ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Mortality
from
systemic
erythematosus
lupus
in
Brazil:
evaluation
of
causes
according
to
the
government
health
database
夽
Luisa
Ribeiro
Costi,
Hatsumi
Miyashiro
Iwamoto,
Dilma
Costa
de
Oliveira
Neves,
Cezar
Augusto
Muniz
Caldas
∗CentroUniversitáriodoEstadodoPará(CESUPA),Belém,PA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18August2016 Accepted10May2017
Availableonline9October2017
Keywords:
Systemicerythematosuslupus Mortality
Brazil
a
b
s
t
r
a
c
t
Objective:Tocharacterizethecausesofmortalityinpatientswithsystemiclupus erythe-matosus(SLE)inBrazilbetween2002and2011.
Methods:Anexploratoryecologicalstudy ofa timeseriesusingdatafromtheMortality InformationSystemofDATASUS,theDepartmentoftheUnifiedHealthSystem(Brazil’s NationalHealthSystem).
Results:Brazil’sSLEmortalityratewas4.76deaths/105inhabitants.Themortalityratewas
higherintheMidwest,NorthandSoutheastregionsthaninthecountryasawhole.There were6.3% fewerand 4.2%moredeathsthanexpectedinthe NortheastandSoutheast regions,respectively.Themeanageatdeathwas40.7±18years, and45.61%ofdeaths occurredbetweentheagesof20and39.Incidencewashighestinwomen(90.7%)andwhites (49.2%).Disordersofthemusculoskeletalsystemandconnectivetissuewerementionedas anunderlyingcauseofdeathin77.5%ofcases,anddiseasesofthecirculatorysystemand infectiousandparasiticdiseaseswerealsonotedinfewercases.SLEwasmentionedas anunderlyingcauseofdeathin77%ofcases,withnodifferencebetweentheBrazilian regions(p=0.2058).ThemainSLE-relatedcausesofdeathwere,sequentially,diseasesofthe respiratoryandcirculatorysystemsandinfectiousandparasiticdiseases.
Conclusions:Thisstudyidentifiedaneedforgreatercontrolofriskfactorsforcardiovascular diseasesandabetterunderstandingofthepathogenesisofatherosclerosisinSLE.Infectious causesarestillfrequent,andmanagementshouldbeimproved,especiallyintheearlystages ofthedisease.
©2017ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
WorkdevelopedattheCentroUniversitáriodoEstadodoPará(CESUPA),Servic¸odeReumatologia,Belém,PA,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.A.Caldas).
http://dx.doi.org/10.1016/j.rbre.2017.09.001
Mortalidade
por
lúpus
eritematoso
sistêmico
no
Brasil:
avaliac¸ão
das
causas
de
acordo
com
o
banco
de
dados
de
saúde
do
governo
Palavras-chave:
Lúpuseritematososistêmico Mortalidade
Brasil
r
e
s
u
m
o
Objetivo: Caracterizar as causas de mortalidade em pacientes comlúpus eritematoso sistêmico(LES)noBrasilentre2002e2011.
Métodos: EstudoecológicoexploratóriodeumasériecronológicacomdadosdoSistemade Informac¸õessobreMortalidadedoDepartamentodeInformáticadoSistemaÚnicodeSaúde (Datasus).
Resultados:AtaxademortalidadeporLESnoBrasilfoide4,76mortes/105habitantes.Ataxa demortalidadefoimaiornasregiõesCentro-Oeste,NorteeSudestedoquenopaíscomoum todo.Houve6,3%menose4,2%maismortesdoqueoesperadonasregiõesNordestee Sud-este,respectivamente.Amédiadeidadeaoóbitofoide40,7±18anose45,61%dosóbitos ocorreramentre20e39anos.Aincidênciafoimaiornasmulheres(90,7%)enosbrancos (49,2%).Osdistúrbiosdosistemamusculoesqueléticoedotecidoconjuntivoforam men-cionadoscomoacausasubjacentedemorteem77,5%doscasos;tambémforamobservadas doenc¸asdosistemacirculatórioeinfecciosaseparasitárias,emboraemmenorfrequência. OLESfoimencionadocomoacausasubjacentedeóbitoem77%doscasos,semdiferenc¸a entreasregiõesbrasileiras(p=0,2058).AsprincipaiscausasdemorteassociadasaoLES foram,emordem,doenc¸asdossistemasrespiratórioecirculatórioedoenc¸asinfecciosase parasitárias.
Conclusões: Esteestudoidentificouanecessidadedemaiorcontroledosfatoresderisco paradoenc¸ascardiovasculareseumamelhorcompreensãoda patogêneseda ateroscle-rosenoLES.Ascausasinfecciosasaindasãofrequenteseomanejodevesermelhorado, especialmentenosestágiosiniciaisdadoenc¸a.
