T
HYROID
AUTOANTIBODIES IN HEALTHY
VENEZUELANS
M. S2nchez-Borges,2 J. L. CeuaZZos,3 R. Stiikez-Chachz, 2 K GaZZego, 2 M. L6peq3 A. 0rozc0,~ R. Drayer, 3
M. C. SaZas, 3 and I? de Zos RZo#
I
NTRODUCTION
The clinical significance of an- tibodies reacting with thyroid antigens in apparently healthy individuals is uncer- tam (I). Some authors claim those anti- bodies provide evidence of chronic thy- roiditis (2) , a point of view supported by the presence of lymphocytic infiltration in thyroid glands from autopsied anti- body-positive subjects without overt thy- roid disease (3, 4). However, other inves- tigations have not found thyroid antibodies in patients with biopsy- proven thyroiditis (3, S).
A previous article by mem- bers of our group reported on the signifi- cance of antithyroid microsomal anti- bodies in the diagnosis of thyroid autoallergic disease (6). However, there have been no studies in Venezuela on the prevalence of thyroid antibodies among the general population, and this preva-
1 The work reported here was supported by the Venezue- lan Foundation of Immunology (Fundaci6n Venezo- lana de Inmunologia-FUNVENI). This article will also be published in Spanish in the Boletin de la Ofi- &a Sanitaria Panamericana, vol. 104, 1988. * Immunology Laboratory, Oncology Chemotherapy and
Hematology Center, M.S.A.S., P.O. Box 20253, Cata- cas 1020, Venezuela.
3 Clinical Research Laboratory, “Luis Ratetti” School of Medicine, Medical Faculty, Central University of Vene- zuela, Caracas, Venezuela.
lence has an extremely important bear- ing on how to interpret detection of such antibodies in people with symptoms sug- gesting thyroid disease. Accordingly, the study reported here was designed to es- tablish the prevalence, as well as the clin- ical and physiopathologic implications, of thyroid-specific antibodies in appar- ently healthy individuals residing in Caracas.
M
AmlWiLSAND
METHODS
The study sample included
145 healthy volunteers (111 females and 34 males) recruited at their places of work. These individuals were textile fac- tory workers, medical students, and lab- oratory personnel. Their age and sex dis-
tributions are presented in ‘Table 1. % m 1 All the subjects were ques- - tioned about any possible personal or s family history of thyroid or other endo- 2 crine diseases. Specific inquiry was made .g QJ
3 2
2
TABLE 1. Aqe and sex distributions of the study group.
Age (in years) Females Males Total 15-24 27 1; 34
25-34 33 49
35-44 43 IO 53
245 8 1 9
Total 111 34 145
Average age
+ 1 standard deviation 32.8 +- 8.4 30.2 + 6.5 31.5 iT 9.1
regarding the following symptoms: as- thenia, cold or heat intolerance, diar- rhea, constipation, bradypsychia or ta- chypsychia, dry or sweating skin, dys- phonia, insomnia, sleepiness, hair loss, brittle nails, menstrual disturbances, de- creased sexual appetite, depression, anxi- ety, obesity, weight loss, anorexia, tremor, muscle strength loss, palpita- tions, chest pain, and exophthalmos.
The physical examination of the subjects included measurement of their weight, height, pulse rate, blood pressure, thyroid size and consistency, and osteomuscular reflexes. We consid- ered that the size of a normal thyroid gland (designated In) was that of a gland weighing approximately 20 g.
Sera were obtained from blood specimens after clotting the blood at room temperature, and were stored at
- 70°C.
Serum antithyroglobulin and antimicrosomal thyroid antibodies were measured by means of the passive he- magglutination test (Fujirebio Inc., To- kyo, Japan) kindly donated by Dr. N. Amino of Osaka, Japan. A titer of 1: 20
or more was considered positive for both antimicrosomal and antithyroglobulin antibodies. Thyroid-stimulating hor- mone (TSH) and free thyroxine (T4) in the study sera were measured by ra- dioimmunoassay (Amersham Interna- tional PLC, England). Thyroid function data were analyzed by Student’s t test.
ICE
SULTSGoiter
Abnormally large thyroids
( L 1.5n) were found in 35 individuals (24.1% of the study group). These in-
cluded 28 women (25.2 % of the female study subjects) and seven men (20.5 % of the male study subjects).
