w w w . e l s e v ie r . c o m / l o c a t e / b j i d
The
Brazilian
Journal
of
INFECTIOUS
DISEASES
Brief
communication
Early-onset
neonatal
sepsis
and
the
implementation
of
group
B
streptococcus
prophylaxis
in
a
Brazilian
maternity
hospital:
a
descriptive
study
Felipe
Teixeira
de
Mello
Freitas
a,b,∗,
Gustavo
Adolfo
Sierra
Romero
b aSecretariadeEstadodeSaúdedoDistritoFederal,HospitalMaternoInfantildeBrasília,Brasília,DF,Brazil bUniversidadedeBrasília,NúcleodeMedicinaTropical,Brasília,DF,Brazila
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received4May2016 Accepted30September2016 Availableonline19November2016
Keywords: Neonatalsepsis
GroupBstreptococcaldisease Escherichiacoliinfection Brazil
a
b
s
t
r
a
c
t
Objectives:Todescribeearly-onsetneonatalsepsis(EOS)epidemiologyinapublicmaternity hospitalinBrasilia,Brazil.
Methods:WedefinedEOSasapositivebloodcultureresultobtainedfrominfantsaged≤72 hoursoflifeplustreatmentwithantibiotictherapyfor≥5days.Incidencewascalculated basedonthenumberofcasesandtotallivebirths(LB).Thisisadescriptivestudycomparing theperiodof2012–2013withtheperiodof2014–September2015,beforeandafter implemen-tationofantibioticprophylaxisduringlaborforgroupBstreptococcus(GBS)prevention, respectively.
Results:Overall,36infantsdevelopedEOSamong21,219LB(1.7casesper1000LB)and16died (casefatalityrateof44%).From2014,305vaginal-rectalswabswerecollectedfromhigh-risk womenand74(24%)turnedoutpositiveforGBS.AfterimplementationofGBSprevention guidelines,nonewcasesofGBSweredetected,andtheEOSincidencewasreducedfrom1.9 (95%CI1.3–2.8)to1.3(95%CI0.7–2.3)casesper1000LBfrom2012–2013to2014–September 2015(p=0.32).
Conclusions:AlthoughthereductionofEOSincidencewasnotsignificant,GBScolonization amongpregnantwomenwashigh,nocasesofneonatalGBShaveoccurredafter implemen-tationofpreventionguidelines.
©2016SociedadeBrasileiradeInfectologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/ by-nc-nd/4.0/).
Introduction
Early-onsetsepsis(EOS)inneonatesisafeared andsevere complicationwithhighfatalityrates.Indevelopedcountries,
∗ Correspondingauthor.
E-mailaddress:[email protected](F.T.Freitas).
theepidemiologyofEOShasbeenwelldescribedwith Strepto-coccusagalactiae,alsoreferredasgroupBstreptococcus(GBS), andEscherichiacoliresponsibleformostoftheseverecases.1,2 Additionally, preventionstrategiesbased on GBS screening andintrapartumantibioticprophylaxis(IAP)toreducevertical
http://dx.doi.org/10.1016/j.bjid.2016.09.013
1413-8670/©2016SociedadeBrasileiradeInfectologia.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
transmission of invasive GBS infection have been imple-mented for morethan a decade.3,4 As aconsequence, the incidenceofGBSinfectionintheUnitedStateswasreduced from1.7casesper1000livebirthsintheearly1990sto0.34 casesper1000livebirthsaftertheimplementationof antibi-oticprophylaxisduringlabor.3
Nevertheless, the epidemiology of EOS has rarely been describedindevelopingcountries,includingBrazil.One Brazil-ianstudy,publishedmorethanadecadeago,describedGBS asthepathogenresponsiblefor50%ofculture-provenEOS.5 TheincidenceofGBSinfectionsinBrazilhasrangedfrom0.39 and1.0per1000livebirths.6–9 TheuseofIAPhasnotbeen adoptedasanationalstrategytopreventGBSdisease,andno dataconcerningtheimpactofIAPhavebeenpublishedinthe country.
