w w w . r b o . o r g . b r
Original
Article
Analysis
on
the
mechanical
resistance
of
fixation
of
femoral
neck
fractures
in
synthetic
bone,
using
the
dynamic
hip
system
and
an
anti-rotation
screw
夽
,
夽夽
Anderson
Freitas
a,∗,
Gustavo
Melo
Torres
b,
André
Cezar
de
Andrade
de
Mello
e
Souza
b,
Rafael
Almeida
Maciel
b,
Diogo
Ranier
de
Macedo
Souto
a,
George
Neri
de
Barros
Ferreira
aaOrthopedicHospitalforSpecializedMedicine,Brasília,FederalDistrict,Brazil
bGamaRegionalHospital,Brasília,FederalDistrict,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18November2013 Accepted6January2014 Availableonline27October2014
Keywords:
Femoralneckfractures Internalfixators Biomechanics
a
b
s
t
r
a
c
t
Objective:Tostatisticallyanalyzetheresultsobtainedfrombiomechanicaltestsonfixation offemoralneckfracturesofPauwelsIIItype,insyntheticbone,usingthedynamichipsystem withananti-rotationscrew,versusacontrolgroup.
Methods:TensyntheticbonesfromaBrazilianmanufacturer(modelC1010)wereusedand dividedintotwogroups:testandcontrol.Inthetestgroup,fixationofanosteotomywas performedwith70◦ ofinclinationatthelevel ofthefemoralneck,using DHSwithan
anti-rotationscrew.Theresistanceofthisfixationwasevaluated,alongwithitsrotational deviationat5mmofdisplacement(phase1)andat10mmofdisplacement(phase2),which wasconsideredtobefailureofsynthesis.Inthecontrolgroup,themodelsweretestedin theirentiretyuntilfemoralneckfracturingoccurred.
Results:Thetestvaluesinthetestgroup(samples1–5)inphase1 were:1512N,1439N, 1205N,1251Nand1273N,respectively(mean=1336N;standarddeviation[SD]=132N).The rotationaldeviationswere:4.90◦,3.27◦, 2.62◦,0.66◦ and0.66◦,respectively(mean=2.42◦;
SD=1.81◦).Inphase2,weobtained:2064N,1895N,1682N,1713Nand1354N,respectively
(mean=1742N;SD=265N).Thefailureloadingvaluesinthecontrolgroupwere:1544N, 1110N,1359N,1194Nand1437N,respectively(mean=1329N;SD=177N).Thestatistical analysisusingtheMann–Whitneytestshowedthatthetestgrouppresentedmaximum loadingatadisplacementof10mm,i.e.significantlygreaterthanthefailureloadingofthe controlgroup(p=0.047).
Conclusion:Themechanicalresistanceofthetestgroupwassignificantlygreaterthanthat ofthecontrolgroup.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:FreitasA,TorresGM,SouzaACAM,MacielRA,SoutoDRM,FerreiraGNB.Análisedaresistênciamecânicade fixac¸ãodefraturadocolofemoralemossosintéticocomDHSeparafusoantirrotatório.RevBrasOrtop.2014;49:586–592.
夽夽
WorkdevelopedattheOrthopedicHospitalforSpecializedMedicine,Brasília,FederalDistrict,Brazil,andattheMechanicalTest Laboratory,DepartmentofMaterialsEngineering,SchoolofMechanicalEngineering,StateUniversityofCampinas(UNICAMP),Campinas, SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.Freitas).
http://dx.doi.org/10.1016/j.rboe.2014.01.016
Análise
da
resistência
mecânica
de
fixac¸ão
de
fratura
do
colo
femoral
em
osso
sintético
com
DHS
e
parafuso
antirrotatório
Palavras-chave:
Fraturasdocolofemoral Fixadoresinternos Biomecânica
r
e
s
u
m
o
Objetivo: Analisarestatisticamenteresultadosobtidosemensaiosbiomecânicosdefixac¸ão defraturadocolofemoraltipoPauwelsIII,emossosintético,comousodosistemadinâmico doquadril(DHS)comparafusoantirrotatóriovsumgrupocontrole.
