SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Update
Article
Is
it
safe
to
use
local
anesthesia
with
adrenaline
in
hand
surgery?
WALANT
technique
夽
Pedro
José
Pires
Neto
∗,
Leonardo
de
Andrade
Moreira,
Priscilla
Pires
de
Las
Casas
HospitalFelícioRocho,DepartamentodeOrtopediaeTraumatologia,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30August2016 Accepted5September2016 Availableonline19July2017
Keywords:
Localanesthesia/methods Localanesthesia/administration anddosage
Hand Surgery Adrenaline
a
b
s
t
r
a
c
t
Inthepastitwastaughtthatlocalanestheticshouldnotbeusedwithadrenalinefor proce-duresintheextremities.Thisdogmaistransmittedfromgenerationtogeneration.Itstruth hasnotbeenquestioned,northesourceofthedoubt.Inmanysituationsthebenefitofuse wasnotunderstood,becauseitwasoftenthoughtthatitwasnotnecessarytoprolongthe anestheticeffect,sincetheproceduresweremostlyofshortduration.Afterthedisclosureof studiesofCanadiansurgeons,cametounderstandthatthebenefitswentbeyondthetime ofanesthesia.TheWALANTtechniqueallowsasurgicalfieldwithoutbleeding,possibilityof informationexchangewiththepatientduringtheprocedure,reductionofwastematerial, reductionofcosts,andimprovementofsafety.Thus,afterpassingthroughtheinitialphase ofthedoubtsintheuseofthistechnique,theauthorsverifieditsbenefitsandthepatients’ satisfactioninbeingabletoimmediatelyreturnhomeaftertheprocedures.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
É
seguro
o
uso
de
anestésico
local
com
adrenalina
na
cirurgia
da
mão?
Técnica
WALANT
Palavras-chave:
Anestesialocal/métodos Anestesialocal/administrac¸ãoe dosagem
Mão Cirurgia Adrenalina
r
e
s
u
m
o
Aprendemos quenão deveríamos usar um anestésico local comadrenalina para
pro-cedimentos nasextremidades. Esse dogmaé transmitido de gerac¸ãoem gerac¸ão. Não
questionávamos a sua veracidade ou a origem da dúvida. Em muitas situac¸ões não
entendíamosobenefíciodouso,poismuitasvezespensávamosnãosernecessárioprolongar oefeitoanestésico,jáqueosprocedimentoseram,nasuamaioria,decurtadurac¸ão.Após adivulgac¸ãodeestudosdoscirurgiõescanadenses,passamosaentenderqueosbenefícios seestendiamalémdotempodeanestesia.AtécnicaWalantpermiteumcampocirúrgico
夽
StudyconductedattheHospitalFelícioRocho,DepartamentodeOrtopediaeTraumatologia,BeloHorizonte,MG,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](P.J.PiresNeto).
http://dx.doi.org/10.1016/j.rboe.2017.05.006
semsangramento,possibilidadedetrocadeinformac¸õescomopacienteduranteo proced-imento,reduc¸ãodematerialdedescarte,reduc¸ãodecustosemelhoriadaseguranc¸a.Dessa forma,apóspassarpelafaseinicialdasdúvidasquantoaousodessatécnica,verificamos osseusbenefícioseasatisfac¸ãodospacientesempoderemretornardeimediatoparacasa apósosprocedimentos.
©2017SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Thereisagrowinginterestinperforminghandandwrist surgi-calprocedureswithlocalanesthesiawithoutsedation.Studies havedemonstratedthatsurgicalprocedurescanbeperformed safelyandonanoutpatientbasis.Experiencehasshownthat theuseoflocalanesthesiawithepinephrine,inadditionto providingsafety,allowsintraoperativecontrolofmovement andassessmentoffunctionduringtendonrepairortransfer procedures.
Thisarticleaimedtodiscusspossibilitiesandconcepts,and toassessthesafetyandthetechniquesoflocalanestheticuse withepinephrineinhandsurgery.Patientsoperatedwiththis typeofanesthesiadonotrequiresedation,whichallowsan exchangeofinformationduringtheprocedure,active move-mentoftheoperatedlimb,andafasterhospitaldischargeafter surgery.1
What
is
the
‘wide-awake’
or
WALANT
technique?