Therefore,wepresentEOSdatafromourhospital,which isthelargestpublicmaternityhospitalinBrasilia,Brazil.We haveimplementedGBSscreeningandrisk-basedIAPin2014, andhereinwecomparetheepidemiologyofEOSintheperiods beforeandaftertheimplementationofIAP.
Methods
SettingsandGBSprophylaxisprotocol
OurhospitalisthelargestpublicmaternityhospitalinBrasilia, centralBrazil.Itisaregionalreferralcenterforpreterm-births andneonatalsurgery;ithasa30-bedneonatalintensivecare unit(NICU)andanintermediatecareunitwith16beds.Before 2014,therewasnopolicyforGBSscreeningandprophylaxis. IAPwas implementedinJanuary2014, basedon the latest CentersforDiseaseControlandPrevention(CDC)guidelines,3 andconsistedofaprotocolthatinstructedthecollectionof avaginal-rectalswabforGBSscreeningforeverywoman≥24 weeksofpregnancyadmittedtothehospitalwithpremature labororprematureruptureofmembranes.Additionally,it rec-ommendedIAPfor(1)everywomanwithapositiveGBSswab; (2)every woman, regardlessofswabresult,withapositive urinecultureforGBSanytimeduringpregnancy,orwitha his-toryofapreviouschildwithGBSsepsis;and(3)everywoman withanunknownGBScolonizationstatus,whowasinlabor <37weeksofpregnancyor≥18hofruptureofmembranesor withfever(temperature≥38◦C)duringlabor(Fig.1).Itis impor-tanttonotethatGBSscreeningduringprenatalcarewasnota policyandthatthevastmajorityofwomenhadanunknown GBSstatuscolonizationuponarrivalatthematernityhospital. Theswabwas collected and immediately placedbythe assistant physician in the Todd-Hewitt broth, a selective enrichmentbrothusedtoidentifyGBS,andthenforwardedto themicrobiologylaboratory.Afterenrichment,GBSwas iso-latedbysubculturesonbloodagarplateswithCAMP-disktest forpresumptiveidentification.
Infant blood cultures were submitted to an automated continuousmonitoringsystemforbacterialdetection(Bactec fluorescent series system® Becton Dickinson Microbiology System). Then, anautomated panel ofbacterial identifica-tion(MicroScanWalk-Away® DadeBehringInc.)wasusedto identifybacteriaspeciesandperformantimicrobial suscep-tibilitytest.ThelaboratoryusedtheClinicalandLaboratory
StandardsInstitute(CLSI)manualforinterpretationof mini-muminhibitoryconcentrations(MIC).10
Datacollectionandstatisticalanalysis
Weobtainedthepositivebloodculturedatafromthe micro-biologylaboratorydatabasefortheperiodofJanuary2012to September2015.Similarly,thenumberofvaginal-rectalswabs collected inthematernity hospitaland theirpositivityrate aftertheimplementationoftheprotocol,fromJanuary2014 toSeptember2015werealsoabstracted.
EOS was defined asisolation ofa pathogen from blood culture samples drawn within 72h ofbirth plus antibiotic treatmentfor≥5daysordeath<5dayswhileonantibiotic treatment. Coagulase-negative staphylococci (CoNS) grown aloneinasingleculturebottlewereconsideredcontaminants. Patients’ records were reviewed, and maternal and infantinformationwascollected.Thematernalinformation includedgestationalage,timeofruptureofmembranes, pres-enceofintrapartumfever,diagnosisofchorioamnionitis,type of delivery, statusof GBS colonization, IAPtreatment, and antibioticsreceived.Theinfants’informationincludeddateof birth,dateofNICUadmission,sex,birthweight,andoutcome (death or discharge from hospital).Antibiotic susceptibility datawereanalyzed,ifavailable.
