w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Sociodemographic
and
clinical
features
and
quality
of
life
in
stomized
patients
夽
Merifane
Januário
de
Sousa
a,b,
Smalyanna
Sgren
da
Costa
Andrade
c,d,∗,
Karen
Krystine
Gonc¸alves
de
Brito
b,c,
Suellen
Duarte
de
Oliveira
Matos
c,d,
Hemílio
Fernandes
Campos
Coêlho
e,f,
Simone
Helena
dos
Santos
Oliveira
b,c,daHospitalGeneralEdsonRamalho,JoãoPessoa,PB,Brazil
bGrupodeEstudosePesquisasemTratamentodeFeridas(GEPEFE),JoãoPessoa,PB,Brazil cPost-GraduatePrograminNursing,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil dGrupodePesquisaemDoenc¸asCrônicas(GEPDOC),JoãoPessoa,PB,Brazil
ePost-GraduatePrograminHealthandDecisionModels,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil fDepartmentofStatistics,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received26July2015 Accepted6December2015 Availableonline10February2016
Keywords: Qualityoflife Ostomy Health
a
b
s
t
r
a
c
t
Objectives: Toidentifyuserswithanintestinalostomyconcerningtheirsociodemographic andclinicalcharacteristics,andtodeterminethescoresforqualityoflifeaccordingtothe domainsofthequestionnaireCityofHope.
Method:Thisisahousehold,descriptive,transversal,quantitative-approachsurvey, accom-plishedwith30registeredusersattheOstomyAssociationoftheStateofParaíba,Brazil.A specificformforostomypatientswasapplied,anddataanalysiswasperformedwiththe useofthesoftwareStatisticalPackageforSocialSciences(SPSS)version20.0.Thisstudy wasapprovedbyCAAENo.17224613.8.0000.5183.
Results:Mostparticipantswereover60years,wereCatholics,withelementaryeducation, anincomeuptothreeminimumwages,marriedorinastablerelationship,withalmost allqualityoflifescoresabovethemidpointoftherangeofthevariablesofthedomains surveyedbythequestionnaireCityofHope.
Conclusion: Thequestionnaireledtotheconclusionthattherespondentswithostomyhad asatisfactoryqualityoflife.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
夽
ResearcharisingfromMaster’sDissertation,“Qualidadedevidadepessoascomestomiaintestinal”,ProgramadePós-Graduac¸ãoem Enfermagem,UniversidadeFederaldaParaíba(UFPB),JoãoPessoa,PB,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](S.S.daCostaAndrade).
http://dx.doi.org/10.1016/j.jcol.2015.12.005
Características
sociodemográficas
e
clínicas
e
qualidade
de
vida
de
pessoas
com
estomia
intestinal
Palavras-chave: Qualidadedevida Estomia
Saúde
r
e
s
u
m
o
Objetivos: Caracterizarosusuárioscomestomiasintestinaisquantoaosaspectos sociode-mográficoseclínicosedeterminarosescoresdequalidadedevidasegundodomíniosdo questionárioCityofHope.
Método: Trata-sedeinquéritodomiciliar,descritivo,transversaledeabordagem quanti-tativa,realizadocom30usuárioscadastradosnaAssociac¸ãode OstomizadosdoEstado daParaíba.Utilizou-seformulárioespecíficoparaestomizadoseaanálisedosdadosfoi realizadacomoauxíliodoprogramaStatisticalPackagefortheSocialScience(SPSS),versão 20.0.ApesquisafoiaprovadacomCAAEn.17224613.8.0000.5183.
Resultados: Amaioriatinhamaisde60anos,católicos,comensinofundamental,rendade atétrêssalários,casadosouemuniãoestável,comquasetodososescoresdequalidade devidaacimadopontomédiodaescalaparaasvariáveisdosdomíniosexploradospelo questionárioCityofHope.