Antithyroid antibodies
The incidence of antithyroid antibodies is shown in Table 2. The posi- tive titers observed ranged from 1: 100 to 1: 26,214,400 for antimicrosomal anti-
bodies and from 1: 400 to 1: 6,400 for antithyroglobulin antibodies. It can be seen that antimicrosomal antibodies were found in 16 subjects (11 %), there being a higher prevalence in females (13.5%) than in males (2.9%).
TABLE 2. AnMhymid antibodies found in the study population of apparently healthy individuals, by sex.
Study population Males Females Total
No. of persons
34 111 145
Positive for antimicrosomal
antibodies No. (%I
(2.9) 1: (13.5) 16 (11.0)
Positive for antiihyroglobulin
antibodies No. (%I
0 (0) 4 (3.6) 4 (2.8)
Positive for antimicrosomal and
antithyroglobulin antibodies No. (%I
0 (0) 2 (1.8) 2 (1.4)
mal antibodies than those without goi- roid disease; seven (43.7%) had symp- ter, as indicated in Table 3, but this was toms suggestive of thyroid disease; and not statistically significant. five (31.2 %) had goiter.
Antithyroglobulin antibodies without antimicrosomal antibodies were found in four of the study subjects
(2.7%). All four were females, and three of the four had goiter. Only two study subjects had both antimicrosomal and antithyroglobulin antibodies; both of these were female subjects with goiter (see l&bles 2 and 3).
Thyroid Function
In order to determine whether possible functional disturbances existed among the subjects with thyroid autoallergy, the free T4 and TSH in their sera were measured.
Table 4 gives a brief list of clinical characteristics associated with thyroid disease that were found among some of the 16 subjects with antimicroso-
mal antibodies. Three (18.7%) had a family history of thyroid disease; two (12.5 % ) had a personal history of thy-
Table 5 presents the results of these hormonal determinations. It can be seen that the average level of free T4
TABLE 3. Antfthymid antibodies in study subjects with and without gdkr.
Subjects without goiter (thyroid size < 1.5n) Subjects with goiter
(thyroid size 2 1.5n)
No. of study subjects
110 35
Positive for Positive for antimicrosomal antithyroglobulin
antibodies antibodies No. (%) No. W)
11 (10.0) 1 (0.9) 5 (14.2) 3 (8.5)
Positive for anQmicrosomal and
antithyroglobulin antibodies No. (%I
TABLE 4. Clinical characteristics associated with thyroid disease that were found among the 16 study subjects with antfmicrosomal antibodies. Fiffeen of these 16 sub- jects were females, and the average age of the 16 was 35.7 years with a standard deviation of 27.2 years.
Clinical findina
Study
subjects No. (%I Family history of thyroid disease 3116 (18.7%) Personal history of thyroid
diseasea 2116 (12.5%) Symptoms suggestive of thyroid
diseaseb 7116 (43.7%) Goiter (thyroid size 2 1 Lin) 5116 (31 2%)
d Bath had simple goiter. We considered them “apparently heailhy” be- cause the goiter had turned up as an Incidental finding during a previous routine medical examination given to apparently healthy people. b The most frequently observed of these symptoms were a:,thenia. consti-
pation, dry skin, hair loss, menstrual disturbances, and weight increases.
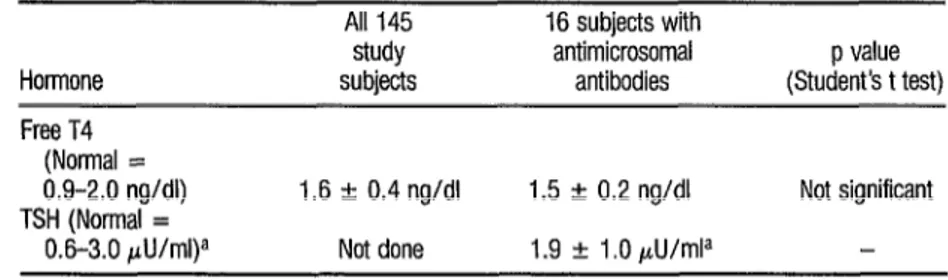
was normal in sera from the whole popu- lation sample (1.6 f 0.4 ngldl), and also in sera from the subjects with anti- microsomal antibodies (1.5 + 0.2 ng/
dl). Indeed, only one of the 16 subjects with antimicrosomal antibodies showed an abnormally high serum level of free T4 (2.1 ng/dl).