The incidenceofEOS was calculated using the number ofEOSdividedbythenumbersoflivebirths(LB)duringthe periodofstudy.Weanalyzedthedatadescriptively,using pro-portionsfordiscretevariablesandthemedianforcontinuous variables.Thedatawereexaminedoverallandbetweentwo periods:before(2012and2013)andafter(2014and2015)the implementationoftheGBSpreventionprotocol.Weused Chi-squaretestanda95%confidenceinterval(95%CI)tocompare theEOSincidenceratesbetweenthesetwoperiods.Wealso compareddatabetweeninfantsinfectedwithGBSandE.coli.
Results
Pathogensandinfectionrates
During2012–2013,therewere26casesofEOSand13,627LB, anincidenceof1.9per 1000LB(95% CI1.3–2.8); 12infants died,afatalityrateof46%.During2014–September2015,there were 10 casesofEOS and7592LB, anincidence of1.3per 1000LB(95%CI0.7–2.3);4infantsdied,afatalityrateof40%. Thus,forthewholeperiodofstudytherewere36casesofEOS and 21,219LB, anincidenceofEOSof1.7per1000LB(95% CI1.2–2.3),andatotalof16deaths,anoverallfatalityrateof 44%.Therewasnosignificantdifferenceintheincidenceof EOSbetweenthetwoperiods(p=0.32).
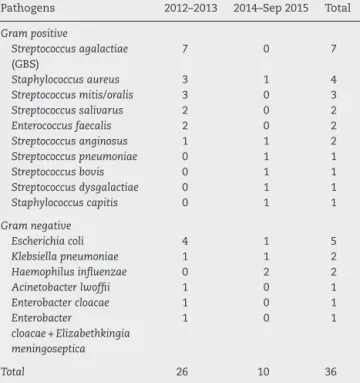
Thedistribution ofpathogens isolated during thestudy periodispresentedinTable1.GBSwasthemainpathogen isolated from 36 infants, but remarkably no new cases of GBS have been isolated since the implementation of IAP. E.coliwasthesecondmostfrequentlyisolatedpathogen, fol-lowedbyStaphylococcusaureus,otherStreptococcusspecies,and EnterococcusfaecalisamongGrampositivebacteriaandother entericbacilliand HaemophilusinfluenzaamongGram nega-tivebacteria.Therewasonlyoneinfantwithmorethanone
Obtain vaginal-rectal swab for GBS screening for every women ≥24 weeks of pregnancy, upon arrival at the maternity hospital with preterm labor or with premature rupture of membranes
Intrapartum GBS prophylaxis indicated
- Previous infant with invasive GBS disease- GBS bacteriuria during any trimester of the current pregnancy
- Positive GBS vaginal-rectal screening culture in late gestation during current pregnancy
- Unknown GBS status at the onset of labor (culture not done, incomplete, or results unknown) and any of the following:
- Delivery at < 37 weeks’ gestation - Amniotic membrane rupture ≥18 hours - Intrapartum temperature ≥38.0°C
Intrapartum antibiotic prophylaxis during labor
- Penicillin G, 5 million units IV initial dose, then 2,5 - 3 million units IV every 4 hours until delivery
OR
- Ampicillin, 2 g IV initial dose, then 1 g IV every 4 hours until delivery
If patient has a history of allergy (anaphylaxis, angioedema, respiratory distress or urticaria) after receiving penicillin or a cephalosporin
- Clindamycin 900mg IV every 8 hours until delivery
Intrapartum GBS prophylaxis not indicated
- Negative vaginal-rectal GBS screening culture during the current pregnancy, regardless of intrapartum risk factors
- Cesarean delivery performed before onset of labor on a woman with intact amniotic membranes, regardless of GBS colonization status or gestational age
Observations
- A negative GBS screen is considered valid for 5 weeks, after this time, repeat screening if the women has not delivered
- If the women is receiving ampicillin and/or clindamycin for presumed
chorioamnionitis or premature rupture of membranes during labor, she does not need additional antibiotic
Fig.1–GroupBstreptococcalcolonizationscreeninganduseofintrapartumantibioticprophylaxisprotocolforwomenwith pretermlabororprematureruptureofmembranes,Brasilia,Brazil.