The term wide-awake indicates that the hand surgery is
performed with the patient fully awake. WALANT is the
acronym for ‘wide-awake local anesthesia no tourniquet’.
WALANTisthecurrent preferred termtoindicate thatthe
procedure is performed withthe patient in a non-sedated
state, under local anesthesia and without tourniquet. In
this technique, only two drugs are used, lidocaine and
epinephrine.2
Adrenaline
or
epinephrine
Epinephrine,alsoknownasadrenaline,isasympathomimetic
hormoneandneurotransmitter3derivedfromthe
modifica-tion ofan aromatic amino acid (tyrosine) secreted by the adrenalglands,socalledbecausetheyarepositionedabove thekidneys.Thenameadrenalinecomesfromad-(prefixthat indicatesproximity),renalis(pertainingtothe kidneys),and thesuffix-ine,whichappliestocertainchemicalsubstances (amines).
It affects both the beta-1adrenergic receptors (cardiac)
and beta-2 adrenergic receptor (pulmonary). It has
alpha-adrenergicpropertiesthatresultinvasoconstriction.InBrazil, thenameadrenalineispreferred.
Hemostasis
instead
of
a
tourniquet
for
hand
surgery
Manyhandsurgeonshaveswitchedfromtraditionalsurgery
witha tourniquetandsedation tothe WALANTtechnique.
Lidocaine and epinephrine are the only drugs injected for
anesthesiaandhemostasisatthedissectionsites,andatthe Kirschnerwiresinsertionsitesinosteosynthesis.
Benefits
of
WALANT
(1) Nouseofsedationortourniquet,whichincreasespatient comfortandconvenience.Patientscanhavetheirhands operatedsimilarlytoasmallprocedureatthedentist.
(2) Theelimination ofthe anesthesiology/sedation
compo-nents decreasesthe surgicaltimeforthe proceduresin thetreatmentofcarpaltunnelsyndrome,DeQuervain’s tenosynovitis,andtriggerfinger.
(3) Duringtheprocedure,thepossibilityofobservingand cor-rectingsuturedtendonsandofverifyingthestabilityofan osteosynthesiswiththefullrangeofactivemovements,
and with the patient in acomfortable and cooperative
position, allows betterresults intendon repair, tendon transfer,andfixationofphalangealfractures.
(4) WALANTisnotindicatedforallpatients,butmostofthose whocanundergodentaltreatmentswithoutsedationcan alsohavetheirhandsoperatedonusingthistechnique.1
Is
it
safe
to
use
epinephrine
in
the
finger?
Thesafetyofepinephrineuseinthefingerimpliesnoneedto usetourniquet.
Therise and fallofthemyth ofthe dangerofinjecting epinephrineinthefingergoesbacktobeforethe1950s,when surgeons believed that epinephrine caused finger necrosis. Thisdogmahasspreadandrootedintheteachingsin medi-calschools,whereitwascommontoteachthatepinephrine should not be injected into the extremities (fingers, nose, penis,andfeet).Evidence-basedmedicinehasalreadycleared thismisconception.Thefollowingisthestoryofhowthis hap-pened.
The
myth
Thesourceofthe epinephrine myth,whicharosebetween
Itwas“thenew‘-caine’,”inventedin1903toreplacecocaine. Thislocalanesthetic was used until1948, when lidocaine, whichhasa saferprofile,wasintroduced. Procaine started withapHof3.6;whenstoredforalongtime,itwouldacidify, anditspHwouldreachaslowas1.Itwasthisaciditythat causedfingernecrosis,nottheuseofepinephrine.5TheFood
andDrugAdministration(FDA)oftheUnitedStatesreported intheJournaloftheAmericanMedicalAssociationthattheyhad foundprocainelotsforinjectioninhumanswithapHof1.6
Is
it
possible
to
reverse
the
effect
of
epinephrine?
