ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Influence
of
medical
care
in
the
quality
of
life
(WHOQOL-100)
of
women
living
with
systemic
lupus
erythematosus
Juliana
Passos
da
Silva,
Janete
Lane
Amadei
∗CentroUniversitáriodeMaringá(UniCesumar),Maringá,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12August2014 Accepted28January2015
Availableonline11September2015
Keywords:
Systemiclupuserythematosus Qualityoflife
Patientcare
a
b
s
t
r
a
c
t
Lupusrequirescarefultreatmentbymedicalspecialists.Thisstudyaimedtoevaluatethe qualityoflifeofpatientslivingwithSystemicLupus Erythematosus(SLE). Themethod approachedwomenwithaconfirmeddiagnosisofSLEundermedicalsupervisionina Uni-versityhospitaloutpatientclinicorinaprivateclinic.Weusedaninstrumentcontaining relevantinformationofthepatientandalsothePortugueseversionoftheWorldHealth Orga-nizationQualityofLifeGroup(WHOQOL-100)questionnaire.Thestudypopulationconsisted of39women,marriedintheirmajority(56.4%);prevalentlyaged37–60yearsold;prevalence ofdiagnosistimeoverfiveyears(66.7%);andinuseoflessthan5medications(69.2%). 92.3%hadthediseaseinactivewithhighermeansinmobility(p=0.0463)andqualityof life(p=0.0199)facets;ontheotherhand,thephysicalsafetyandsecurityfacet(p=0.0093) showedhighermeanforpeoplewithactivedisease.Healthandsocialcareanalysisshowed availabilityandquality(p=0.0434),evenwhenwithotherassociateddiseases(33.3%);and thehighestmeanswereDependenceonmedicinalsubstancesandmedicalaids(p=0.0143). Thenegativeresultsforassociateddiseaseswerehigherinsexualactivity(p=0.0431)and transportation(p=0.0319)facets.Inconclusion:ifwomenlivingwithSLEreceivecontinuous medicalattention,theywillenjoygoodqualityoflife,whileminimizingthecomplications inherentinthiscondition.
©2015ElsevierEditoraLtda.Allrightsreserved.
Influência
da
atenc¸ão
médica
na
qualidade
de
vida
(WHOQOL-100)
de
mulheres
com
lúpus
eritematoso
sistêmico
Palavras-chave:
Lúpuseritematososistêmico Qualidadedevida
Assistênciaaopaciente
r
e
s
u
m
o
Olúpusexigetratamento cuidadosopor médicos especialistas. Esteestudoteve como objetivoavaliaraqualidadedevidadepacientescomlúpuseritematososistêmico(LES). OmétodoabordoumulherescomdiagnósticoconfirmadodeLESsobacompanhamento médicoemambulatóriodehospitalescolaouparticular.Usou-seinstrumentoquecontinha informac¸õesrelevantesdopacienteeaversãoemportuguêsdoinstrumentodepesquisa
∗ Correspondingauthor.
E-mail:[email protected](J.L.Amadei). http://dx.doi.org/10.1016/j.rbre.2015.08.017
WorldHealthOrganizationQualityofLifeGroup(WHOQOL-100).Apopulac¸ãoestudada per-fez39mulheres,nasuamaioriacasadas(56,4%);comidadeprevalentede37a60anos;tempo dediagnósticoprevalentemaiordecincoanos(66,7%);usodemenosdecinco medicamen-tos(69,2%).Obteve-seque92,3%estavamcomadoenc¸acontroladacommédiasmaiores nasfacetasmobilidade(p=0,0463)equalidadedevida(p=0,0199).Jáafacetaseguranc¸a físicaeprotec¸ão(p=0,0093)apresentoumédiamaiorparapessoascomadoenc¸aemestado ativado.Asanálisesdecuidadosdesaúdeesociaisapresentaramdisponibilidadee qual-idade(p=0,0434)mesmocomoutraspatologiasassociadas(33,3%)easmaioresmédias foramdependênciademedicac¸ãooudetratamentos(p=0,0143).Osresultadosnegativos paradoenc¸aassociadaforammaioresnasfacetasatividadesexual(p=0,0431)etransporte (p=0,0319).Conclui-sequeseamulhercomLESreceberatenc¸ãomédicadeformacontinua apresentaráqualidadedevidaqueminimizaráascomplicac¸õesinerentesaessapatologia. ©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune chronicdiseasewithhighestincidenceintheagegroupfrom 15to40yearsold.1 SLEaffects10timesmorewomenthan
men,its treatmentvaries accordingto thetype and sever-ityofsymptomsand,duetoitscomplexnature,thisdisease requiresactiveparticipationofthepatienttomaintaina sat-isfactorylevelofhealth. SLEhasapoor prognosis,but the advancementoftherapeuticpossibilitieshasprovidedbetter qualityoflife(QoL)forpeoplelivingwiththisdisease.2
Beingachronicdisease,SLEhasaprevalentpsychosomatic dimension,anditisimportanttoconsiderthestressandthe psychosocialsufferingonitsonset,evolution,aggravationand potentialcontrol.Thisdisease requiresan interdisciplinary interventionforitscare,inadditiontoconsideringthe pecu-liarwaywithwhichthediseaseisexpressedinthelifeofevery individual,asthepsychosocialaspectscontributetothe com-plexityofthedevelopmentandexacerbationofsymptoms.3
Theeffectofthechangescausedbythe diseaseprocess anditstreatmentintheclinicalcourseofthediseasedemand measuresthatfavorQoLasacriticalinstrumentofsatisfaction forpatientsandhealthprofessionals.InpeoplewithSLE,a decreaseofQoLoccurscomparedwiththegeneralpopulation. ThisQoLlossisduetophysicalandemotionalchangescaused bythediseaseprocess,especiallyinperiodsofexacerbation ofSLE.1
QoL can be understood as consisting of three factors: subjectivewell-being,whichreferstothe perceptionofthe individual,his/hervaluesandbeliefs;health,understoodasa stateofphysical,mentalandsocialwell-beingandnotmerely astheabsenceofdisease;andthirdly,socialwell-being,which referstothesituationofthepersoninrelationtohis/her envi-ronmentandsociety.4
The assessment of QoL for women with SLE can be as important as the measurement of their morbidity and mortality,5 focusing on the ability to live without disease
or overcoming difficulties stemmed from morbidstates or conditions.6
Inmanycases,thedifficultyinunderstandingtheetiology andthepathophysiologicalprocessrelatedtothisdifficultto diagnosediseasepreventsitsspecifictreatment.7
TheassessmentofQoLinthese patientsisanessential elementsothatonecangetanideaoftheimpactofthedisease anditstreatmentinadistinctandcomplementaryway,which contributestoabettercareofpatientsandtheirfamiliesin theemotionaldistressmanagement,andalsofacilitatesthe experiencewithadiseasethatispainful,chronicandoften disabling.