Table1–Distributionofpathogensisolatedfrom early-onsetneonatalsepsisduring2012–2013and 2014–September2015,Brasilia,Brazil.
Pathogens 2012–2013 2014–Sep2015 Total
Grampositive Streptococcusagalactiae (GBS) 7 0 7 Staphylococcusaureus 3 1 4 Streptococcusmitis/oralis 3 0 3 Streptococcussalivarus 2 0 2 Enterococcusfaecalis 2 0 2 Streptococcusanginosus 1 1 2 Streptococcuspneumoniae 0 1 1 Streptococcusbovis 0 1 1 Streptococcusdysgalactiae 0 1 1 Staphylococcuscapitis 0 1 1 Gramnegative Escherichiacoli 4 1 5 Klebsiellapneumoniae 1 1 2 Haemophilusinfluenzae 0 2 2 Acinetobacterlwoffii 1 0 1 Enterobactercloacae 1 0 1 Enterobacter cloacae+Elizabethkingia meningoseptica 1 0 1 Total 26 10 36
microorganismgrowninculture.Therewere12bloodcultures withCoNS,butonlyoneincludedastheremainingwere con-sideredcontaminants.
AllsevenGBSisolatesweresensitivetopenicillin, ampi-cillin,andvancomycin;theywerenottestedforclindamycin susceptibility.AllfiveE.coliisolateswereresistantto ampi-cillinand sensitivetothirdgeneration cephalosporins;one isolatewasgentamicinresistant.NoS.aureuswasmethicillin resistantandnoE.faecaliswasvancomycinresistant.
Maternalandneonatalclinicalfeatures
All36infantsdevelopedsymptomaticillness(requiredblood pressuresupportorhad respiratorydistress) ofEOS during theperiodofstudy;allreceivedampicillin,penicillin,or cefa-zolinwithgentamicin.Eighteen(50%)weremaleand19(53%) werebornthroughvaginaldelivery.Twenty-nine(81%)were preterm(<37weeksofgestation);themediangestationalage was31weeks(24–41weeks).Twenty-one(58%)were≤1500g; themedianbirthweightwas1307.5g(470–3800g).
Eighteen (50%) pregnant women had rupture of mem-branes atdelivery.For the other 18pregnant women, with ruptureofmembranesbeforedelivery,themediandurationof membranerupturewas72h(1hto42days).Overall,14(39%) hadaperiodofruptureofmembraneslongerthan18h.Seven (19%)pregnantwomenhadfeveroradiagnosisofpresumed chorioamnionitisduringlabor.
ImplementationofGBSprophylaxis
During2012–2013,amongthe26pregnantwomenwhohad aninfantwithEOS,noneofthewomenhadavaginal-rectal swab result at labor. According to the latest guidelines,3,4 whenconsideringthe unknownstatusofGBScolonization,
21 (81%) womenmet the criteria forreceiving IAP (12 had premature labor; six had premature labor and rupture of membranes≥18h;twohadprematurelabor,ruptureof mem-branes≥18handfeverduringlabor;andonehadtermlabor andruptureofmembrane≥18h).However,onlythree(11%) womenreceivedantibioticsduringlabor:twowomenreceived clindamycinbecauseofpresumedchorioamnionitis,andone receivedampicillin andazithromycin forprolonged prema-tureruptureofmembranes.
From2014,theIAPprotocolwasimplemented,anduntil September2015,305vaginal-rectalswabswerecollectedfrom womenadmittedwithpretermlaborand74(24%)were posi-tive.Outof10pregnantwomenwhohadaninfantwithEOS, onlyonehadavaginal-rectalswabcollectedthatturnedout negative.However,theresultwasknownafterdelivery.Only onewomanhad atermlaborwithunknownGBS coloniza-tion status, no riskfactors forEOSand thus, didnothave indicationsforIAP.Therefore,nine(90%)womenshouldhave receivedIAP,accordingtotheprotocol(threehadpremature labor; onehad prematurelaborand ruptureofmembranes ≥18h;fourhadprematurelabor,ruptureofmembranes≥18h and fever during labor; and one had premature labor and feverduringlabor);however,onlyfive(55.5%)received antibi-oticsduringlabor: four receivedclindamycinforpresumed chorioamnionitis,andonereceivedampicillinasprophylaxis, accordingtoprotocol,becauseshehadapretermlaborand ruptureofmembranes≥18h.