The level of TSH in serum was determined only for individuals with antimicrosomal antibodies. The average TSH value was within normal limits (1.9
+ 1 .O microunits per milliliter) and
none of the 16 subjects was found to
have an abnormally high serum level of this hormone.
Overall, the thyroid function of individuals with thyroid antibodies appeared normal4
D
ISCUSSION
It is generally accepted that thyroid autoantibodies are associated with autoallergic thyroid disease. Some 95 % of the patients with goitrous Hashi- mote’s thyroiditis have antimicrosomal antibodies, and 70% have antithyroglo- bulin antibodies (7, 8). High titers of both antibodies are also found in pa- tients with Graves’ disease.
Because of their complement- fixing properties, greater pathogenetic
4 In our opinion the one subject with microsomai anti- bodies and increased T4 did not have Graves’ disease because he had neither obvious symptoms nor abnor- malities detected at the physical examination. It is con- ceivable that he could have had what some authors call “subclinical disease.”
TABLE 5. Free T4 and TSH found in the sera of all study subjects and those with antimicrosomal antibodies. The values shown are average values 2 one standard deviation.
All 145 16 subjects with
study antimicrosomal p value Hormone subjects antibodies (Student’s t test) Free T4
(Normal =
0.9-2.0 ng/dl) 1.6 + 0.4 ng/dl 1.5 r 0.2 ng/dl Not significant TSH (Normal =
0.6-3.0 pU/ml)a Not done 1.9 + 1 .O @mla
significance has been ascribed to antimi- crosomal antibodies, a view further sup- ported by the presence of microsomal an- tigen at the thyroid cell membrane (9).
The incidence of thyroid au- toantibodies among the general popula- tion varies in ways that could depend on geographic, ethnic, genetic, or other fac- tors. For example, Volpe has observed that up to 16% of elderly women have thyroid autoantibodies whose presence correlates with occult thyroid disease, and that most individuals with antimi- crosomal antibodies do not have overt Hashimoto’s disease (7). Also, Hawkins and coworkers have reported that up to 16 % or more of the elderly have thyroid autoantibodies (I 0).
These same authors (10) have found a 6.7 % prevalence of antimicroso- ma1 antibodies among healthy people (9.8% in females and 2.8% in males), while in the present study we found a prevalence of 11% in the whole sample (13.5% in females and 2.9% in males). Our results are similar to those reported by Amino et al. (11).
Other population differences have been reported by Mittra et al., who found a higher incidence of microsomal and thyroglobulin antibodies in healthy British women than in healthy Japanese women (12).
In our study, we found the overall prevalence of antithyroglobulin antibodies to be 2.7 % , which is higher than the percentage reported by Ericsson et al. for Swedish people (1) but lower than the prevalence reported in Australia by Hawkins’ group (10). On the other hand, the prevalence we found of anti- thyroglobulin antibodies in women (3.6 %) was lower than the prevalences reported elsewhere in Australian (9.8 % ) , British (9.9%), and Japanese (5.2%)
women (12).
Variable antithyroglobulin antibody frequencies have also been re- ported in other populations. For exam- ple, Dingle et al. found a prevalence of 16 % among females and 4 % among males in Northeast England (13); Couch- man et al. found prevalences ranging from 2 % to 15 % in New Zealand women, depending on their age (14). Gordin has reported prevalences of 8% to 11% for Finnish people (15), and Tunbridge has reported finding a 2% prevalence in England (16). Some of the variations appear to arise from methodo- logic differences and also from the cutoff values used as criteria for positivity. Among other things, it has been sug- gested that the enzyme-linked immuno- sorbent assay (ELISA) and radioimmu- noassay are more sensitive than hemagglutination, immunofluorescence , or complement furation (I, 8, 12). Un- fortunately, we have not been able to find information in the literature dealing with antithyroid antibodies in Latin
American populations. 2 An intriguing question is the 8 relative importance of antimicrosomal $ and antithyroglobulin antibodies in the E diagnosis of autoallergic thyroid disease. 5 In this respect, we found that our normal e population had a higher prevalence of
antimicrosomal antibodies (11% ) than 3 of antithyroglobulin antibodies (2.7 % ), Q a finding different from that reported by
Irvine, who found 15 % of his study pop- E ulation to have antimicrosomal antibod-
s
ies and 17% to have antithyroglobulin . antibodies (17). 4; -3
2 2 P 4
2 3 $2 2
Like other authors, we found thyroid antibodies more frequently in women than in men. This is not an unex- pected observation, since it is well known that antibody responses are stronger in the female sex and that autoantibodies and autoallergic diseases occur more of- ten among women.
