w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Prevalence
of
the
American
College
of
Rheumatology
hematological
classification
criteria
and
associations
with
serological
and
clinical
variables
in
460
systemic
lupus
erythematosus
patients
Thelma
Skare
∗,
Renata
Damin,
Renata
Hofius
HospitalUniversitárioEvangélicodeCuritiba(HUEC),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10November2014 Accepted24December2014 Availableonline31January2015
Keywords:
Systemiclupuserythematosus Hemolyticanemia
Leukopenia Thrombocytopenia
a
b
s
t
r
a
c
t
Objective:TostudysystemiclupuserythematosusinaBrazilianpopulationusingthe
Amer-icanCollegeofRheumatologyhematologicalclassificationcriteriaandreportassociations ofthediseasewithserologicalandclinicalprofiles.
Methods:Thisisaretrospectivestudyof460systemiclupuserythematosuspatientsfollowed
inasinglerheumatologiccenterduringthelast10years.Hematologicalmanifestations con-sideredforthisstudywerehemolysis,leukopenia,lymphocytopeniaandthrombocytopenia.
Results:The cumulativeprevalences ofleukopenia, thrombocytopenia,lymphocytopenia
and hemolyticanemia were29.8%, 21.08%, 17.7%and 8.4%,respectively.A higher per-centageofpatientswithhemolysishadanticardiolipinIgM(p-value=0.002).Thosewith leukopeniahadmorelymphopenia(p-value=0.02),psychosis(p-value=0.01), thrombocy-topenia(p-value<0.0001)andanti-doublestrandedDNAantibodies(p-value=0.03).Patients with lymphopeniahadmore leukopenia(OR=1.8;95%CI=1.01–3.29)andlupus antico-agulant antibodies (OR=2.2; 95% CI=1.16–4.39) and those with thrombocytopenia had moreleukopenia(OR=3.1;95%CI=1.82–5.44)andantiphospholipidsyndrome(OR=3.1;95% CI=1.28–7.87).
Conclusion: Themostcommonhematologicalfindingwasleukopeniaandtheleast
com-mon washemolysis.Associationsoflowplateletcountandhemolysiswerefoundwith antiphospholipidsyndromeandanticardiolipinIgMpositivity,respectively.Leukopeniaand lymphocytopeniaarecorrelatedandleukopeniaismorecommoninsystemiclupus erythe-matosuspatientswithpsychosis,thrombocytopeniaandanti-doublestrandedDNA.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:Servic¸odeReumatologia,HospitalUniversitárioEvangélicodeCuritiba,RuaAugustoStellfeld,1908,80730-150
Bigorrilho,Curitiba,PR,Brazil.
E-mailaddress:[email protected](T.Skare). http://dx.doi.org/10.1016/j.bjhh.2015.01.006
Introduction
Systemiclupuserythematosus(SLE),asystemicautoimmune diseasemostcommoninyoungfemales,hasavery hetero-geneousclinicalprofile.1Thegeneticbackgroundofpatients
affectsnotonlytheprevalenceofSLEbutalsothephenotype.2
Accordinglyethnicfeaturesfavortheappearanceof autoan-tibodies and clinical clusters that define the subtypes of the disease.3,4 These aspects highlight the need to know
lupusclustersasthisawarenessallowstheclinicianto pre-dictafuturemanifestationfromonealreadypresent.Italso highlightstheneedforlocalknowledgeofdiseasebehavior, particularlyin apopulation suchas the Brazilianwhich is highlymixedfromtheethnicpointofview.