Thisstudywas conductedwiththeaimtoevaluateQoL ofpatients livingwithSLEmedicallytreated inthe Cityof Maringa,StateofParana,aimingtoqualifytheassociated fac-torsandtheirinterferenceinQoL,withspecificcontributions tothisareaofknowledge.
Patients
and
methods
Thisisacross-sectionalstudyinvolvingwomenwith estab-lishedSLE,agedover18years,seenataRheumatologyprivate clinicandatauniversityhospitaloutpatientcliniclocatedin Maringa,Parana.Forinclusioninthestudy,thewomenmust havehadanappointmentfrequencyofatleastonceayear, withmedicalfollow-up,regardlessofthenatureofthepoint ofcare.
Thenumber ofparticipantswas delimitedbasedon the accesstopatientsand ontheiragreementtoparticipatein thestudy,andalsobytheirregularityinattendancetomedical careforatleastonceayear.
After signingthe Informed ConsentForm inagreement withthestudy,thepatienthadscheduledtheplaceanddate forcompletionofthestudyquestionnaires;orthecompletion ofthequestionnaireswascarriedoutwhenthewomanwas approached,afterobtainingherwrittenconsent.
The World Health Organization Quality of Life Group (WHOQOL-100) questionnaire is a generic QoL instrument drawnup in1998bytheWorldHealth Organization(WHO) basedonamulticenterstudy.WHOQOL-100contains ques-tionsthataddressthefollowingareas:physicalhealth(pain, discomfort,energyandfatigue,sleepandrest);psychological (positive feelings, thinking, learning, memory, concentra-tion,self-esteem,bodyimageandphysicalappearance,and negativefeelings);independencelevel(mobility,daily activi-ties,dependenceonmedicinalsubstancesandmedicalaids and working capacity); social relationships (personal rela-tionships,socialsupportandsexualactivity);environmental (physical safety and security, home environment, finan-cial resources, health care, social care, recreation/leisure, physical environment and transportation) and spiritual aspects/religion/personal beliefs (spirituality, religion, per-sonalbeliefs).
TheresultsofWHOQOL-100areexpressedthroughscores assigned for each facet and domain. For obtaining these scores,descriptivestatistics ofeachitemwere heldforthe followingelements:mean,standarddeviation,andminimum andmaximumvalues.8ToassessQoL,itwasdecidedthatthe
closerfrom100wasthesumofthescoresofthedomains,the betterthequalityoflife;thereverseistrue.
DatawerecomputedinMicrosoftExcelspreadsheet soft-ware (2010). For statistical analysis, the tool provided by Pedrosoetal.(2011),8basedonMicrosoftExcelsoftware,was
used.Thisinstrumentperformscalculationsresultingfrom theWHOQOL-100 application,according tothesyntax pro-posedbythe WHO WHOQOLGroup. Non-pairedt-testsfor domainsandfacetswere performed,alwaysconsideringas referencethestatisticalprogramsStatistica8.0andSAS Sys-tem9.1.
The project was evaluated and approved by CESUMAR EthicsCommittee(CEP-CESUMAR),accordingtocertificateNo. 106/2011andprotocolNo122/2011.
Results
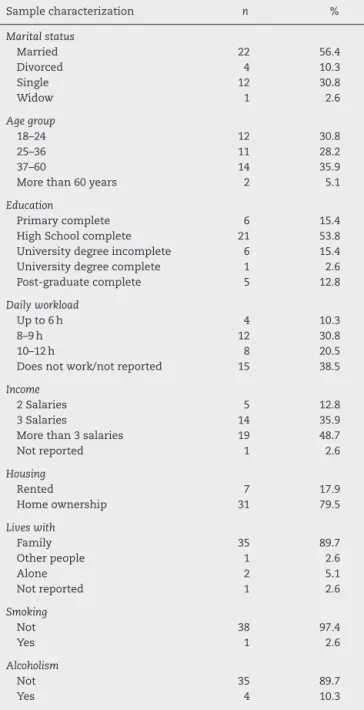
Thestudypopulationconsistedof39femalepatients;most weremarried(56.4%)andtheprevalentagegroupwasthatof 37–60yearsold(35.9%),followedby18–24yearsold(30.8%). Thisgrouphadagoodeducationallevel: 84.6%reported11 yearsormoreofstudy.Withrespecttosocialsupport,30.8% work 8–9h/day, and 20.5% work 10–12h/day;an incomeof threeormoreminimumwageswereprevalent(84.6%)inthe group. Asforhousing, 79.5% were homeownersand 89.7% werelivingwithfamilymembers.Aboutreportedhabits,97.4% didnotusetobaccoand89.7%didnotusealcohol(Table1).