GroupBStreptococcusandE.coli
ThetotalnumberofinfantswithGBSinfectionwassevenwith anincidencerateofinfectionduring2012–2013was0.51per 1000LBor0.33per1000LBforthewholeperiodofstudy.No caseofEOSduetoGBSwasdetectedafterthe implementa-tionoftheIAPprotocol.Four(57%)infantswerepreterm;the medianbirthweightamongGBSinfectedinfantswas2751g (569–3800g).Threeinfantsdied,afatalityrateof43%.
ThetotalnumberofinfantswithE.coliinfectionwasfive withanincidencerateofinfectionwithE.coliwas0.23per1000 LBduringthewholeperiodofstudy.Allinfantswerepreterm; themedianbirthweightamonginfantsinfectedwithE.coli was1270g(855–2020g).Fourinfantsdied,afatalityrateof80%.
Discussion
ThisanalysisofaregionalreferralmaternityhospitalinBrazil withapproximately20,000LBshowsthattheburdenofEOSis concentratedamongpreterminfants.Theincidencedensity ofcultureprovenEOSwas1.7casesper1000LBandthefatality ratewas44%,figuresthatarehigherthanthoseobservedin developedcountries.EOSincidencedensitywas0.98per1000 LBintheUnitedStates2and0.9per1000LBinEngland.11
GBS and E. coli have been the predominant causative microorganismsofEOS,butinthisstudyitcorrespondedto onlyathirdofcasesand almost onehalfofdeaths.Other microorganisms,especiallyGrampositivebacteria,suchasS. aureus,otherStreptococcusspecies,andE.faecaliscorresponded toasignificantshareofcasesofEOSinourstudy.Although Staphylococcus and other Streptococcusspeciesareviewed as
possiblecontaminants,alltheinfantswhohadbloodcultures withthesepathogens,presentedclinical orlaboratory find-ingssuggestiveofinfection andreceivedantibiotics.Asthe importanceofCoNSasanEOSpathogenremains controver-sial,weonlyconsideredCoNSasthecauseofEOSinthecaseof oneinfantwhohadmorethanoneculturegrowingCoNS.Itis worthytonotethattherewasnocaseofListeriamonocytogenes. ThestrategyofIAPindevelopedcountrieshasreducedthe incidenceofEOSbyreducingthecasesofGBS.Theincidenceof GBSinourstudy(0.51per1000LB),beforetheimplementation ofIAP,iswithintherangeofpreviousBrazilianstudies,6–9but higherthantheincidenceobservedindevelopedcountries, morethan adecadeafterIAPimplementation.3,4 Wefound a positive vaginal-rectal swab prevalence of 24%. This is similar tothe range observed inother Brazilian studies of 17.9–27.6%12–14 and the prevalenceof 26% observed inthe UnitedStates.15 Despitethishighrateofwomenwith colo-nization,screeningofGBSduringprenatalcareandIAPduring laborisnotanationalpolicyinBrazil.Duringtheperiodof study,morethan80%ofwomenwhohadaninfantwithEOS shouldhavereceived IAP,according tothelatestAmerican andEuropeanguidelines,3,4 but only11%ofwomenduring 2012–2013and55.5%ofwomenduring2014–September2015, respectively,receivedIAP. Thesewere missedopportunities forGBSprophylaxisingeneral,andforpretermlaborin par-ticular;antibioticsweremorelikelytohavebeenprescribed whenthere wasapresumed diagnosis ofchorioamnionitis oralongperiodofmembranerupture.ABrazilianstudyhad alreadyrevealeda57%inappropriatecompliancewiththeIAP protocol.16Nevertheless,weobserved18monthsfollowingthe implementationoftheIAPprotocol,nonewcasesofGBShave appeared,andthecrudeEOSincidencehasbeenreduced.