Métodos: Foramusadosdezossossintéticos,deumfabricantenacional,domodeloC1010, divididos emdoisgrupos:testee controle.Nogrupoteste foifeitafixac¸ãode osteoto-mia,com70◦ deinclinac¸ãoemníveldecolofemoral,comousodeDHScomparafuso
antirrotatório.Avaliou-searesistênciadessafixac¸ãoeseudesviorotacionalem5mmde deslocamento(fase1)eem10mmdedeslocamento,consideradocomofalênciada sín-tese(fase2).Nogrupocontrole,osmodelosforamensaiadosemsuaintegridadeatéque ocorresseafraturadocolofemoral.
Resultados: Os valores do ensaio no grupo teste na fase 1, nas amostras de 1 a 5, foram:1.512N,1.439N,1.205N,1.251Ne1.273N,respectivamente(média=1.336N;desvio padrão [DP]=132N).Os desviosrotacionais foram:4,90◦;3,27◦;2,62◦;0,66◦ e 0,66◦,
res-pectivamente (média=2,42◦; DP=1,81◦).Na fase 2, obtivemos: 2.064N, 1.895N,1.682N,
1.713Ne1.354N,respectivamente(média=1.742N;DP=265N).Osvaloresdacargade falên-cianogrupocon-troleforam:1.544N,1.110N,1.359N,1.194Ne1.437N,respectivamente (média=1.329N;DP=177N).AanáliseestatísticapelotestedeMann-Whitneydemonstrou queogrupotesteapresentoucargamáxima,em10mmdedeslocamento,significativamente maiordoqueacargadefalênciadogrupocontrole(p=0,047).
Conclusão: Aresistênciamecânicadogrupotestefoisignificativamentesuperioràdogrupo controle.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Hipfractures account for around 20% ofthe surgical frac-turesseenatorthopedictraumaunitsandgeneratesignificant
annual cost in any healthcare system. Femoral neck
frac-turesaccountforapproximately50%ofallfracturesofthehip region.Theymainlyaffectelderlypeopleandareuncommon amongindividualsundertheageof60years.1
TheWorldHealthOrganizationhaspredictedthatthe inci-denceof osteoporoticfractures of the proximalfemur will tripleby2050.2Inthepopulationundertheageof65years,
theincidenceoffemoralneckfracturesis2–4casesper10,000 inhabitants.However,theincidenceismuchhigherinthe
pop-ulationover theageof70years:28/10,000amongmenand
64/10,000amongwomen.3,4
Amongyoungadults,fracturesinthehipregionare gen-erallyuncommon.However,becauseofhigh-energyaccidents involvingsportspracticesandtrafficaccidents,thisincidence
has been increasing. The pattern of this type of fracture
frequentlyhasa verticallinewith unstable characteristics, classified as Pauwels III. This classification correlates the prognosiswiththeangleofthefractureplane:astheangle increases, theinstability ofthefracture also increasesand thecomplications relatingto itsfixation and consolidation worsen.1
Thetreatmentforfemoralneckfractures varies
accord-ingtothepatient’s ageandthefracture pattern.5Inyoung
patients,osteosynthesisshouldalwaysbeprioritized,whilein
olderpatients,arthroplastyshouldbecogitated.For middle-agedpatients(40–65years),theindicationshouldbedefined individually.6
For femoral neck fractures without displacement,
rigid fixation with early mobility for the patients is the
standard treatment. Multiple cannulated screws (MCS) or
the Dynamic Hip System (DHS) is commonly used in the
treatment.5
Failureoffixationandpseudarthrosisarethemainformsof complicationfollowingfixationoffemoralneckfractures,with
or withoutdisplacement.Pseudarthrosisoccurs more
com-monlyandaffectsbetween3.1%and8.8%ofthecases,witha meanofaround6%.1
Inthelightofthesituationdescribedabove,weproposed to conduct a statistical analysis in order to evaluate the mechanicalresistanceofthefixationoffemoralneckfractures classifiedasPauwelsIII,inwhichtheDHSandantirotational
screwswereusedinsyntheticbones,incomparisonwitha
controlgroup.
Material
and
methods
Allthesamplesofthetestgroupwerepreviouslydrilled fortheinitialplacement ofthe implant underfluoroscopic guidancebeforetheosteotomy,inordertofacilitate
anatom-ical reduction and ideal positioning for the implant. The
osteotomiesofthe testgroupwere performedusinga
pre-fabricatedtemplatesothattherewouldnotbeany angular differencebetweenthemandinordertosimulateafemoral neckfractureofPauwelsIIItypethatwouldbethesameinall thebones.