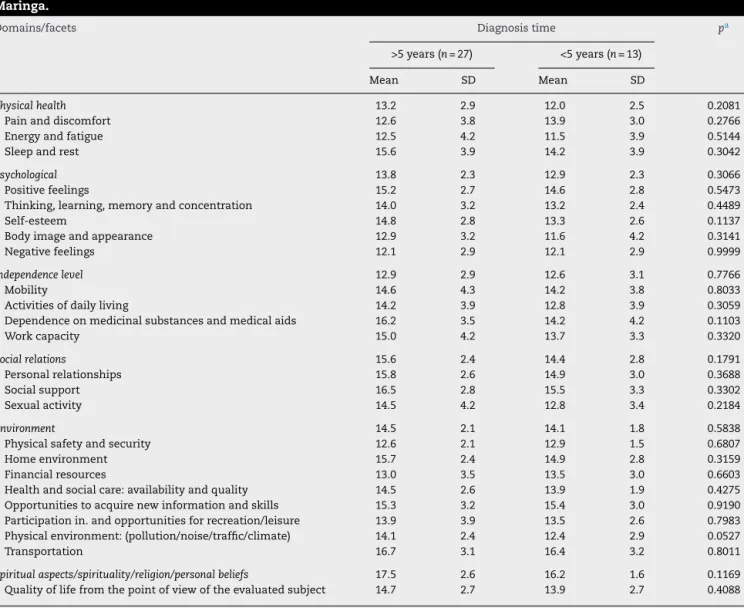
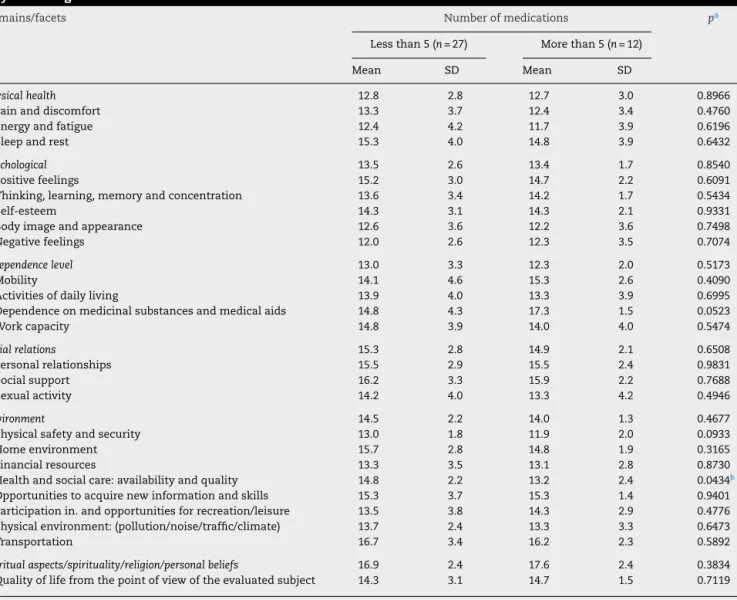
Atthetime oftheinterview,92.3% hadtheir disease in acontrolledstateand7.7%exhibitedanactivedisease.For most women (66.7%), the diagnosis had been established over5yearsago,andmost(69.2%)usedlessthan5 medica-tions.33.3%ofparticipantsreportedotherassociateddiseases. Comparing the domains of QoL (WHOQOL-100) with the timeelapsed sincethe diagnosis ofSLE,the highestmean (17.5±2.6)scorewasobtainedforSpiritualaspectsdomain, andthelowestmean(12.9±2.9)wasfoundforIndependence level.Withregardtototalscores(QoL),patientswithlessthan
Table1–Characterizationofsocio-demographicdataof womenwithSLE,CityofMaringa.
Samplecharacterization n %
Maritalstatus
Married 22 56.4
Divorced 4 10.3
Single 12 30.8
Widow 1 2.6
Agegroup
18–24 12 30.8
25–36 11 28.2
37–60 14 35.9
Morethan60years 2 5.1
Education
Primarycomplete 6 15.4
HighSchoolcomplete 21 53.8
Universitydegreeincomplete 6 15.4
Universitydegreecomplete 1 2.6
Post-graduatecomplete 5 12.8
Dailyworkload
Upto6h 4 10.3
8–9h 12 30.8
10–12h 8 20.5
Doesnotwork/notreported 15 38.5
Income
2Salaries 5 12.8
3Salaries 14 35.9
Morethan3salaries 19 48.7
Notreported 1 2.6
Housing
Rented 7 17.9
Homeownership 31 79.5
Liveswith
Family 35 89.7
Otherpeople 1 2.6
Alone 2 5.1
Notreported 1 2.6
Smoking
Not 38 97.4
Yes 1 2.6
Alcoholism
Not 35 89.7
Yes 4 10.3
5yearselapsedsincethediagnosisofSLEhadbetterqualityof life(87.3)versusthosewithmorethan5years(82.2).Inthe set-tingofastatisticalsignificanceof5%,nodifferencewasfound betweenthemeansforpatients,regardingthetimeelapsed sincethediagnosisofSLE(Table2).