Conclusão: Oinstrumentopermitiuinferirqueosestomizadospesquisadospossuíam qual-idadedevidasatisfatória.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Themakingofastomaindicatesthetemporaryorpermanent externalizationofahollowviscusinthebody.Dependingon theexternalizedsegment,thetypeofostomyreceivesnames suchascolostomy,ileostomy,andurostomy,amongothers. Thistherapeuticprocedureiscausedbyvariousdiseases.1,2
AlthoughofficialinformationfromtheMinistryofHealth on the situation of ostomized people in Brazil are non-existent,3 data published by the Brazilian Association of Ostomized People estimate that 33,864 people live with a stomainourcountry,with4,176livingintheNortheastRegion, ofwhich496areinthestateofParaiba.4
Thebiopsychosocialconsequencesofanostomyprocedure areassociatedwiththesurgicaltreatment,andinfluencethe livesofthesepeopleandoftheirfamilies.Thebowelostomy hasbeenidentifiedasthemainchangethatcouldaffect inter-personal,social,labor,sexandleisureaspects.5,6
Of all the changes caused by the stoma, the physi-calchanges stand out, notonly byaffectingthe intestinal physiological process,but by its impact on self-imageand self-esteem.Ontheotherhand,thepresenceofastomacan leadtomentalandemotionalimbalance,aswellas interfer-ing directly inthe quality oflife. Thephysicalappearance assumesincreasinglyconsiderabledimensionswhenitcomes tochronicwounds,giventhattheskinpossessesan essen-tialandalmostsymboliccharacteristiconthelivesofeach individual,representing aworld wherebody and spiritget together.Thus,theskinconfiguresitsself-wellness.7
Themultipletransformationsresultingfromthecolostomy deeplyaffectthequalityoflifeofpatientsundergoingthis pro-cedure,whichpromptedtostudiesonthissubject.8–11Onecan observethat,inordertohaveagoodqualityoflife,itiscritical thatpeoplefeelsatisfiedinmanyways,includingmaintaining
theirphysicalintegrity,whichisbrokenduringtheprocessof makingthestoma.12
Therefore,theknowledgeofsocialandclinical character-isticsandofaspectsofqualityoflifeofostomypeoplemay facilitatetheplanningofassistanceinreliefprograms, consid-eringthemaintenanceofaconcomitantadjuvanttreatment andofdemandsofotherneedsarisingfromtheclinical con-ditionofthebowelostomizedpatient,which,aftertheradical change that occurred intheir pattern ofelimination,must relearntolivewithhimselfandwithhis/herfamily,friends andsociety.
Consideringthesensitivityofthesubject,weconsiderthat theinvestmentinresearchseekingfurtherclarificationonthe issueishighlyrelevant.Thus,theobjectivesoutlinedinthis studywere:tocharacterizeuserswithanintestinalostomyas sociodemographicand clinicalcharacteristics,and to deter-mine the quality of life scores according to the domains coveredinthequestionnaireCityofHope.
Method
Thisishouseholdsurvey,descriptive,cross-sectionalandof quantitativeapproachstudy.Theinitialcontributiontothis study came from the Ostomy Association of the State of Paraíba (AOEPB).AOEPB isconsidered a referral servicefor stomizedpeopleinthatState,beinglinkedtotheoutpatient departmentofateachinghospitalinthecityofJoãoPessoa.
peopleregisteredatAOEPBuptoDecember2012were identi-fied.Atfirst,telephonecontactattemptsweremade,but92 individuals couldnot bereachedforvarious reasons (non-existentphonenumber,orphonenumbernotfound).
Ofthe131remainingregisteredpeople,77individualsdid notmeetthe inclusion criteria, i.e.theywere excluded for beingunder legalage, byreversal ofthe colostomy and/or death. In addition, 24 refused a home visit, claiming that theydidnotfeelcomfortabletalkingaboutthissubject.Thus, 30individualsremainedinthesample.Afterconfirmingthe desiretoparticipate,avisitwasscheduledtoadministerthe questionnaireintheparticipant’shome.
Fordatacollection,twoinstrumentswereused:aform con-sistingofsociodemographicquestionsandclinicaldataofthe participants,andaquestionnaire,theCityofHope–Quality ofLifeQuestionnaireforaPatientwithanOstomy.13Thetotal scorewasobtainedbythearithmeticmeanofthe43questions containedintheinstrument(i.e.,thesumofthescoresofall itemsoftheinstrument,dividedby43).Thearithmeticmean ofalldomainswasobtainedtakingintoaccountthenumber ofvariablesineachofthedomains.
