l i ca t i o n o f Bi PAP® i n COPD p a t i e n t s.
I ncr eases in r espir at or y m uscle st r engt h t hr ough t he
use of pr essur e suppor t hav e also been obser v ed( 13)
w hen applying NI V t o COPD pat ient s dur ing t he night .
Mor eov er, ou r r esu lt s in d icat ed a p r ob ab le
im p r ov em en t in ex er cise t oler an ce af t er t r eat m en t
w it h NI V, as w e f ou n d a sig n if ican t in cr ease in t h e
dist ance w alked dur ing t he 6MWT w hich, alt hough ver y
sim ple, has been fr equent ly used in field st udies( 14).
D e s p i t e t h e p h y s i c a l l i m i t a t i o n s CO PD p a t i e n t s
n or m ally pr esen t , t h e dist an ce w alk ed by all of ou r
pat ient s ex ceeded 54 m et er s, as show n in Figur e 1.
Th is h as b een m en t ion ed( 1 5 ) as a g ood in d icat or of
t hese pat ient s’ clinical im pr ov em ent .
Sim ilar result s w ere found in a research( 3) t hat
assessed t he effect s of BiPAP® w hen applied for t w o
h ou r s d u r in g t h e d ay, f or on e w eek . Th is r esear ch
an aly zed sev er e bu t st able COPD pat ien t s, eigh t of
w hom w er e t r eat ed w it h a placebo m et hod ( w it hout
NI V) an d sev en w it h BiPAP® t w o h ou r s per day f or
fiv e consecut iv e day s. These aut hor s( 3) dem onst r at ed
t hat BiPAP® im pr oved t oler ance and r educed pat ient s’
dy spnea, w hile t he placebo gr oup did not obt ain any
significant im pr ov em ent . How ev er, t he st udy neit her
ev idenced a clinical im pr ov em ent nor an incr ease in
t hese pat ient s’ r espir at or y m uscle st r engt h( 15).
No n i n v a si v e v e n t i l a t i o n , a s a r e so u r ce t o
i m p r o v e r esp i r at o r y m u scl e st r en g t h an d p h y si cal
per f or m an ce, m ay r equ ir e a lon ger t r eat m en t t im e,
i n v o l v i n g o r i e n t a t i o n s a b o u t d i a p h r a g m a t i c
b r e a t h i n g( 1 1 ). Th i s i s ch a r a ct e r i ze d a s Fu n ct i o n a l
Respir at or y Reeducat ion. The use of NI V for few days
r em ains r est r ict ed t o suppor t ing a r est per iod for t he
r esp ir at or y m u scles, an d d oes n ot ob lig at or y en t ail
c h a n g e s i n CO PD p a t i e n t s ’ r e s p i r a t o r y m u s c l e
st r engt h, nor in t heir phy sical condit ion.
Wit h r espect t o CF, SpO2 and subj ect ive feeling
of d y sp n ea, w e d id n ot f in d st at ist ically sig n if ican t
dif f er en ces du r in g t h e 6 MWT, w h en m easu r ed af t er
N I V t r e a t m e n t . Th e se r e su l t s d e m o n st r a t e t h a t ,
alt hough pat ient s w alk ed a longer dist ance aft er t he
t r e a t m e n t , t h e se v a r i a b l e s r e m a i n e d st a b l e . Th i s
in d icat es an im p r ov em en t in t h e p at ien t s’ p h y sical
condit ion or t olerance, alt hough w e could not com par e
v a l u e s f o r t h e s a m e e f f o r t i n t e n s i t y, w h i c h c a n
n or m ally b e con t r olled d u r in g t est s car r ied ou t on
er gom et r ic equipm ent , such as a t r eadm ill or bicycle.
Mor eover, fr om a clinical per spect ive, SpO2 pr esent ed
a b et t er sat u r at ion r an g e af t er NI V an d p er ceiv ed
dyspnea, alt hough not significant , show ed a dow nw ar d
t en d en cy.
Alt hough t hese r esult s ar e encour aging, som e
m et hodological lim it at ions need t o be highlight ed, such
as t he lack of a cont r ol gr oup t o pr ov ide m or e solid
support t o t he efficacy of t his alt er nat ive and auxiliar y
t herapeut ic t echnique in t he physical t raining of COPD
pat ien t s. Fu r t h er m or e, ou r f in din gs r ev eal t h e n eed
f or n ew st u d ies, in v olv in g a m et h od olog y t h at can
ex p lor e t h ese asp ect s w it h ou t ig n or in g each COPD
pat ient ’s ow n physical lim it at ions; t aking int o account
different obst ruct ion levels, using a larger sam ple and
m or e com p lex ev alu at ion s, su ch as er g osp ir om et r y
and blood lact at e lev els.
Fin ally, w e can con clu de t h at , in ou t pat ien t
clinics, noninvasive vent ilat ion is an auxiliary t echnique
f o r t h e p h y s i c a l c o n d i t i o n i n g o f COPD p a t i e n t s ,
esp eci al l y w i t h a v i ew t o cau si n g a r est f o r t h ei r
r esp ir at or y m u scles, allow in g f or g r eat er t oler an ce
t o bu r den s in r espir at or y m u scle t r ain in g. Th is is a
r el ev an t asp ect , as t h ese p at i en t s p r esen t l i m i t ed
a b i l i t i e s t o m a k e p h y si ca l e f f o r t s, w e a k n e ss a n d
REFERENCES
1. Cont i G, Mar ino P, Cogliat i A, Dell’Ut r i D, Lappa A, Rosa G, et al. Non iv v asiv e v en t ilat ion t o acu t e r espir at or y failu r e in p a t i e n t s w i t h h e m a t o l o g i c m a l i g n a n ci e s: a p i l o t st u d y. I n t en siv e Car e Med 1 9 9 8 ; 2 4 : 1 2 8 3 - 8 .