©2017ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Systemiclupuserythematosus(SLE),achronicautoimmune disease whose etiology is not fully known, is diagnosed basedonclinicalandlaboratorycriteriaandprobablyresults fromtheinteractionofgenetic,hormonal,environmentaland infectiousfactorsthatleadtothelossofimmunological toler-ancewiththeproductionofautoantibodies.1
According to the literature, mortality in SLE follows a bimodalpattern:intheearlystages,deathismainlycaused byinfection,followedbysevererenalorcentralnervous sys-tem(CNS)activity,whileinthemoreadvancedstagesofthe disease,thereisanincreaseinmortalityfromcardiovascular diseasesassociatedwithatherosclerosis,partiallyrelatedto corticotherapyandchronicinflammation.1,2
According to the Ministry of Health, the death certifi-cate is the standard document for collecting information on mortality and is the source of vital and epidemiologi-calstatisticsinBrazil.3Thecausesofdeathtoberegistered
on the international death certificate are all those dis-eases, morbid conditions or injuries that either resulted in or contributed to death and the circumstances of the accidentorviolencethatproducedanysuchinjuries. Under-lying Cause of Death is defined as the disease or injury thatinitiatedthetrainofmorbideventsleadingdirectly to death.3
The Conditions and Causes of Death section of the death certificate is in accordance with the international
deathcertificate model adoptedbythe World Health Orga-nization (WHO),whichisextremelyimportantgiventhat it containstheunderlyingcauseandinjuriesleadingtodeath.It isdividedintotwoparts.PartIisforreportingthedirectcause ofdeath(immediatecause–line A)and themorbid condi-tionsthatledtothecauseregisteredinlineA(antecedentor sequentialcauses–linesBandC,andtheunderlyingcause –lineD).PartIIisforreportingcontributingcausesthatwere notpartofthechaindefinedinPartI,includinganydiseasesor injuriesthatcontributedtodeathbutwerenotdirectlyrelated tothepathologicalstateleadingtodeath.3
In Brazil,withits size and thedifferent levels of socio-economicdevelopmentinitsvariousregions,aswellasthe differentlevelsoforganizationandproblem-solving capabil-itiesofhealthassistancenetworks,thecauses ofmortality may vary according to region and may reflect differences incareand accesstohealthservicesbetweenregions.This study therefore aims to determine the causes of mortal-ity inSLEpatientsinBrazil,accordingtoregion, from2002 to2011.
Patients
and
methods
(DATASUS),4whichiswhyitwasnotnecessarytosubmitthis
studytotheHumanResearchEthicsCommitteeforapproval. ThedatabasewaspreparedusingTabWin®.
Theselectedvariablesweretheregionwherethepatient lives(North,Northeast,Midwest,SouthandSoutheast), gen-der(maleorfemale),race(mixedrace,white,black,eastAsian andindigenous),ageandunderlyingandsequentialcausesof deathrecordedintheyearsofthehistoricalseries.
Thisstudyconsideredastheunderlyingcauseofdeathall thecausesofdeathregisteredassuchinaccordancewiththe TenthRevisionoftheInternationalClassificationofDiseases (ICD-10)andavailableinDATASUS.
SLEisadiseasedescribedinChapterXIIIofICD-10,called “DiseasesoftheMusculoskeletalSystemandConnective Tis-sue”(M00toM99).5
Thedatacollectedincluded informationfromthe death certificatesofpatientsaged15andoverandwhosePartI(lines, a, b,c and d) or IIof theConditions and Causes ofDeath section included disease M32 - SLE and its sub-categories (M32.0–Drug-inducedsystemiclupuserythematosusM32.1– Systemiclupuserythematosuswithorganorsystem involve-ment;M32.8–Otherformsofsystemiclupuserythematosus; and M32.9 – Systemic lupus erythematosus, unspecified).5
Deathcertificatesthatdidnotmentionagewereexcluded. Thepopulationsofthestatesandregionsasdisclosedby DATASUS,whicharebasedoncensusandintercensus data publishedbytheBrazilianInstituteofGeographyand Statis-tics(IBGE),6wereusedtocalculatetheincidencerate,while
theaveragepopulationinthetwomiddleyearsofthe stud-iedperiod(2006and2007)wasusedtocalculatetheaverage incidenceintheperiod.
Statisticalanalysiswascarriedoutusingdescriptiveand inferential statistical methods. The number of expected deathsforeachregionwascalculatedbyassumingtheaverage Brazilianpopulationinthehistoricalseriesasthestandard population under absolute risk in each region. Quantita-tivevariables had an average standard deviation of ±1.96, were submittedtothe D’Agostino normality testand were comparedusing the Ztest. Qualitative variables were ana-lyzedintermsofabsoluteandrelativefrequencies,andtheir distributionwasevaluatedusingtheChi-squaretest.A signif-icancelevelof˛<5%wasestablishedbeforehandtorejectthe
nullhypothesis.Statisticalprocessingwasperformedusing BioEstat®version5.3andGrafTable®version2.0.
Table2–Distributionbygender,raceandageatdeathof patientswithsystemiclupuserythematosusinBrazil between2002and2011.
Variables n=8761 %
Gender
Male 812 9.3
Female 7949 90.7a
Race
White 4310 49.2a
Mixedrace 2917 33.3
Black 815 9.3
Yellow 44 0.5
Indigenous 9 0.1
Notreported 666 7.6
Age
15–19 789 9.01
20–39 3996 45.61a
40–59 2888 32.96
60–79 955 10.90
80andover 133 1.52
Source:MortalityInformationSystem(SIM)oftheITDepartmentof theUnifiedHealthSystem–DATASUS.
a p-Value<0.0001,Chi-squaretestofgoodnessoffit.
Results
Thisstudyidentified8761reportsofdeathsofSLEpatients inBrazil,givinga specificmortalityrateof4.76 deaths/105
inhabitants.TheMidwest,NorthandSoutheastregionshad rates of 6.44, 5.4 and 5.23 deaths/105 inhabitants,
respec-tively, which were above the Brazilian average. Thelowest rate of mortality from SLE was found in the Northeast region (3.69/105 inhabitants), and the present study
identi-fied a statistically significant difference (p<0.0001) of6.3% fewerdeathsthanexpectedinthisregion,whilethe South-eastregionhad4.2%moredeathsthanexpected(p<0.0001) (Table1).
Table 2shows asignificant predominance (p<0.0001)of women(90.7%),whites(49.2%)andthoseagedbetween20and 39years(45.61%).