Evidence shows that phentolamine, an alpha blocker that
becameavailablein1957,reliablyreversesthevasoconstrictor actionofepinephrine.7However,itsuseisseldomnecessary
inclinicalpractice.8
Theliteraturefeaturesstudiesinwhichepinephrinehas beenusedwithoutinducingnecrosis.8,9
Furthermore,nocasesofnecrosiswerereportedevenwith highdosesofepinephrine(1:1000)afteraccidentalinjections ofepinephrineintoafinger.10,11
Therefore,epinephrineisunlikelytocausedamagetothe fingers at a concentration of 1:100,000. More cases of fin-gerinjurieshavebeenreportedfromimproperlyuseddigital tourniquetsthanfromlidocainewithepinephrine.12,13
Safe
dosage
of
lidocaine
with
epinephrine
• The most widely reported dose of lidocaine with
epinephrine is 7mg/kg. This dosage had already been
suggestedbefore1950,atthebeginningoftheuseof lido-caine.Sincethen,Burketal.14reportedsafebloodlevelsof
lidocainewhen35mg/kgareinjectedforliposuction. • SincemostpatientssubmittedtoWALANTareoperatedon
anoutpatientbasis,theauthorssuggesttheuseofdosages withintheverysafelimitof7mg/kgformosthand surger-ies.Ina70-kgadult,thismeans:
• Safedosage:lidocaine/epinephrine. <50mL:1/100,000
50–100mL:0.5/200,000 100–200mL:0.25/400,000
The
concentrations
of
premixed
epinephrine
with
lidocaine
vary
by
country.
• InCanadaandintheUnitedStates,theanestheticis pre-mixedas1%lidocainewith1:100,000epinephrine.
• Todate,1%lidocainewith1:200,000epinephrineisavailable
asapre-mixedsolutioninmanyEuropeancountriesand
thisworksverywellforsurgeons.InIsrael,lidocaine pre-mixedwithepinephrineisnotavailable,andthemixture hastobemadebysurgeonsthemselves.InHongKongand Brazil,2%lidocainewith1:200,000epinephrineisavailable aspremix.InEgypt,premixed2%lidocainewith1:100,000 epinephrineisavailable,whileinIndonesia,thepremix2% lidocainewith1:80,000epinephrineisavailable.
• Thereisstillnoevidenceintheliteraturethatprovesan idealanduniqueepinephrineconcentration.
How
to
inject
local
anesthetic
with
minimal
pain
Itispossibleandeasy tolearn andteachmedicalstudents andresidentshowtoinjectlocalanestheticforhandsurgeries. Theauthorsuseathinneedle(13×4.5)andminimizethepain ofthefirstpinch.Patientswillgreatlyappreciatethe physi-cianhavinginvestedthetimeneededtolearnthetensimple rules listedbelow.Themostimportantare rules7through 10.Patientswillbesurprisedandcaptivatedwiththesmall amountofpaintheywillfeelduringtheinjections.15–27
RULE1.Buffer:1%lidocaine,1:100,000epinephrine,and10:1 8.4%sodiumbicarbonate.
RULE2.Donotusearefrigeratedlocalanesthetic. RULE3.Localanesthesiawithsmallneedle(13×4.5). RULE4.Createasensorydistractionintheinjectionsite. RULE5.Stabilizethesyringewithbothhandsandkeepthe thumbreadytopresstheplungertoavoidthepainofa mov-ingneedle.
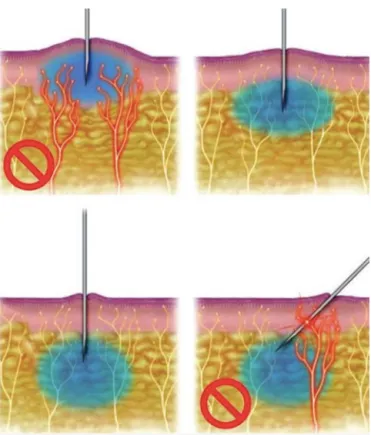
RULE 6. Inject 0.5mL with a needle perpendicularly just belowthedermisandthenpauseuntilthepatientreports thatthepainofthepinchhasdisappeared(Fig.1).
