Faculdade de Motricidade Humana
Biomechanical and morphological adaptations in women during
pregnancy and the postpartum period in walking
Tese elaborada com vista à obtenção do Grau de Doutor em Motricidade Humana, na especialidade de Biomecânica
Tese por compilação de artigos, realizada ao abrigo da alínea a) do nº2 do artº 31º do Decreto-Lei nº 230/2009
Orientadora: Professora Doutora Rita Alexandra Prior Falhas Santos Rocha, Professora
Coordenadora, Escola Superior de Desporto de Rio Maior do Instituto Politécnico de Santarém
Coorientadora: Professora Doutora Maria Filomena Soares Vieira, Professora Auxiliar, Faculdade de Motricidade Humana da Universidade de Lisboa
Júri: Presidente:
Reitor da Universidade de Lisboa Vogais:
Doutor António Prieto Veloso, Professor Catedrático, Faculdade de Motricidade Humana da Universidade de Lisboa
Doutor Renato Manuel Natal Jorge, Professor Associado com Agregação, Faculdade de Engenharia da Universidade do Porto
Doutora Rita Alexandra Prior Falhas Santos Rocha, Professora Coordenadora, Escola Superior de Desporto de Rio Maior do Instituto Politécnico de Santarém
Doutora Filipa Manuel Alves Machado de Sousa, Professora Auxiliar, Faculdade de Desporto da Universidade do Porto
Doutor Augusto Gil Brites de Andrade Pascoal, Professor Auxiliar, Faculdade de Motricidade Humana da Universidade de Lisboa
Marco António Colaço Branco
III
DECLARAÇÃO Nome: Marco António Colaço Branco
Endereço eletrónico: marcobranco@esdrm.ipsantarem.pt Telefone: 967987322 Número do Bilhete de Identidade/Cartão de Cidadão: 11300903
Título da Tese: Biomechanical and morphological adaptations in women during pregnancy and the postpartum period in walking
Orientadoras: Doutora Rita Alexandra Prior Falhas Santos Rocha, Doutora Maria Filomena Soares Vieira
Ano de conclusão: 2016
Designação do ramo de conhecimento do Doutoramento: Biomecânica
Nos exemplares das teses de doutoramento entregues para a prestação de provas na Universidade e dos quais é obrigatoriamente enviado um exemplar para depósito legal na Biblioteca Nacional e pelo menos outro para a Biblioteca da FMH/UL deve constar uma das seguintes declarações:
1. É AUTORIZADA A REPRODUÇÃO INTEGRAL DESTA TESE/TRABALHO APENAS PARA EFEITOS DE INVESTIGAÇÃO, MEDIANTE DECLARAÇÃO ESCRITA DO INTERESSADO, QUE A TAL SE COMPROMETE.
2. É AUTORIZADA A REPRODUÇÃO PARCIAL DESTA TESE/TRABALHO (indicar, caso tal seja necessário, nº máximo de páginas, ilustrações, gráficos, etc.) APENAS PARA EFEITOS DE INVESTIGAÇÃO, MEDIANTE DECLARAÇÃO ESCRITA DO INTERESSADO, QUE A TAL SE COMPROMETE.
3. DE ACORDO COM A LEGISLAÇÃO EM VIGOR, (indicar, caso tal seja necessário, nº máximo de páginas, ilustrações, gráficos, etc.) NÃO É PERMITIDA A REPRODUÇÃO DE QUALQUER PARTE DESTA TESE/TRABALHO.
Faculdade de Motricidade Humana – Universidade de Lisboa, 10 de fevereiro de 2016
Assinatura:
V
DEDICATÓRIA:
VII
A realização deste trabalho deve-se ao esforço de um conjunto de pessoas às quais quero manifestar o meu profundo apreço.
Em primeiro lugar, quero agradecer à minha orientadora Professora Doutora
Rita Santos Rocha, por me ter acompanhado desde o início da minha vida
académica, não só participando ativamente no meu enriquecimento científico, mas também por me ter proporcionado diversas oportunidades de aprendizagem profissionais.
À minha coorientadora Professora Doutora Filomena Vieira que com a sua tranquilidade apoiou-me nos momentos de maior pressão, depositando confiança no meu trabalho.
Ao Professor Doutor António Veloso pela disponibilidade em me aceitar na equipa de investigação no Laboratório de Biomecânica e Morfologia Funcional, sem a qual não teria a capacidade de desenvolver esta tese.
O meu profundo agradecimento ao Professor Doutor Augusto Gil Pascoal e à Professora Doutora Filomena Carnide que em diversos momentos utilizaram o seu precioso tempo para me ajudar em revisões de artigos ou no tratamento estatístico, e sem os quais teria sido bastante mais difícil a elaboração desta tese.
A toda a equipa do Laboratório de Biomecânica e Morfologia Funcional, em especial aos colegas Fátima Ramalho, Liliana Aguiar, Vera Moniz Pereira, Filipa João, Ricardo Matias, Sílvia Cabral, Maria Machado, Sandra Amado, e aos Doutores Wangdo Kim, Paulo Armada-da-Silva, Margarida Espanha, Pedro Mil-Homens e Carlos Andrade, que de forma direta ou indireta, me auxiliaram neste percurso académico, introduzindo mais-valias para o meu conhecimento.
A Professora Doutora Maria Raquel G. Silva, que na fase final da tese ajudou na revisão do texto, dando o seu generoso contributo do seu conhecimento e experiência.
Ao Professor Doutor David Catela que ao longo destes vários anos, tem sido companhia constante no meu desenvolvimento pessoal e profissional, que contribuiu com generosas opiniões e conselhos para esta tese, e que tão pouco este agradecimento pode expressar a minha profunda gratidão.
sucesso profissional.
O meu agradecimento aos meus familiares, pelo apoio constante, pelo acompanhamento nos momentos mais difíceis e pelo estímulo que deram para o meu constante desenvolvimento.
Por fim, e não menor, o agradecimento mais ternurento para a minha família, a
Fátima e em especial para o Gabriel, que reforçou diariamente o apoio à conclusão
IX
This study was supported by FCT - FUNDAÇÃO PARA A CIÊNCIA E TECNOLOGIA / Portuguese Foundation for Science and Technology (http://alfa.fct.mctes.pt/), and is related to the following grants:
Project reference: PTDC/DES/102058/2008. Effects of biomechanical loading on the musculoskeletal system in women during pregnancy and postpartum period. Principal researcher: Rita Santos-Rocha.
This study was also supported by European Union – QREN-InAlentejo - Programa Operacional do Alentejo-2007-2013 / National Strategic Reference Framework. Project Title: Alentejo’s Science and Technology Park – Sport and Health Research Center. Promotor: Polytechnic Institute of Santarém - Sport Sciences School of Rio Maior / Health School of Santarém. Project Coordinator: Rita Santos-Rocha. Project reference: ALENT-07-0262-FEDER-001883.
XI
Adaptações biomecânicas e morfológicas na mulher durante a gravidez e pós-parto, na execução da marcha
Sumário
A gravidez é uma fase especial da vida, com diversas alterações nos sistemas hormonais, anatómicos, e na composição corporal da mulher. No entanto, não é claro que alterações biomecânicas tridimensionais ocorrerem. Através do acompanhamento da mulher na gravidez e pós-parto, os objetivos da presente tese foram: 1) determinar os parâmetros temporais e espaciais do ciclo da marcha; 2) descrever a cinemática angular do membro inferior; 3) calcular os momentos e potências articulares do tornozelo, joelho e coxofemoral, utilizando o cálculo por dinâmica inversa; 4) descrever as magnitudes dos picos dos momentos e potências articulares dos membros inferiores; 5) identificar possíveis diferenças entre as fases de recolha relativamente aos parâmetros biomecânicos; 6) descrever longitudinalmente a composição corporal as alterações morfológicas; 7) analisar a influência das alterações antropométricas na cinética articular. Os resultados mostram que as mulheres mantêm os parâmetros temporais e espaciais da marcha. A cinemática angular do membro inferior tem o mesmo padrão, no entanto, a magnitude de alguns picos, especialmente na bacia e coxofemoral durante a fase terminal do apoio, pré-balanço e de balanço, apresentam alterações significativas. A coxofemoral é a articulação com mais alterações na cinética articular, com um aumento da carga interna associada aos momentos articulares da coxofemoral no plano transversal. No entanto, diversos momentos e potências articulares revelam uma diminuição significativa para o final da gravidez e/ou um aumento entre alguns trimestres da gravidez e o pós-parto. Como esperado, a maioria das variáveis associadas à composição corporal e às dimensões corporais tem um aumento significativo durante a gravidez e uma diminuição no pós-parto. Os modelos desenvolvidos para prever a carga interna aplicada ao membro inferior da grávida através de variáveis antropométricas, incluem quatro modelos com variáveis associadas à quantidade de gordura, quatro modelos com variáveis associadas à massa corporal global, três modelos que incluem a massa livre de gordura, e um modelo que inclui a forma do tronco. Os altos valores do R2 ajustado, mostram que as alterações na composição corporal e morfologia, determinam em grande parte a cinética articular da mulher nesta fase particular da vida.