Table2–Comparisonofqualityoflifedomainsandfacets(WHOQOL-100)relatedtothetimeofdiagnosis,Cityof Maringa.
Domains/facets Diagnosistime pa
>5years(n=27) <5years(n=13)
Mean SD Mean SD
Physicalhealth 13.2 2.9 12.0 2.5 0.2081
Painanddiscomfort 12.6 3.8 13.9 3.0 0.2766
Energyandfatigue 12.5 4.2 11.5 3.9 0.5144
Sleepandrest 15.6 3.9 14.2 3.9 0.3042
Psychological 13.8 2.3 12.9 2.3 0.3066
Positivefeelings 15.2 2.7 14.6 2.8 0.5473
Thinking,learning,memoryandconcentration 14.0 3.2 13.2 2.4 0.4489
Self-esteem 14.8 2.8 13.3 2.6 0.1137
Bodyimageandappearance 12.9 3.2 11.6 4.2 0.3141
Negativefeelings 12.1 2.9 12.1 2.9 0.9999
Independencelevel 12.9 2.9 12.6 3.1 0.7766
Mobility 14.6 4.3 14.2 3.8 0.8033
Activitiesofdailyliving 14.2 3.9 12.8 3.9 0.3059
Dependenceonmedicinalsubstancesandmedicalaids 16.2 3.5 14.2 4.2 0.1103
Workcapacity 15.0 4.2 13.7 3.3 0.3320
Socialrelations 15.6 2.4 14.4 2.8 0.1791
Personalrelationships 15.8 2.6 14.9 3.0 0.3688
Socialsupport 16.5 2.8 15.5 3.3 0.3302
Sexualactivity 14.5 4.2 12.8 3.4 0.2184
Environment 14.5 2.1 14.1 1.8 0.5838
Physicalsafetyandsecurity 12.6 2.1 12.9 1.5 0.6807
Homeenvironment 15.7 2.4 14.9 2.8 0.3159
Financialresources 13.0 3.5 13.5 3.0 0.6603
Healthandsocialcare:availabilityandquality 14.5 2.6 13.9 1.9 0.4275
Opportunitiestoacquirenewinformationandskills 15.3 3.2 15.4 3.0 0.9190
Participationin.andopportunitiesforrecreation/leisure 13.9 3.9 13.5 2.6 0.7983
Physicalenvironment:(pollution/noise/traffic/climate) 14.1 2.4 12.4 2.9 0.0527
Transportation 16.7 3.1 16.4 3.2 0.8011
Spiritualaspects/spirituality/religion/personalbeliefs 17.5 2.6 16.2 1.6 0.1169
Qualityoflifefromthepointofviewoftheevaluatedsubject 14.7 2.7 13.9 2.7 0.4088
SD,standarddeviation. a Non-pairedttest.
ofpatientstakinglessthanfivemedications(5%significance level).
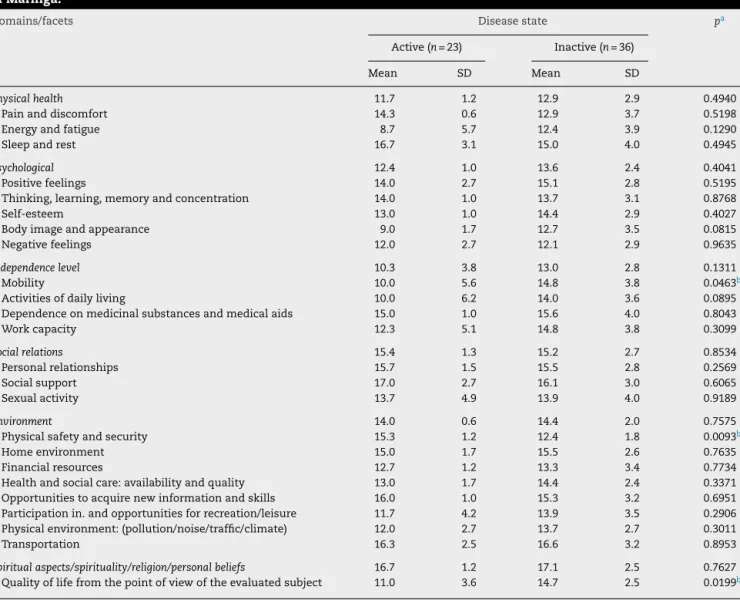
Table4showsthecomparisonbetweengroupsforactive orinactivedisease,wherethehighestmeanscorebelongsto Spiritual/Religion/PersonalBeliefsaspects(16.7±1.2)andthe lowestforindependencelevel(10.3±3.8),andthemeansof domainsbothforpatientswithactiveversusinactivedisease didnotdiffer,ata5%significancelevel.
Withrespecttothe individual analysis offacets,it was found that in people with inactive disease their means werehigherformobility(p=0.0463)andqualityoflifefacets reported by the interviewee(p=0.0199), while for physical safetyandsecurityfacet(p=0.0093)thegroupwithactive dis-ease(Table4)hadahighermean.
ItwasobservedthatQoLisbetterforthosepatientswith diseaseremission(86.1)versusthosewithactivedisease(80.5). Asignificantdifference(p<0.05)forthemeansoftheanalyzed domainswasnotevidenced(Table4).
AstodiseasesassociatedwithSLE,sixpatientsreported havinganotherdisease(s):oneofthe intervieweesreported
morethanonecondition,quoting osteoarthritis, osteoporo-sis,andfibromyalgia;andtheothers,onlyoneconditionfor each:bronchitis,anemia,hypertriglyceridemia, antiphospho-lipidsyndrome,anddrug-inducedhepatitis.