Thefixationsofthefivebonesofthetestgroupwere
per-formedonebyone usingthe DHS,withthree holes and a
guideof135◦.Thereferencepointestablishedforplacingthe
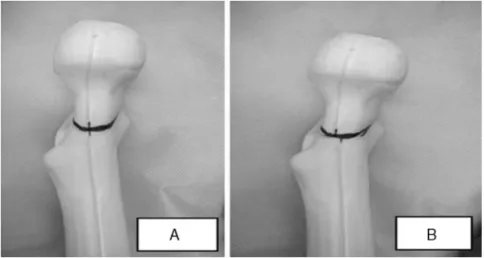
90mmslidingscrewwas2cmdistallytothelessertrochanter, atthecenterofthelateraldiaphysis.Theplatewasfixedtothe femoraldiaphysisusingthree4.5mmcorticalscrews.Lastly, thesystemwaslockedusingacotterpin,whichprovided com-pressiontothefocusoftheosteotomy.Anantirotationalscrew wasthenplacedbyhand,positionedparalleltoandabovethe slidingscrew.Tocheckforcorrectpositioning,fluoroscopyin anteroposteriorandlateralviewswasusedduringeachstage ofthe procedure.After theprocedure, all the bonesinthe testgroup(Fig.1)weresubjectedtoradiographytoevaluate thereductionandwhetherthesynthesiswaswellpositioned (Fig.2).
Theotherfiveboneswereusedwithoutinterferencewith theirintegrityandwereidentifiedasthecontrolgroup.Inthis
manner,theysimulatedthemaximumresistanceloadofthe
femoralneckofintactsyntheticbone.Thus,theydefinedthe goldstandardforresistancepriortotheoccurrenceofthe frac-tureandthecomparisonparameterfortheneedforresistance inthesynthesismethodusedinthetestgroup(Fig.3AandB).
Testgroup
Thefixedsyntheticfemurswere200mminlengthandwere
positioned vertically with an inclination of 25◦ of valgus
(Fig.4A).Theloadapplicationsystemtransmittedtheforce
ontheapex ofthe femoralheadanddetermined theforce
Fig.2–RadiographonsyntheticbonefixedwithDHS beforethetest.
appliedandloadatthetimeoffailure.Theanalysisonthe mechanicaltestonthisgroupwasdividedintotwophases:
Phase1:resistanceofthefixationwith5mmof displace-ment(Fig.4B).
Phase2:resistanceofthefixationwith10mmof
displace-ment,which was taken tobefailure ofthe osteosynthesis
(Fig.4C).
Duringphase1,therotationaldisplacementsofthefemoral neckwerealsoevaluated(Fig.5).
The format ofthis test sought toconcentrate the force
appliedon the focus oftheosteotomy, inorder tomakea
Fig.3–(A)Controlinthemachinebeforethetest.(B)Controlafterthetest,showingfailure.
Fig.4–(A)DHSinthemachinebeforethetest.(B)DHSinphase1ofthetest.(C)DHSinphase2ofthetest.
moreappropriateanalysisontheresistanceofthesynthesis assembly.
Controlgroup
Thenon-fixedsyntheticfemurswere125mminlengthand
werepositionedvertically,withneutralinclination.Theload applicationsystemtransmittedtheforceattheapexofthe
femoralheadandthiswasapplieduntilthefemoralneck frac-tured(Fig.3),inordertosimulatethemaximumpre-fracture resistance.
A load application velocity of 20mm/min was used, in
the Materials Testing System (MTS)machine (model 810 –
FlexTest 40) with a capacity of100kN. In the test, a
cali-bratedand measured loadcell ofcapacity10kNwas used.
An axial force was applied tothe femoralhead by means
Fig.6–Testmachineused.
Table1–LoadvaluesinNwith5mmofdisplacement,
maximumloadvaluesandrotationaldisplacement,in
thetestgroup.
Sample Loadwith5mm
ofdisplacement (N)
Maximum load(N)
Rotation (degrees)
1 1512 2064 4.9
2 1439 1895 3.27
3 1205 1682 2.62
4 1251 1713 0.66
5 1273 1354 0.66
Mean 1336 1742 2.42
Standarddeviation 132 265 1.81
offitting it to the surface of the piston of the equipment (Fig.6).