XIII
Biomechanical and morphological adaptations in women during pregnancy and the postpartum period in walking
Abstract
Pregnancy is a special phase of women's lives, which process leads to several changes in hormonal, anatomical, body composition, and musculoskeletal systems of women. However, it is not clear what three-dimensional biomechanical changes occur at this stage. With the longitudinal monitoring of woman's in pregnancy and postpartum, the purposes of the present thesis were to: 1) determine the temporal parameters of the gait cycle pregnant women; 2) describe the angular kinematics of the lower limb of the pregnant women; 3) calculate net moments of force in ankle, knee and hip joints, using inverse dynamics; 4) describe peak magnitudes of the joint moments of force of the pregnant women; 5) to identify potential differences between the four collection phases on the biomechanical parameters, concerning gait cycle; 6) describe the body composition of women and their morphological changes; 7) Analyse the influence of anthropometric variables in the kinetics of joints of women. Results show that women maintain the same temporal and spatial parameters of gait throughout pregnancy and in the postpartum period. The angular kinematics of lower limb have the same curve pattern, however the magnitude of some peaks, especially in pelvis and hip joint during terminal stance, pre-swing and mid-swing phases, suffer significant changes. The hip is the joint with the greatest changes in joint kinetics during pregnancy, with an increase of the internal loading associated with the hip moments in the transverse plane. In the other planes of motion, joint moments and power shows a significant decrease to the end of pregnancy or an increase from some stages of pregnancy to the postpartum period. As expected, most of the variables associated with body composition and body dimensions showed, a significant increase during pregnancy and a decrease in the postpartum. The models developed to predict women's internal loading through anthropometric variables include, four models with variables associated with the amount of fat, four models that with variables related to overall body weight, three models that include fat-free mass, and one model that includes the shape of the trunk as a predictor variable. The high values of adjusted r square, show that changes in maternal’s body composition and morphology, largely determine kinetic dynamics of the female joints in this particular stage of life.
XV Acknowledgments ... VII Supporting Grants ... IX Título ... XI Sumário ... XI Title ... XIII Abstract ... XIII Contents ... XV List of Tables ... XIX List of Figures ... XXI List of Abbreviations ... XXIII
1 Introduction ... 1
Rationale for the Investigation ... 2
General Research Questions ... 3
Purposes of the Thesis ... 4
Thesis Overview ... 4
Supporting... 6
Methodological Considerations ... 6
References... 9
2 Biomechanics of gait during pregnancy: a review ... 11
Abstract ... 12
Introduction ... 13
Aim of the review... 14
Methods ... 14
Eligibility criteria ... 14
Information source ... 15
Search strategy and study selection ... 15
Study selection and characteristics ... 15
Outcome measures: spatial and temporal parameters ... 17
Outcome measures: joint kinematics ... 17
Outcome measures: joint kinetics ... 18
Discussion... 18
Limitations ... 19
Conclusions ... 20
References... 21
3 Three-dimensional Kinematic adaptations of gait throughout pregnancy and post-partum ... 23
Abstract ... 24
Introduction ... 25
Objectives ... 26
Materials and Methods ... 26
Subjects ... 26
Data Collection and Processing ... 27
Statistical Analysis ... 30
Results ... 31
Spatial and Temporal parameters ... 31
Joint Kinematics ... 31 Sagittal Plane ... 31 Frontal Plane... 34 Transverse Plane ... 35 Discussion... 37 Conclusions ... 39 References... 41
4 Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum ... 43
XVII
Objectives ... 46
Materials and Methods ... 47
Subjects ... 47
Data Collection and Processing ... 47
Statistical Analysis ... 50
Results ... 50
Ground Reaction Forces ... 50
Joint Moments of Force ... 52
Sagittal Plane ... 52 Frontal Plane... 55 Transverse Plane ... 56 Joint Power ... 57 Sagittal Plane ... 57 Frontal Plane... 59 Transverse Plane ... 60 Discussion... 60 Conclusions ... 63 References ... 65
5 Influence of anthropometric and body composition changes on kinetics parameters of gait throughout pregnancy and in postpartum period ... 67
Abstract ... 68
Introduction ... 69
Objectives ... 70
Materials and Methods ... 70
Subjects ... 70
Anthropometric and body composition profile ... 72
Regression models for joint moments ... 75
Regression models for joint powers ... 77
Discussion... 79
Conclusions ... 83
References... 84
6 General Discussion and Conclusions ... 87
General Discussion and Conclusions ... 88
Recommendations for practice ... 93
Recommendations for Future Research ... 94
References... 96
Global Reference List ... 99
Appendix 1 ... 105
XIX
TABLE 1. SEGMENT, PARENT SEGMENT AND ITS INVERSE KINEMATICS CONSTRAINTS, EXTRACTED FROM VISUAL 3D SOFTWARE... 8 TABLE 2. STUDIES INCLUDED IN THE REVIEW, LISTED BY CHRONOLOGICAL ORDER OF PUBLICATION, REGARDING AUTHORS, SAMPLE SIZE, DATA COLLECTION PHASES, SAMPLE MEAN AGE, OUTCOME VARIABLES AND BIOMECHANICAL INSTRUMENTS USED. ... 16 TABLE 3.CHARACTERISTICS OF THE SAMPLE DATA FOR WEIGHT, BODY MASS INDEX (BMI) AND GESTATIONAL WEEKS, IN EACH COLLECTION PHASE. ... 26 TABLE 4-SPATIAL AND TEMPORAL PARAMETERS (MEAN±SD) OF GAIT DURING PREGNANCY
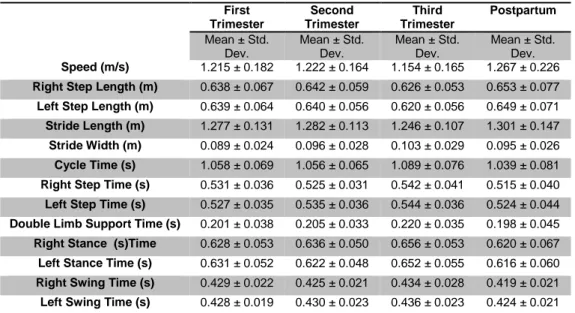
AND IN THE POSTPARTUM PERIOD (N=11). ... 31 TABLE 5.MEAN AND STANDARD DEVIATION OF THE JOINT ANGLE PEAKS, AND SIGNIFICANCE
LEVELS OF THE PAIRS OF COLLECTIONS WITH SIGNIFICANT CHANGES FOR THE SAGITTAL PLANE. ... 33 TABLE 6.MEAN AND STANDARD DEVIATION OF THE JOINT ANGLE PEAKS, AND SIGNIFICANCE
LEVELS OF THE PAIRS OF COLLECTIONS WITH SIGNIFICANT CHANGES FOR THE FRONTAL PLANE. ... 35 TABLE 7-MEAN AND STANDARD DEVIATION OF THE JOINT ANGLE PEAKS, AND SIGNIFICANCE LEVELS OF THE PAIRS OF COLLECTIONS WITH SIGNIFICANT CHANGES FOR THE TRANSVERSE PLANE. ... 36 TABLE 8.MEAN AND STANDARD DEVIATION OF THE PEAK VALUES FOR VERTICAL, ANTERIOR -POSTERIOR, AND MEDIAL-LATERAL COMPONENTS OF THE GROUND REACTION FORCES. ... 52 TABLE 9. MEAN AND STANDARD DEVIATION OF THE JOINT MOMENT PEAKS, AND SIGNIFICANCE LEVELS OF THE PAIRS OF COLLECTIONS WITH SIGNIFICANT CHANGES FOR SAGITTAL, FRONTAL AND TRANSVERSE PLANES. ... 54 TABLE 10. MEAN AND STANDARD DEVIATION OF THE JOINT POWER PEAKS, AND
SIGNIFICANCE LEVELS OF THE PAIRS OF COLLECTIONS WITH SIGNIFICANT CHANGES FOR SAGITTAL, FRONTAL AND TRANSVERSE PLANES. ... 58 TABLE 11. WEIGHT, BODY MASS INDEX (BMI) AND GESTATIONAL WEEKS OF THE
SIGNIFICANT VALUES OF POST-HOC TESTS. ... 73 TABLE 13.BODY COMPOSITION VARIABLES OF THE PARTICIPANTS DURING PREGNANCY AND IN POSTPARTUM PERIOD. MEAN VALUES ± STANDARD DEVIATION OF VARIABLES AND SIGNIFICANT VALUES OF POST-HOC TESTS (P<0.05). ... 74 TABLE 14.MEAN VALUES AND STANDARD DEVIATION OF JOINT MOMENTS AND POWERS, AND GRF DURING COLLECTION PHASES. ... 75 TABLE 15. LINEAR REGRESSION MODELS FOR JOINTS MOMENT IN SAGITTAL PLANE OF MOTION. ... 76 TABLE 16.REGRESSION MODELS FOR JOINTS MOMENT IN TRANSVERSE PLANE OF MOTION.