Therationalchoiceofantibioticsfortheinfantwith pre-sumedinfection requires review ofantibioticsusceptibility ofthe predominant organismsthat cause the disease at a locallevel.Ampicillinandgentamicinaretherecommended empiricantibioticsfortheinfantatriskofEOS.Inourstudy,all theGBSweresensitivetoampicillinorpenicillin,butoneout offiveE.coliinfectionswasresistanttogentamicin.This find-ingisworrisomebecausepreviousstudieshavealreadyshown thatE.colihasbecomethemostfrequentpathogen among preterminfants,whoareatthehighestriskofseveredisease anddeath.17–19 TheincidenceofE.coli(0.23per1000LB)in ourstudyisveryclosetothatobservedintheUnitedStates (0.28per1000LB).2Themedianbirthweightofinfantsinfected withE.coliwaslowerthanthatobservedininfantsinfected withGBS,withahigherfatalityrate.Data from developing countrieshave alreadyreported 13% gentamicinresistance amongE.colineonatalinfections.20
Amonglimitationsofthepresentstudy,itdidnothavean uninfectedcomparisongrouptoassessriskfactorsandGBS preventionstrategiesmorebroadly.Additionally, wehavea relativesmallsamplesizeforanunusualoutcome, culture-provenEOS,andashortperiodoftimeafterimplementation ofIAPstrategy.Thesefactorsmayexplainwhywedidnotfind asignificantdifferencebetweentheEOSincidencesforthetwo periodsofstudy.Moreover,ourresultsareecologicalfindings, anditisnotpossibletoaffirmthatthereductioninGBS infec-tionswascausedonlybytheIAPprotocol.Wealsohadlimited externalvaliditybecausethisstudywascarriedoutinonly
one singleregional maternity hospital.Different situations mayexistinBrazilbecauseitissuchadiversecountry.Larger studies,includingmultiplecenters,longertimeperiods,and adifferent designcontrollingforconfounding variables are necessarytobetterdescribetheepidemiologyofEOSandto evaluatetheimpactofIAPstrategyinBrazil.
Inconclusion,EOSincidenceinthestudiedscenarioseems higherthanthatobservedindevelopedcountries.EOSis con-centrated among preterm infants and GBS and E. coli are themainpathogensofneonatalinfection.Althoughwedid notfindasignificantdifferenceinEOSincidencebeforeand aftertheimplementationofIAPinourhospital,theEOS inci-dencewasreducedandnonewcasesofGBSwereobserved. Evidence-basedstrategiestoreducetheburdenofEOSshould beimplemented,alongwitheffortstodecreasepretermbirth rates and toreduce the number ofdeathsassociatedwith theseinfections.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Wethankthehospitalmicrobiologylaboratoryforproviding theculturedataandtheobstetricandNICUstafffor suppor-tingtheimplementationofaGBSpreventionprotocol.
r
e
f
e
r
e
n
c
e
s
1.LeDoareK,HeathPT.AnoverviewofglobalGBS epidemiology.Vaccine.2013;31S:D7–12.
2.StollBJ,HansenNI,SánchezPJ,etal.Earlyonsetneonatal sepsis:theburdenofgroupBstreptococcalandE.colidisease continues.Pediatrics.2011;127:817–26.
3.VeraniJR,McGeeL,SchragSJ,DivisionofBacterialDiseases, NationalCenterforImmunizationandRespiratoryDiseases CentersforDiseaseControlandPrevention(CDC).Prevention ofperinatalgroupBstreptococcaldisease–revisedguidelines fromCDC,2010.MMWRRecommRep.2010;59:1–36.
4.DiRenzoGC,MelinP,BerardiA,etal.IntrapartumGBS screeningandantibioticprophylaxis:aEuropeanconsensus conference.JMaternFetalNeonatalMed.2015;28:766–82. 5.Pessoa-SilvaCL,RichtmannR,CalilR,etal.