2. Ebeo CT, Byr d RP Jr, Benot t i PN, Elm aghaby Z, Lui J. The ef f ect of bi- lev el posit iv e air w ay pr essu r e on post oper at iv e pulm onar y funct ion follow ing gast r ic sur ger y for obesit y. Resp Med 2 0 0 2 ; 9 6 ( 9 ) : 6 7 2 - 6 .
3. Renst on JP, Dim ar co AF, Supinsk i GS. Respirat or y m uscle r est u si n g n asal Bi PAP v en t i l at i on i n p at i en t s w i t h st ab l e sev er e COPD . Ch est 1 9 6 4 ; 1 0 5 : 1 0 5 3 - 6 0 .
4. Wij k st ra PJ, Lacasse Y, Guyat t GH, Casanov a C, Gay PC, Meecham JJ, et al. A m et a- analy sis of noct ur nal noninv asiv e p osit iv e p r essu r e v en t ilat ion in p at ien t s w it h st ab le COPD. Ch e st 2 0 0 3 ; 1 2 4 ( 1 ) : 3 3 7 - 4 3 .
5 . B a r b é F, To g o r e s B, Ru b i M , M a i m ó A , A g u s t i A G. Noninv asiv e v ent ilat or y suppor t does facilit at e r ecov er y fr om acu t e r esp ir at or y f ailu r e in ch r on ic ob st r u ct iv e p u lm on ar y d isease. Eu r Resp ir J 1 9 9 6 ; 9 ( 6 ) : 1 2 4 0 - 5 .
6 . Ca s a b u r i R. S k e l e t a l m u s c l e d i s f u n c t i o n i n c h r o n i c obst r uct ive pulm onar y disease. Med & Sci in Spor t s & Exer cise 2 0 0 1 ; 3 3 ( 7 ) : 6 6 2 5 - 5 .
7. Sar m ient o R, Or ozco- Levi M, Guell R, Bar r eir o E, Her nandez N, Mot a S, et . al. I nspir at or y m uscle t r aining in pat ient s w it h chr onic obst r uct iv e pulm onar y disease: st r uct ur al adapt at ion and phy siologic out com es. Am J Respir Cr it Car e Med 2002; 1 6 6 : 1 4 9 1 - 7 .
8. Am er ican Thor acic Societ y. St andar dizat ion of spir om et r y. Am Rev Resp ir Dis 1 9 8 7 ; 1 3 6 : 1 2 8 5 - 9 9 .
9. Cost a D, Sam paio LMM, Pir es Di Lor enzo VA, Jam am i M, Dam aso AR. Ev alu ación da la fu r za m u scu lar r espir at or io y am plit ud t or ácica y abdom inal después de la RFR en individuos o b se so s. Re v La t i n o - a m En f e r m a g e m 2 0 0 3 m a r ço - a b r i l ; 1 1 ( 2 ) : 1 5 6 - 6 0 .
10. Am er ican Thor acic Societ y St at em ent . Guidelines for t he si x - m i n u t e w a l k t e st . Am J Re sp i r Cr i t Ca r e Me d 2 0 0 2 ; 1 6 6 : 1 1 1 - 7 .
11. Cost a D. Fisiot er apia Respir at ór ia Básica. São Paulo ( SP) : At h en eu ; 1 9 9 9 .
12. Pir es Di Lor enzo VA, Silva AB, Sam paio LMM, Jam am i M, Oish i J, Cost a D. Ef eit os d o t r ein am en t o f ísico e m u scu lar r esp ir at ór io em p acien t es com DPOC g r av e su b m et id os a BiPAP. Rev Br as Fisiot er 2 0 0 3 ; 7 : 6 9 - 7 6 .
13. Diaz PO, Ram os JV, Gallar do RJ, Tor r ealba FB, Lisboa BC. Non in v asiv e m ech an ical v en t ilat ion in p at ien t s w it h sev er e st ab le COPD. Rev Med Ch il 1 9 9 9 ; 1 2 7 : 6 4 7 - 5 4 .
14. Silva AB, Pir es Di Lor enzo VA, Sam paio LMM, Jam am i M, Cost a D, Bald isser a V. A in f lu ên cia d o Tr ein am en t o Físico ( TF) sobr e as r espost as car dior r espir at ór ias e a lact acidem ia em p acien t es com DPOC. Rev Br as At iv Fís Saú d e 2 0 0 3 ; 8 ( 1 ) : 3 0 - 7 .
15. Solway S, Br ooks D, Lacasse Y, Thom as SA. A qualit at ive sy st e m a t i c o v e r v i e w o f t h e m e a su r e m e n t p r o p e r t i e s o f f u n ct ion al w alk t est s u sed in t h e car dior espir at or y dom ain . Ch e st 2 0 0 1 ; 1 1 9 : 2 5 6 - 7 0 .