Inthisstudy,ascoreof5wassetasthecutoffpoint.Thus, means>5indicateagoodQoL,andmeans<5suggestapoor QoL.Thescore5isthemidpointonthescaleofassessment ofthevariablesthatmakeuptheinstrumentapplied.13For acorrectinterpretationoftheresults,someitemshadtheir scoresreversed;theseitemswere:1–12,15,18and19,22–30, 32–34and37.13Thecontactphasewascarriedout between September2013andFebruary2014.Datacollectionoccurred fromFebruarytoApril2014.
Data were compiled and analyzed using the Statistical PackagefortheSocialSciences(SPSS)program,version20.0, usingdescriptive statistics (absolute frequency, percentage, andmean/standarddeviation).Theprojectwasapprovedby theResearchEthicsCommitteeunderreportnumber370838 andCertificateNo.17224613.8.0000.5183.Allparticipantswere informedaboutthepurposeoftheresearch,itssecrecy,the rightofwithdrawal,andsigningoftheFreeandInformed Con-sentform,bearing inmindthe requirementsofResolution 466/12oftheNationalHealthCouncil.14
Results
Participantshadameanageof60.67±11.76years,with preva-lenceintheagegroups51–59yearsand59–67years,bothwith 8(26.7%)respondents.Astogender,therewasequityinthe distribution,since15(50%)werewomenand15(50%)men, constitutingacoincidenceofequality,becausethisisnota controlledvariable,sinceourswasanonprobabilisticsample. Abouttheoccupation,fivecategorieswerecited:20(66.7%) retirees,4(13.3%)pensioners,3(10.0%)ofdomesticchores,6 (6.7%)autonomousand1(3.3%)unemployed.Onreligion,only twocategorieswerementioned:Catholicismpractitioners,26 (86.7%)andEvangelicalChurchattendants,4(13.3%).
Itwasfoundthat15(50%)participantshadprimary edu-cation,16(53%)receiveduptothreeminimumwages,were marriedorlivinginastableunion.Themeanfamilyincome rangedfrom<1(1)to>5(5)timestheminimumwage,with
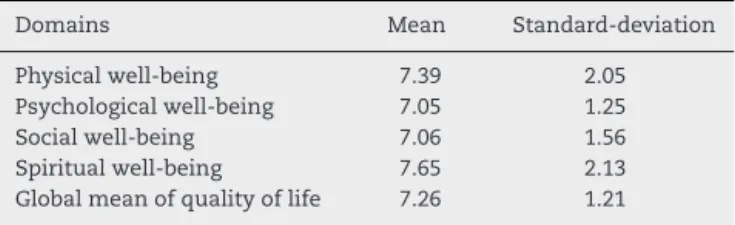
Table1–MeanofscoresforCityofHopeQuestionnaire domains.JoãoPessoa,Paraíba,2015(n=30).
Domains Mean Standard-deviation Physicalwell-being 7.39 2.05 Psychologicalwell-being 7.05 1.25 Socialwell-being 7.06 1.56 Spiritualwell-being 7.65 2.13 Globalmeanofqualityoflife 7.26 1.21
prevalenceofthe group from 1to3 salarieswith15 (50%) participants.
Clinicallyitwasobservedthatmostofsurgerieshada ther-apeuticindication,forthetreatmentofbowelcancer(24;80%). Ofthe30respondents,22(73%)hadapermanentstoma,27 (90%)showedaninadequatepositionofthestoma,13(44.8%) hadacolostomyforovertenyearsand24(80%)didnotpresent anykindofcomplication.WithregardtoBMI,15(50%)were overweightand13(43%)remainedwiththeirweightwithin normallimits.
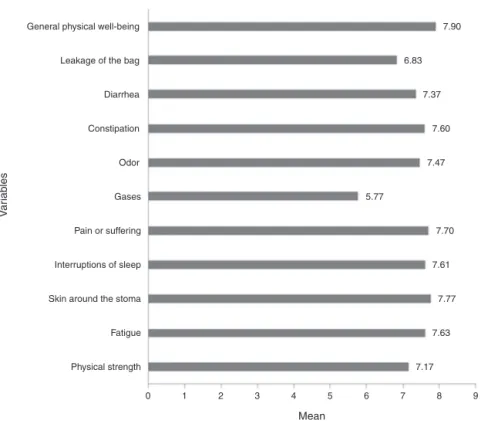
Consideringthe structureproposed bythe City ofHope questionnaire,wepresentedthemeansforeachdomainand fortheirvariables,aswellasthe totalscoreofQoLamong theparticipantsofthestudy.Onthebehaviorofvariablesof “physicalwell-being”domain,theoverallmeanwas7.39,and itwasobservedinitsvariablesthatthelowestmeanconcerns togases(5.77)andthehighestmeanrefersto“overallphysical well-being”(7.90)(Fig.1).