Healthcare-associatedinfectionsamongneonatesinBrazil. InfectControlHospEpidemiol.2004;25:772–7.
6.MiuraE,MartinMC.GroupBstreptococcalneonatal infectionsinRioGrandedoSul,Brazil.RevInstMedTropSao Paulo.2001;43:243–6.
7.VacilotoE,RichtmannR,dePaulaFiodCostaH,KusanoEJ,de AlmeidaMF,AmaroER.Asurveyoftheincidenceofneonatal sepsisbyGroupBStreptococcusduringadecadeinaBrazilian maternityhospital.BrazJInfectDis.2002;6:55–62.
8.FioloK,ZanardiCE,SalvadegoM,etal.Infectionrateand
Streptococcusagalactiaeserotypesinsamplesofinfected neonatesinthecityofCampinas(SãoPaulo),Brazil.RevBras GinecolObstet.2012;34:544–9.
9.EvangelistaML,FreitasFT.GroupBStreptococcusneonatal infectioninanintensivecareunitinBrazil:highfatalityand missedopportunitiesforantibioticprophylaxis.BrazJInfect Dis.2015;19:98–9.
10.CLSI.PerformanceStandardsforAntimicrobialSusceptibility Testing;Twenty-ThirdInformationalSupplement.CLSI documentM100-S23.Wayne,PA:ClinicalandLaboratory StandardsInstitute;2013.
11.VergnanoS,MensonE,KenneaN,etal.Neonatalinfectionsin England:theNeonINsurveillancenetwork.ArchDisChild FetalNeonatalEd.2011;96:F9–14.
12.ZusmanAS,BaltimoreRS,FonsecaSN.Prevalenceofmaternal groupBstreptococcalcolonizationandrelatedriskfactorsin aBrazilianpopulation.BrazJInfectDis.2006;10:242–6. 13.CostaAL,LamyFilhoF,CheinMB,BritoLM,LamyZC,Andrade
KL.[PrevalenceofcolonizationbygroupBStreptococcusin pregnantwomenfromapublicmaternityofNorthwest regionofBrazil].RevBrasGinecolObstet.2008;30:274–80. 14.NomuraML,PassiniJúniorR,OliveiraUM,CalilR.[GroupB
Streptococcusmaternalandneonatalcolonizationinpreterm ruptureofmembranesandpretermlabor].RevBrasGinecol Obstet.2009;31:397–403.
15.CampbellJR,HillierSL,KrohnMA,FerrieriP,ZaleznikDF, BakerCJ.GroupBstreptococcalcolonizationand
serotype-specificimmunityinpregnantwomenatdelivery. ObstetGynecol.2000;96:498–503.
16.CostaNDL,CarvalhoM,PoneSM,JúniorSCG.Beta-hemolytic
Streptococcusinpregnantwomenandtheirnewborninfants:a criticalanalysisoftheprotocolusedatFernandesFigueira Institute,OswaldoCruzFoundation,inBrazil.RevPaul Pediatr.2010;28:155–61.
17.StollBJ,HansenN,FanaroffAA,etal.Changesinpathogens causingearly-onsetsepsisinvery-low-birth-weightinfants.N EnglJMed.2002;347:240–7.
18.BizzarroMJ,DembryLM,BaltimoreRS,GallagherPG. ChangingpatternsinneonatalEscherichiacolisepsisand ampicillinresistanceintheeraofintrapartumantibiotic prophylaxis.Pediatrics.2008;121:689–96.
19.StollBJ,HansenNI,HigginsRD,etal.Verylowbirthweight preterminfantswithearlyonsetneonatalsepsis:the predominanceofgram-negativeinfectionscontinuesinthe NationalInstituteofChildHealthandHumanDevelopment NeonatalResearchNetwork,2002–2003.PediatrInfectDisJ. 2005;24:635–9.
20.ThaverD,AliSA,ZaidiAK.Antimicrobialresistanceamong neonatalpathogensindevelopingcountries.PediatrInfect DisJ.2009;28:S19–21.