r e v b r a s r e u m a t o l . 2014;54(5):356–359
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
www . r e u m a t o l o g i a . c o m . b r
Original
article
Evaluation
of
frequency
and
the
attacks
features
of
patients
with
colchicine
resistance
in
FMF
Gozde
Yildirim
Cetin
a,∗,
Ayse
Balkarli
b,
Ali
Nuri
Öksüz
a,
Gezmis¸
Kimyon
c,
Yavuz
Pehlivan
c,
Ozlem
Orhan
a,
Bunyamin
Kisacik
c,
Veli
Cobankara
b,
Hayriye
Sayarlioglu
d,
Ahmet
Mesut
Onat
c,
Mehmet
Sayarlioglu
daSutcuImamUniversity,SchoolofMedicine,DepartmentofInternalMedicine,DivisionofRheumatology,Kahramanmaras,Turkey
bPamukkaleUniversity,SchoolofMedicine,DepartmentofInternalMedicine,DivisionofRheumatology,Denizli,Turkey
cGaziantepUniversity,SchoolofMedicine,DepartmentofInternalMedicine,DivisionofRheumatology,Gaziantep,Turkey
dOndokuzMayisUniversity,SchoolofMedicine,DepartmentofInternalMedicine,DivisionofNephrology,Samsun,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26August2013
Accepted17March2014
Availableonline20August2014
Keywords:
FamilialMediterraneanfever
Colchicineresistance
Treatment Depression
a
b
s
t
r
a
c
t
Introduction:Colchicine is the mainstay for the treatment of FMF, which is an
auto-inflammatorydiseasemainlywithrelapsingpolyserositis.Despitedailydosesof2mgor
moreeachday,approximately5%to10%ofthepatientscontinuetosufferfromitsattacks.
Inthisstudy,weaimedtoinvestigatethedepressionandattackfeaturesinpatientswith
FMFwhohavecolchicineresistance(CR).
PatientseMethods:CRwasdefinedforFMFpatientswith2ormoreattackswithinthelast
6monthsperiodwhileusing2mg/daycolchicine.Eighteenpatients(9Female/9Male)were
enrolledintotheCRgroupand41patientswereenrolledintothecontrolgroup(12Male/29
Female).Demographic,clinicalelaboratory findings,treatment adherence,andtheBeck
DepressionInventory(BDI)scoreswereevaluated.
Results:TheageofonsetofFMFwassignificantlylowerintheCRgroup(12.3yrsvs.16.9yrs,
P=0.03).DiseasedurationwaslongerintheCRgroup(P=0.01).Abdominalandlegpaindue
toexerciseweresignificantlymorefrequentintheCRgroupversuscontrols(83%vs.51%;
P=0.02e88%vs.60%;P=0.04,respectively).PatientswithBDIscoresover17pointswere
morefrequentintheCRgroupcomparedtocontrols(50%vs.34.1%;P<0.001).
Discussion:Wefoundthat:(1)theageofdiseaseonsetwaslowerand(2)thediseaseduration
waslongerinCRgroup.Pleuriticattacks,hematuriaeproteinuriaweremorefrequentinCR
patients.Weproposethatdepressionisanimportantfactortoconsiderinthesusceptibility
toCR.
©2014ElsevierEditoraLtda.Allrightsreserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.03.022.
∗ Correspondingauthor.
E-mail:[email protected](G.Y.Cetin).
http://dx.doi.org/10.1016/j.rbre.2014.03.022
rev bras reumatol.2014;54(5):356–359
357
Avaliac¸ão
da
frequência
e
aspectos
dos
ataques
de
pacientes
com
resistência
à
colchicina
em
febre
familiar
do
Mediterrâneo
(FFM)
Palavras-chave:
FebrefamiliardoMediterrâneo
ResistênciaàColchicina
Tratamento Depressão
r
e
s
u
m
o
Introduc¸ão: Colchicinaéaviga-mestraparaotratamentodeFFM,queéumadoenc¸a
autoin-flamatóriacompolisserositerecidivante comoprincipal manifestac¸ão.Apesarde doses
diáriasde2mgoumais/dia,aproximadamente5%-10%dospacientescontinuamasofrerde
seusataques.Nesteestudo,objetivamosinvestigarosaspectosdadepressãoedosataques
empacientescomFFMapresentandoresistênciaàcolchicina(RC).