RULE7.Neverlettheneedleprogressinfrontofthelocal anesthetic(blowslowbeforeyougo)(Figs.2and3).
Fig.2–“Blowslowbeforeyougo”injectiontechnique.The anestheticisinjectedslowlybeforetheneedleis
progressed.Inthisway,thenerveendingswillbeblocked bytheanestheticandtheprocesswillbepainless(Courtesy DonaldLalond).
RULE8.Reinsert theneedle atleast1cminto thealready injectedarea.Thiscanbedefinedbypalpationorassessing thecoloroftheskin;
RULE9.Askeachpatienttogiveascore(0–10)regardingthe intensityofpainduringtheinjectionoftheanesthetic. RULE10.Morelocalanestheticisbetterthaninsufficientlocal anesthetic.
Palmar
and
dorsal
scars
and
folds
are
natural
barriers
to
the
diffusion
of
the
local
anesthetic
solution
• Thelocalanestheticdoesnotdiffusewellintothescars.It willoftenbenecessarytoinjectlocalanesthetic onboth sidesofalinearscar.Formarkedlyscarredareas,the sur-geonshouldtrytoinitiatetheinjectionfromtheproximalto distalandintohealthysubcutaneoustissue,andthenfinish underthescarifnecessary.
Fig.3–Blockadewithlidocaineandadrenaline30min beforethesurgicalprocedureforcarpaltunnelrelease.
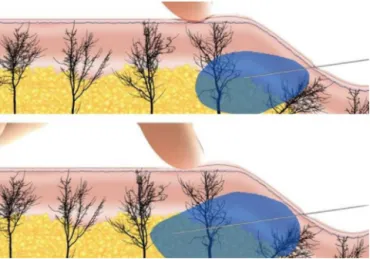
• Allnaturalskinfoldsonthehandandwrist,aswellasthe foldsbetweenthefingersand palm, haveligaments that attach the skin to deeper structures, such as the flexor sheaths.Thesecanslowthediffusionoftheswollenlocal anesthetic to the other side ofthe fold. Thelocal anes-theticwillcrossbelowtheskinfold,butonlyslowly,under pressure,andatlargevolumes.Itissensibletoinjecton bothsidesofthenaturalfolds,fromproximaltodistal,to decreasetheinjectionpain(Fig.4).
Epinephrine
and
vasovagal
syncope
adverse
reaction
Althoughlidocaineandepinephrineareprobablytwoofthe safestmedicationsinuse,injectingthemcancauserelatively commonsideeffects.Afterinjectionoflocalanestheticwith epinephrine,thepatientmayexperiencesymptomsof agita-tion,tremors,andnervousness.Thevasovagalreactionmay appearinresponsetoneedlepenetration.
Lossofconsciousnessor faintingafter avasovagal
syn-cope occurs because there is notenough blood going into
thebrain.Nature’ssolution,fainting,bringstheheaddown toallowmorebloodtoreachthebrainthroughtheeffectof gravity.
Asimplechangeofbandagesortheremovalofaplaster castmaycausefainting.Thepinchofaneedle,withorwithout localanesthesia,isalsoanothercommontriggerforfainting (vasovagalsyncope).
Ifthepatientshowssignsthathe/sheisabouttofaint,more blood can besenttothe brainwithsimplegravity-shifting maneuvers.
If the patientissitting,the surgeoncan askhim/herto liedown.Injectionofanestheticintheseatedpositionisnot recommended.
Ifthepatientislyingdown,he/shecanbeaskedtoplace thehandsunderthekneesandraisethembyflexingthehips andknees,sothatthebloodfromthelowerlimbsincreases cerebralirrigation.
Thesurgeonshouldremovethepillowunderthepatient’s headandplaceitunderhis/herfeet.