Between 2002and2011,thenationalmean ageatdeath was 40.7±18 years, with significant differences from this mean (p<0.0001)inthe North (34.1±13.7years) andSouth
Table1–Distributionofobservedandexpecteddeathsofpatientswithsystemiclupuserythematosusbyregion between2002and2011.
Region Deaths/100,000inhabitants Observeddeaths(n) Observed(%) Expected(%) Dif.(%)
Brazil 4.76 8761 100.0 100.0 0.0
North 5.40 789 9.0 7.9 1.1
Northeast 3.69 1902 21.7 28.0 −6.3a
Southeast 5.23 4076 46.5 42.3 4.2a
South 4.28 1143 13.0 14.5 −1.5
Midwest 6.44 851 9.7 7.2 2.5
(44.7±17years)regions.IntheNortheast,Southeastand Mid-westregions,themeansageatdeathwere37.1±15.1years, 42.9±20yearsand38.8±15.3years,respectively.
InSLEpatients,theICD-10group“Disordersofthe Mus-culoskeletalSystemandConnectiveTissue”(6794)accounted for77.5%ofunderlyingcausesofdeath,withastatistically sig-nificantdifference(p<0.0001)inrelationtotheotherrecorded underlyingcausesofdeathinthesepatients.SLE(M32),asone ofthediseasesthatispartofthisICD-10group,represented approximately100%(6745)ofallrecordsofunderlyingcause ofdeathinthisgroup.SLEaloneaccountedfor77%ofrecords ofunderlyingcauseofdeath(6745/8761)amongthetotal num-berofdeaths ofpatients withthis disease.There was not astatisticallysignificant difference(p=0.2058) betweenthe percentageofdeathsclassified asM32amongthe Brazilian regions(Table3).
OtherunderlyingcausesofdeathrecordedforSLEpatients included circulatorysystem (6.0%), infectious and parasitic
(2.8%),respiratorysystem(2.2%),digestivesystem(2.1%)and genitourinarysystem(1.9%)diseases(Table3).
Table 3 shows that the predominance of records was not uniformacross the regions exceptforthose related to thecirculatorysystemandinfectiousandparasiticdiseases. Although the Southeast region had the lowest percentage ofcases ofSLEwithSLEas the underlyingcause ofdeath (74.3%=3030/4076),itaccountedfor46.5%(4076/8761)oftotal deathsofSLEpatients inthe country,aswell asthe high-estproportionofmostconditionsrecordedastheunderlying causeofdeath.
Thedistributionofsequentialcausesofdeathrelatedto SLE(Table4)showedhighlysignificantdifferences(p<0.0001) for respiratory system (26.4%), circulatory system (20.7%), infectious and parasitic (18.9%) and genitourinary system (14.7%)diseases.
The comparison of sequential causes between regions (Table5)showedapredominanceofdiseasesoftherespiratory
Table3–Distributionofcausesofdeathofpatientswithsystemiclupuserythematosus(SLE)byBrazilianregionbetween 2002and2011.
ICDGroup MW NE N SE S Total
n % n % n % n % n % n %
Musculoskeletalsystem andconnectivetissue
677 79.6 1471 77.3 629 79.7 3056 75.0 961 84.1 6794 77.5a
SLE 670 98.9 1467 99.7 625 99.4 3030 99.1 953 99.2 6745 99.3b
Otherdisordersofthe musculoskeletal systemand connectivetissue
7 1.1 4 0.3 4 0.6 26 0.9 8 0.8 49 0.7
Circulatorysystem 58 6.8 99 5.2 31 3.9 281 6.9 60 5.2 529 6.0
Infectiousandparasitic diseases
23 2.7 96 5.1 35 4.4 158 3.9 19 1.7 331 2.8
Respiratorysystem 13 1.5 38 2.0 11 1.4 112 2.7 21 1.8 195 2.2
Digestivesystem 16 1.9 40 2.1 16 2.0 99 2.4 17 1.5 188 2.1
Genitourinarysystem 17 2.0 38 2.0 19 2.4 83 2.0 6 0.5 163 1.9
Immunedisorders 11 1.3 36 1.9 7 0.9 79 1.9 13 1.1 146 1.7
Endocrine,nutritional andmetabolic diseases
7 0.8 34 1.8 18 2.3 62 1.5 7 0.6 128 1.5
Neoplasms 9 1.1 14 0.7 7 0.9 73 1.8 20 1.7 123 1.4
Nervoussystem 6 0.7 12 0.6 6 0.8 30 0.7 9 0.8 63 0.7
Musculoskeletaland connectivetissue
7 0.8 4 0.2 4 0.5 26 0.6 8 0.7 49 0.6
Skinandsubcutaneous tissue
4 0.5 5 0.3 7 0.9 21 0.5 3 0.3 40 0.5
Pregnancy,childbirth, andthepuerperium
7 0.8 14 0.7 3 0.4 13 0.3 6 0.5 43 0.5
Congenital malformations
1 0.1 2 0.1 0 0 2 0 0 0 5 0.1
Othergroups 1 0.1 1 0.1 0 0 5 0.1 0 0 5 0.1
Mentaldisorders 1 0.1 0 0 0 0 2 0 1 0.1 4 0
Eye,earandmastoid process
0 0 2 0.1 0 0 0 0 0 0 2 0
Total 851 100 1902 100 789 100 4076 100 1143 100 8761 100
Source:MortalityInformationSystem(SIM)oftheITDepartmentoftheUnifiedHealthSystem–DATASUS. MW,Midwest;NE,Northeast;N,North;SE,Southeast;S,South.
a ICDGroups(p-value<0.0001),Chi-squaretest.