The classical hematological manifestations in SLE are hemolyticanemia,leukopenia,andthrombocytopenia;these manifestationsarepartofthe1997revisedAmericanCollege ClassificationCriteriaforSLE5aswellasthenew2012
Sys-temicLupusInternationalCollaboratingClinicsClassification Criteria.6
According to previous works, thrombocytopenia has a prevalenceinthelupuspopulationrangingfrom7to30%.7–9
Althoughthrombocytopenia isnot directlyassociated with end organ damage,it defines a subgroup of patients with highermorbidityandconsequentlyhasimportantprognostic implications.10
LeukopeniaisatypicalfeatureofSLEandmayoccur as a resultoflymphopenia, neutropenia or both.11
Neutrope-nia,which maybemediatedbyanti-neutrophil antibodies, iscommon,withaprevalenceintheorder of47%.11,12 The
prevalenceof lymphopenia isvariable, ranging from 20 to 81% and correlateswith disease activity.12,13 Both T and B
lymphocytesare reducedwhilenaturalkiller (NK)cells are elevated.11,14 Althoughthereare numerous reportsof
lym-phocytotoxicantibodies,11,15theirsignificanceinthiscontext
remains uncertain. Reducedsurface expressionof comple-ment regulatoryproteinssuch asCD55and CD59has also beenimplicatedinthepathogenesisoflupuslymphopenia, asthisdeficiencywillmakecellssusceptibleto complement-mediatedlysis.11,16
Autoimmune hemolytic anemia (AIHA) is described in 7–15%oflupuspatientsandmayoccurtogetherwithimmune thrombocytopeniaintheEvanssyndrome.17,18Itisassociated
withthepresenceofwarm(predominantly)andcoldanti-red bloodcellautoantibodies.17
Theaimofthecurrentstudywastoassesstheprevalence ofhematologicalmanifestationsinacohortofBrazilianlupus patientsaswellasitsassociationswithclinicaland autoanti-bodyprofiles.
Methods
Thisisaretrospectivestudy,approvedbythelocalResearch EthicsCommittee.Thechartsof460SLEpatientsseenoverthe last10yearsinasingletertiarycenterwerereviewed.Tobe includedinthisstudy,patientshadtocomplywithatleastfour ofthe1997revisedAmericanCollegeofRheumatology classi-ficationcriteriaforSLE.5Patientsdiagnosedbeforetheageof
16yearsand thosewithincompleterecordswere excluded. Data on demographic, clinical and serological profile were obtained.Thedefinitionofallclinicalfindingsfollowedthose oftheACRclassificationcriteria.5Thecriteriawere
cumula-tivelyconsideredwhenthepatienthadnoknowninfections. According to these criteria, hematological manifestations weredefinedasthepresenceofhemolyticanemia,leukopenia defined asless than 4×103 cells/mL on atleasttwo
occa-sions,lymphopeniadefinedaslessthan1.5×103cells/mLon
atleasttwooccasionsandthrombocytopeniadefinedasless than100×103cells/mLintheabsenceofanoffendingdrug.5
Antiphospholipidsyndrome(APS)wasdiagnosedaccordingto the2006modifiedAPScriteria.19Thecompletecellcountwas
performedusinganautomatedanalyzer(XE2100D, Sysmex) andthewhitecelldifferentialcountwasperformedmanually usingGiemsastain.
Statisticalanalysis
All obtaineddata were collected as frequencies in contin-gencytables.TheKolmogorov–Smirnovtestwasusedtostudy datadistribution.Groupsofpatientswithonehematological manifestation(hemolyticanemia,leukopeniaor thrombocy-topenia) were comparedwiththose without thisparticular manifestationinrespecttootherclinicalmanifestationsand their autoantibodyprofile.Central tendency wasexpressed asmedianandinterquartilerange(IQR)whennumericdata were nonparametricandmeanand standarddeviation(SD) when parametric. Association studies were performed by Fisher’sexactandchi-squaretestsfornominaldataandwith Mann–Whitney and unpaired t-test fornumerical data. All variablesthathadsignificancewithap-value<0.1in univari-ateanalysis,werefurtherstudiedusinglogisticregressionto assessindependency.Statisticalanalysesweremadeusingthe Medcalcsoftwareversion10.0,andsignificancewassetforan alphaerrorof5%.
Results
Analysisofthesample
Thesamplewascomprisedof93.5%femalesand6.5%males withages rangingfrom 16to88 yearsand mediandisease durationof8years.Theclinicandserologicalprofilesarelisted inTable1.
Studyoflupuspatientswithhemolyticanemia
Thecomparisondataofpatientswithandwithouthemolytic anemia(p-value<0.1)areshowninTable2.