Thesurgeoncanalsoleantheheadofthebedtothe Tren-delenburgposition(headdownandfeetup).28,29
Tips
on
how
to
talk
to
patients
about
WALANT
Forpatients,thefearoftheunknownandanxietyaboutpain
arethetwomainconcernsofbeingawakeduringthehand
surgery.However,iftheprocessisexplainedtopatientscalmly, clearly,andconfidently,thefearoftheunknowncanbe over-come.Bygainingknowledgeoftheprocedure,thepatientcan feellikeanactiveparticipantinthetreatmentprocess,awake andcooperative.Ifthelocalanestheticinjectionhappensas described aboveandwithafine needle,thepatient willbe surprisedathowbriefandmildthediscomfortwillbe.
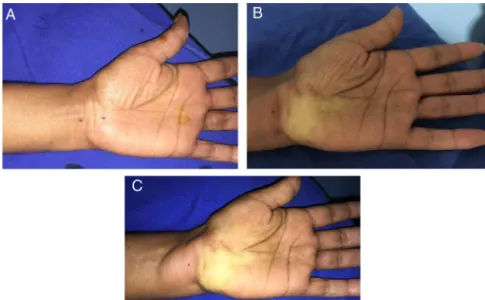
Fig.4–(A)Blockadewithlidocaineandadrenalineproximalanddistaltothewristfold;(B)beginningofthe vasoconstrictioneffectafter15min;(C)completeeffectafter30min.
Thepatientmay talk tothe physicianduringthe injec-tion of the local anesthetic. A slow injection will be less painful.
Afterfinishingtheinjection,thepatientmayfeel alittle nervousorabitagitated,asiftheyhavehadtoomuchcoffee. Theyshouldbeinformed thatthisisnotaneffectofbeing nervous,butratherthefactthatthereisabitofepinephrine inanestheticmedication.Thissensationiscompletelynormal andnotdangerous.Ifthishappens,itisimportanttomention thatitwilldisappearin5–30min,andthatitdoesnotmean thatsomethingiswrong.
The patient should be informed that they will feel
their hands cold and moist and that, during the surgery,
they will feel pulling and moving in the operated
site.
Aftersurgery,theywillsimplygetupandgohome;their handwillfeelasifitwasbiggerthantheirheart.Thepatients willhavesomerestriction.Theyshouldkeepthelimbelevated toreduceswellingandpain.
Talking
to
patients
during
surgery
Whenhandsurgeryisperformedwithsedation,itisnot pos-sibletoguidepatientsduringtheprocedure.Sedationdoes notallowthepatienttorememberwhatthephysicianspoke
tothemduetodrugsthatcause amnesia.When usingthe
WALANTtechnique,orientationpassedtothepatientduring surgeryisfoundtobeveryuseful.Duringtheprocedure, sur-geonscanguidetheirpatientsaboutpost-operativecareand onhowtoavoidcomplications.
Thetimespenttalkingtopatientsduringsurgeryisatime savedbeforeoraftersurgery.
Thistimewillhelptoreducethecomplicationsthatcould takeplaceinthepostoperativeperiod.
Things
that
should
not
be
said
or
done
during
surgery
Never say somethinglike “oops.”Surgeons must createan
atmosphereofcalmness,efficiency,andcompetence. Asilentsurgeonmayseemquitecompetent,whiletheone whotalksalotwithoutlisteningtothepatientcannotreassure him/her.
Thepatientwillbefullyawakeandattentivetoeverything thathappens.Therefore,whenorderinginstrumentsfromthe
roomnurse,surgeonsmustdosousingsignsortermssuch
as“number15”instead of“scalpelblade15”.“Singlehook” shouldbeusedinsteadof“skinhook”.
The surgeon should avoid passing compresses,
gauze, or instruments with blood in front of the
patient.
Sterile
surgical
drapes
for
simple
cases
Inthesterilesurgicalfield,smalldrapessheetsthatarethe sizeofcompressspongesareused(fenestrated40cm×40cm
sheet). The surgeon wears a mask and sterile gloves, and
does not wear a sterile apron. Therefore, only the drape
used willbe sterile,asin skincancer removalprocedures.