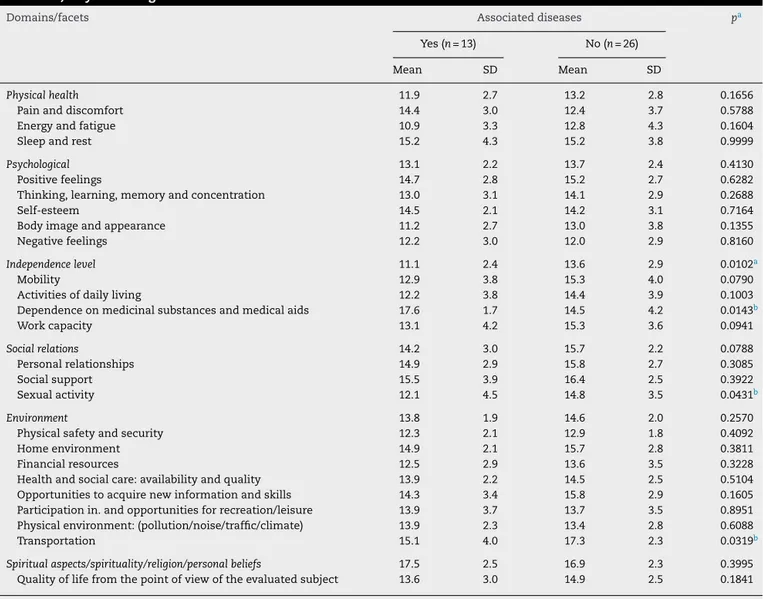
Table 5shows the means forthe comparisonofgroups
with respecttodiseases associated, withhigher scoresfor theenvironment(13.8±1.9).Themeanforindependencelevel domaindifferswhenpatientswithversuswithoutassociated diseaseswerecompared,withmeansof11.1±2.4vs.13.6±2.9 (p=0.0102),respectively,consideringthesignificancelevelof 5%.
Intheanalysisoffacets,withrespecttothereferenceof associateddiseases,itwasfoundthatthemeanofaffirmative referenceswashigherformedication ortreatment depend-ency facet(p=0.0143).Thenegativereferenceswere higher in Sexualactivity (p=0.0431) andtransportation (p=0.0319) facets.
Table3–Comparisonofqualityoflifedomainsandfacets(WHOQOL-100)relatedtotheamountofmedicationstaken, CityofMaringa.
Domains/facets Numberofmedications pa
Lessthan5(n=27) Morethan5(n=12)
Mean SD Mean SD
Physicalhealth 12.8 2.8 12.7 3.0 0.8966
Painanddiscomfort 13.3 3.7 12.4 3.4 0.4760
Energyandfatigue 12.4 4.2 11.7 3.9 0.6196
Sleepandrest 15.3 4.0 14.8 3.9 0.6432
Psychological 13.5 2.6 13.4 1.7 0.8540
Positivefeelings 15.2 3.0 14.7 2.2 0.6091
Thinking,learning,memoryandconcentration 13.6 3.4 14.2 1.7 0.5434
Self-esteem 14.3 3.1 14.3 2.1 0.9331
Bodyimageandappearance 12.6 3.6 12.2 3.6 0.7498
Negativefeelings 12.0 2.6 12.3 3.5 0.7074
Independencelevel 13.0 3.3 12.3 2.0 0.5173
Mobility 14.1 4.6 15.3 2.6 0.4090
Activitiesofdailyliving 13.9 4.0 13.3 3.9 0.6995
Dependenceonmedicinalsubstancesandmedicalaids 14.8 4.3 17.3 1.5 0.0523
Workcapacity 14.8 3.9 14.0 4.0 0.5474
Socialrelations 15.3 2.8 14.9 2.1 0.6508
Personalrelationships 15.5 2.9 15.5 2.4 0.9831
Socialsupport 16.2 3.3 15.9 2.2 0.7688
Sexualactivity 14.2 4.0 13.3 4.2 0.4946
Environment 14.5 2.2 14.0 1.3 0.4677
Physicalsafetyandsecurity 13.0 1.8 11.9 2.0 0.0933
Homeenvironment 15.7 2.8 14.8 1.9 0.3165
Financialresources 13.3 3.5 13.1 2.8 0.8730
Healthandsocialcare:availabilityandquality 14.8 2.2 13.2 2.4 0.0434b
Opportunitiestoacquirenewinformationandskills 15.3 3.7 15.3 1.4 0.9401
Participationin.andopportunitiesforrecreation/leisure 13.5 3.8 14.3 2.9 0.4776
Physicalenvironment:(pollution/noise/traffic/climate) 13.7 2.4 13.3 3.3 0.6473
Transportation 16.7 3.4 16.2 2.3 0.5892
Spiritualaspects/spirituality/religion/personalbeliefs 16.9 2.4 17.6 2.4 0.3834
Qualityoflifefromthepointofviewoftheevaluatedsubject 14.3 3.1 14.7 1.5 0.7119
SD,standarddeviation. a Non-pairedttest.
b Significantconsideringasignificancelevelof5%.
whoreportedcomorbidity(81.6).Theanalyzedpatientshad totalmeanvaluesabove80inallaspectsanalyzed,meaning agoodqualityoflife.
Discussion
Thequalityoflifequestionnairesprovideamorecomplete assessmentoftheimpactofdiseaseandoftreatmentinthe patients’dailylife.9
Withregardtodiagnosis,ahighermeanforindependence level was found. A diagnosis with definition of pathology representatimewhenlifecanundergosignificantchanges, dependingofthespecificsofthediseaseandthesymptoms experienced,besidestheneedtocontroland/orminimizethe recurrenceofthesesymptoms.