... 77 TABLE 17.REGRESSION MODELS FOR JOINTS POWER IN SAGITTAL PLANE OF MOTION. ... 77 TABLE 18.REGRESSION MODELS FOR JOINTS POWER IN TRANSVERSE PLANE OF MOTION. 78 TABLE 19.REGRESSION MODELS FOR GROUND REACTION FORCES... 79
XXI
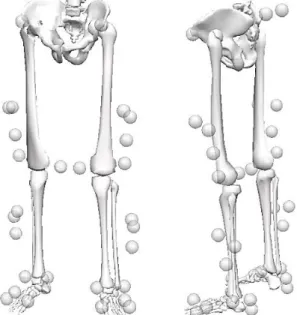
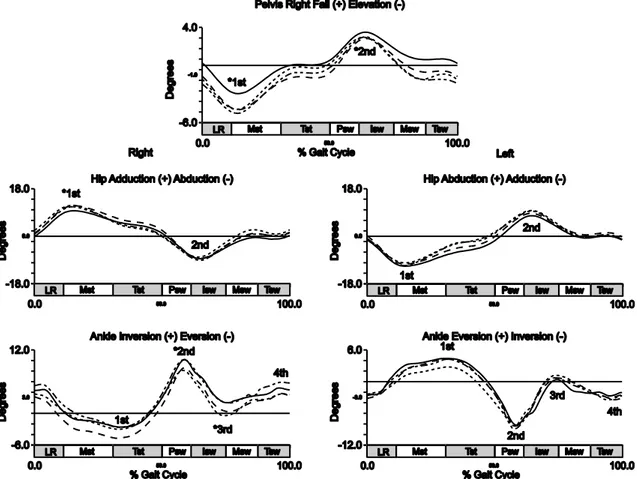
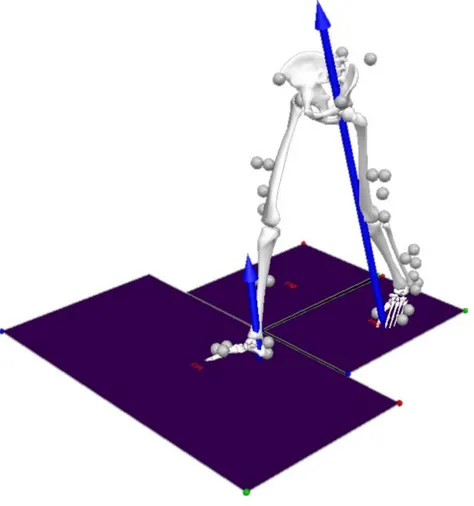
FIGURE 1. RECONSTRUCTED BIOMECHANICAL MODEL IN VISUAL 3D WITH MARKER SETUP USED FOR MOTION CAPTURES.ANTERIOR AND LATERAL VIEW OF THE MODEL. ... 28 FIGURE 2.MEAN ANGLES OF THE LOWER LIMB JOINTS, IN THE SAGITTAL PLANE.KINEMATIC PARAMETERS OF THE GAIT OF PREGNANT WOMEN IN THE LATER STAGES OF FIRST (DOTTED LINE), SECOND (DASHED LINE) AND THIRD TRIMESTER (SOLID LINE) AND OF THE POSTPARTUM PERIOD (DASH DOT DOT LINE). ... 32 FIGURE 3.MEAN ANGLES OF THE LOWER LIMB JOINTS, IN THE FRONTAL PLANE.KINEMATIC PARAMETERS OF THE GAIT OF PREGNANT WOMEN IN THE LATER STAGES OF FIRST (DOTTED LINE), SECOND (DASHED LINE) AND THIRD TRIMESTER (SOLID LINE) AND OF THE POSTPARTUM PERIOD (DASH DOT DOT LINE). ... 34 FIGURE 4. MEAN ANGLES OF THE LOWER LIMB JOINTS, IN THE TRANSVERSE PLANE.
KINEMATIC PARAMETERS OF THE GAIT OF PREGNANT WOMEN IN THE LATER STAGES OF FIRST (DOTTED LINE), SECOND (DASHED LINE) AND THIRD TRIMESTER (SOLID LINE) AND OF THE POSTPARTUM PERIOD (DASH DOT DOT LINE). ... 36 FIGURE 5. RECONSTRUCTED BIOMECHANICAL MODEL IN VISUAL 3D WITH MARKER SETUP USED FOR MOTION CAPTURES.ANTERIOR AND LATERAL VIEW OF THE MODEL. ... 48 FIGURE 6. MEAN VALUES OF GROUND REACTION FORCES OF EACH GROUP (IN
BODYWEIGHT). EACH LINE REPRESENT THE LATER STAGES OF FIRST (DOT LINE), SECOND (DASHED LINE) AND THIRD TRIMESTERS (SOLID LINE) AND OF POSTPARTUM PERIOD (DASH DOT DOT LINE).MEAN VERTICAL, ANTERIOR - POSTERIOR, AND MEDIAL -LATERAL COMPONENTS OF GRF, FOR RIGHT AND LEFT LOWER LIMBS. THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST, 2ND, AND 3RD, AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 51 FIGURE 7.JOINTS MOMENTS IN THE SAGITTAL PLANE DURING GAIT (IN N.M.KG-1).EACH LINE REPRESENT THE LATER STAGES OF FIRST (DOT LINE), SECOND (DASHED LINE) AND THIRD TRIMESTERS (SOLID LINE) AND OF POSTPARTUM PERIOD (DASH DOT DOT LINE). MEAN JOINT MOMENTS OF THE HIP, KNEE, AND ANKLE, FOR RIGHT AND LEFT LOWER LIMBS. THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST, 2ND, AND 3RD, AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 53 FIGURE 8.JOINTS MOMENTS IN THE FRONTAL PLANE DURING GAIT (IN N.M.KG-1).EACH LINE
THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST AND 2ND, AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 55 FIGURE 9.JOINTS MOMENTS IN THE TRANSVERSE PLANE DURING GAIT (IN N.M.KG-1. EACH
LINE REPRESENT THE LATER STAGES OF FIRST (DOT LINE), SECOND (DASHED LINE) AND THIRD TRIMESTERS (SOLID LINE) AND OF POSTPARTUM PERIOD (DASH DOT DOT LINE). MEAN JOINT MOMENTS OF THE HIP, AND ANKLE, FOR RIGHT AND LEFT LOWER LIMBS. THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST AND 2ND AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 56 FIGURE 10. JOINTS POWER IN THE SAGITTAL PLANE DURING GAIT (IN W.KG-1). EACH LINE REPRESENT THE LATER STAGES OF FIRST (DOT LINE), SECOND (DASHED LINE) AND THIRD TRIMESTERS (SOLID LINE) AND OF POSTPARTUM PERIOD (DASH DOT DOT LINE). MEAN JOINT POWERS OF THE HIP, KNEE, AND ANKLE, FOR RIGHT AND LEFT LOWER LIMBS. THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST, 2ND, AND 3RD AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 57 FIGURE 11. JOINTS POWER IN THE FRONTAL PLANE DURING GAIT (IN W.KG-1).EACH LINE REPRESENT THE LATER STAGES OF FIRST (DOT LINE), SECOND (DASHED LINE) AND THIRD TRIMESTERS (SOLID LINE) AND OF POSTPARTUM PERIOD (DASH DOT DOT LINE). MEAN JOINT POWERS OF THE HIP, AND ANKLE, FOR RIGHT AND LEFT LOWER LIMBS.THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST, 2ND, 3RD AND 4TH AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 59 FIGURE 12. JOINTS POWER IN THE TRANSVERSE PLANE DURING GAIT (IN W.KG-1). EACH
LINE REPRESENT THE LATER STAGES OF FIRST (DOT LINE), SECOND (DASHED LINE) AND THIRD TRIMESTERS (SOLID LINE) AND OF POSTPARTUM PERIOD (DASH DOT DOT LINE). MEAN JOINT POWERS OF THE HIP, AND ANKLE, FOR RIGHT AND LEFT LOWER LIMBS.THE CURVE PEAKS ARE INDICATED BY NUMBERS: 1ST, 2ND,3RD AND 4TH AND (*) POINTS THE SIGNIFICANT DIFFERENCES. ... 60 FIGURE 13. SCATTER PLOTS AND REGRESSION LINES OF JOINT MOMENT PREDICTIVE
MODELS. ... 76 FIGURE 14.SCATTER PLOTS AND REGRESSION LINES OF JOINT POWER PREDICTIVE MODELS. ... 78 FIGURE 15.SCATTER PLOTS AND REGRESSION LINES OF GRF PREDICTIVE MODELS. ... 79
XXIII
2D - Bidimensional
3D - Tridimensional
Abds - Abductors
Adds - Adductors
BMG - Body Mass Gain
BMI - Body Mass Index
BW - Bodyweight CG - Centre of Gravity Evs - Evertors Ext - External Exts - Extensors Flexs - Flexors
GRF - Ground Reaction Forces
Int - Internal
Invs - Invertors
ISAK - International Society for the Advancement of Kinanthropometry
RM - Repeated Measures
ROM - Range of motion
Rots - Rotators
Chapter
1
Rationale for the Investigation
Pregnancy is a special phase of life, in which women suffer visible morphological changes in their body, and also other less visible changes in physiological and hormonal systems. In addition to these changes, the growth and development of the foetus, the uterus, all pregnancy-associated tissues, including placenta and foetal membranes and also the amount of liquid, contribute to an increase in the woman’ body weight in an average of 12 kilograms. Of these, the weight of the foetus may contribute to 3.5 kg, plus 2 kg corresponding to the weight of the amniotic fluid, placenta and foetal membranes, more 1 kg for uterine weight and 1 kg for woman's breasts. The remaining 4.5 kg corresponds to an increase of blood volume and extracellular fluid (3 kg), and an increase of body fat (1.5 kg). Much of these tissues are expelled during birth, and in the following days, the fluid in excess is excreted in the urine (Guyton & Hall, 2006).
Recent evidence-based studies show that exercise is safe for both mother and foetus. The literature supports the recommendation to initiate or continue exercise in most pregnancies (Paisley, Joy, & Price, 2003; Parad, Leonard, & Handler, 2015), even when it comes to moderate-to-vigorous resistance exercise, since it's a healthy pregnancy (Petrov Fieril, Glantz, & Fagevik Olsen, 2015). Different modes of exercise, such as walking, jogging, cycling and swimming, with low and high intensity are not associated with increased miscarriage rates between the first trimester until the middle of the second trimester (Parad et al., 2015). Walking appears as one of the preferred modes of exercise, not only because it is an exercise that uses large muscle groups in a continuous and rhythmic way, but also because it is a physical activity that is easy to control regarding the intensity of exercise (A.C.O.G., 2003).