Studies have shown that, for some hand surgery
proce-dures, the steriledrape issufficient, does notincrease the
risk of infection, and reduces the cost by four times or
more.30–33
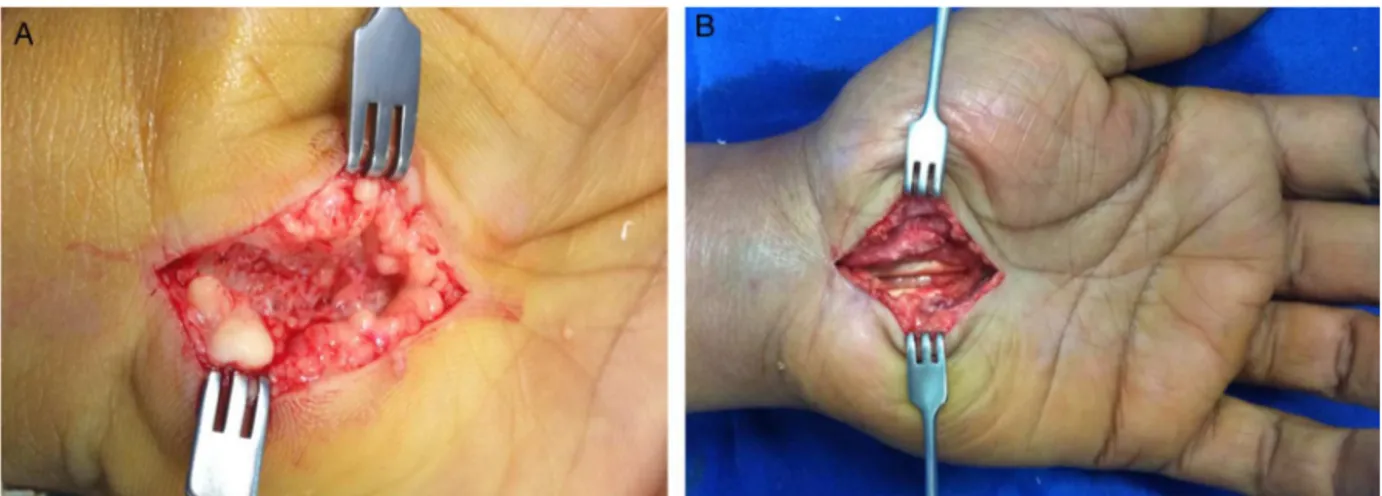
Fig.5–(A)Carpaltunnelreleaseapproachunderlidocaine/adrenalineeffect;(B)aftertheprocedureandstillunder lidocaine/adrenalineeffect,maintainingabloodlessoperatingfield.
Increased
revenue
and
reduced
costs
with
WALANT
• Iftheneedofatourniquetiseliminatedandalocal anes-theticisinjectedinanalmostpain-freeprocedure,thetwo mainreasonsfortheneedofsedationinmosthand sur-geriesareremoved.Oncepatientsunderstandthebenefits ofWALANT,mostwillnotwantsedationforhandsurgery (Fig.5).
• Theeliminationofsedationalsomeansthatmanyhand sur-geriescanbeeasilyperformedinsmallerprocedurerooms, whereonlytheoperativefieldissterile,inthesamewayas skintumorsareremoved.
• Theeliminationofthetourniquet,sedation,andtheneed foracompletelysterileroomforhandsurgerywhenusing
WALANTincreasespatient safetyandconvenience while
loweringcosts.Itreducesunnecessaryspendingsandmore patientswillbenefitfromhandsurgeries.33
• Eventually, insurance companies and governments will
understandthatsedationisnotnecessaryformanyhand surgeries. They will become receptive to the concept of increasingpatientsafetyandconveniencewhilelowering costs.
• Over time, insurance companies and governments will
be made aware of evidence-based medicine that
sup-ports the concept that a sterile field is safe and far
less expensivefor many hand surgeries. Thiswill lower costs.
• Negotiationbetweenhealth careproviders,insurers, and thegovernmentwillbenecessarysothatsomesurgeries
canbeperformedusingtheWALANTtechniqueinsimpler
operatingrooms.Certainly,everyonewillbereceptivetothe conceptofincreasingpatientsafetyandconveniencewhile loweringcosts.