Statisticalanalysis
Thestatisticalmethodforcomparingthemaximumforce(N)
betweenthegroupswastheMann–Whitneytest.A
nonpara-metricmethodwasusedbecausethemaximumforcedidnot
presentnormaldistribution(Gaussiandistribution),duetothe smallnumberofsamplesanalyzedineachgroup.
Thecriterion usedfordeterminingsignificance wasthe
levelof5%.Thestatisticalanalysiswasprocessedusingthe SAS6.11software(SASInstitute,Inc.,Cary,North Carolina, USA).
Results
Testgroup
TheloadvaluesinNewtons(N)thatwereapplieduntil dis-placementofthefractureby5mmwere:1512,1439,1205,1251 and1273,respectively,forsamples1–5.Themeanvaluewas 1336N,withastandarddeviationof132N(Table1,Fig.7).
Extension (mm)
0
1
2
3
4
5
6
7
8
9 10 11 0
200 400 600 800 1000 1200 1400 1600 1800 2000 2200
Load (N)
1 2 3 4 5
Fig.7–Forcevs.displacementcurveforthetestgroup.
Table2–MaximumloadvaluesinNinthecontrolgroup.
Sample Maximumload(N)
1 1544
2 1110
3 1359
4 1194
5 1437
Mean 1329
Standarddeviation 177
ThemaximumloadvaluesinNewtonsthatwereapplied untildisplacementofthefractureby10mmwere:2064,1895, 1682,1713and1354,respectively,forsamples1–5.Themean valuewas1742N,withastandarddeviationof265N(Table1,
Fig.7).
Therotationaldisplacementvaluesforthefivesamplesin degrees,afterphase1,were:4.90◦,3.27◦,2.62◦,0.66◦and0.66◦,
respectively.Themeanwas2.42◦andthestandarddeviation
was1.81◦(Table1).
Controlgroup
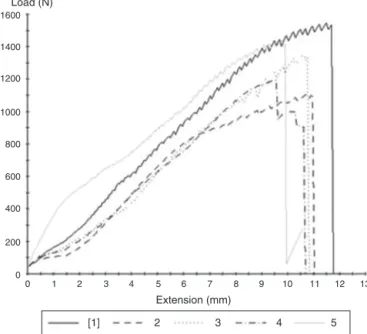
ThemaximumloadvaluesinNewtonsinthefivesamplesof
thecontrolgroupwere,respectively,1544,1110,1359,1194and 1437.Themeanvaluewas1329Nandthestandarddeviation was177N(Table2,Fig.8).
AccordingtotheMann–Whitneytest,itwasobservedthat
thetestgrouppresentedamaximumforceat10mmof
dis-placement that was significantly greater than that of the
controlgroup(p=0.047),asshowninFig.9.
Discussion
1600 1400 1200 1000 800 600 400 200 0
0
1
2
3
4
5
6
7
8
9 10 11 12 13
Extension (mm)
[1]
2
3
4
5 Load (N)
Fig.8–Forcevs.displacementcurveforthecontrolgroup.
A
B
Maximum force (N)
Median p=0.047 2200 2000 1800 1600 1400 1200 1000 800 600 400
Fig.9–Comparisonbetweenthetestgroup(A)andthe controlgroup(B).
healingprocess,soastoallowrapidandsecurerecoveryfor thepatientandareturntoactivitiesofdailyliving.Secure fix-ationalsoreducesthehighratesofcomplicationsrelatingto treatmentsforthistypeoffracture.7
Duringdailyactivities,theloadonthefemoralhead alter-natesanteriorlyandposteriorlyand causesvarusforces.In thepresenceoffracturesthis loadcausesverticalshearing.
Theforceappliedtotheheadofthefemoralneckdepends
onthepatient’sweightandontheactivitycarriedout.These parametersarefundamentalforevaluatingtheresistanceof theimplantincasesoffemoralneckfracture.Inourstudy,we usedanaxialforceof1400Nastheforceappliedtothehip ofanindividualweighing70kgwhoisstandingononeleg.8
ThevaluesobtainedinthesetestsusingtheDHSand antiro-tationalscrews,with5mmofdisplacement,reachedamean loadof1336Nandameanrotationaldisplacementof2.42◦.