Forthedomain“socialwell-being”,theoverallmeanwas 7.06.Itisevidentthat, forthisdomain,alargernumberof variablesstaysclosertothemidpointofthescale(5);the low-est meanobtainedwasfor“interferencewiththe abilityto travel”(5.27)andthehighestmeanwasfor“privacyathome” (inrelationtothecareofthestoma)(8.93)(Fig.2).
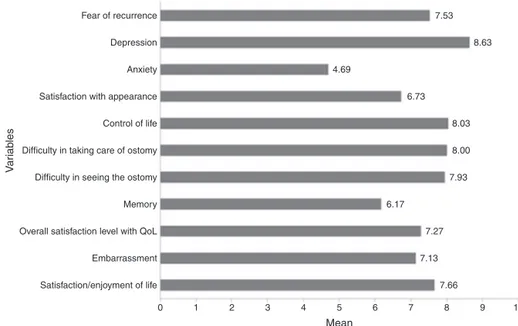
Thedomain“psychologicalwell-being”hadameanof7.05, andwastheonlydomainaveraging<5ononeofitsvariables (anxiety,4.69).“Depression”wasthevariablethatcontributed forthehighestmean(8.63)(Fig.3).
Fig.4depictsthemeanscoresofthevariablesthatmake upthedomain“spiritualwell-being”.Thelowestmean corre-spondstothe“uncertaintyaboutpersonalfuture”(5.30)and the highest mean refersto the variable “spiritual support” (8.83).
Byobservingthedistributionoftheoverallmeansforthe four domains of the questionnaire, it was found that the domainwiththebestscoresforqualityoflifecorresponded to“spiritualwell-being”(7.65),andthatthemeansobtained forthedomains“psychologicalwell-being”(7.05)and“social well-being”(7.05)hadthelowestmeans.Astothestandard deviationofthedomains“psychologicalwell-being”andsocial well-being”,agreaterhomogeneityamongthemeansofthe variablesthatmakeupthesedomainswasconfirmed,in com-parisonwithotherdomains,whichshowedgreatervariability
(Table1).
Discussion
General physical well-being
Leakage of the bag
Diarrhea
Constipation
V
ar
iab
les
Odor
Gases
Pain or suffering
Interruptions of sleep
Skin around the stoma
Fatigue
Physical strength
Mean
7.90
6.83
7.37
7.60
7.47
5.77
7.70
7.61
7.77
7.63
7.17
9 8 7 6 5 4 3 2 1 0
Fig.1–Meanscoresofthevariablesthatmakeupthephysicalwell-beingdomainoftheCityofHopequestionnaire.João Pessoa,2015,n=30(mean=7.39,SD=2.05).
physiologicalprocessofthebody,illnessesorchronic condi-tionstendtoaffectpeople.Inthecaseofcancer,althoughthis diseasedoesnotresultofphysiologicalaging,itisobserved that,withincreasingage,thereisahigherincidenceof cer-taintypesofcancers,distributedbetweengendersinaspecific way.Colonandrectalcanceroccursinbothgenders.15
Regarding gender, the factof beinga woman or aman didnotinfluencethefactofbeingacolostomizedsubject.In theliterature,somestudiesshowapredominanceofmales,16 whileinothersthereisafemalepredominance.11,17Thisfact relates to the diversity of the population and depends on theareasurveyed.Althoughsomeauthors18,19claimthatthe
V
ar
iab
les
Enough privacy
Privacy at home
Interference in intimacy
Interference in social activities
Interference with recreational activities/sports
Support from friends and family
Isolation caused by stoma
Interference in personal relationships
Interference with the ability to travel
Distressing for the family
Resultant financial burden
Difficulty in meeting people
6.03
8.93
7.40
6.97
6.10
8.27
7.73
7.93
5.27
5.73
5.77
8.70
Mean
0 1 2 3 4 5 6 7 8 9 10
V
ar
iab
les
Fear of recurrence
Depression
Anxiety
Satisfaction with appearance
Control of life
Difficulty in taking care of ostomy
Difficulty in seeing the ostomy
Memory
Overall satisfaction level with QoL
Embarrassment
Satisfaction/enjoyment of life
7.53
8.63
4.69
6.73
8.03
8.00
7.93
6.17
7.27
7.13
7.66
Mean
0 1 2 3 4 5 6 7 8 9 10
Fig.3–Meanscoresofthevariablesthatmakeupthepsychologicalwell-beingdomainoftheCityofHopequestionnaire. JoãoPessoa,2015,n=30(mean=7.05,SD=1.25).