PacienteseMétodos: EmpacientescomFFM,RCfoidefinidacomodoisoumaisataques
nosúltimosseismeses,quandoemmedicac¸ãocomcolchicina2mg/dia.Dezoitopacientes
(novemulheresenovehomens)foramrecrutadosnogrupoRCe41pacientesnogrupo
decontrole(29mulheres/12homens).Foramavaliadososachadosdemográficos,clínicose
laboratoriais,afidelidadeaotratamentoeosescoresdoBeckDepressionInventory(BDI).
Resultados: A idade de surgimento da FFM foi significativamentemenor no grupo RC
(12,3anosvs.16,9anos,P=0,03).Adurac¸ãodadoenc¸afoimaiornogrupoRC(p=0,01).
Doresabdominaisenaspernasemdecorrênciadoexercícioforamsignificativamentemais
frequentesnogrupoRCversuscontroles(83%vs.51%;p=0,02e88%vs.60%;p=0,04,
res-pectivamente).PacientescomescoresBDI>17pontosforammaisfrequentesnogrupoRC
versuscontroles(50%vs.34,1%;p<0,001).
Discussão:Verificamosque:(1)aidadedosurgimentodadoenc¸afoimaisbaixae(2)adurac¸ão
dadoenc¸afoimaiornogrupoRC.Ataquespleuríticos,hematúriaeproteinúriaforammais
frequentesempacientescomRC.Propomosqueadepressãoéfatorimportanteaserlevado
emconsiderac¸ãonasensibilidadeàRC.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Familial Mediterranean fever (FMF) is a hereditary and an
auto-inflammatorydisease predominantly characterizedby
repeated attacks of fever, abdominal pain, pleuritic chest
pain,arthritis,and erysipelas-likeerythema.Thedisease is
most prevalent among non-Ashkenazi Jews, Arabs, Turks,
andArmenians.1 Thepathogenesisismainlybased onthe
absence or insufficiency of pyrin production, which is a
peptideinvolvedin theinflammatorycascade thatinhibits
complement5a(C5a).ThemainmechanismsthattriggerFMF
attackshavenotbeenestablished.Colchicineisstillthe
main-stayinthetreatmentofthedisease.Itcompletelyorpartially
preventsFMF attacks and subsequent reactive amyloidosis
thatisregardedasthemostdangerouscomplicationofFMF.2
Interestingly, colchicine resistance (CR) is prevalent in
nearly10%oftheFMFpatients.Theattackfrequencyor
inten-sity may goon with similar or diminished frequency and
severity.TheCRpatientscouldbedividedinto completeor
partiallynon-responders.Manyfactorsmightbeinvolvedin
theCR,includinggeneticpredispositionaswellas
environ-mentalandpsychiatricconditions.Still,littleisknownabout
theabsoluteetiologyofCRinFMFpatients.Treatment
adher-enceandpotentialreasonsincludingdemographicalfactors,
socio-economic status, clinical and laboratory factors, and
psychiatricdynamicsarethoughttobecontributingfactors.
The Beck Depression Inventory (BDI) was developed by
Beckand colleagues(1979) and adaptedto TurkishbyHisli
(1988).TheBDIisaself-reportscaleof21itemsmeasuringthe
emotional, somatic, cognitive, and motivational symptoms
exhibited indepression. Thescale isnotdesignedto
diag-nosedepressionbuttoobjectivelydeterminetheseverityof
depressive symptoms. Correlation coefficients between the
EnglishandTurkishversionsofthescalewerecalculatedas
0.81and0.73(languagevalidity);splithalfreliabilitywas0.74,
and criterion-relatedvaliditywithMMPI-D(Minnesota
Mul-tiphasicPersonalityInventory)was0.63.TheBDIscores≥17
werereportedtodiscriminatedepressionthatmightrequire
treatmentwithmorethan90% accuracy.Thescoreofeach
itemrangesfrom0to3,andthedepressionscoreisobtained
byaddingthescoreofeachitem.Thehighestobtainablescore
is63.3,4
As a consequence, different therapeutic strategies are
ongoingtolimitCRinFMFpatients.Inthisstudy,weaimed
toinvestigatethedepressionandattackfeaturesinpatients
withFMFwhohavetheCR.