Theaccreditation process forasurgical roomthat does
not use sedation is less expensive than that of a
facil-ity that uses sedation or general anesthesia. If sedation
is not used, the costs of its equipments and medications
disappear.
Final
considerations
Surgicalproceduresofthehandwiththepatientfullyawake
are beingpracticedbyagrowingnumberofhandsurgeons
in mostcountries ofthe world. This number isincreasing
becausethetechniqueissafer,moreconvenient,andmuch
moreaccessibleforbothpatientsandsurgeons.
These innovations depend on the cultural changes of
physicians, patients, institutions, and healthcare plans or insurersresponsibleforthecostsoftheprocedures.Surgeons mustrememberthattheyarealsoresponsibleforthecosts. MostsurgeonswhohavetestedWALANTcontinuetouseit.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.LalondeDH,MartinA.Epinephrineinlocalanesthesiain
fingerandhandsurgery:thecaseforwide-awakeanesthesia.
JAmAcadOrthopSurg.2013;21(8):443–7.
2.PhillipsA,JagodzinskiN,LalondDonaldH.Whatis
wide-awakehandsurgery?In:LalondeDH,editor.General
principlesofwide-awakehandsurgery.NewBrunswick:CRC
Press;2016.p.17–22.
3.BerecekKH,BrodyMJ.Evidenceforaneurotransmitterrole
forepinephrinederivedfromtheadrenalmedulla.AmJ
Physiol.1982;242(4):H593–601.
4.ThomsonCJ,LalondeDH,DenklerKA,FeichtAJ.Acritical
lookattheevidenceforandagainstelectiveepinephrineuse
inthefinger.PlastReconstrSurg.2007;119(1):260–6.
5.ChowdhryS,SeidenstrickerL,CooneyDS,HazaniR,Wilhelmi
BJ.Donotuseepinephrineindigitalblocks:mythortruth?
PartII.Aretrospectivereviewof1111cases.PlastReconstr
Surg.2010;126(6):2031–4.
6.Food,Drug,Administration.Warning–procainesolution.
JAMA.1948;138:599.
7.NodwellT,LalondeD.Howlongdoesittakephentolamineto
reverseadrenaline-inducedvasoconstrictioninthefingerand
Dalhousieprojectexperimentalphase.CanJPlastSurg. 2003;11(4):187–90.
8. LalondeD,BellM,BenoitP,SparkesG,DenklerK,ChangP.A
multicenterprospectivestudyof3,110consecutivecasesof
electiveepinephrineuseinthefingersandhand:the
DalhousieProjectclinicalphase.JHandSurgAm.
2005;30(5):1061–7.
9. LalondeDH,LalondeJF.Discussion.Donotuseepinephrinein
digitalblocks:mythortruth?PartII.Aretrospectivereviewof
1111cases.PlastReconstrSurg.2010;126(6):2035–6.
10.Fitzcharles-BoweC,DenklerK,LalondeD.Fingerinjection
withhigh-dose(1:1,000)epinephrine:doesitcausefinger
necrosisandshoulditbetreated?Hand(NY).2007;2(1):5–11.
11.MuckAE,BebartaVS,BorysDJ,MorganDL.Sixyearsof
epinephrinedigitalinjections:absenceofsignificantlocalor
systemiceffects.AnnEmergMed.2010;56(3):270–4.
12.HouSM,LiuTK.Salvageoftourniquet-inducedthumb
necrosisbyamodifiedwraparoundprocedure.JTrauma.
1987;27(7):803–5.
13.DenklerK.Acomprehensivereviewofepinephrineinthe
finger:todoornottodo.PlastReconstrSurg.
2001;108(1):114–24.
14.BurkRW3rd,Guzman-SteinG,VasconezLO.Lidocaineand
epinephrinelevelsintumescenttechniqueliposuction.Plast
ReconstrSurg.1996;97(7):1379–84.
15.FarhangkhoeeH,LalondeJ,LalondeDH.Teachingmedical
studentsresidentshowtoinjectlocalanesthesiaalmost
painlessly.CanJPlastSurg.2012;20(3):169–72.