genderinfluencesthesocialadaptationoftheostomized indi-vidual,emphasizingthatwomenaremoreresilientandbest suitedtonewhabits.
Asforworkingoccupation,ingeneralallworkers,after con-tributingtoSocialSecurity, acquiretheright toenjoytheir labor retirement. In addition, the permanent condition of colostomyguaranteesretirementtotheindividual affected. Inthis study,this relationshiphasnot beenverified. How-ever,a similarstudy identifiedpredominanceofretirees in colostomizedgroups.20
Consideringthereligious aspect,it ispossibletoensure thatthisfactorstrengthensfaithandconsolidatesvaluesand beliefs thatdirectly affect the quality oflifeofastomized person,favoring his/her rehabilitation.21 It isbelieved that religionisanimportantfactortoimprovehealth,by provid-ingspiritual support,regardlessofwhich religiouscreed is
followedbytheindividual,althoughinthepresentstudythe majorityofoursamplestatedtoprofessCatholicism(86.7%).
Withregardtoeducation,halfofthesamplestudiedonly uptoprimaryschool.Schoolingisarelevantaspectfor under-standingtheguidelinesforthecareofthestoma,thedevice forwastecollection,theregularmonitoringofhealth, nutri-tionandhygiene,aswellasthevariousconditionssettledfrom thesurgery.
Aboutmaritalstatus,itisassumedthatthefactthat53.4% of respondentsare married or ina stablerelationship can haveapositiveinfluenceonthe waythe ostomizedperson dealswithhis/hernewstateofhealth,thankstotheemotional supportofferedbyhis/herpartner.Regardingthisaspect,our studyconfirmsthatmanyoftheostomizedpeoplearemarried and livingwithhis/herspouse,but noassociationbetween resilienceandmaritalstatuswasproved.11,22
Positive changes
Religious support
Spiritual support
V
ar
iab
les
Hope
Inner peace
Reason to be alive
Uncertainty in future
Mean
0 1 2 3 4 5 6 7 8 9 10 6.60
7.50
8.83
7.87
8.80
8.67
5.30
Asformonthlyincome,itisknownthatthefinancial situa-tionmayinfluencethewayoflivingwithacolostomy,because thisstaterequiresspecialcareandtheacquisitionofmaterials thatburdenthefamilybudget.Astooursample,wefoundthat 50%livewithanincomeof1–3minimumwages.Theincome caninterferewiththe acquisition ofconsumablematerials relatedtoostomycare,reallyaffectingthequalityoflife.10
Withregardtotheclinicalcharacterization,most partici-pantsshowanimproperpositioningofthestomaandhigh bodymassindexes.Perhapsthesetwovariablesmaybelinked. However,itwasnotpossibletosaywhethertheinadequacyof thestomacomesfromweightgain(whichcollaborateswithan increaseofabdominalcircumference),orwhetherthis inade-quacyisaresultoflack/inadequacyinthedemarcationofthe stomaduringsurgery.Thisfindingonlywouldbepossibleif theassessmentwasperformedimmediatelyaftersurgeryand oftheedemaregression,commonlyoccurringpostoperatively, oraftersurgicalhealinghavebeenoccurred.
Mostoftheparticipantsdidnotpresent post-colostomy complications,and only10% reporteddermatitis.Thismay suggest that: the surgery was successful, the physicians conducted their guidelines efficiently, and/or the family care/self-carewasadequate.