Table4–Distributionofthesequentialcausesrecordedindeathcertificatesofpatientswithsystemiclupus erythematosusastheunderlyingcauseofdeathinBrazilbetween2002and2011.
Sequentialcause No.ofrecords % No.ofrecords/6745
Respiratorysystem 5081 26.4 75.3a
Circulatorysystem 3989 20.7 59.1
Infectiousandparasiticdiseases 3823 19.9 56.7
Genitourinarysystem 2821 14.7 41.8
Immunedisorders 823 4.3 12.2
Digestivesystem 809 4.2 12.0
Endocrineandmetabolicdiseases 735 3.8 10.9
Nervoussystem 380 2.0 5.6
Musculoskeletalsystemandconnectivetissue 233 1.2 3.5
Skinandsubcutaneoustissue 226 1.2 3.4
Neoplasms 187 1.0 2.8
Mentaldisorders 65 0.3 1.0
Pregnancy,childbirth,andthepuerperium 64 0.3 0.9
Congenitalmalformations 10 0.1 0.1
Eye,earandmastoidprocess 7 0.0 0.1
Total 19,253 100
Source:MortalityInformationSystem(SIM)oftheITDepartmentoftheUnifiedHealthSystem–DATASUS. a p-Value<0.0001,Chi-squaretestofgoodnessoffit.
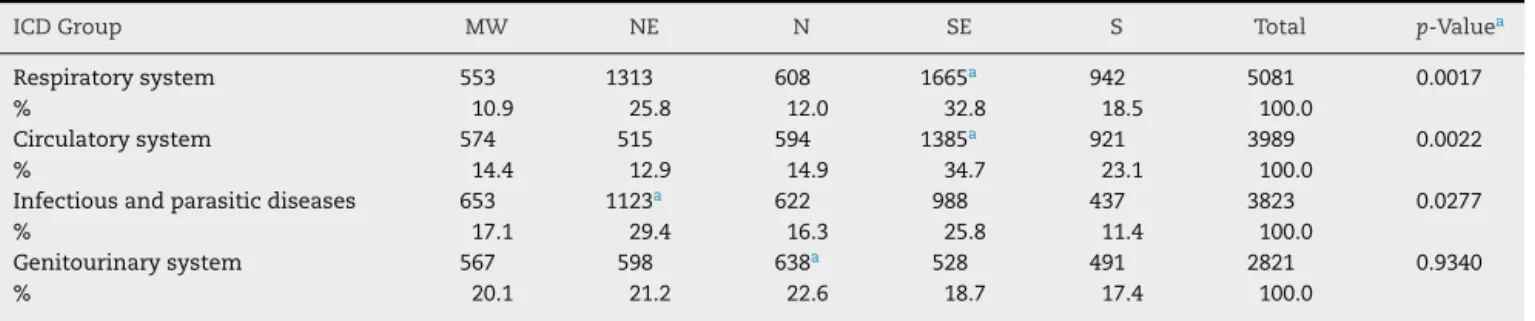
Table5–MainsequentialcausesofdeathfromsystemiclupuserythematosusbyBrazilianregionbetween2002and 2011.
ICDGroup MW NE N SE S Total p-Valuea
Respiratorysystem 553 1313 608 1665a 942 5081 0.0017
% 10.9 25.8 12.0 32.8 18.5 100.0
Circulatorysystem 574 515 594 1385a 921 3989 0.0022
% 14.4 12.9 14.9 34.7 23.1 100.0
Infectiousandparasiticdiseases 653 1123a 622 988 437 3823 0.0277
% 17.1 29.4 16.3 25.8 11.4 100.0
Genitourinarysystem 567 598 638a 528 491 2821 0.9340
% 20.1 21.2 22.6 18.7 17.4 100.0
Source:MortalityInformationSystem(SIM)oftheITDepartmentoftheUnifiedHealthSystem–DATASUS. MW,Midwest;NE,Northeast;N,North;SE,Southeast;S,South.
a Comparisonbetweentheregions:Chi-squaretest.
system (32.8%) and the circulatory system (34.7%) in the Southeast,withstatisticallysignificantdifferencesinrelation totheotherregions(p<0.0017andp<0.0022,respectively).For infectiousandparasiticdiseases,theNortheastaccountedfor thehighestnumberofrecords(29.4%),andthisdifferencewas statisticallysignificant(p<0.0277).Inregardtodiseasesofthe genitourinarysystem,therewerenodifferencesbetweenthe regions(p=0.9340),althoughthehighestproportionofcases occurredintheNorth(22.6%).