Patients
and
methods
Thestudygroupwascomposedof59 FMFpatientswith18
CR(9female/9male)and41(12male/29female)complete
colchicine responders.Patientshaving otheraccompanying
diseasesincludinginfections,malignancies,autoimmuneor
metabolic diseases and patients who were diagnosed for
depressionpreviouslyandunder-treatmentwith
antidepres-sants wereexcluded. Thediagnosiswascheckedonemore
timethroughthere-questioningofthepatientsinaccordance
withtheLivnehcriteriaofFMF.5
CRwasdefinedastwoormoreFMFattacksinasix-month
358
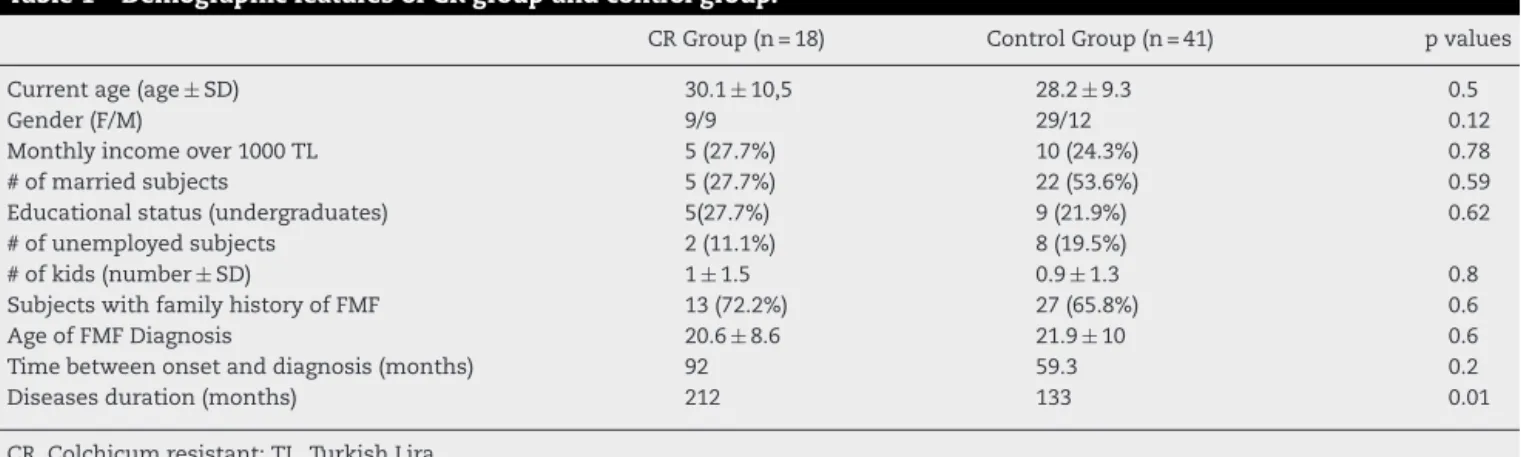
rev bras reumatol.2014;54(5):356–359Table1–DemographicfeaturesofCRgroupandcontrolgroup.
CRGroup(n=18) ControlGroup(n=41) pvalues
Currentage(age ± SD) 30.1 ± 10,5 28.2± 9.3 0.5
Gender(F/M) 9/9 29/12 0.12
Monthlyincomeover1000TL 5(27.7%) 10(24.3%) 0.78
#ofmarriedsubjects 5(27.7%) 22(53.6%) 0.59
Educationalstatus(undergraduates) 5(27.7%) 9(21.9%) 0.62
#ofunemployedsubjects 2(11.1%) 8(19.5%)
#ofkids(number ± SD) 1± 1.5 0.9± 1.3 0.8
SubjectswithfamilyhistoryofFMF 13(72.2%) 27(65.8%) 0.6
AgeofFMFDiagnosis 20.6 ± 8.6 21.9± 10 0.6
Timebetweenonsetanddiagnosis(months) 92 59.3 0.2
Diseasesduration(months) 212 133 0.01
CR,Colchicumresistant;TL,TurkishLira.