Onthe permanenceofthe stoma, 73.3% ofparticipants claimed to have a permanent colostomy, which can be observedinotherstudies.3,23Withreferencetothereasonfor thesurgery,cancerhasbeen themostfrequentlycondition cited.Otherstudieshaveshowntheprevalenceofcolostomies inassociationwithcasesofcolorectalcancer.24–26
About colostomy time, mostparticipantsreported more than ten years of surgery. During the development ofthis study,itbecameclearthat,overtime,theseindividualshave founda parsimoniouswaytolive withtheir current state, thanks for their religious faith, the seemingly irreversible definitivecondition,orsimplyforthefactofbeingalive.This attitudeseemstocontributetoimprovingthequalityoflifeof theseindividuals.
Regardingthe domain“physicalwell-being,”itisknown that gases cause bloating, which can lead to viewing the prominencebelowthegarment,ortheaccidentaldetachment ofthebag.Therefore,flatulencecancausediscomfort,since theyare anuncontrollable phenomenon,and althoughthe non-externalizationoftheodor,thankstotheclosureofthe device,yetthesoundcausedbygasesmayresult embarras-singforostomypatientsorpersonswhowitnessthissituation. Thus, it ispossible that these reasons justify the smallest meanofthedomain,anditsclosestpositionwithrespectto themidpointofthescaleforthevariable“gases”(Fig.1).
Forthedomain“socialwell-being”,travelscanbeaform ofrecreation(Fig.2).However,the colostomyimplies some peculiarities,suchastheneedforaplaceandspecial materi-alsforcleaningthedevicebytheostomizedperson,aswellas theneedforprivacytoremovethecollectorbag,andlastbut notleast,thenuisancecausedbythecuriosityofother wit-nessespresent.Consideringallthat,implicationscanaccrue forhowostomizedpeopleperceiveandexperiencethesocial coexistence.
The social non-isolation is an imperative factor in the restorationofself-esteemofostomizedpeople.Social inter-actioncancontributetoovercomingthefeelingofmutilation,
as a network ofrelationships will provide distraction and momentsofjoy,favoringrecoveryandraisinghopesforthe continualseekingforabetterqualityoflife.27
Asforthedomain“psychologicalwell-being”,itisknown thatanxietyispartofthefieldofemotions,andthatitmay arise inneworunexpectedsituations.Thescorebelowthe midpoint5indicatesanegativeinterferenceinthequalityof lifeoftheparticipants,despitethefindingofameanofthe domainabove7,whichmaybeattributedtothevalueofthe othervariables’means,which,inthreecases,wassuperiorto 8(Fig.3).
Ontheotherhand,thecolostomycanbeseenasa“breath oflife”,ahopesignal,orasanewopportunityafterapainful diagnosisofcancer.Inthisstudy,itissuggestedthatthe rela-tionshipbetweenthecolostomytimeandthesadnessfeltby theostomizedindividualisinverselyproportional,thatis,over time,theindividualcangetusedtothecolostomy,not allow-inghim/herselftobedepressed,andneitherthatitinterferes withhis/herqualityoflife.
Onthissubject,astudyfoundthatfeelingsofdenialand depressionweremorefrequentintheearlystagesofthenew condition, becausethesadnesswascausedbythe shockof thechangeinbodyesthetics,orbytheseverityoftheclinical picture.Overtheyears,therewasadecreaseinthefrequency ofreportsoffeelingsofsadness.11
Regardingthedomain“spiritualwell-being”,itisbelieved thattheimpactcausedbyanegativediagnosiscanleadtofear ofdeath,frustrationaboutupcomingplans,anddoubtsasto theeventsoflife.
However,religiouspracticesmaybeimportantresources intheprocessofminimizationofthenegativeshockcaused bythestoma,forhelpinginthesubject’sfidelitytotreatment, reducingstress/anxiety,andinthesearchofameaningforthe newsituation.28,29
Thus,itisunderstandablethatthegrouphadobtaineda lowermeanforuncertaintyinthefuture,thankstothenature ofthediseaseanditstreatment;butneverthelessthesepeople showedgoodmeansforspiritualsupportandinnerpeace,as theseaspectsinteractwitheachother(Fig.4).
The resultsin Table 1indicate that, despitethe means above 7, some variables evaluated in the fields presented resultsclosetothemidpointoftherange,underwhichthe qualityoflifeisnotevaluatedatagoodlevel,whichisinline withstudies performed inTeresina,PI16 and Iran,30 whose meansandstandarddeviationsobtainedwere6.16(SD=2.83) and7.48(SD=0.9),respectively.