The high prevalence of goiter among our study subjects (a prevalence of 24%) clearly deserves notice. How- ever, no correlation was found between thyroid autoantibodies and goiter, since only 14% of those with goiter were found to have antimicrosomal antibod- ies. We postulate that other unidentified causes, distinct from autoallergic thyroid disease, must be responsible for the high prevalence of enlarged thyroid glands found in our study subjects.
Regarding thyroid function, we found that levels of free T4 and TSH were normal in the sera of antibody-posi- tive subjects. These results do not agree with those of Hawkins et al., who ob- served increased serum TSH in 72 % of a group of subjects with persistent antimi- crosomal antibodies (10). However, the apparent discrepancy should be inter- preted cautiously, since some authors have suggested that serum levels of T3, T4, and TSH may be variable in Hashi- moto’s thyroiditis-depending on the degree of lymphocytic infiltration versus the degree of follicular hyperplasia of the % gland (18)-and that an increase of se- 2 rum TSH in response to an intravenous
.
s bolus of thyrotropin-releasing hormone 2 would be a better indication of subclini-
.g cal thyroid dysfunction (19, 20).
172
It appears that follow-up of antibody-positive individuals could help to define the clinical significance of thy- roid autoantibodies in healthy people. In this regard, Volpe has stated that about
10% of such people will develop overt disease within 10 years (7).
Our results support the con- cept that autoallergic phenomena occur in the absence of clinical or physiologic disturbances. Interestingly, Ruf et al. (21) have recently found identical fine specificities for antithyroglobulin anti- bodies in subjects with normal and path- ologic conditions. On the basis of their results, they theorize that autoantibodies are produced in normal subjects but are kept at low levels by regulatory processes that fail with respect to selected epitopes in autoimmune diseases (21).
C
ONCLUSIONS
l A high incidence of goiter
(24.1% ) was observed among a group of 145 apparently healthy study subjects.
. Antithyroid microsomal anti- bodies were found in 11% of the study subjects, and antithyroglobulin antibod- ies were found in 2.7 % .
. No correlation was found be- tween increased thyroid size and the presence of thyroid autoantibodies.
0 Levels of free T4 and TSH in the sera of subjects with antithyroid anti- bodies were within normal limits.
l These results suggest the exis-
tence of thyroid autoallergy without clin- ical disease.
A
CKNOWLEDGMENTS
To help assess the frequency of thyroid autoantibodies in the general population of Caracas, a sample popula- tion of 145 healthy individuals was stud- ied. A high incidence of goiter (24%)
was found. Antimicrosomal antibodies were found in 11% of the study subjects
(13.5% of the women, 2.9% of the men), whereas antithyroglobulin anti- bodies were found in 2.7 % (3.6% of the women and none of the men).
No correlation was observed between the presence of antithyroid anti- bodies and the presence of goiter. Healthy subjects with antithyroid anti- bodies in their sera appeared to have nor- mal thyroid function, as indicated by se- rum levels of free T4 and TSH. We conclude that thyroid autoallergy is com- mon in our healthy population and does not necessarily imply a morbid state.
t
IL
FERENCES
Ericsson U-B., S. B. Christensen, and J. I. Thorell. A high prevalence of thyroglobulin autoantibodies in adults with and without thy- roid disease, as measured with a sensitive solid- phase immunosorbent radioassay. C&z Im- mund Immunophd 37: 154-162, 1785. Doniach, D., G. F. Bottazzo, and R. C. Rus- sell. Goitrous autoimmune thyroiditis Hashi-
I moto’s disease). C&z Endocrind Metu 8:63- 80. 1777.
Goudie. R. B., J. R. Anderson, and K. G. Gray. Complement-fLuing antithyroid anti- bodies in hospital patients with asymptomatic thyroid lesions. J Pathd Batted 771387400, 1757.
Loeb, P B., A. L. Drash, and F. M. Kenny. Prevalence of low-titer and “neeative” anti- thyroglobulin antibodies in biopiy-proved ju- venile Hashimoto’s thyroiditis. J Pediatr 82:17-21, 1973.