However,this osteosynthesis withstood a mean maximum
load of1742N beforefailure, with10mmof displacement. Thisvaluewas significantlyhigher(p=0.047)than theload
withstoodbyanintactsyntheticfemur(controlgroup),which withstoodameanof1329N.
Stiasnyet al.conductedastudythat comparedthe
sur-gicalresultsfrom112patientswhoweretreatedusingMCS, DHSorDHSplusantirotationalscrews.Theyconcludedthat
comparableresultscouldbeobtainedthroughusingMCSor
DHSforsurgicaltreatmentofstablefracturesofthefemoral neck(Gardentypes1and2).Incasesofunstablefracturesof thefemoralneck(Gardentypes3and4),goodresultsfrom thetreatmentdependongoodreductionandstabilizationof thefracture,whichcanbeachievedthroughusingtheDHS. Inthesepatients,withfracturesofGardentypes3and4,the likelihood ofobtaininggood resultsthroughusingtheDHS
wasthreetimesgreater thaninthosewhounderwent
fixa-tionusingMCS.Intheevaluationontheuseofantirotational screws,itwasconcludedthattheiruseinadditiontotheDHS prolongedthedurationofthesurgery,increasedthebloodloss
and didnotimprovethe biomechanicsofthe femoralneck
fixation.9
Inastudyoncadaverbones,Blairetal.comparedthe resis-tanceofbasicervicalfracturefixationusingMCS,DHSorDHS plusantirotationalscrewsandreachedmeanvaluesfor resis-tance toaxial loadingof1736±494NforMCS, 2880±679N forDHSand2903±598NforDHSplusantirotationalscrews.
TheyconcludedthattheDHSwasbiomechanicallysuperior
to MCS for treating femoral neck fractures at the base of
the neck. Moreover, theyobserved that althougha spongy
screw located superiorly would beable to control rotation duringtheinsertionoftheslidingscrewofthehip,itwould notprovideadditionalfixationafterplacementofthissliding screw.10
Biomechanical tests on implants perform a vital role
in evaluating any new implant technology.11 It is difficult
and may be extremely expensive to obtain fresh
cadav-ericbone thatisfreefrom diseases,foruse inmechanical
tests on orthopedic implants.12 Another problem is that
cadaver samples are not uniform, which results in
inclu-sionofsampleswithbonequalityandstrengththatisvery variable.13,14 Differencesin age and degree ofosteoporosis
amongspecimensfromcadaversmayalsopartiallyinfluence thevariabilityofthemechanicalproperties.15,16This
variabil-ityingeometricandmaterialpropertiesofcadaverspecimens frequentlyrequiresprohibitivelylargesamplesizes,inorder to detect statistically significant differences in implant performance.17
Werecognizethelimitationsofourstudy.Useofsynthetic bonesinsteadofbonesfromcadaversdoesnotcorrectly trans-latetheanatomyofthefemoraltrabeculaeandtheforcesthat theycanwithstand.Wedidnotsimulateallthephysiological componentsoftheforce(cyclical,torsionalandaxial)towhich thehipissubjectedduringtheprocessesofwalkingormuscle contractionalone.Directionalforcevectorsmayhaveresulted inchangestotheloadvaluesandconsequentlychangestothe stabilizationoftheimplant.Anaxialloadinasingledirection
does notsimulatethecomplex loadsystemthatisapplied
Syntheticboneswerechosentoensurecomparable biome-chanicalpropertiesbetweenthegroupsandeliminatecertain variables.13Thus,weremovedpossiblevariationsinherentto
humanbonesthatwould cause difficulty inevaluatingthe
methodologyoffixationbecauseoftheirnon-uniform char-acteristics(bonedensity,diameterandlength).
Webelievethattheprincipleofosteosynthesisfor treat-ingfemoralneckfracturesrequiresmethodologythatprovides
absolutestability and that it is improved whenperformed
in a minimally invasive manner. Although the DHS does
notincludetheprincipleofabsolutestability,withor with-out antirotationalscrews, it presentssurprisingly favorable results.9,10 This may contribute towards a less pessimistic
prognosisintreatingunstablefracturesofthefemoralneck.
Wesuggestthatnewstudiesshouldbeconducted.These
couldmakeuseofthepresentresultstodevelopnewimplants thatwouldrespecttheneedforabsolutestabilityandcouldbe
implementedinaminimallyinvasivemanner.