Association studies of hemolytic anemia with disease duration, age at diagnosis, gender, photosensitivity, oral ulcers,malarrash,discoidlesions,arthritis, glomerulonephri-tis,seizures,psychosis,serositis,lymphopenia,anti-Ro/SS-A, anti-La/SS-B, anti-ribonucleoprotein (anti-RNP), anti-double strandedDNA(anti-dsDNA),rheumatoidfactorandAPSwere notsignificant.
Table1–Clinicalandserologicalprofileoflupus patients.
n %
Photosensitivity 347/452 76.7 Oralulcers 205/437 46.9 Malarrash 230/441 52.1 Discoidlesions 57/441 15.1
Arthritis 281/458 61.3
Glomerulonephritis 183/457 40.0
Seizures 48/457 10.5
Psychosis 23/455 5.0
Serositis 81/457 17.7
Leukopenia 136/455 29.8
Lymphopenia 80/450 17.7
Hemolyticanemia 39/460 8.4 Thrombocytopenia 97/460 21.08 AntiRo/SS-A 161/441 36.5 AntiLa/SS-B 80/440 18.1
AntiRNP 110/421 26.1
AntiSM 87/434 20.0
Anti-dsDNA 150/444 33.7
AnticardiolipinIgG 54/443 12.1 AnticardiolipinIgM 53/443 11.9 Lupusanticoagulant 59/407 14.4 Rheumatoidfactor 95/411 23.1 Antiphospholipidsyndrome 33/439 7.5
anticardiolipinIgMremainedsignificant[p-value=0.002; OR 5.1;95%confidenceinterval(CI)=1.7–14.9].
Associationstudieswithleukopenia
Dataofpatientswithandwithoutleukopenia(p-value<0.1) arelistedinTable3.Comparisonsofage,diseaseduration,age atdiagnosis,gender,photosensitivity,oralulcers,malarrash, discoidlesions,arthritis,glomerulonephritis,serositis, pres-enceofanti-Ro/SS-A;Anti-La/SS-B,anti-RNP,anticardiolipin IgGandIgM,rheumatoidfactorandAPSwerenotsignificant. On including the variables with a p-value <0.1 in the univariateanalysisinalogisticregressionmodel, lymphope-nia (p-value=0.02; OR=1.8; 95% CI=1.06–3.15), psychosis (p-value=0.01;OR=3.1;95%CI=1.22–8.03);thrombocytopenia (p-value<0.0001;OR=3.2;95%CI=1.93–5.33);andanti-dsDNA (p-value=0.03; OR=1.6; 95% CI=1.02–2.54) were indepen-dentlyassociatedwithleukopenia.
Associationstudiesofthrombocytopenia
Association studies of thrombocytopenia are shown in Table 4. Comparative analysis of associations with age, disease duration, age at diagnosis, gender, oral ulcers, malar rash, discoid lesions, glomerulonephritis, psychosis, serositis, anti-Ro/SS-A, anti-La/SS-B, anti-RNP, anti-SM, anti-dsDNA and rheumatoid factor were found to be non-significant.
When the variables with p-values <0.1 in univariate analysis were assessed using logistic regression, arthritis remainedinverselyassociatedtothrombocytopenia(OR=0.3; 95%CI=0.20–0.61)andleukopenia(OR=3.1;95%CI=1.82–5.44) and APS (OR=3.1; 95% CI=1.28–7.87) were associated to thrombocytopenia.