The biomechanical loading assessment of gait in the musculoskeletal system of pregnant women is of particular interest because this information becomes very important to implement exercise programs for pregnant women and to develop strategies to increase adherence. There are many anatomical changes during pregnancy that could potentially lead to gait alterations, and those alterations may contribute to musculoskeletal overuse conditions such as back and lower limb pain (Foti, Davids, & Bagley, 2000). Nevertheless, to conduct an evaluation of the human motion, it is necessary to proceed with a description of the pattern, which in the case of the walking is well defined and described in the literature (Los Amigos Research Education Institute Inc et al., 2001; Perry & Burnfield, 2010; Rose & Gamble, 2006; Vaughan, Davis, & O'Connor, 1999; Whittle, 2007). It is not clear whether the temporal,
3
spatial, kinematic and kinetic patterns of gait during pregnancy are the same as the apparently healthy adult population, if the changes that happen in this period are due to pregnancy, or due to the normal processes that take place over time in a perspective of lifespan development.
In the last decades, few studies have analysed the mechanics of walking in the body of the woman from the beginning of pregnancy (Falola, Gouthon, Koussihouede, Agossa, & Brisswalter, 2009; W. L. Gilleard, 2013; Hagan & Wong, 2010; Huang, Lin, Ho, Yu, & Chou, 2002). These studies have reported few changes to the temporal, spatial, kinematic and kinetic pattern of walking gait, but are not mentioned the inherent calibration errors of the systems they use, and only some of them use the last technology devices to accomplish these assessments. Thus, it becomes essential a detailed quantitative analysis of the movement data, attempting to access the women from the beginning of pregnancy. It is necessary to take into account, however, the great privacy that women give to their condition during at least the first trimester, usually because many spontaneous miscarriages happen during this period, which can be a major barrier to getting women for the sample of the first trimester. Another aspect that must be considered is the longitudinal follow-up of the women throughout pregnancy, to the detriment of analysis by cohorts with a cross-sectional design. In order to detect changes that are due to the course of pregnancy, should be implemented an experimental design of longitudinal and prospective type. This type of experimental design aims to collect data from the same subjects at more than one point over the forward passage of time (Bowling, 2002). To this end we intend to perform a biomechanical evaluation, which is considered a powerful way of observation at the highest level of evaluation, where it possible to compare in detail (Winter, 2005), the changes that are due to the pregnancy.
General Research Questions
Since there is some diversity in the results and only a minority of studies considers early pregnancy, the questions that arise were the following:
1. Are there any changes in temporal and spatial parameters, and in the kinematics of the pregnant woman gait, especially in the joints kinematics of the lower limb?
2. Are there any changes in kinetic parameters of the pregnant woman gait, especially in the joints kinetics of the lower limb?
3. Are morphological and body composition changes of women happening consistently since the beginning of pregnancy?
4. Are there any effects of the morphology on the kinetic parameters during pregnancy and postpartum?
Purposes of the Thesis
In order to better understand the biomechanics of woman's gait during pregnancy and in the postpartum period, the purposes of the present thesis were to:
1. Determine the temporal parameters of the gait cycle; 2. Describe the angular kinematics of the lower limbs;
3. Calculate net moments of force in ankle, knee and hip joints, using inverse dynamics;
4. Describe peak magnitudes of the joint moments and joint powers;
5. Identify potential differences between the four collection phases - first, second and third trimesters of pregnancy and postpartum period - on the biomechanical parameters, concerning gait cycle;
6. Describe the body composition of women and their morphological changes throughout pregnancy and postpartum;
7. Analyze the influence of anthropometric variables in the kinetics of lower limb joints.
Thesis Overview
Following the present introduction (chapter 1), this thesis embraces a compilation of four papers, as follows.
The aim of the first study (chapter 2) was to analyze the available evidence on the biomechanical adaptations of gait that occur throughout pregnancy and in postpartum, specifically with regard to the temporal, spatial, kinematic and kinetic parameters of gait. The paper is published at:
Branco M, Santos-Rocha R, & Vieira F (2014). Biomechanics of Gait during Pregnancy (Review Article). The World Scientific Journal, Volume 2014 (2014), Article ID 527940, 5 pages. http://dx.doi.org/10.1155/2014/527940
The aim of the second study (chapter 3) was to quantify and verify the kinematic changes of gait as pregnancy progresses. If the changes were confirmed, the second objective was to ascertain whether women could recover the initial kinematic patterns
5
in the postpartum period. In terms of the main objective, it is necessary to describe the kinematic variables in the joints of the lower limb during gait at the end of the first, second and third trimesters of pregnancy and in the postpartum period. The paper is published at:
Branco M, Santos-Rocha R, Aguiar L, Vieira F, & Veloso A (2015). Three-dimensional Kinematic adaptations of gait throughout pregnancy and post-partum. http://www.johk.pl/terms_and_conditions.html. Acta of Bioengineering and Biomechanics. (in press)
The aim of the third study (chapter 4) was to assess the gait kinetics, in order to check if there are any changes in the dynamics of the load of women throughout pregnancy and after delivery. To achieve the main objective, it was necessary to describe and quantify the kinetic variables relating to the GRF, joint moments of force, and joint power of ankle, knee and hip, during gait, at the end of the first, second and third trimesters of pregnancy and in the postpartum period. The paper is published at:
Branco, M., Santos-Rocha, R., Vieira, F., Aguiar, L., & Veloso, A. P. (2015). Three-Dimensional Kinetic Adaptations of Gait throughout Pregnancy and Postpartum. Scientifica, 2015, 14. doi: 10.1155/2015/580374.