Araújo and Traverso-Yépez (2007)3 suggested that most
womenfinditdifficulttofacesuchadiagnosis,andmostof themexpressasenseofshock,centeredonthefindingofa dis-easethathasnocure.Whenevaluatingpatientsfollowedin
arheumatologyoutpatientclinic,SantiagoDantas,Carvalho, Viana,andFontenele10foundthat86.7%ofpatientswhowere
hospitalizedhadupto5yearsofdiagnosis.Assisiand Baak-lini(2009)11stressedthatthesurvivalofpatientswithSLEhas
increasedinrecentdecades,thankstoearlierdiagnosesand theuseofmedications.
Theuseoflessthanfivemedicationsmaybecriticalfor QoL.ThesamenumberwasobtainedbySantos(2009)12;these
authorsshowedthatthenumberofmedicationsrangedfrom oneto15,withameanof5.09±2.48.Thisamountof medi-cationsisjustifiedbyBorbaetal.(2008)13;intheirview,the
maintenanceofdrugtherapyininactivepatientsreducesthe possibilityofanewoutburstofactivity,improvestheirlipid profileandreducestheriskofthrombosis.
Table4–Comparisonofqualityoflifedomainsandfacets(WHOQOL-100)relatedtodiseasestate–activeorinactive,City ofMaringa.
Domains/facets Diseasestate pa
Active(n=23) Inactive(n=36)
Mean SD Mean SD
Physicalhealth 11.7 1.2 12.9 2.9 0.4940
Painanddiscomfort 14.3 0.6 12.9 3.7 0.5198
Energyandfatigue 8.7 5.7 12.4 3.9 0.1290
Sleepandrest 16.7 3.1 15.0 4.0 0.4945
Psychological 12.4 1.0 13.6 2.4 0.4041
Positivefeelings 14.0 2.7 15.1 2.8 0.5195
Thinking,learning,memoryandconcentration 14.0 1.0 13.7 3.1 0.8768
Self-esteem 13.0 1.0 14.4 2.9 0.4027
Bodyimageandappearance 9.0 1.7 12.7 3.5 0.0815
Negativefeelings 12.0 2.7 12.1 2.9 0.9635
Independencelevel 10.3 3.8 13.0 2.8 0.1311
Mobility 10.0 5.6 14.8 3.8 0.0463b
Activitiesofdailyliving 10.0 6.2 14.0 3.6 0.0895
Dependenceonmedicinalsubstancesandmedicalaids 15.0 1.0 15.6 4.0 0.8043
Workcapacity 12.3 5.1 14.8 3.8 0.3099
Socialrelations 15.4 1.3 15.2 2.7 0.8534
Personalrelationships 15.7 1.5 15.5 2.8 0.2569
Socialsupport 17.0 2.7 16.1 3.0 0.6065
Sexualactivity 13.7 4.9 13.9 4.0 0.9189
Environment 14.0 0.6 14.4 2.0 0.7575
Physicalsafetyandsecurity 15.3 1.2 12.4 1.8 0.0093b
Homeenvironment 15.0 1.7 15.5 2.6 0.7635
Financialresources 12.7 1.2 13.3 3.4 0.7734
Healthandsocialcare:availabilityandquality 13.0 1.7 14.4 2.4 0.3371
Opportunitiestoacquirenewinformationandskills 16.0 1.0 15.3 3.2 0.6951
Participationin.andopportunitiesforrecreation/leisure 11.7 4.2 13.9 3.5 0.2906
Physicalenvironment:(pollution/noise/traffic/climate) 12.0 2.7 13.7 2.7 0.3011
Transportation 16.3 2.5 16.6 3.2 0.8953
Spiritualaspects/spirituality/religion/personalbeliefs 16.7 1.2 17.1 2.5 0.7627
Qualityoflifefromthepointofviewoftheevaluatedsubject 11.0 3.6 14.7 2.5 0.0199b
SD,standarddeviation. a Non-pairedttest.
b Significantconsideringasignificancelevelof5%.
environment. Theperceptionofthe environmental dimen-siondependsonahierarchyofvaluesandthisisanindividual process,butitreflectsthecurrentconditionsofcollectivelife anditsimpactonthelivesofwomenanalyzedinthisstudy. WomenwithactiveSLEhadworseQoLinphysical, psycho-logicalandenvironmentaldomains.InSLEpatientswithan intenselyactivedisease,itwasobservedaworseconditionof QoLversuswomenwithinactiveSLE.1
ThumbooandStrand(2007)14foundthatpatientswithSLE
showmajordeficienciesinfunctionalstatuscomparedtothe generalpopulation,and that the specificmanifestationsof lupus(diseaseactivity,priorrenalinvolvementand fibromyal-gia)caninfluencetheQoLreported.
Freire et al. (2011)15 suggested that, inmany cases, the
organicandpsychologicaldamagetowhichpatientswithSLE aresubjectresultinphysicalormentaldisability,besidesother drawbacks,worseningQoL,whichhasbeenrecognizedasan importantindicatorofhealthforpatientswithchronic dis-eases.