Associationstudiesoflymphocytopenia
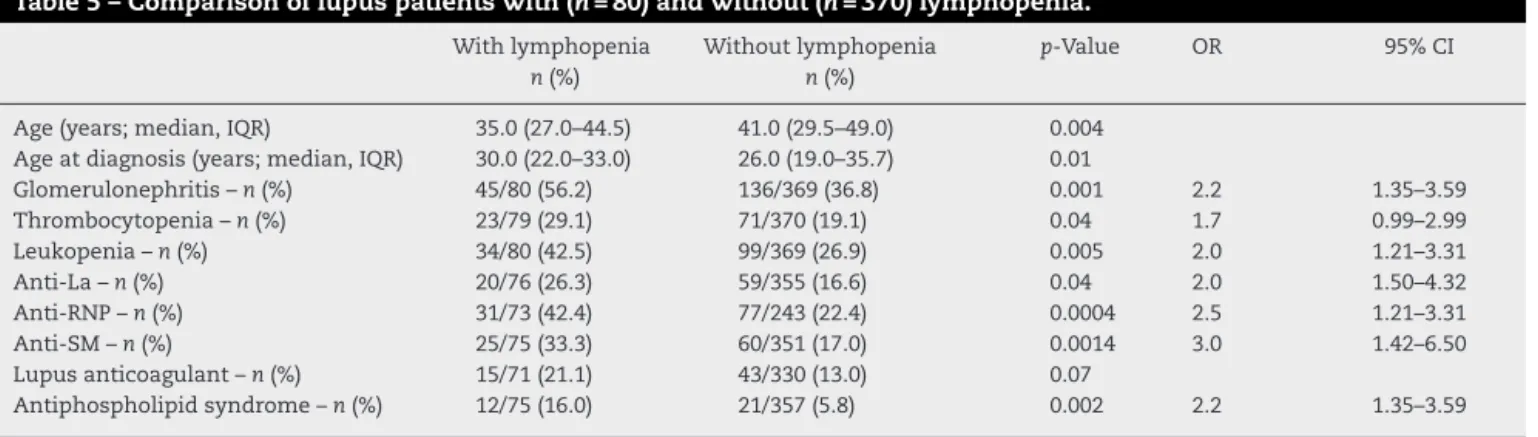
Associationsofvariableswithlymphocytopeniaareshownin Table 5. Analysisofdisease duration,gender, photosensiti-vity,oralulcers,malarrash,discoidlesions,arthritis,seizures, psychosis,serositis,hemolyticanemia,anti-Ro,anti-dsDNA, anticardiolipinIgGandIgMandrheumatoidfactorwere non-significant.
Inthelogisticregressionstudyofvariableswithp-values <0.1 in the univariate analysis, only leukopenia (OR=1.8; 95% CI=1.01–3.29) and lupus anticoagulant (OR=2.2; 95% CI=1.16–4.39)remainedindependentlysignificant.
Discussion
Hematologicalfindings inlupus patientsare very common and may be the presenting feature of the disease. In the current study hemolytic anemia was the least common manifestation(8%)followedbylymphopenia(18%), thrombo-cytopenia(21%)andleukopenia(30%).
Therewasanassociationbetweenhemolyticanemiaand anticardiolipin IgM antibodies; this association has been described in other studies. Lang et al.20 described
asso-ciations with both anticardiolipin IgG and IgM antibodies. Sultanetal.,18 studying305lupuspatientsfromtheUnited
Kingdom,foundanassociationwithanticardiolipinIgG anti-bodiesbutDelezeetal.21studyingSpanishlupuspatientsand
Cerveraetal.8 analyzingaMexicansamplereportedstrong
Table2–Associationstudiesofdemographic,clinicalandserologicalvariablesoflupuspatientswithhemolyticanemia.
Withhemolyticanemia n=39
Withouthemolyticanemia n=421
p-Value OR 95%CI
Ageyears–median(IQR) 35.0(23.0–47.0) 40.0(30.0–49.0) 0.06
Leukopenia–n(%) 17/39(43.5) 119/416(28.6) 0.0506 1.9 0.9–3.7 Thrombocytopenia–n(%) 14/31(35.8) 83/416(19.9) 0.02 2.2 1.1–4.5 Anti-SM–n(%) 10/36(27.7) 77/398(19.3) <0.0001 5.4 2.6–1.4 AnticardiolipinIgG–n(%) 10/38(26.3) 44/405(10.8) <0.0001 5.8 3.0–11.2 AnticardiolipinIgM–n(%) 14/38(36.8) 39/404(9.6) <0.0001 5.4 2.6–11.4 Lupusanticoagulant–n(%) 12/34(35.2) 47/373(12.6) 0.001 3.7 1.7–8.1
Table3–Comparisonoflupuspatientswith(n=136)andwithout(n=319)leukopenia.