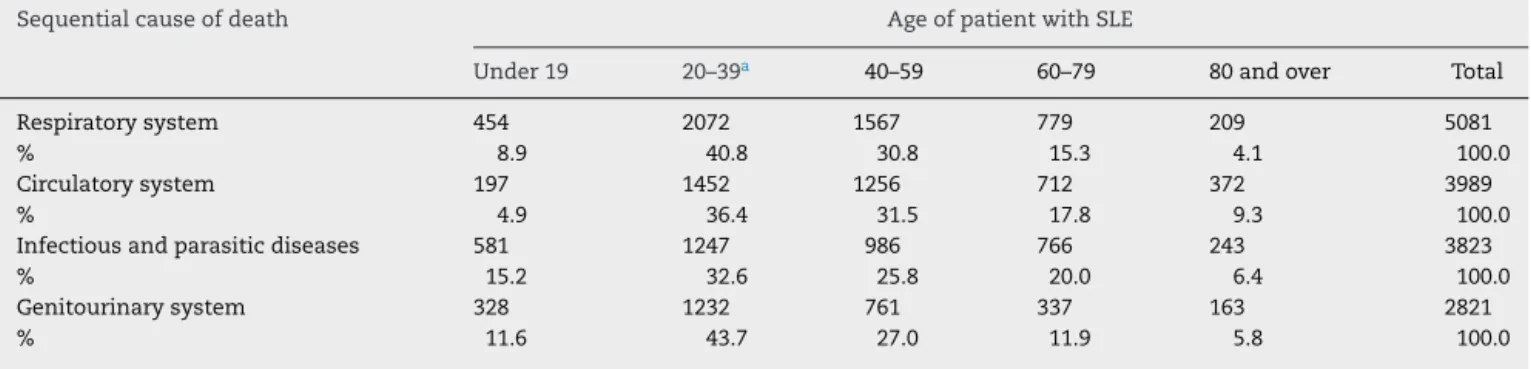
Anevaluationofthedistributionofthemainsequential causes by age (Table 6) showed a decline in the propor-tion ofdiseases ofthe respiratory system inpatients over 80 years of age, while patients between 20 and 39 years old (p<0.0001) accountedforthe largest shareofthe main groupsofsequentialcauses.Morethan60%ofthesegroups ofcauseswereidentifiedinpatientsbetween20and59years ofage.
Discussion
The mortality rate of SLE patients in Brazil is 4.76 deaths/100,000 inhabitants,andthereisapredominanceof women and whites in this group of patients. Differences betweentheregionsareevident,withtheSouthand South-eaststateshavinglowermortalityandtheNorthregionhaving higher mortality.Itisworthnotingthe differencefoundin relationtoapopulationstudyconductedinNorway,where mortalitywasamereonedeathper100,000inhabitants.7
The North region had the lowest mean age at death (34.1±13.7 years) of all Brazilian regions, similar to that recordedinSaudiArabia(33±18years).8Ontheotherhand,
Table6–MainsequentialcausesofdeathfromsystemiclupuserythematosusbyageinBrazilbetween2002and2011.
Sequentialcauseofdeath AgeofpatientwithSLE
Under19 20–39a 40–59 60–79 80andover Total
Respiratorysystem 454 2072 1567 779 209 5081
% 8.9 40.8 30.8 15.3 4.1 100.0
Circulatorysystem 197 1452 1256 712 372 3989
% 4.9 36.4 31.5 17.8 9.3 100.0
Infectiousandparasiticdiseases 581 1247 986 766 243 3823
% 15.2 32.6 25.8 20.0 6.4 100.0
Genitourinarysystem 328 1232 761 337 163 2821
% 11.6 43.7 27.0 11.9 5.8 100.0
Source:MortalityInformationSystem(SIM)oftheITDepartmentoftheUnifiedHealthSystem–DATASUS. a p<0.0001,Chi-squaretestofindependence.
In2010, astudy10 waspublished analyzingmortality in
SLEpatientsinSãoPaulostate,inBrazil’sSoutheastregion, between1985and2004.Accordingtothisstudy,themeanage atdeathinthis periodwas35.1±15.0years,allowingusto inferthattherehasbeenanimprovementinthesurvivalof SLEpatientsinrecentyearsgiventhatthemeanageatdeath washigherthanthis figureinBrazilasawholeandinthe South,SoutheastandMidwestregions.Ontheotherhand,it underlinesthediscrepancybetweenBrazilianregions,given thatthemeanageatdeathfromSLEintheNorthand North-eastregionshasbeenlowerthanthatinSãoPaulostatefor morethantenyears.
The number of deaths in the Northeast and Southeast regions was respectively lower and higher than expected. According to the United Nations Development Programme (UNDP),11 the states with municipalities having the
low-est Municipal Human Development Indices (MHDI) in the country are located the North and Northeast regions. As a result, it is necessary to be cautious when comparing mortality in the different Brazilian regions due to defi-ciencies in the service network currently available to the population in the North and Northeast regions. Accord-ing to information provided by the IBGE,12 the North and
Northeastregionshaveproblemsrelatedtothereportingof deathsin general, withhigh under-reporting rates. Under-reporting is extremely high in the Northeast (more than 26%) compared withthe national average (12%)and espe-cially with the Center-South (under 10%). This difference can explain why the number of deaths was lower than expectedintheNortheast andhigherthan expectedinthe Southeast.
AnanalysiscarriedoutinMorocco13reportedthatthe
epi-demiologyofSLEindevelopingcountriesisstillunknownand isprobably underestimated,making it difficult tocompare datawithotherinternationalstudies.MostBrazilianstudies arerestrictedtotheSoutheastregion.14–16
InoneofthefewBrazilianstudiescarriedoutoutsidethe Southeastregion,ananalysisof63 SLEpatients monitored inParaíba state, inBrazil’s Northeast region, established a relationshipbetweenpoorerqualityoflife,measuredatthe beginningofthestudy,andahigherlikelihoodofdeathafter asecond analysissixyearslater.Ofthedeathsobservedin that study,two were caused bysystemic infection,two by
renalcomplicationsandtwobySLE-relatednervoussystem complications.17
Areviewpublishedin201418emphasizedthatSLEpatients
inemergingcountries,suchasBrazil,hadaworseprognosis asaresultofthelowsocioeconomicandeducationallevelof thesepopulations,inadditiontodelayindiagnosis,difficulties accessinghealthservicesandmorefrequentinfections and diseasecomplications.
SLEaffectsmorewomenthanmen,witharatioof10:1.19
However, according to studies carried out in the United Kingdom,20SaudiArabia8andintheUnitedStates,21aswell
asbymultinationalteams,22mortalityfromSLEishigherin
men.Thedisagreementwiththefindingsofthepresentstudy mayhavebeencausedbytheuseofdeathrecords,whichdid notallowfortheassessmentoftheprevalenceofthedisease inthepopulationoritslethalitybygender.