The aim of the fourth study (chapter 5) was to quantify the maternal anthropometric and body composition changes throughout pregnancy and in the postpartum period, and identify what is the contribution of these parameters on the lower limb joints kinetic during walking gait. The paper was submitted to:
Branco, M., Santos-Rocha, R., Vieira, F., Silva, M-R. G., Aguiar, L., & Veloso, A. P. (submitted). Influence of body composition changes in kinetics parameters of gait throughout pregnancy and in the postpartum period. Scientifica, 2016 (in press).
Finally, in chapter 6, a general discussion, the main conclusions of the thesis and the recommendations for practice are presented, as well as few recommendations for future research.
The study was approved by ethics committee of Faculty of Human Kinetics, University of Lisbon.
Supporting
The present publication was supported by the following projects:
(1) Funder: FCT – Fundação para a Ciência e Tecnologia / Portuguese Foundation for Science and Technology. Project title: Effect of biomechanical loading on the musculoskeletal system in women during pregnancy and the postpartum period. Promotor: CIPER / FMH-UL / ESDRM-IPS. Principal Researcher: Rita Santos-Rocha. Project reference: PTDC/DES/102058/2008.
(2) Funder: European Union – QREN-InAlentejo-Programa Operacional do Alentejo-2007-2013 / National Strategic Reference Framework. Project title: Alentejo’s Science and Technology Park – Sport and Health Research Center. Polytechnic Institute of Santarém - Sport Sciences School of Rio Maior / Health School of Santarém. Project Coordinator: Rita Santos-Rocha. Project reference: ALENT-07-0262-FEDER-001883.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Methodological Considerations
Regarding the means and methods used in the present work, several methodological definitions are possible to use. However, considering the different publications, the methods used to build the biomechanical model of the woman's lower limbs throughout pregnancy and in the postpartum period, was based on the definitions recommended by Robertson, Caldwell, Hamill, Kamen, and Whittlesey (2014). For the construction of the Cartesian system for three-dimensional collections the definitions established by Hamill, Selbie, and Kepple (2014), were considered in what concerns to a setup with at least ten high-speed infrared cameras (Oqus-300, Qualisys, Sweden; FR: 500 Hz) positioned statically to minimize light reflection artefacts, and three force platforms (two Kistler AG, Winterthur, Switzerland, and one Advanced Mechanical Technology, Inc., Watertown, U.S.A.; FR: 1000 Hz) in order to collect at least two consecutive contacts of the feet on the ground. The three-dimensional space was calibrated by wand type, with an exact wand length of 751.4 mm moved randomly across the recorded field before the data collection of each participant. Calibration was accepted if the standard deviation of the wand length measures was below 0.5 mm. The marker setup follows the recommendation of Cappozzo, Cappello, DellaCroce, and Pensalfini (1997) for lower limb segments, and CODA (Charnwood Dynamics Ltd,
7
Leicestershire, United Kingdom) protocols for models of the pelvis segment. The explanation of the setup marks, to define each segment can be found in Chapters 3 and 4.
Due to major changes in the pelvic and abdominal volume of the pregnant woman, some care has been taken in the construction segment of the pelvis, not only in the placement of markers (point 1), but also in the selection of the regression equations used to compute the joint center of the hip (point 2). Thus, for the first point, to ensure the correct placement of the reflective markers throughout pregnancy, a comparison of the length of each segment (whose size is defined by the markers placed in proximal and distal extremities) was performed, in particular the right and left segments of the shank and the feet. After this comparison, no differences were found in the size of the segments of shank (F(3,30)=0.049, p=0.985 and F(3,30)=0.580, p=0.633, respectively for right and left shank) and of the feet (F(3,30)=0.372, p=0.774 and F(3,30)=0.190, p=0.902, respectively for right and left foot).
In the second point, for the estimation of hip joint center after the construction of the pelvis model, the equations developed by Bell and colleagues (Bell, Brand, & Pedersen, 1989; Bell, Pedersen, & Brand, 1990), by Harrington, Zavatsky, Lawson, Yuan, and Theologis (2007) and by Davis, Ounpuu, Tyburski, and Gage (1991) were considered. Although there are no specific equations to compute the hip joint center of the pregnant woman, our choice falls on the equations of Bell and colleagues (Bell et al., 1989; Bell et al., 1990), for being frequently used and so there are the same basis for comparing the results found with the existing publications.
In the construction of the model global optimization algorithms were considered, originally proposed by Lu and O'Connor (1999), where it is assumed that the model consists of rigid bodies connected by joints, and where the optimized position is one whose multilink model minimizes difference between the measurement and the model given by the coordinates of the markers. These algorithms were then mathematically improved by van den Bogert and Su (2008), which considers a minimum markers for describing the position of the segments. In the present study we also use the Levenberg-Marquardt algorithm in order to make the more efficient calculation of common minimization algorithms (Levenberg, 1944; Marquardt, 1963). In this global optimization is considered a hierarchy between segments, and in this case the construction of the model and respective kinematic calculations are performed from proximal to distal segments. In order to reduce errors of the model it is possible to define constraints (limit some degrees of freedom) of every joint, which are presented in Table 1.
Table 1. Segment, parent segment and its inverse kinematics constraints, extracted from Visual 3D software.
Segment Parent Translations Rotations
Pelvis LAB X Y Z R1 R2 R3
Right Hip Pelvis 0 0 0 R1 R2 R3
Right Shank Right Hip 0 0 0 R1 0 0 Right Foot Right Shank 0 0 0 R1 R2 R3
Left Hip Pelvis 0 0 0 R1 R2 R3
Left Shank Left Hip 0 0 0 R1 0 0 Left Foot Left Shank 0 0 0 R1 R2 R3
For the calculations of the angles between segments, the Cardan-Euler system was used, for having provided an optimal representation of the joint angles of the lower extremities (Hamill et al., 2014), with a sequence of rotation XYZ.
Given that in the calculation of the joint angles, the matrix of rotation considers the coordinate system of the proximal segment, which allows making an angle normalization, where the "zero" position corresponds to the standing posture, taken in the standing trial with all anatomical markers. This procedure allows standardizing the analysis of the participants over time and guarantees uniformity across participants.
The determination of the kinetic variables of the joint moments and joint powers was performed by means of inverse dynamics analysis. Therefore three kinds of data are needed. In first place, the anthropometric data, specifically: the location of the coordinate system of each segment in its proximal joint center; the segment mass; its center of mass; and also, its moment of inertia. The determination of the mass of the segments was based on regression equations by Dempster (1955). To calculate the center of mass and moment of inertia of the segments, its primitive geometric shape was considered (Hanavan, 1964), set by the segment length, the proximal radius and distal radius of the segment, calculated by V3D software based on the location of the markers. The kinematic calculations are the second kind of data needed for each segment, in order to provide the center of gravity position, translational velocity, translational acceleration, angular velocity, and angular acceleration, which in this work, were also computed in V3D. Finally, the third kind of data were the external forces, which were collected by three force platforms (two Kistler force platforms and one AMTI) in order to achieve contact forces of the feet during two consecutive gait cycles. All steps for calculating by means of inverse dynamics method are described in Robertson et al. (2014) and in C-Motion (2015) website.
9
References
A.C.O.G. (2003). Exercise during pregnancy and the postpartum period (Reprinted from American College of Obstetricians and Gynecologists.). Clinical Obstetrics and Gynecology, 46(2), 496-499.