Withleukopenia n(%)
Withoutleukopenia n(%)
p-Value OR 95%CI
Seizures 20/136(14.7) 28/316(8.8) 0.06
Psychosis 14/136(10.2) 9/317(2.8) 0.0009 3.9 1.6–9.3 Lymphopenia 34/133(25.5) 46/315(14.6) 0.005 2.00 1.21–3.31 Hemolyticanemia 17/135(12.5) 22/319(6.8) 0.04 1.9 0.99–3.7 Thrombocytopenia 51/136(37.5) 46/317(14.5) <0.0001 3.5 2.2–5.6 Anti-dsDNA 55/134(41.0) 95/307(30.9) 0.03 1.55 1.02–2.36 Lupusanticoagulant 27/123(21.9) 32/283(11.3) 0.005 2.20 1.25–3.87
OR:oddsratio;95%CI:95%confidenceinterval.
Table4–Comparisonoflupuspatientswith(n=97)andwithout(n=363)thrombocytopenia.
WithTCP n(%)
WithoutTCP n(%)
p-Value OR 95%CI
Photosensitivity 67/96(69.7) 268/356(75.2) <0.0001 3.2 2.02–5.18 Arthritis 45/97(46.3) 221/361(61.2) 0.008 0.54 0.34–0.86 Seizures 14/96(14.5) 30/361(8.3) 0.06
Hemolyticanemia 14/96(14.5) 20/361(5.5) 0.002 2.9 1.41–6.00 Lymphopenia 23/94(24.4) 54/356(15.1) 0.03 1.8 1.04–3.14 Leukopenia 51/97(52.5) 82/358(22.9) <0.0001 3.7 2.33–5.96 AnticardiolipinIgG 18/95(18.9) 34/348(9.7) 0.01 2.1 1.15–4.02 AnticardiolipinIgM 17/95(17.8) 34/347(9.7) 0.01 2.1 1.15–4.02 Lupusanticoagulant 21/89(23.9) 37/318(11.6) 0.004 2.3 1.29–4.26 Antiphospholipidsyndrome 16/94(17.02) 17/345(4.9) <0.0001 3.9 1.91–8.18
TCP:thrombocytopenia;OR:oddsratio;95%CI:95%confidenceinterval.
associationswithanticardiolipinIgMantibodiessimilartothe currentstudy.
Leukopenia was the most common hematological find-ing in this study appearing in almost one inthree ofthe patients.Theimportanceofthisfindingishighlightedwhen one notes that infections are a leading cause of death in SLE patients.22 Bacterial infections are the most common,
followed by viral and fungal infections.22 In this sample,
leukopenia was associated with lymphopenia, psychosis, thrombocytopeniaandanti-dsDNA.Thecorrelationbetween this finding, lymphopenia and ds-DNA has been reported byothers.17 A low lymphocyte count isfound to be
inde-pendentof(althoughcontributoryto)leukopenia17and has
beenassociated,intheliterature,tohigherlupusactivity,23
moresevereacraldamage,23andsomeclinicaldisease
char-acteristicssuchasneurologicinvolvement.17 Inthecurrent
sample, althoughlymphopeniawasfoundtobeassociated with glomerulonephritis,thrombocytopenia, anti-RNP, anti-SM,APS,lupusanticoagulantandleukopenia,onlythelasttwo remainedsignificant afterlogisticregression.Lupusdisease activityandcumulativedamagewerenotstudied.
SLEthrombocytopeniaresultsfromdiseaseactivityorfrom suppressionofthebonemarrowbyanimmunosuppressant.24
Autoantibodiesagainstplatelets,againstthrombopoietinand bone marrow abnormalities have been detected in these patients.24Althoughantibodiesagainstplateletsarecommon
amongthrombocytopenicpatientstheyarenotalwayslinked to low platelet counts.24 Furthermore, anti-thrombopoietin
Table5–Comparisonoflupuspatientswith(n=80)andwithout(n=370)lymphopenia.