When referring associateddiseases,the patientsin this studyindicatedthatthedependenceonmedicinalsubstances and medical aids facet interferes with QoL. Araújo and Traverso-Yépez(2007)3reportedthatsomepatientsreported
thattheynolongerhada“normal”life,alsoadmittingwith regret theneed“tohavetodependonmedicationforlife.” Medicationisthekeyfactorforhelpingindiseasecontrol.The lackofmedicationwouldalsobethemaindetrimentalfactor forthesepatients.However,itisclearthatnotallparticipants makethisrelationship,whenindicatingemotionalfactorsas majorcontributorstotheiruncontrolleddisease.
Amongthenegativeresponses,significancewasobserved for sexual activity and transportation facets. Silva (2009)16
showed that 4% of women and adult men with SLE pre-sentedsexualdysfunctions,accordingtotheirmedicalhistory. FolomeevandAlekberova(1990)17identifiedahighfrequency
Table5–Comparisonofqualityoflifedomainsandfacets(WHOQOL-100)relatedtoreportsofotherdiseasesassociated withSLE,CityofMaringa.
Domains/facets Associateddiseases pa
Yes(n=13) No(n=26)
Mean SD Mean SD
Physicalhealth 11.9 2.7 13.2 2.8 0.1656
Painanddiscomfort 14.4 3.0 12.4 3.7 0.5788
Energyandfatigue 10.9 3.3 12.8 4.3 0.1604
Sleepandrest 15.2 4.3 15.2 3.8 0.9999
Psychological 13.1 2.2 13.7 2.4 0.4130
Positivefeelings 14.7 2.8 15.2 2.7 0.6282
Thinking,learning,memoryandconcentration 13.0 3.1 14.1 2.9 0.2688
Self-esteem 14.5 2.1 14.2 3.1 0.7164
Bodyimageandappearance 11.2 2.7 13.0 3.8 0.1355
Negativefeelings 12.2 3.0 12.0 2.9 0.8160
Independencelevel 11.1 2.4 13.6 2.9 0.0102a
Mobility 12.9 3.8 15.3 4.0 0.0790
Activitiesofdailyliving 12.2 3.8 14.4 3.9 0.1003
Dependenceonmedicinalsubstancesandmedicalaids 17.6 1.7 14.5 4.2 0.0143b
Workcapacity 13.1 4.2 15.3 3.6 0.0941
Socialrelations 14.2 3.0 15.7 2.2 0.0788
Personalrelationships 14.9 2.9 15.8 2.7 0.3085
Socialsupport 15.5 3.9 16.4 2.5 0.3922
Sexualactivity 12.1 4.5 14.8 3.5 0.0431b
Environment 13.8 1.9 14.6 2.0 0.2570
Physicalsafetyandsecurity 12.3 2.1 12.9 1.8 0.4092
Homeenvironment 14.9 2.1 15.7 2.8 0.3811
Financialresources 12.5 2.9 13.6 3.5 0.3228
Healthandsocialcare:availabilityandquality 13.9 2.2 14.5 2.5 0.5104
Opportunitiestoacquirenewinformationandskills 14.3 3.4 15.8 2.9 0.1605
Participationin.andopportunitiesforrecreation/leisure 13.9 3.7 13.7 3.5 0.8951
Physicalenvironment:(pollution/noise/traffic/climate) 13.9 2.3 13.4 2.8 0.6088
Transportation 15.1 4.0 17.3 2.3 0.0319b
Spiritualaspects/spirituality/religion/personalbeliefs 17.5 2.5 16.9 2.3 0.3995
Qualityoflifefromthepointofviewoftheevaluatedsubject 13.6 3.0 14.9 2.5 0.1841
SD,standarddeviation. a Non-pairedttest.
b Significantconsideringasignificancelevelof5%.
lubrication,andsexualsatisfactioninthegroupwithlupus
versusamatchedcontrolgroup.
Silva(2009)16 showedthat sexual dysfunctioninfemale
adolescentswithlupusisamultifactorialconditionandcan occurrelatedtodiseaseactivityitself,orbymedicationssuch ascorticosteroidsandimmunosuppressants. Thestudy has notshown anassociation betweensexual dysfunctionand lupusactivity,thecumulativedamagecausedbydisease,or medicationuse.
Incontrast,Reis(2009)19assessedsatisfactioninthe
rela-tionshipand affectioninthe periodofexacerbationofthe disease among74 womenwith SLEwho keptheterosexual relationship,andnotedthatthosewomenwho hadgreater physicalintimacywiththeirpartnersreportedgreat satisfac-tionwiththeirrelationship; thosewho avoidedor hadless physicalintimacypointedtoanintenselynegativeeffect.This studyalsorevealedthedilemmasfacedbywomentomaintain intimacywiththeirpartnersduringdiseaseactivity.
Vido and Scanavini (2007)20 emphasized that economic
dependence,discrimination,difficultiesaffectingsexualand
reproductivelivesandinadequatehousingandenvironmental conditionsarefactorsthatcontributetoprogressive deteriora-tionofhealth,relationshipsandQoLtothosewhoexperience SLE.
Thetransportationreferencedbyintervieweeswas charac-terizedbyReis(2009),19whenthisauthoridentifieddifficulties
experiencedbywomeninordertomaintaintheirtreatment and accesstocare. Transportationwas notalways guaran-teed, thedistances werelarge, the traveltime lengthy, the access to specific medications was poor and the women had difficultyinmeeting theirrequirementsforfoodwhile traveling.
Final
considerations
optimism,withacceptanceoftheirlimitationsandenjoying whatis best forthem in their life,seeking intheir family andpersonalbeliefsforcesforthechallengesthatthedisease imposes.