with≤1FMF attackwithinthesixmonthsorwithoutany attacksoverthetwelvemonthswererandomizedintothe con-trolgroup. Patientsinthecolchicine resistancegroupwere using2mg/dayand higherdoses,and inthecontrolgroup patientswereusingcolchicinebelowthedosesof2mg/day. Thedemographicdata,adherencetotreatment,clinicaland attack features of the disease including the leg pain and amyloidosis,laboratoryfindings,andBDIscores,alcohol,and narcoticusagewererecorded.ABDIscore>17wasconsidered significantforseveredepressionthatrequirestreatment.
The age of disease onset as well as diagnosis and the time period from symptoms to diagnosis were carefully questioned.Thedemographicdataincludedsocio-economic featuressuchasmonthlyincome,educationandliteracy, mar-ital status, number of children, and employment. Patients were compared by the minimum wage in our country for their economic status. Concerning the educational status, post-graduatepatientswerecomparedwitheachother.Urine analyseswere assessedwith adipstick duringattacks and werecollectedfromfiles.
Thelocalethicalcommitteeapprovedthestudyprotocol and all the participant consentforms were collected. Stu-dent’sttestandone-wayANOVAwereusedforcomparison ofaverages.Pearson’scorrelationanalyseswereperformedto evaluateotherfactors.Pvalueof<0.05wasacceptedas statis-ticallysignificant.
Results
WhileCRpatientswereregularlyimplementingthetreatment protocolduringthe6-monthfollow-up, 40%ofthepatients incontrol group were misusingthe drugs. Baseline demo-graphicfeaturesofbothgroupsaredemonstratedinTable1.
Therewasnostatisticallysignificantdifferencebetweenthe
groupsconcerningthemonthlyincome,educationaland
mar-italstatus,numberofkids,andemployment.Distributionof
thepatientswithfamilyhistoryofFMFwassimilar.Disease
onsetagewassignificantlylowerinCRgroupincontrastto
thecontrols(12.3yearsand16.9years;p=0.03)anddisease
durationwassignificantlylongerinCRgroup(212monthsand
133months;p=0.01).Thereweresimilarresultsconcerning
thetimefromdiseaseonsettodiagnosis,andthedifference
wasnotsignificantbetweenthegroups.Whenwecompared
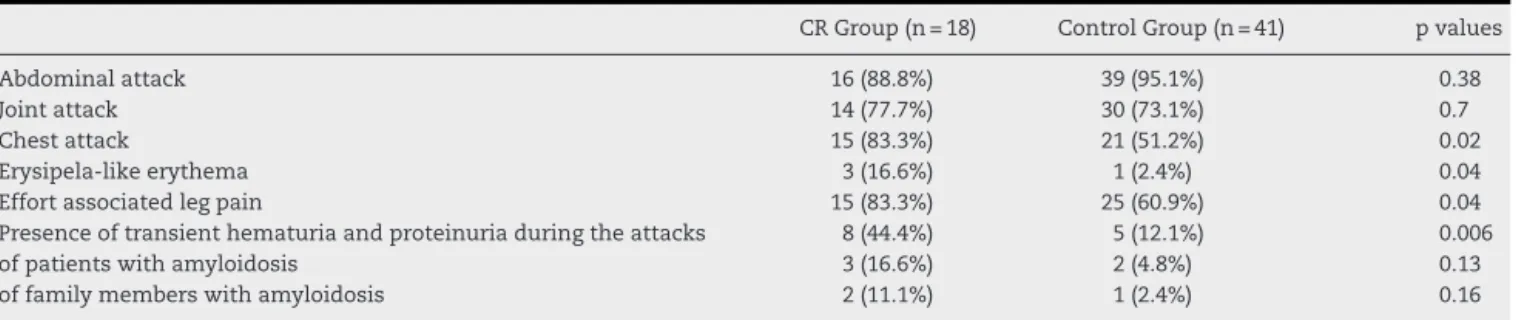
the accompanyingcomplaints duringthe attacks, pleuritic
chestpain,erysipelas-likeerythemaandeffortassociated,leg
pain wassignificantlymorefrequentinCRgroup(83%and
51% p=0.02;16.6%and 2.4%p=0.04;88%and 60% p=0.04;
respectively).Moreover,transientproteinuriaandhematuria
weresignificantlymorefrequentinCRgroup(p=0.006).There
wasnotavaluabledifferencebetweenthegroupsconcerning
abdominalpainandarthritis(Table2).Therewereno
alco-hol ornarcoticshistory amongthe groups. Thenumberof
patientswithamyloidosisinbothgroupswassimilar(Table2).