Conclusion
Theanalysisshowedthatthe mechanicalresistanceofthe
testgroupwassignificantlygreater thanthatofthecontrol groupandestablishedthepossibilitythattheDHSand antiro-tationalscrewscanbeusedforosteosynthesisoffemoralneck fractures,especiallythoseofPauwelstypeIII.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
ToProf.AnaPatríciaPaula, supervisorofthe master’s pro-gramoftheFoundationforTeachingandResearchinHealth Sciences(FEPECS),forherunconditionalassistance.
r
e
f
e
r
e
n
c
e
s
1. KeatingJ.Fracturesoftheneckoffemur.In:BucholzRW, HeckmanJD,Court-BrownCM,editors.RockwoodandGreen’s fracturesinadults.7thed.Philadelphia:LippincottWilliams &Wilkins;2010.p.1561–87.
2. CooperC,CampionG,MeltonLJ3rd.Hipfracturesinthe elderly:aworld-wideprojection.OsteoporosInt. 1992;2(6):285–9.
3.SingerBR,McLauchlanGJ,RobinsonCM,ChristieJ. Epidemiologyoffracturesin15,000adults:theinfluenceof ageandgender.JBoneJointSurgBr.1998;80(2):243–8.
4.CummingsSR,NevittMC,BrownerWS,StoneK,FoxKM, EnsrudKE,etal.Riskfactorsforhipfractureinwhitewomen. StudyofOsteoporoticFracturesResearchGroup.NEnglJMed. 1995;332(12):767–73.
5.Yih-ShiunnL,Chien-RaeH,Wen-YunL.Surgicaltreatmentof undisplacedfemoralneckfracturesintheelderly.IntOrthop. 2007;31(5):677–82.
6.SendtnerE,RenkawitzT,KramnyP,WenzlM,GrifkaJ. Fracturedneckoffemur–internalfixationversus arthroplasty.DtschArzteblInt.2010;107(23):401–7.
7.KaplanT,AkesenB,Demira ˘gB,BilgenS,DurakK. Comparativeresultsofpercutaneouscannulatedscrews, dynamiccompressiontypeplateandscrewforthetreatment offemoralneckfractures.UlusTravmaAcilCerrahiDerg. 2012;18(1):65–70.
8.DenhamRA.Hipmechanics.JBoneJointSurgBr. 1959;41B:550–7.
9.StiasnyJ,DraganS,KulejM,MartynkiewiczJ,PłochowskiJ, DraganSŁ.Comparisonanalysisoftheoperativetreatment resultsofthefemoralneckfracturesusingside-plateand compressionscrewandcannulatedAOscrews.Ortop TraumatolRehabil.2008;10(4):350–61.
10.BlairB,KovalKJ,KummerF,ZuckermanJD.Basicervical fracturesoftheproximalfemur.Abiomechanicalstudyof3 internalfixationtechniques.ClinOrthopRelatRes. 1994;(306):256–63.
11.ChouekaJ,KovalKJ,KummerFJ,CrawfordG,ZuckermanJD. Biomechanicalcomparisonoftheslidinghipscrewandthe domeplungereffectsofmaterialandfixationdesign.JBone JointSurgBr.1995;77(2):277–83.
12.SzivekJA.Syntheticmaterialsandstructuresusedasmodels forbone.In:AnYH,DraughnRA,editors.Mechanicaltesting ofboneandthebone-implantinterface.BocaRaton:CRC Press;1999.p.159–75.
13.CristofoliniL,VicecontiM,CappelloA,ToniA.Mechanical validationofwholebonecompositefemurmodels.JBiomech. 1996;29(4):525–35.
14.MartiA,FankhauserC,FrenkA,CordeyJ,GasserB. Biomechanicalevaluationofthelessinvasivestabilization systemfortheinternalfixationofdistalfemurfractures.J OrthopTrauma.2001;15(7):482–7.
15.HeinerAD,BrownTD.Structuralpropertiesofanewdesignof compositereplicatefemursandtibias.JBiomech.
2001;34(6):773–81.
16.BolligerNetoR,RossiJD,LeivasTP.Experimental
determinationofbonecortexholdingpoweroforthopedic screw.RevHospClinFacMedSaoPaulo.1999;54(6): 181–6.