Bell, Alexander L., Brand, Richard A., & Pedersen, Douglas R. (1989). Prediction of Hip-Joint Center Location from External Landmarks. Human Movement Science, 8(1), 3-16. doi: http://dx.doi.org/10.1016/0167-9457(89)90020-1
Bell, Alexander L., Pedersen, Douglas R., & Brand, Richard A. (1990). A comparison of the accuracy of several hip center location prediction methods. Journal of Biomechanics, 23(6), 617-621. doi: http://dx.doi.org/10.1016/0021-9290(90)90054-7
Bowling, Ann. (2002). Research methods in health : investigating health and health services (2nd ed.). Buckingham ; Philadelphia: Open University Press.
C-Motion. (2015, 27 January 2015). C-Motion Product Documentation. 2015, from
http://c-motion.com/v3dwiki/index.php?title=Main_Page
Cappozzo, A., Cappello, A., DellaCroce, U., & Pensalfini, F. (1997). Surface-marker cluster design criteria for 3-D bone movement reconstruction. Ieee Transactions on Biomedical Engineering, 44(12), 1165-1174. doi:
http://dx.doi.org/10.1109/10.649988
Davis, R. B., Ounpuu, S., Tyburski, D., & Gage, J. R. (1991). A Gait Analysis Data-Collection and Reduction Technique. Human Movement Science, 10(5), 575-587.
Dempster, W. T. (1955). Space requirements of the seated operator. Wright-Patterson Air Force Base. Ohio: WADC Technical Report.
Falola, J. M., Gouthon, P., Koussihouede, F. E. , Agossa, B., & Brisswalter, J. (2009). Gait coordination in pregnancy: A study in a rural population in Africa. Science & Sports, 24(1), 49-51.
Foti, T., Davids, J. R., & Bagley, A. (2000). A biomechanical analysis of gait during pregnancy. Journal of Bone and Joint Surgery-American Volume, 82A(5), 625-632.
Gilleard, W. L. (2013). Trunk motion and gait characteristics of pregnant women when walking: report of a longitudinal study with a control group. BMC Pregnancy Childbirth, 13, 71. doi: http://dx.doi.org/10.1186/1471-2393-13-71
Guyton, Arthur C., & Hall, John E. (2006). Textbook of medical physiology (11th ed.). Philadelphia: Elsevier Saunders.
Hagan, Laura, & Wong, Christopher Kevin. (2010). Gait in Pregnant Women: Spinal and Lower Extremity Changes From Pre- to Postpartum. Journal of Women’s
Health Physical Therapy, 34(2), 46-56. doi:
http://dx.doi.org/10.1097/jwh.0b013e3181e8fd4d
Hamill, Joseph, Selbie, W. Scott, & Kepple, Thomas M. (2014). Three-Dimensional Kinematics. In D. G. E. Robertson, G. E. Caldwell, J. Hamill, G. Kamen & S. N. Whittlesey (Eds.), Research Methods in Biomechanics (Second ed., pp. 35-59). Champaign, IL, USA: Human Kinetics.
Hanavan, E. (1964). A Mathematical Model for the Human Body. Technical Report. Ohio: Wright-Patterson Air Force Base.
Harrington, M. E., Zavatsky, A. B., Lawson, S. E. M., Yuan, Z., & Theologis, T. N. (2007). Prediction of the hip joint centre in adults, children, and patients with cerebral palsy based on magnetic resonance imaging. Journal of Biomechanics, 40(3), 595-602. doi: DOI 10.1016/j.jbiomech.2006.02.003
Huang, Tsan-Hsun, Lin, Sheng-Che, Ho, Chin-Shan, Yu, Chia-Yuen, & Chou, You-Li. (2002). The gait analysis of pregnant women. Biomedical Engineering - Applications, Basis & Communications, 14(2), 4. doi:
http://dx.doi.org/10.4015/s1016237202000103
Levenberg, K. (1944). A method for the solution of certain problems in least squares. Quarterly of Applied Mathematics, 2, 164-168. doi: citeulike-article-id:1951284 Los Amigos Research Education Institute Inc, Service, Rancho Los Amigos Medical
Center. Pathokinesiology, Center, Rancho Los Amigos National Rehabilitation, Department, Rancho Los Amigos Medical Center. Physical Therapy, Service, Rancho Los Amigos National Rehabilitation Center. Pathokinesiology, & Department, Rancho Los Amigos National Rebabilitation Center. Physical Therapy. (2001). Observational Gait Analysis: Los Amigos Research and Education Institute, Rancho Los Amigos National Rehabilitation Center.
Lu, T. W., & O'Connor, J. J. (1999). Bone position estimation from skin marker co-ordinates using global optimisation with joint constraints. Journal of Biomechanics, 32(2), 129-134. doi: Doi 10.1016/S0021-9290(98)00158-4 Marquardt, D. W. (1963). An Algorithm for Least-Squares Estimation of Nonlinear
Parameters. Journal of the Society for Industrial and Applied Mathematics, 11(2), 431-441.
Paisley, T. S., Joy, E. A., & Price, R. J., Jr. (2003). Exercise during pregnancy: a practical approach. Curr Sports Med Rep, 2(6), 325-330.
Parad, A., Leonard, E., & Handler, L. (2015). Exercise and pregnancy loss. Am Fam Physician, 91(7), 437-438.
Perry, Jacquelin, & Burnfield, Judith M. (2010). Gait analysis : normal and pathological function (2nd ed.). Thorofare, NJ: SLACK.
Petrov Fieril, K., Glantz, A., & Fagevik Olsen, M. (2015). The efficacy of moderate-to-vigorous resistance exercise during pregnancy: a randomized controlled trial. Acta Obstet Gynecol Scand, 94(1), 35-42. doi: 10.1111/aogs.12525
Robertson, D Gordon E , Caldwell, Graham E, Hamill, Joseph , Kamen, Gary , & Whittlesey, Saunders N (2014). Research Methods in Biomechanics (Second ed.). Champaign, IL, USA: Human Kinetics.
Rose, Jessica, & Gamble, James Gibson. (2006). Human walking (3rd ed.). Philadelphia: Lippincott Williams & Wilkins.
van den Bogert, A. J., & Su, A. (2008). A weighted least squares method for inverse dynamic analysis. Computer Methods in Biomechanics and Biomedical Engineering, 11(1), 3-9. doi: 10.1080/10255840701550865
Vaughan, Christopher L., Davis, Brian L., & O'Connor, Jeremy C. (1999). Dynamics of human gait (2nd ed.). South Africa: Kiboho Publishers.
Whittle, Michael. (2007). Gait analysis : an introduction (4th ed.). Edinburgh ; New York: Butterworth-Heinemann.
Winter, David A. (2005). Biomechanics and motor control of human movement (3rd ed.). Hoboken, New Jersey: John Wiley & Sons.
Chapter
2
2 Biomechanics of gait during pregnancy: a
review
1
1 Published as: Branco, M., Santos-Rocha, R., & Vieira, F. (2014). Biomechanics of Gait during Pregnancy. The Scientific World Journal, 2014, 5. doi: 10.1155/2014/527940 (Appendix 2)
Abstract
During pregnancy women experience several changes in the body's physiology, morphology and hormonal system. These changes may affect the balance and body stability and can cause discomfort and pain. The adaptations of the musculoskeletal system due to morphological changes during pregnancy are not fully understood. Few studies clarify the biomechanical changes of gait that occur during pregnancy and in postpartum. The purpose of this review was to analyse the available evidence on the biomechanical adaptations of gait that occur throughout pregnancy and in postpartum, specifically with regard to the temporal, spatial, kinematic and kinetic parameters of gait. Three databases were searched and 9 studies with a follow-up design were retrieved for analysis. Most studies performed a temporal, spatial and kinematic analysis. Only three studies performed a kinetic analysis. The adaptation strategies to the anatomical and physiological changes throughout pregnancy are still unclear, particularly in a longitudinal perspective and regarding kinetic parameters.
13
Introduction
Pregnancy is a unique time in the life of women with many changes that affect the musculoskeletal system (Artal & O'Toole, 2003). Over 38 to 42 weeks, women experience several changes in the body's physiology, morphology and hormonal system. These changes are visible especially in increased weight and skeletal alignment. Other less visible changes are the increased joint laxity, and change in the centre of gravity. Altogether, these changes affect the balance and body stability and can cause discomfort and pain (Butler, Druzin, & Sullivan, 2006). The displacement of the centre of gravity has been discussed over the years with different statements. Some studies indicate that the centre of gravity (CG) moves upper and anteriorly (e.g., Foti et al., 2000; Rodacki, Fowler, Rodacki, & Birch, 2003). Other studies state that the CG shifts on the upper and posterior direction (e.g., Fries & Hellebrandt, 1943). Whitcome, Shapiro, and Lieberman (2007), evaluated the evolution of lumbar lordosis in bipedal hominids, and the results elucidate that the CG moves anteriorly until the foetus reaches 40% of the expected final weight. From that moment, the woman increases the lordotic adjustment which in turn enables the control of the CG, but with greater biomechanical costs (Foti et al., 2000).