Therewasnorenalinsufficiencyinbothgroups.Patientswith
BDIscoresover17pointsweremorefrequentintheCRgroup
comparedtothecontrols(50%vs34.1%;p<0.001).
Discussion
Thisprospectivelydesignedstudy attemptstoevaluatethe
factorsthatmayleadtoCRamongtheFMFpatients.Disease
onsetagewassignificantlylowerinCRgroupincontrastto
thecontrol,anddiseasedurationwassignificantlylongerin
CRgroup.QuestionnaireresultsshowedthatpatientsinCR
group were receiving their drugs regularly under full drug
compliance. Patientswithinfrequent attacks forgottotake
thecolchicine.Additionally,therewerenoalcoholornarcotics
history amongthe CRpatients.Infact, themaintriggering
etiologicalfactorsbehindCRarenotknown.Intheprevious
study,Lidaretal.foundthatpatientswithsevereFMF
prog-nosishad moreCR.6 Thesefindingsare ingoodagreement
withourstudy.Obviously, patientswithlong disease
dura-tion,highBDIscores,weresignificantlymorefrequentinthe
CR group.And attacksinCR groupwere moresevere than
controlgroup.Whenwecomparedtheaccompanying
com-plaintsduringtheattacks,pleuriticchestpain,erysipelas-like
erythema,andeffortassociatedlegpainweremorefrequent
inCRgroup.Moreover,proteinuriaandhematuriapresence
duringtheattacksweremorefrequentinCRgroup.AlsoLidar
etal.demonstratedthattheabdominalattack,chestpain,and
arthritisweremorefrequentandsevereinCRgroup,while
erysipelas-likeerythemaattacksweresimilarinbothgroups.
Thepresenceofdepressioncouldincreasethefrequencyof
FMFattacksorthecombinationoffrequentFMFattacksand
inflammatory painmight cause depression.The activityof
rev bras reumatol.2014;54(5):356–359
359
Table2–Symptomaticfeaturesofallpatients.
CRGroup(n=18) ControlGroup(n=41) pvalues
Abdominalattack 16(88.8%) 39(95.1%) 0.38
Jointattack 14(77.7%) 30(73.1%) 0.7
Chestattack 15(83.3%) 21(51.2%) 0.02
Erysipela-likeerythema 3(16.6%) 1(2.4%) 0.04
Effortassociatedlegpain 15(83.3%) 25(60.9%) 0.04
Presenceoftransienthematuriaandproteinuriaduringtheattacks 8(44.4%) 5(12.1%) 0.006
ofpatientswithamyloidosis 3(16.6%) 2(4.8%) 0.13
offamilymemberswithamyloidosis 2(11.1%) 1(2.4%) 0.16
provoketheFMF attacks.7 Itwasdemonstratedthat
initiat-ing selectiveserotonin reuptakeinhibitors (SSRI) decreases
thefrequencyofFMF attackswithCR.8 Accordingly,itwas
shownthatstressfactorsfacilitatedepressionandincrease
thesecretionofinflammatorycytokines.9 Therearestudies
arguingtheroleofdepressionintheseverityofFMFandthat
depressiontreatmentalsodiminishesthenumberofattacks.