The main underlyingcause of deathobserved was SLE itself, whichis consistent withthe findings of aEuropean study.9Diseasesofthecirculatorysystem,includingalltypes
ofheart,vesselandcerebrovasculardiseases,werethesecond mostcommonunderlyingcauseofdeath,inlinewithother studies.19,23–25
Acomplexinteractionofseveralfactors,includingthe dis-ease’schronicinflammatorynature,contributestoSLEbeing a risk factor for cardiovascular events. Inflammatory and immunologicalmechanismsareresponsibleforboththe for-mationofatheroscleroticplaquesandtheirinstability,which maycauseruptures,thrombosesandvesselocclusion, lead-ing toischemiaand tissueinfarction.26 Renalinvolvement,
whichisfrequentlypresent,contributestothedevelopment of premature coronary artery disease.Traditional risk fac-tors, suchas high blood pressure and hyperlipidemia,are common in lupuspatients due todisease activity and the useofglucocorticoids.27Theseconditionsareinadditionto
endothelialdysfunctionandantiphospholipidantibodies,also implicatedinacceleratedatherosclerosisinSLE.28Theoverall
resultishighprematuremortalityfromdiseasesofthe circu-latorysystem,asobservedinaFinnishstudyinwhich37% ofdeathsofSLEpatients wereattributed tocardiovascular causes.29
among the most important in that region, in addition to renal failure and infectious causes led bypneumonia and septicemia.15
Theresultsregardinginfectiousandparasiticdiseasesasa causeofdeathinpatientswithSLEwereinlinewiththeresults ofaEuropeanstudy.9InaBrazilianstudy30thatevaluated113
autopsiesofSLEpatients,infectionwasthecauseofdeathin 58%ofthecases.Itiswellestablishedintheliteraturethat infections,usuallyattributedtotheuseof immunosuppress-ivedrugs,areafrequentcauseofdeathinSLEpatients.22The
incidenceofinfectionsinpatientswithSLEvariesbetween 50and150episodesforevery100patients/year31;themost
common sites are the respiratory, digestive and urinary tracts19;andthemostfrequentetiologicalagentsarefungi,
Gram-negative bacteria, and opportunistic agents, such as pneumocystispneumonia,cytomegalovirusandmembersof theHerpesviridaefamily.32
Disease activity was identified as an independent risk factorforinfections.33,34Theclinicalhematological
manifes-tationsofSLE,suchaslymphopeniaandneutropenia,aswell as the treatment itself,are also risk factors for infectious diseases.35Glucocorticoidsexerttheiranti-inflammatoryand
immunosuppressive effects through several mechanisms, suchasinterferenceinthefunctioningofleukocytes, fibro-blastsandendothelialcells,aswellasreductioninthenumber ofcirculatingmonocytesandmacrophages.Theintensityof theseeffectsisproportionaltothedosageandtheduration ofthetreatment, and it isnotclearifthere isathreshold belowwhichthesedrugsareconsideredsafe.36Antimalarial
drugs,ontheotherhand,reducetheoccurrenceofinfections. Bothchloroquineandhydroxychloroquinehaveantibacterial, antifungaland antiviral effects in addition totheir known antiparasiticactivity.33
In Minas Gerais, a state in Brazil’s Southeast region, a prospective observational study that analyzed 179 SLE patients during 3.3 years observed a higher frequency of deathsinthispopulationthaninthegeneralpopulation, espe-ciallydeathsrelatedtoinfectionsandSLEitself.16
Due to the clinical relevance of infections in SLE, it is necessarytoadoptpreventivemeasures.Vaccinationisthe most important of these preventive measures and should beperformedinperiodswhen thedisease isstable, avoid-ing the BCG and live virus vaccines.33 Although slightly
weakimmuneresponseshavebeen observed,theyare still effective.33,37–39
DeathsfrominfectionarestillhigherinSLEpatientsthan inthegeneralpopulation;however,inrecentyears,therehas beenadeclineintotalSLEmortality,andthisdeclinehasbeen associatedwithareductioninthecasesofinfectionandrenal problems,15althoughtheproportionofdeathswithdiseases
ofthe circulatory system asa sequentialcause have been increasing.22
Patients with SLE have a higher chance of developing malignanciesthandoesthegeneralpopulation.19Inastudy
involving23collaboratingcentersfromsevencountries,22
can-ceraccountedformoredeathsthaninfectiousdiseasesand wassecondonlytocardiovasculardiseases;themostfrequent typeswerenon-Hodgkinlymphomaandlungcancer.Inthe presentstudy,itwasnotpossibletoevaluatetheassociation
betweenSLEandmalignanciesduetotheuseofcauses clas-sifiedaccordingtoICD-10groupsinthemethodology.
The main causes of mortality resulting from SLE were diseases of the respiratory and circulatory systems, infec-tiousandparasiticdiseases,anddiseasesofthegenitourinary system.Thesefindings aresimilartotheresultsofanother study15inwhichthemainsequentialcauseswererelatedto
the circulatory,respiratory,digestiveandgenitourinary sys-temsandtocertaininfectiousdiseases.
AccordingtostudiescarriedoutintheUnitedStates40,41
andinTunisia,42inemergingcountriesandethnicminorities,
SLE tends to bemore severe and moresymptomatic. Dis-easeactivityratesarehigher,leadingtoaccelerateddamage accrualintargetorgansandhighermortality.
In lupus patients ofAsian ethnicity evaluated ina U.S. study,43theprevalenceofnephritiswashigh,rangingbetween
45%and75%,andthemortalityratewasthreetimeshigher thanthatofwhitepatients.