Thus,awatchfuleyetotheaspectswhichcancause dam-agetothequalityoflifeofstomizedpeopleiscritical,because in this way new perspectives may emerge and favor the proposition ofactions, be they educational or therapeutic, bydifferenthealthprofessionalsandinrelatedfields.These dimensionswouldculminateinimprovementsinaspectsthat revealedmorefragilityinthegroupstudied.
Conclusion
profile,astoqualityoflifescores.Infact,onecannothidethe physical,social,economic andpsychologicaldisorders that involve the process oflearning and livingwiththe stoma. Therefore,itiscriticaltostronglyemphasizetheimportance ofhealthteamsinallinstances,inordertoencourage inter-ventionsthatwillbeconvertedintovaluableimpulsesforthe lifeofostomizedpeople.
Weemphasizethe importanceofthe work ofthe team inchargeoftheserviceintheusers’care,stressingthatthe supportandhealth educationare unique waysinthe self-acceptanceprocess.Thelackoftelephonedataupdatinginthe sectorresearchedandthedifficultaccessthroughhousehold surveyswerelimitationsinthisstudy.Newresearchshould beencouraged,inorder toacquireadeeperunderstanding ofthe physical,psychologicaland spiritual conditionsthat functionassubsidiesfortheestablishmentofmoreeffective strategiesaimedatimprovingthequalityoflifeofstomized people.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SilvaRCL,FigueiredoNMA,MeirelesIB.Feridas:Fundamentos
eAtualizac¸õesemEnfermagem.In:2nded.revisadae
ampliada.SãoCaetanodoSul:Yendis;2009.p.211–36.
2. OliveiraG,MaritanCVC,MantovanelliC,RamalheiroGR,
GavilhiaTCA,PaulaAAD.Impactodaestomia:Sentimentose
habilidadesdesenvolvidosfrenteànovacondic¸ãodevida.
RevEstima.2010;8:18–24.
3. RamosRS,BarrosMD,SantosMM,GawryszewiskARB,Gomes
AMT.Operfildospacientesestomizadoscomdiagnóstico
primáriodecâncerderetoemacompanhamentoem
programadereabilitac¸ão.CadSaúdeColet.2012;20:
280–6.
4. Associac¸ãoBrasileiradeOstomizados(ABRASO).Quantitativo aproximadodePessoasOstomizadasnoBrasil[Internet]; 2014.Availableat:http://www.abraso.org.br/estatistica
ostomizados.htm[cited10.01.14].
5. ViolinRMI,SalesCA.Experiênciascotidianasdepessoas
colostomizadasporcâncer:enfoqueexistencial.RevEletrEnf.
2010;12:278–86.
6. SouzaPCM,CostaVRM,MaruyamaSAT,CostaALRC,
RodriguesAEC,NavarroJP.Asrepercussõesdevivercomuma
colostomiatemporárianoscorpos:individual,sociale
político.RevEletrEnf.2011;13:50–9.
7. EgidoA.Lapieltieneunacaracterísticasimbólicaporquees
dondeelcuerpoyelespírituse,unen.Gerokomos.
2011;22:43–5.
8. KimuraCA,KamadaI,GuilhemD,MonteiroPS.Qualityoflife
analysisinostomizedcolorectalcancerpatients.J
Coloproctol.2013;33:2237–9363.
9. AttoliniRC,GallonCW.Qualidadedevidaeperfilnutricional
depacientescomcâncercolorretalcolostomizados.J
Coloproctol.2010;30:289–98.
10.FernandesRM,MiguirELB,DonosoTV.Perfildaclientela
estomizadaresidentenomunicípiodePonteNova,Minas
Gerais.JColoproctol.2010;30:385–92.
11.SallesVJA,BeckerCPP,FariaGMR.Ainfluênciadotempona
qualidadedevidadopacienteportadordeestomiaintestinal.
JColoproctol.2014;34:73–5.
12.MahjoubiB,MirzaeiR,AziziR,JafariniaM,Zahedi-Shoolami
L.Across-sectionalsurveyofqualityoflifeincolostomates:a
reportfromIran.HealthQualLifeOutcomes.2012;10:01–6.