ThesefindingsrevealtheroleofdepressioninCR.8
Increases in inflammation can affect the
pathophysi-ology of the depression.8 In cytokine based FMF studies,
plasmaconcentrationsofinterleukin-2(IL),IL-12,IL-18and
tumor necrosis alpha (TNF-␣) were elevated in depressive
patients.10,11 Thepro-inflammatorycytokine,IL-12,was
ele-vatedbothduringtheattacksandintheattackfreeperiod,
contrasting healthy control studies.12 In addition to IL-12
secretion,cytotoxicTcellsIL-2,IFNgamma,andTNF-alpha
alsoincreasedinFMFpatients.Thesecytokineswereelevated
bothinFMFand depression.Ourstudyhasalimitationfor
theMEFVmutationsofthepatientsthatdidn’tholdforall
ofthepatientsenrolledintothestudy.Butouraimwasthe
investigationofotherfactorsaffectingCR.
Consequently,wecanarguethatdepressionisan
impor-tantreasonamongthefactorsthatmayleadtoCR.Consistent
withprevious studies,we havefoundout theCR patients’
depressionfindings are moresevere than thecontrols.
Cli-niciansshouldconsider theinitiation ofSSRI incolchicum
resistantpatients.Wefoundthatdiseaseonsetagewaslower
anddiseasedurationwaslonger.Inaddition,pleuritisattacks,
transientmicroscopichematuria,andproteinuriaweremore
frequentinCRpatientsduringattackepisodes.Further
large-scalescreeningisrequired.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. LidarM,LivnehA.FamilialMediterraneanfever:clinical, molecularandmanagementadvancements.NethJMed. 2007;65:318–24.
2.OzturkMA,KanbayM,KasapogluB,OnatAM,GuzG,Furst DE,etal.TherapeuticapproachtofamilialMediterranean fever:areviewupdate.ClinExpRheumatol.2011;29: 77–86.
3.Savas¸ırI,SahinNH.Bilis¸sel-davranıs¸cıterapilerde
de ˘gerlendirme:Sıkkullanılanölc¸ekler[Cognitivebehavioral therapyevaluation:Commonscales.].AnkaraTürk PsikologlarDerne ˘giYayınları.1997:23–38.
4.OzerA,OrhanFÖ,Ekerbic¸erHC¸.Sociodemographicvariables anddepressioninTurkishwomenfrompolygamousversus monogamousfamilies.HealthCareWomenInt.
2013;34:1024–34,doi:10.1080/07399332.2012.692414.Epub 2013Feb27.
5.LivnehA,LangevitzP,ZemerD,ZaksN,KeesS,LidarT,etal. CriteriaforthediagnosisoffamilialMediterraneanfever. ArthritisRheum.1997;40:1879–85.
6.LidarM,ScherrmannJM,ShinarY,ChetritA,NielE, Gershoni-BaruchR,etal.Colchicinenon-responsivenessin familialMediterraneanfever:clinical,genetic,
pharmacokinetic,andsocioeconomiccharacterization. Semin.ArthritisRheum.2004;33:273–82.
7.Ozc¸akarL,OnatAM,KaymakSU,UretenK,AkinciA.Selective serotoninreuptakeinhibitorsinfamilialMediterraneanfever: arewetreatingdepressionorinflammation?RheumatolInt. 2005;25:319–20.
8.OnatAM,OztürkMA,Ozc¸akarL,UretenK,KaymakSU,Kiraz S,etal.Selectiveserotoninreuptakeinhibitorsreducethe attackfrequencyinfamilialmediterraneanFever.TohokuJ ExpMed.2007;211:9–14.
9.KuberaM,MaesM.Serotonininteractionsinmajor depression.In:PetersonCK,editor.Neuro-Immune InteractionsinNeurologicandPsychiatricDisorders.Berlin: Springer-Verlag;2000.p.79–87.
10.SutcigilL,OktenliC,MusabakU,BozkurtA,CanseverA,Uzun O,etal.Pro-andanti-inflammatorycytokinebalancein majordepression:effectofsertralinetherapy.ClinDev Immunol.2007;2007:76396.
11.MerendinoRA,DiRosaAE,DiPasqualeG,MinciulloPL, MangravitiC,CostantinoA,etal.Interleukin-18andCD30 serumlevelsinpatientswithmoderate-severedepression. MediatorsInflamm.2002;11:265–7.