AMoroccanstudyraisedaquestionaboutthe discrepan-ciesinseverityandmortalitybetweenminoritygroupsand whiteindividuals.Itquestionedwhethertheaggressive symp-tomsinethnicminoritiescan,infact,beexplainedbygenetic riskfactorsorbiologicaldifferencesorwhethertheysimply reflectthesocioeconomicdifferencesbetweenthesegroups andwhitepeople.13
Diseases of the circulatory system and infections were morefrequentlymentionedinthedeathsofpatientsoverthe ageof50years.15Respiratorysysteminvolvementcanoccur
atsomestageofthediseaseinmorethan50%ofpatients,who canpresentpleurisy,pneumonitis,interstitiallungdiseaseor pulmonaryhypertension.44
Itisthusclearthatthereisaneedformoreeffectivecontrol oftheriskfactorsforcardiovasculardiseases,bothtraditional riskfactorsandthoserelatedtoSLEtreatmentandactivity; additionally, a betterunderstanding ofthepathogenesisof atherosclerosisinthisdiseaseisneeded.Infectiousdiseases arestillveryfrequent,underliningthefactthattherehasnot beenappropriatecontrolofriskfactors,especiallyintheearly stagesofSLE,andthathealthprofessionalsneedtofocusmore onpreventionwithvaccines.
Conclusion
In Brazilian SLEpatients, SLEitself was cited asthe main underlying cause of death, followed by diseases of the circulatorysystem,infectiousandparasiticdiseasesand dis-easesoftherespiratory,digestiveandgenitourinarysystems, whichtogetheraccountedfortheapproximately23%ofthe cases in which lupus was not identified as the underly-ingcause.Therearealsoimportantdifferencesbetweenthe studied regions, and it is important to take into consid-eration the under-reporting and socioeconomic differences amongthem.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. AssisMR,BaakliniCE.Lúpuseritematososistêmico.RevBras Med.2009;66:274–85.
2. VossA,LaustrupH,HjelmborgJ,JunkerP.Survivalinsystemic erythematosuslupus,1995–2010.Aprospectivestudyina Danishcommunity.Lupus.2013;22:1185–91.
3. MinistryofHealth.HealthSurveillanceSecretariat. DepartmentofAnalysisoftheHealthStatus.Instructions ManualforFillinginDeathCertificates.Brasília/DF;2011. 4. DATASUS.MortalityInformationSystem.Availablefrom:
ftp://ftp.datasus.gov.br/dissemin/publicos/SIM/CID10/DORES
[accessed13.04.13].
5. WorldHealthOrganization.BrazilianCenterofClassification ofDiseases.InternationalStatisticalClassificationofDiseases andRelatedHealthProblems.10threvision–ICD-10,vol.1; 1997.p.605–52.
6. DATASUS.Demographicdata.Availablefrom:
http://www.datasus.gov.br[accessed13.04.13].
7. LerangK,GilboeIM,SteinarThelleD,GranJT.Mortalityand yearsofpotentiallifelossinsystemicerythematosuslupus:a population-basedcohortstudy.Lupus.2014;23:1546–52.
8. HellerT,AhmedM,SiddiqqiA,WallrauchC,BahlasS. SystemicerythematosuslupusinSaudiArabia:morbidity andmortalityinamultiethnicpopulation.Lupus.2007;16: 908–14.
9. CerveraR,KhamashtaMA,FontJ,SebastianiGD,GilA,Lavilla P,etal.Morbidityandmortalityinsystemiclupus
erythematosusduringa10-yearperiod.Medicine(Baltimore). 2003;82:299–308.
10.SouzaDC,SantoAH,SatoEI.Trendsinsystemic
erythematosuslupusmortalityratesinthestateofSaoPaulo, Brazilfrom1985to2004.ClinExpRheumatol.2010;28:519–24.
11.UnitedNationsDevelopmentProgramme(PNUD).MHDI RankingofFederationUnits2010.Availablefrom:
http://www.pnud.org.br/atlas/ranking/Ranking-IDHM-UF-2010.aspx[accessed10.02.13].
12.MinistryofPlanning,Budget,andManagement.Brazilian InstituteofGeographyandStatistics.Socio-demographicand HealthIndicatorsinBrazil;2009.
13.MezalekZT,BonoW.Challengesforlupusmanagementin emergingcountries.PresseMed.2014;43:209–20.
14.SouzaDC,SantoAH,SatoEI.Mortalityprofilerelatedto systemicerythematosuslupus:amultiplecause-of-death analysis.JRheumatol.2012;39:496–503.
15.SouzaDC,SantoAH,SatoEI.Mortalityprofilerelatedto systemiclupuserythematosus:amultiplecause-of-death analysis.JRheumatol.2012;39:496–503.
16.TellesRW,LannaCC,SouzaFL,RodriguesLA,ReisRC,Ribeiro AL.CausesandpredictorsofdeathinBrazilianlupus patients.RheumatolInt.2013;33:467–73.
17.FreireE,BruscatoA,CiconelliR.Qualityoflifeinsystemic erythematosuslupuspatientsinNortheasternBrazil:is health-relatedqualityoflifeapredictorofsurvivalforthese patients?ActaReumatolPort.2009;34:207–11.
18.TaziMezalekZ,BonoW.Challengesforlupusmanagementin emergingcountries.PresseMed.2014;43Pt2:e209–20.
19.IppolitoA,PetriM.Anupdateonmortalityinsystemic erythematosuslupus.ClinExpRheumatol.2008;26Suppl 51:S72–9.