Withlymphopenia n(%)
Withoutlymphopenia n(%)
p-Value OR 95%CI
Age(years;median,IQR) 35.0(27.0–44.5) 41.0(29.5–49.0) 0.004 Ageatdiagnosis(years;median,IQR) 30.0(22.0–33.0) 26.0(19.0–35.7) 0.01
Glomerulonephritis–n(%) 45/80(56.2) 136/369(36.8) 0.001 2.2 1.35–3.59 Thrombocytopenia–n(%) 23/79(29.1) 71/370(19.1) 0.04 1.7 0.99–2.99 Leukopenia–n(%) 34/80(42.5) 99/369(26.9) 0.005 2.0 1.21–3.31 Anti-La–n(%) 20/76(26.3) 59/355(16.6) 0.04 2.0 1.50–4.32 Anti-RNP–n(%) 31/73(42.4) 77/243(22.4) 0.0004 2.5 1.21–3.31 Anti-SM–n(%) 25/75(33.3) 60/351(17.0) 0.0014 3.0 1.42–6.50 Lupusanticoagulant–n(%) 15/71(21.1) 43/330(13.0) 0.07
Antiphospholipidsyndrome–n(%) 12/75(16.0) 21/357(5.8) 0.002 2.2 1.35–3.59
autoantibodiesareconsideredtohaveaweakeffectonplatelet counts.24 In the current study positive associations were
found for thrombocytopenia with APS and with leukope-nia.TheassociationbetweenAPSand thrombocytopeniais well known not only in lupus but in other autoimmune thrombocytopenias.17
Conclusion
The most common hematological abnormality of the SLE classification criteria in a cohort of Brazilian SLE patients wasleukopeniafollowedbythrombocytopenia,lymphopenia and hemolyticanemia. Low platelet countsand hemolysis were associated to APS and anticardiolipin IgM, respec-tively.Leukopenia andlymphocytopenia arecorrelated and leukopeniaismorecommoninSLEpatientswithpsychosis, thrombocytopeniaandanti-dsDNA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. LutzCA,JamesJA.Antibodiestospliceosomalcomponents. In:WallaceDJ,HahnBH,editors.Dubois’lupus
erythematosus.Philadelphia:Lippincott,Williams&Wilkins; 2007.p.500–13.
2. BoackleSA.Advancesinlupusgenetics.CurrOpin Rheumatol.2013;25(5):561–8.
3. JurencákR,FritzlerM,TyrrellP,HirakiL,BenselerS,Silverman E.Autoantibodiesinpediatricsystemiclupuserythematosus: ethnicgrouping,clusteranalysis,andclinicalcorrelations.J Rheumatol.2009;36(2):416–21.
4. ToCH,PetriM.Isantibodyclusteringpredictiveofclinical subsetsanddamageinsystemiclupuserythematosus? ArthritisRheum.2005;52(12):4003–10.
5. HochbergMC.UpdatingtheAmericanCollegeof Rheumatologyrevisedcriteriafortheclassificationof systemiclupuserythematosus.ArthritisRheum. 1997;40(9):1725.
6. PetriM,OrbaiAM,AlarcónGS,GordonC,MerrillJT,FortinPR, etal.Derivationandvalidationofthesystemiclupus internationalcollaboratingclinicsclassificationcriteriafor systemiclupuserythematosus.ArthritisRheum.
2012;64(8):2677–86.
7. WangF,WangCL,TanCT,ManivasagarM.Systemiclupus erythematosusinMalaysia:astudyof539patientsand comparisonofprevalenceanddiseaseexpressionindifferent racialandgendergroups.Lupus.1997;6(3):248–53.
8. CerveraR,KhamashtaMA,FontJ,SebastianiGD,GilA,Lavilla P,etal.Morbidityandmortalityinsystemiclupus
erythematosusduringa5-yearperiod.Amulticenter prospectivestudyof1.000patients.EuropeanWorkingParty onSystemicLupusErythematosus.Medicine.
1999;78(3):167–75.