Hormonal changes in women are quite variable throughout pregnancy. However, the hormone relaxin may have a more decisive role in the mechanics of movement, as it provides greater ligament laxity in the pelvis and on the peripheral joints (Butler et al., 2006; Calguneri, Bird, & Wright, 1982; Schauberger et al., 1996). The concentration peak of relaxin occurs around the 12th week of gestation, which means that there is enough time to act on osteoarticular structures until the end of pregnancy.
One of the aspects that most influences the musculoskeletal system is the increase in maternal weight. When weight is in excess it may cause several adverse maternal effects, including gestational hypertension, gestational diabetes, difficulties during labour, weight retention in postpartum, and subsequent maternal obesity with the risk for unsuccessful breastfeeding (Institute of Medicine and National Research Council of the National Academies, 2009). The ideal weight gain during pregnancy is related to the women's weight or body mass index (BMI) before pregnancy. The weight gain may range between 12.5 Kg and 18 Kg for women under weight (BMI < 18.5); between 11.5 Kg and 16 Kg for women with normal weight (18.5 ≤ BMI < 25); between 7 Kg and 11.5 Kg for women who are overweight (25 ≤ BMI < 30) and; between 5 Kg and 9 Kg and for obese women (Institute of Medicine and National Research Council of
the National Academies, 2009). The weight gain during pregnancy is related to several factors, such as, the amount of blood, the increased volume of the breasts, the increased fat mass and extracellular fluid (Whitcome et al., 2007). The foetal tissues, the placenta and the amniotic fluid are related to the weight gain of the foetus (Institute of Medicine and National Research Council of the National Academies, 2009).
A strategy to control weight gain during pregnancy is by performing structured or recreational physical activity. The guidelines for exercise prescription of the American College of Obstetricians and Gynecologists recommend aerobic exercise consisting of activities that use large muscle groups in a continuous, rhythmic manner (Artal & O'Toole, 2003). Walking emerges as a highly recommended physical activity for pregnant women. Walking is one of the movements most commonly performed by people in the day-to-day tasks and it is easy to control exercise intensity.
When performing motor tasks such as walking, the adaptations of the musculoskeletal system due to morphological changes during pregnancy are not fully known. Few studies clarify the biomechanical changes of gait that occur during pregnancy and in postpartum.
Aim of the review
The purpose of this review was to analyse the available evidence on the biomechanical adaptations of gait that occur throughout pregnancy and in postpartum, specifically with regard to the temporal, spatial, kinematic and kinetic parameters of gait.
Methods
Eligibility criteria
The review was limited to studies meeting the following eligibility criteria: 1) healthy pregnant women with no history of foot, ankle, knee, musculoskeletal or neuromuscular trauma or disease; 2) women aged between 20 and 40 years; 3) studies performed in the last 14 years; 4) studies performed by means of optoelectronic systems, image analysis, force platforms and others; 5) outcome measures related to biomechanical variables of gait including, spatial (stride length, step length and stride width), temporal (single and double support time), kinematic (velocity and cadence),
15
and kinetic (ground reaction forces, joint moment and joint power) parameters; 6) study design including cross-sectional, follow-up, quasi-experimental trials and randomized controlled trials.
Information source
The studies were identified by searching three databases - ScienceDirect, PubMed and SciELO – from January 2000 to August 2014. In addition, reference lists of identified studies were also scanned. Studies published in English, Portuguese, Spanish or French were scanned. Only published full papers were included. Unpublished data, books, conference proceedings or academic theses were not included.
Search strategy and study selection
The search was performed using the following keywords in English: 1) gait / walking; 2) pregnancy / pregnant; and 3) biomechanics / kinetics / kinematics. These keywords were in first place identified in the titles and in the abstracts. The study selection was conducted in two stages. The first stage was the screening of the titles and abstracts against the inclusion criteria to identify relevant papers. The second stage was the screening of the full papers to identify whether they met the eligibility criteria.
Data collection process and analysis
After screening each paper, the following data were extracted: 1) study design; 2) sample size; 3) age of the women; 4) gestational phase of data collection; 5) outcome variables: spatial variables; temporal variables; kinematic variables; kinetic variables; 6) biomechanical instruments. The studies were therefore described according to these characteristics and outcome measures.
Results
Study selection and characteristics
The search yielded 741 articles from the three databases. ScienceDirect (711), PubMed (28) and SciELO (2). After removing duplicate articles 21 articles were considered for analysis. Articles were then screened on the basis of title and abstract, with 16 excluded. After searching the reference lists of the selected articles, 4 more
articles were included. The remaining 9 full papers were examined in detail and found to meet the inclusion criteria, and then, included in the review.
The characteristics of the studies included in the review are presented in Table 2. All studies have follow-up design. The sample sizes across the studies ranged from 29 to 1247. All studies reported the mean age and standard deviation, except one (Lymbery & Gilleard, 2005). Different studies used video-based systems for kinematic analysis, except for two studies that use optoelectronic systems (Branco, Santos-Rocha, Aguiar, Vieira, & Veloso, 2013; Forczek & Staszkiewicz, 2012), and one that only uses pedometers (Falola et al., 2009) to analyse the temporal and spatial parameters. Only three studies report a kinetic analysis (Forczek & Staszkiewicz, 2012; Hagan & Wong, 2010; Lymbery & Gilleard, 2005) and most studies provide an analysis of the kinematic, spatial and temporal parameters.
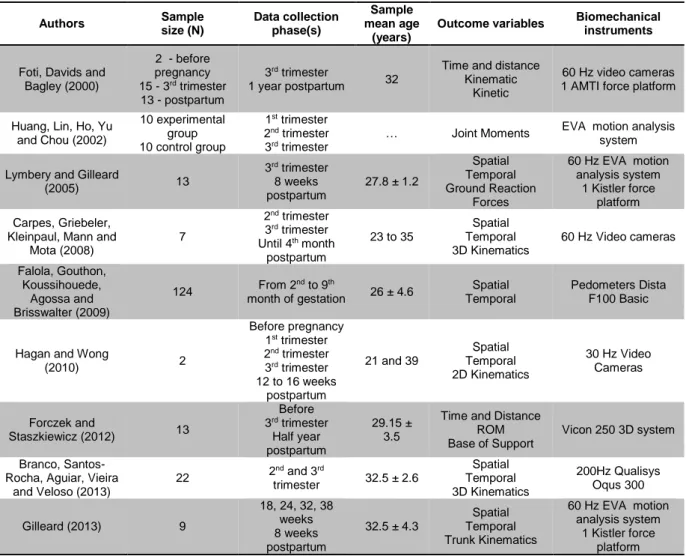
Table 2. Studies included in the review, listed by chronological order of publication, regarding authors, sample size, data
collection phases, sample mean age, outcome variables and biomechanical instruments used.