Itwas demonstrated that womenwith SLEmay have a goodQoL,shouldtheytakeadvantageofspecializedmedical care.Withaneffectivetreatment,thediseaseremains inac-tive,providingsecuritytopatientsandresultinginemotional control,decreasedpainandimprovementinothersymptoms andinimprovedexpectations,meaningthatitispossibleto getonwellwiththedisease,culminatingwithagoodqualityof life.
Astolimitationsofthisstudy,wecanmentionthefactthat SLEpatientscompletedtheinstrumentsusedinthisstudyin thewaitingroomofthemedicaloffice;thisfactcouldimply in concentration difficulties to answer the questionnaires. Anotherlimitationrelatestotheinstrumentusedwhich,by beinglengthyandrepetitive,couldbetiringforthewomen. Theoriginofpatientcarecanbeaweakpointofthisstudy. Duetothenumberofrespondents,itwasnotpossibleto strat-ifythesubjectsinagroupwithpublicunitcareandinanother groupwithprivatehealthcare.Furtherstudieswithspecific groups,accordingtounittype,aresuggested.
Funding
Thisstudywas fundedthroughthe Programade Bolsasde Iniciac¸ãoCientíficadoCesumar(PICC).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
OurthankstotheProgramadeIniciac¸ãoCientificadoUniCesumar
–CentroUniversitáriodeMaringá,whichsupportedthe devel-opmentofthisstudy.
r
e
f
e
r
e
n
c
e
s
1. ReisMG,CostaIP.Qualidadedevidarelacionadaàsaúdeem pacientescomlúpuseritematososistêmiconoCentro-Oeste doBrasil.RevBrasReumatol.2010;50(4):408–14.
2. MattjeGD,TuratoER.LifeexperienceswithSystemicLupus Erythematosusasreportedinoutpatients’perspective:a clinical-qualitativestudyinBrazil.RevLatino-Am Enfermagem.2006;14(4):475–82.
3.AraujoAD,Traverso-YepezMA.Expressõesesentidosdo lúpuseritematososistêmico(LES).Estudpsicol(Natal). 2007;12(2):119–27.
4.CostaCC,BastianiM,GeyerJG,CalvettiPU,MullerMC,Moraes MLA.Qualidadedevidaebem-estarespiritualem
universitáriosdepsicologia.PsicolEstud.2008;13(2):249–55. 5.LamKW,PetriM.Assessmentofsystemiclupus
erythematosus.ClinExpRheumatol.2005;23Suppl. 39:S120–32.
6.MinayoMCS,HartzZMA,BussPM.Qualidadedevidaesaúde: umdebatenecessário.CiêncSaúdeColetiva.2000;5(1):7–18. 7.GalindoCVF,VeigaRKA.Característicasclínicase
diagnósticasdolúpuseritematososistêmico:umarevisão. RevEletrônFarmácia.2010;7(4):46–59.
8.PedrosoB,PilattiLA,SantosCB,PicininCT.Validac¸ãoDa SintaxeUnificadaparaoCálculodosEscoresdos
InstrumentosWHOQOL.Conexões:revistadaFaculdadede Educac¸ãoFísicadaUNICAMP.2011;9(1):130–56.
9.NobreMRC.Qualidadedevida.Availableat:http://www. arquivosonline.com.br/pesquisartigos/Pdfs/1995/v64N4/ 64040002.pdf[accessedin24.09.14].
10.SantiagoMPB,DantasNCB,CarvalhoSBF,VianaRM, FonteneleSMA.Atividade,gravidadeeprognósticode pacientescomlúpuseritematososistêmico.Antes,durantee apósprimainternac¸ão.JHealthBiolSci.2014;2(2):65–73. 11.AssisMR,BaakliniCE.ComodiagnosticaretratarLúpus
EritematosoSistêmico.RevistaBrasileiradeMedicina2009. Availablefromhttp://www.cibersaude.com.br/revistas.asp? fase=r003&idmateria=4087[accessedin09.05.14].
12.SantosMO.Avaliac¸ãodaadesãoàterapêutica medicamentosaempacientescomlúpuseritematoso sistêmicoatendidosemhospitaluniversitárionacidadedo RiodeJaneiro,Brasil.RiodeJaneiro.2009.
13.BorbaEF,LatorreLC,BrenolJCTB,KayserC,SilvaNA, ZimmermannAF,etal.Consensodelúpuseritematoso sistêmico.RevBrasilReumatol.2008;48(4):196–207.
14.ThumbooJ,StrandV.Health-relatedqualityoflifeinpatients withsystemiclupuserythematosus:anupdate.AnnAcad MedSingapore.2007;36(2):115–22.
15.FreireEAM,SoutoLM,CiconelliRM.Medidasdeavaliac¸ãoem lúpuseritematososistêmico.RevBrasReumatol.
2011;51:70–80.
16.SilvaCAA,FebrônioMA,BonfáE,PereiraRMR,PereiraEAG, TakiuitiAD.Func¸ãosexualesaúdereprodutivaemmulheres adolescentescomlúpuseritematososistêmicojuvenil.Rev BrasReumatol.2009;49:690–702.
17.FolomeevM,AlekberovaZ.Impotenceinsystemiclupus erythematosus.JRheumatol.1990;17:117–9.
18.CurrySL,LevineSB,CortyE,JonesPK,KuritDM.Theimpact ofsystemiclupuserythematosusonwomen’ssexual functioning.JRheumatol.1994;21:2254–60.
19.ReisMGR.Qualidadedevidademulheresadultascomlúpus eritematososistêmico.CampoGrande,2009.
[Tese–UniversidadeFederaldeMatoGrossodoSul]. 20.VidoM.B.,ScanaviniR.M.Qualidadedevidaeasaúdeda