9. MokCC,LeeKW,HoCT,LauCS,WongRW.Aprospective studyofsurvivalandprognosticindicatorsofsystemiclupus
erythematosusinasouthernChinesepopulation. Rheumatology(Oxford).2000;39(4):399–406.
10.ZiakasP,GiannouliS,ZintzarasE,TzioufasAG,VoulgarelisM. Lupusthrombocytopenia:clinicalimplicationsand
prognosticsignificance.AnnRheumDis.2005;64(9):1366–9. 11.HepburnAL,SantoshNaratS,MasonJC.Themanagementof
peripheralbloodcytopeniasinsystemiclupus
erythematosus.Rheumatology(Oxford).2010;49(12):2243–54. 12.WorrallJG,SnaithML,BatchelorJR,IsenbergDA.SLE:a
rheumatologicalview.Analysisoftheclinicalfeatures, serologyandimmunogeneticsof100SLEpatientsduring long-termfollow-up.QJMed.1990;74(275):319–30. 13.NossentJC,SwaakAJ.Prevalenceandsignificanceof
haematologicalabnormalitiesinpatientswithsystemic lupuserythematosus.QJMed.1991;80(291):605–12.
14.GlinskiW,GershwinME,BudmanDR,SteinbergAD.Studyof lymphocytesubpopulationsinnormalhumansandpatients withsystemiclupuserythematosusbyfractionationof peripheralbloodlymphocytesonadiscontinuousFicoll gradient.ClinExpImmunol.1976;26(2):228–38. 15.WinfieldJB,WinchesterRJ,KunkelHG.Associationof
cold-reactiveantilymphocyteantibodieswithlymphopeniain systemiclupuserythematosus.ArthritisRheum.
1975;18(6):587–94.
16.Garcia-ValladaresI,Atisha-FregosoY,Richaud-PatinY, Jakez-OcampoJ,Soto-VegaE,Elías-LópezD,etal.Diminished expressionofcomplementregulatoryproteins(CD55and CD59)inlymphocytesfromsystemiclupuserythematosus patientswithlymphopenia.Lupus.2006;15(9):600–5. 17.QuismorioFPJr.Hematologicandlymphoidabnormalitiesin
systemiclupuserythematosus.In:WallaceDJ,HahnBH, editors.Dubois’lupuserythematosus.Philadelphia: Lippincott,Williams&Wilkins;2007.p.801–28.
18.SultanSM,BegumS,IsenbergDA.Prevalence,patternsof diseaseandoutcomeinpatientswithsystemiclupus erythematosuswhodevelopseverehaematologicalproblems. Rheumatology(Oxford).2003;42(2):230–4.
19.MiyakisS,LockshinMD,AtsumiT,CranchDW,BreyRL, CerveraR,etal.Internationalconsensusstatementonan updateoftheclassificationcriteriafordefinite
antiphospholipidsyndrome(APS).JThrombHaemost. 2006;4(2):295–306.
20.LangB,StraubRH,WeberS,RotherE,FleckM,PeterH-H. Elevatedanticardiolipinantibodiesinautoimmune haemolyticanaemiairrespectiveofunderlyingsystemic lupuserythematosus.Lupus.1997;6(8):652–5.
21.DelezeM,Alarcon-SegoviaD,OriaCV,Sánchez-GuerreroJ, Fernández-DominguezL,Gomez-PachecoL,etal. Hemocytopeniainsystemiclupuserythematosus. Relationshiptoantiphospholipidantibodies.JRheumatol. 1989;16(7):926–30.
22.DanzaA,Ruiz-IrastorzaG.Infectionriskinsystemiclupus erythematosuspatients:susceptibilityfactorsandpreventive strategies.Lupus.2013;22(12):1286–94.
23.VolláLM,Alarcón-SegoviaGS,McGwinGJr,BastianHJ,Fessler BJ,ReveilleJD.SystemicLupuserythematosusina
multiethnicUScohort.XXXVII:Associationoflymphopenia withclinicalmanifestations,serologicabnormalities,disease activityanddamageaccrual.ArthritisRheum.
2006;55(5):799–806.