20.ReesF,DohertyM,GraingeMJ,LanyonP,DavenportG,Zhang W.MortalityinsystemicerythematosuslupusintheUnited Kingdom1999–2012.Rheumatology(Oxford).2016;55:854–60.
21.AndradeRM,AlarcónGS,FernándezM,ApteM,ViláLM, ReveilleJD.Accelerateddamageaccrualamongmenwith systemiclupuserythematosus.ArthritisRheum. 2007;56:622–30.
22.BernatskyS,BoivinJF,JosephL,ManziS,GinzlerE,Gladman DD,etal.Mortalityinsystemicerythematosuslupus. ArthritisRheum.2006;54:2550–7.
23.MokCC,KwokCL,HoLY,ChanPT,YipSF.Lifeexpectancy, standardizedmortalityratiosandcausesofdeathinsix rheumaticdiseasesinHongKong,China.ArthritisRheum. 2011;63:1182–9.
24.BartelsCM,BuhrKA,GoldbergJW,BellCL,VisekrunaM, NekkantiS,etal.Mortalityandcardiovascularburdenof systemicerythematosuslupusinaUSpopulation-based cohort.JRheumatol.2014;41:680–7.
25.ThomasG,ManciniJ,Jourde-ChicheN,SarlonG,AmouraZ, HarléJR,etal.Mortalityassociatedwithsystemic
erythematosuslupusinFranceassessedby
multiple-cause-of-deathanalysis.ArthritisRheumatol. 2014;66:2503–11.
26.LibbyP,OkamotoY,RochaVZ,FolcoE.Inflammationin atherosclerosis:transitionfromtheorytopractice.CircJ. 2010;74:213–20.
27.NikpourM,GladmanDD,UrowitzMB.Prematurecoronary heartdiseaseinsystemicerythematosuslupus:whatrisk factorsdoweunderstand?Lupus.2013;22:1243–50.
28.HaqueS,BruceIN.Cardiovascularoutcomesinsystemic erythematosuslupus:bigstudiesforbigquestions.J Rheumatol.2009;36:467–9.
29.ElfvingP,PuolakkaK,KautiainenH,VirtaLJ,PohjolainenT, Kaipiainen-SeppänenO.Mortalityandcausesofdeath amongincidentcasesofsystemicerythematosuslupusin Finland2000–2008.Lupus.2014;23:1430–4.
30.IriyaSM,CapelozziVL,CalichI,MartinsMA,LichtensteinA. Causesofdeathinpatientswithsystemicerythematosus lupusinSaoPaulo,Brazil:astudyof113autopsies.Arch InternMed.2001;161:1557.
31.Hidalgo-TenorioC,Jiménez-AlonsoJ,LunaJD,TalladaM, Martínez-BrocalA,SabioJM.Urinarytractinfectionsand erythematosuslupus.AnnRheumDis.2004;63:431–7.
32.FerreiraM,SalgueiroAB,EstradaJ,RamosJ,VenturaL,Vale MC,etal.Lúpuseritematososistêmico.ActaMedPort. 2008;21:199–204.
33.DanzaA,Ruiz-IrastorzaG.Infectionriskinsystemic erythematosuslupuspatients:susceptibilityfactorsand preventivestrategies.Lupus.2013;22:1286–94.
34.BoschX,GuilabertA,PallarésL,CerveralR,Ramos-CasalsM, BovéA,etal.Infectionsinsystemicerythematosuslupus:a prospectiveandcontrolledstudyof110patients.Lupus. 2006;15:584–9.
35.JanoudiN,BardisiES.Haematologicalmanifestationsin systemicerythematosuslupus.Availablefrom:
http://cdn.intechopen.com/pdfs-wm/33017.pdf[accessed 13.04.13].
36.Ruiz-IrastorzaG,DanzaA,KhamashtaM.Glucocorticoiduse andabuseinSLE.Rheumatology.2012;51:1145–53.
37.AssenSV,Agmon-LevinN,ElkayamO,CerveraR,DoranMF, DougadosM,etal.EULARrecommendationsforvaccination inadultpatientswithautoimmuneinflammatoryrheumatic diseases.AnnRheumDis.2011;70:414–22.
38.MoscaM,TaniC,AringerM,BombardieriS,BoumpasD,Brey R,etal.EuropeanLeagueAgainstRheumatism
recommendationsformonitoringpatientswithsystemic erythematosuslupusinclinicalpracticeandinobservational studies.AnnRheumDis.2010;69:1269–74.
39.BühlerS,EperonG,RibiC,KyburzD,vanGompelF,VisserLG, etal.Vaccinationrecommendationsforadultpatientswith autoimmuneinflammatoryrheumaticdiseases.SwissMed Wkly.2015;145:w14159.
studyofethnicdisparitiesinSLE.ArthritisRheum. 2007;57:576–84.
41.Gómez-PuertaJA,BarbhaiyaM,GuanH,FeldmanCH,Alarcón GS,CostenbaderKH.Racial/Ethnicvariationinall-cause mortalityamongUnitedStatesMedicaidrecipientswith systemicerythematosuslupus:aHispanicandAsian paradox.ArthritisRheumatol.2015;67:
752–60.
42.KhanfirMS,HoumanMH,CherifE,HamzaouiA,SouissiS, GhorbelIB,etal.TULUP(TUnisianLUPus):amulticentric
studyofsystemicerythematosuslupusinTunisia.IntJ RheumDis.2013;16:539–46.
43.MokCC,MakA,ChuWP,ToCH,WongSN.Long-termsurvival ofsouthernChinesepatientswithsystemicerythematosus lupus:aprospectivestudyofallagegroups.Medicine (Baltimore).2005;84:218–24.