13.CityofHopeandBeckmanResearchInstitute.QualityofLife QuestionnaireforaPatientwithanOstomy[Internet];2013. Availablefrom:http://prc.coh.org/Ostomy-11.pdf
14.ConselhoNacionaldeSaúde(CNS).ComissãoNacionalde
ÉticaemPesquisa.Resoluc¸ãon◦466,de12dedezembrode
2012:Sobreasdiretrizesenormasregulamentadorasde
pesquisaenvolvendosereshumanos.Brasília(DF);2012.
15.InstitutoNacionaldoCâncer(INCA).Estimativasda
incidênciaemortalidadeporcâncernoBrasil[Internet];2012. Availableat:http://bvsms.saude.gov.br/bvs/publicacoes/
acoesenfermagemcontrolecancer.pdf[cited15.05.15].
16.TorresCRD,Dissertac¸ão[MestradoemEnfermagem]
Qualidadedevidadepessoascomestomasdeeliminac¸ão
intestinal.Teresina:UniversidadeFederaldoPiauí;2013.
17.SouzaAPMA,SantosIBC,SoaresMJGO,SantanaIO.Clinical
epidemiologicalprofileofpatientsseenandenumeratedin
TheCenterParaibanoofOstomizedJoäoPessoa(Brasil).
Gerokomos.2010;21:183–90.
18.KrouseRS,GrantM,RawlSM,MohlerMJ,BaldwinCM,Coons
SJ,etal.Copingandacceptance:thegreatestchallengefor
veteranswithintestinalstomas.JPsychosomRes.
2009;66:227–33.
19.GrantM,McMullenCK,AltschulerA,MohlerMJ,Hornbrook
MC,HerrintonLJ,etal.Genderdifferencesinqualityoflife
amonglong-termcolorectalcancersurvivorswithostomies.
OncolNursForum.2011;38:587–96.
20.MauricioVC,SouzaNDVO,LisboaMTL.Determinantes
biopsicossociaisdoprocessodeinclusãolaboraldapessoa
estomizada.RevBrasEnferm.2014;67:415–21.
21.LuzMHBA,AndradeDS,AmaralHO,BezerraSMG,Benício
CDAV,LealACA.Caracterizac¸ãodospacientessubmetidosa
estomasIntestinaisemumhospitalpúblicodeTeresina-PI.
TextoContextoEnferm.2009;18:140–6.
22.FortesRC,MonteiroTMRC,KimuraCA.Qualityoflifefrom
oncologicalpatientswithdefinitiveandtemporary
colostomy.JColoproctol.2012;32:253–9.
23.StummEMF,OliveiraERA,KirschnerRM.Perfildepacientes
ostomizados.SciMed.2008;18:26–30.
24.MelottiLF,BuenoIM,SilveiraGV,SilvaMEN,FedosseE.
Characterizationofpatientswithostomytreatedatapublic
municipalandregionalreferencecenter.JColoproctol.
2013;33:70–4.
25.SasakiVDM,PereiraAPS,FerreiraAM,PintoMH,GomesJRJ.
Healthcareserviceforostomypatients:profileofthe
clientele.JColoproctol.2012;32:232–9.
26.SantosAC,MartinsLLT,BrasilAMS,PintoAS,NetoLG,
OliveiraEC.Emergencysurgeryforcomplicatedcolorectal
cancerincentralBrazil.JColoproctol.2014;34:104–8.
27.GladinoYLS,CastroME,PereiraMLD,LimaSSO,SilvaFAA,
GuedesMVC.Ocotidianodapessoaestomizadafrenteàs
necessidadeshumanasbásicasalteradas.RevEstima.
2012;10:22–31.
28.GamboaNSG,AlvarezLST.Cuidadodeunhijoostomizado:
cambiosenlafamilia.AvEnferm.2013;31:59–71.
29.AlmeidaSSL,RezendeAM,SchallVT,ModenaCM.Os
sentidosdacorporeidadeemostomizadosporcâncer.Psicol
Estud.2011;15:761–9.
30.AnarakiA,VafaieM,BehbooR,MaghsoodiN,EsmaeilpourS,
SafaeeA.Qualityoflifeoutcomesinpatientslivingwith