Authors Sample size (N) Data collection phase(s) Sample mean age (years)
Outcome variables Biomechanical instruments
Foti, Davids and Bagley (2000) 2 - before pregnancy 15 - 3rd trimester 13 - postpartum 3rd trimester 1 year postpartum 32
Time and distance Kinematic
Kinetic
60 Hz video cameras 1 AMTI force platform
Huang, Lin, Ho, Yu and Chou (2002) 10 experimental group 10 control group 1st trimester 2nd trimester 3rd trimester
… Joint Moments EVA motion analysis system
Lymbery and Gilleard
(2005) 13 3rd trimester 8 weeks postpartum 27.8 ± 1.2 Spatial Temporal Ground Reaction Forces 60 Hz EVA motion analysis system 1 Kistler force platform Carpes, Griebeler,
Kleinpaul, Mann and Mota (2008) 7 2nd trimester 3rd trimester Until 4th month postpartum 23 to 35 Spatial Temporal 3D Kinematics 60 Hz Video cameras Falola, Gouthon, Koussihouede, Agossa and Brisswalter (2009) 124 From 2 nd to 9th month of gestation 26 ± 4.6 Spatial Temporal Pedometers Dista F100 Basic
Hagan and Wong
(2010) 2 Before pregnancy 1st trimester 2nd trimester 3rd trimester 12 to 16 weeks postpartum 21 and 39 Spatial Temporal 2D Kinematics 30 Hz Video Cameras Forczek and Staszkiewicz (2012) 13 Before 3rd trimester Half year postpartum 29.15 ± 3.5
Time and Distance ROM Base of Support
Vicon 250 3D system
Branco, Santos-Rocha, Aguiar, Vieira
and Veloso (2013) 22 2 nd and 3rd trimester 32.5 ± 2.6 Spatial Temporal 3D Kinematics 200Hz Qualisys Oqus 300 Gilleard (2013) 9 18, 24, 32, 38 weeks 8 weeks postpartum 32.5 ± 4.3 Spatial Temporal Trunk Kinematics 60 Hz EVA motion analysis system 1 Kistler force platform 2D – two-dimensional analysis; 3D – three-dimensional analysis; ROM – range of motion
17
Outcome measures: spatial and temporal parameters
The variables of stride length, step length, stride width and base of support, single and double support time are the spatial and temporal parameters analysed by the papers reviewed. Most papers reviewed showed changes in spatial and temporal parameters in late pregnancy, specifically, a significant decrease in the length of the gait cycle (Branco et al., 2013; Carpes, Griebeler, Kleinpaul, Mann, & Mota, 2008; W. L. Gilleard, 2013; Hagan & Wong, 2010), and in step length (Branco et al., 2013; Carpes et al., 2008; Forczek & Staszkiewicz, 2012; Hagan & Wong, 2010), and a significant increase in the double support time (Branco et al., 2013; Carpes et al., 2008; Foti et al., 2000). Other studies showed a significant reduction in the single support time (Carpes et al., 2008; Foti et al., 2000), and a significant increase in step width (W. L. Gilleard, 2013; Lymbery & Gilleard, 2005). Forczek and Staszkiewicz (2012) also found a significant increase in the base of support. Nevertheless, the remaining studies suggest that pregnant women have the need to increase the body stability, and use the parameters listed above to meet those demands.
Outcome measures: joint kinematics
The variables of velocity (or speed) and cadence are the kinematic parameters analysed by the studies included in the review. Most papers reviewed showed changes in kinematic parameters in late pregnancy, specifically, a significant decrease in speed (Falola et al., 2009; Forczek & Staszkiewicz, 2012; Hagan & Wong, 2010) and a significant reduction in the gait cadence (Falola et al., 2009; Forczek & Staszkiewicz, 2012).
The joint kinematics of the lower limb, shows few changes throughout pregnancy. The angular displacement of the pelvis increases in the anterior tilt of approximately five degrees (Foti et al., 2000; Hagan & Wong, 2010). The joints of the lower limb in the sagittal plane shows an increase in hip flexion during stance phase (Branco et al., 2013; Foti et al., 2000; Hagan & Wong, 2010), an increase of knee flexion during the terminal stance phase (Carpes et al., 2008), a decrease of knee extension (Branco et al., 2013), and a decrease of ankle dorsiflexion and plantarflexion (Branco et al., 2013; Hagan & Wong, 2010). In the frontal plane, W. L. Gilleard (2013) found a reduction in the amplitude of the unilateral elevation of the pelvis. The hip joint had different results considering the two studies performed: Foti et al. (2000) found a peak with greater magnitude in the hip adduction; Branco et al. (2013) found a decrease of this peak.
Outcome measures: joint kinetics
Few studies have evaluated the kinetic parameters of gait during pregnancy. Foti et al. (2000) analysed the joint moments and joint powers with and without normalizing the weight of the women in late pregnancy. Although they found several changes in these parameters without normalization, the authors recommend the analysis with normalization (Foti et al., 2000). The analyses performed with normalized data found a significant increase in the hip extensors moment (Huang et al., 2002), and a significant decrease in the knee extensors moment (Huang et al., 2002) and in the ankle plantarflexors moment (Foti et al., 2000; Huang et al., 2002) in the sagittal plane. In the frontal plane, there was an increase of the hip abductors moment (Foti et al., 2000) and in the knee adductors moment (Huang et al., 2002).
Discussion
The purpose of this review was to analyse the available evidence on the biomechanical adaptations of gait that occur throughout pregnancy and in postpartum. Data from 9 follow-up studies were included in the analysis.
Women are subjected to various anatomical and physiological changes throughout pregnancy. However the adaptation strategies that are pursued are still unclear (Forczek & Staszkiewicz, 2012). Two of the situations they face are, on the one hand the reduction of energy costs associated with gait and, on the other hand, maximizing safety during the motor task. The later strategy seems to be dominant because the increase in step width is associated with a greater energy cost while walking (Donelan, Kram, & Kuo, 2001). This parameter has great consistency between studies. In addition, the development of pregnancy is associated with a reduction in stride length, which together allow the woman to have a larger base of support (Forczek & Staszkiewicz, 2012). Other way found by pregnant women to ensure greater body stability is keeping their feet on the ground for a longer time during the gait cycle and decreasing the single support time, which seems to be also a strategy to support the increased weight (Foti et al., 2000). In fact, the medial-lateral instability of the women as the pregnancy progresses is one result that seems to have great importance among different types of biomechanical parameters. However so far the medial-lateral component of the ground reaction forces show no significant changes, but tend to be higher in late pregnancy (Lymbery & Gilleard, 2005). This observation requires further research.
19
Much of the biomechanical changes occur in the pelvis or in adjacent joints. Although there are few kinematic changes in late pregnancy, most of it are related to the angular motion of the pelvis and the hip joint. The result with greater emphasis on studies is the anterior tilt of the pelvis. The position taken by the pelvis in late pregnancy seems to be a consequence of the weight of the uterus, placenta and foetus placed in the anterior zone of the body, and the weaker capacity to produce force by the rectus abdominis. However, the function of this anterior tilt and the increase of the lumbar lordosis is related to the maintenance of the trunk in an upright position (Foti et al., 2000). The decrease in the range of motion of the pelvis in the frontal and transverse planes, suggests that this may be a way to control the angular momentum caused by the increase of the moment of inertia of the trunk in late pregnancy (W. L. Gilleard, 2013). These changes bring consequences for the muscles attached to the pelvis, particularly a greater participation of the abductors and extensors muscles of the hip, which combined with a higher stretch derived from the anterior tilt of the pelvis, will contribute to lower back, pelvis, hip and sacroiliac pain (Foti et al., 2000; Huang et al., 2002). These types of pain are also associated with a decrease in the participation of the knee extensors and ankle plantarflexors (Huang et al., 2002). The changes in angular motion of the ankle may also be associated with other issues of pregnant women, including a decrease of dorsiflexion that is related to pain and higher probability to trip and fall (Hagan & Wong, 2010).
Limitations
The strength of this review is that a systematic methodology was adopted to identify relevant studies on the biomechanics of gait during pregnancy. However, the review has some limitations. Articles published in other languages than those mentioned above may have been excluded. The search was performed only in peer-reviewed published articles since 2000. There is a possibility of missing data published previously or other unpublished data, which were not included in the analysis. The small sample sizes and the different periods of data collection may have introduced some bias in the analysis performed. The lack of studies on this subject as well as the consistency of the outcome measures is a major limitation to perform a meta-analysis. Cautions should be taken when drawings conclusions about gait adaptations throughout pregnancy, due to the limitations mentioned above.
Conclusions
The evidence from this review suggests biomechanical adaptations of gait throughout pregnancy. Further research is required using common outcome measures and standard follow-up periods of data collection (weeks of gestation and postpartum period). Most of the results presented in this review are consistent between studies. However there is a great scarcity of studies addressing the gait biomechanics of pregnant women in a longitudinal perspective. There is a need to examine the kinematics of the woman closely while walking considering the beginning of pregnancy, in order to confirm the influence of morphological changes in the angular motion of the lower limb segments during the course of pregnancy.
Very few studies analysed the kinetics of gait of pregnant women. Nevertheless, these data are seen as essential to understand the magnitude and implications of changes in the welfare of women. In future research, there must be a special focus on the analysis of moments and joint powers to understand the changes in muscle participation, and if there are changes in the type of contraction during motor tasks.
It is not possible to understand the influence of morphological changes, if body composition and anthropometric variables are not quantified throughout pregnancy. Further research is required to understand to which extent these variables influence the biomechanical parameters.
No studies were found addressing the effects of physical activity, low back and pelvic pain or maternal weight control on the gait biomechanical adaptations of gait throughout pregnancy and postpartum.