16.StrazarAR,LeynesPG,LalondeDH.Minimizingthepainof
localanesthesiainjection.PlastReconstrSurg.
2013;132(3):675–84.
17.FrankSG,LalondeDH.Howacidicisthelidocaineweare
injecting,andhowmuchbicarbonateshouldweadd?CanJ
PlastSurgSummer.2012;20(2):71–3.
18.HoganME,vanderVaartS,PerampaladasK,MachadoM,
EinarsonTR,TaddioA.Systematicreviewandmeta-analysis
oftheeffectofwarminglocalanestheticsoninjectionpain.
AnnEmergMed.2011;58(1):86–98,e1.
19.HöfleM,HauckM,EngelAK,SenkowskiD.Viewinganeedle
prickingahandthatyouperceiveasyoursenhances
unpleasantnessofpain.Pain.2012;153(5):1074–81.
20.AminabadiNA,FarahaniRM.Theeffectofpre-coolingthe
injectionsiteonpediatricpainperceptionduringthe
administrationoflocalanesthesia.JContempDentPract.
2009;10(3):43–50.
21.NanitsosE,VartuliR,ForteA,DennisonPJ,PeckCC.Theeffect
ofvibrationonpainduringlocalanaesthesiainjections.Aust
DentJ.2009;54(2):94–100.
22.ArndtKA,BurtonC,NoeJM.Minimizingthepainoflocal
anesthesia.PlastReconstrSurg.1983;72(5):676–9.
23.MartiresKJ,MalbasaCL,BordeauxJS.Arandomized
controlledcrossovertrial:lidocaineinjectedata90-degree
anglecauseslesspainthanlidocaineinjectedata45-degree
angle.JAmAcadDermatol.2011;65(6):1231–3.
24.LalondeD,WongA.Localanesthetics:what’snewinminimal
paininjectionandbestevidenceinpaincontrol.Plast
ReconstrSurg.2014;1344Suppl.2:9S–40S.
25.WilliamsJG,LalondeDH.Randomizedcomparisonofthe
single-injectionvolarsubcutaneousblockandthe
two-injectiondorsalblockfordigitalanesthesia.Plast
ReconstrSurg.2006;118(5):1195–200.
26.WheelockME,LeblancM,ChungB,WilliamsJ,LalondeDH.Is
ittruethatinjectingpalmarfingerskinhurtsmorethan
dorsalskin?Newlevel1evidence.Hand(NY).2011;6(1):47–9.
27.HamelinND,St-AmandH,LalondeDH,HarrisPG,BrutusJP.
Decreasingthepainoffingerblockinjection:levelIIevidence.
Hand(NY).2013;8(1):67–70.
28.KopinIJ.Monoamineoxidasecatecholaminemetabolism.J
NeuralTransmSuppl.1994;41:57–67.
29.RosenSG,LinaresOA,SanfieldJA,ZechLA,LizzioVP,Halter
JB.Epinephrinekineticsinhumans:radiotracermethodology.
JClinEndocrinolMetab.1989;69(4):753–61.
30.AlamM,IbrahimO,NodzenskiM,StrasswimmerJM,JiangSI,
CohenJL,etal.Adverseeventsassociatedwithmohs
micrographicsurgery:multicenterprospectivecohortstudy
of20,821casesat23centers.JAMADermatol.
2013;149(12):1378–85.
31.LeblancMR,LalondeDH,ThomaA,BellM,WellsN,AllenM,
etal.Ismainoperatingroomsterilityreallynecessaryin
carpaltunnelsurgery?Amulticenterprospectivestudyof
minorprocedureroomfieldsterilitysurgery.Hand(NY).
2011;6(1):60–3.
32.LeblancMR,LalondeJ,LalondeDH.Adetailedcostand
efficiencyanalysisofperformingcarpaltunnelsurgeryinthe
mainoperatingroomversustheambulatorysettingin
Canada.Hand(NY).2007;2(4):173–8.
33.BismilM,BismilQ,HardingD,HarrisP,LamymanE,SansbyL.
Transitiontototalone-stopwide-awakehandsurgery
service-audit:aretrospectivereview.JRSMShortRep.