Bastenie, P. A., P. Neve, M. Bonnyns, L. VanhaeLst, and M. ChaiIly. Clinical and patho- logical significance of asymptomatic atrophic thyroiditis: A condition of latent hypothyroid- ism. &z?zcet l:Y15-918, 1967.
Suarez-Chacon. R., and M. Sanchez-Barges. Laboratory diagnosis in thyroid autoallergic diseases. Ah’erPol Immunobathd (Ma& 14:15-20, 1986: ,. , , VolpE, R. Autoimmune thyroid disease. Hos- pital Practice 17:141-158, 1984.
Wall, J. R., and T Kuroki. Immunologic fac- tors in thvroid disease. Mea’ CLn North Am 67:713-736, 1985.
Chiovato, L., P. Vitti, A. Lombardi, L. D. Kohn, and A. Pinchera. Expression of the mi- crosomal antigen on the surface of continu- ously cultured rat thyroid cells is modulated by thyrotropin. J Chn Endocrind Metab 61: 12- 16, 1985.
10 Hawkins, B. R., R. L. Dawkins, H. G. Burger, I. R. Mackay, P. S. Cheah, S. Whittingham, Y. Patel, and T. A. Welbom. Diagnostic signifi- cance of thvroid microsomal antibodies in a randomly selected population. Lancet 2: lO57- 1057, 1780.
11
12
13
14
Amino, N., S. R. Hagen, N. Yamada, and S. Refetoff. Measurement of circulating thyroid microsomal antibodies by the tanned red cell haemag lutination technique: Its usefulness in the ragnosis of autoimmune thyroid dis- cf eases. Ckn Endoctinol5:115-125, 1976. Mittra, I., I. Perrin, and S. Kumaoka. Thyroid and other autoantrbodies in British and Japa- nese women: An epidemiological study of breast cancer. BrMedJ 1:237-239, 1776. Dingle, P. R., A. Ferguson, D. B. Horn, J. Tubmen, and R. Hall. The incidence of thyro- globulin antibodies and thyroid enlargement in a general practice in North-East England. C/in Exp Immund 1:227-284, 1966. Couchman, K. G., R. D. Wigley, and I. A. M. Prior. Autoantibodies in the Carterton po
15 Gordin, A., l? 0. Heinoner, I? Saarinen, and B. A. Lamberg. Serum thyrotropin in symp- tomless autoimmune thyroiditis. Lancet 1:551-554, 1972.
16 Tunbridge, W. M. G., D. C. Evered, R. Hall, D. Appleton, M. Brewis, F. Clark, J. Grimley Evans, E. Young, T. Bird, and P A. Smith. The spectrum of thyroid disease in a commu- nity: The Wickham survey. C&z Endocrhol (Oxf 7:481-473, 1777.
17 Irvine, W. J. Auto-immunity and endocrine disorders. Practitioner lYY:lSO, IYGG.
New Video
Fmgram
Available
on Natural
Disasters
18 Tunbridge, W. M. G., M. Brewis, J. M. French, D. Appleton, T. Bird, E Clark, D. C. Evered, J. Grimley Evans, R. Hall, P Smith, J. Stephenson, and E. Young. Natural history of autoimmune thyroiditis. Br Med J 282:258-
262, 1781.
17 Gordin, A., and B. A. Lamberg. Natural course of symptomless autoimmune thyroidi- tis. Luncet 2:1234-1238, 1975.
20 Bastenie, P. A., N. Bonnyns, and L. Vanhaelst. Grades of subclinical hvnothvroid- ism in asym
revealed by t R tomatic autoimmune*thyroiditis e thyrotropin-releasing hormone test. J Chz Edocrinol Metab 51:163-166,
1980.
21 Ruf, J., P. Carayon, and S. Lissitzky. Various expressions of a unique anti-human thyro- globulin antibodv repertoire in normal state and autoimmune disease. Ew J Immunol
15:268-272, 1785.
PAHO’s Emergency Preparedness and Disaster Relief Coordination Program has produced a new 25-minute video program entitled “Myths and Realities of Natural Disasters.” It addresses the most commonly held myths regarding the
health outcomes of disasters in an effort to guide the utilization of scarce resources.
For reasons ranging from lack of prior planning to demands made by a fearful population, wasteful recovery measures are sometimes taken in the aftermath of a disaster. The donor community that so generously offers help may be an unwitting accomplice in counterproductive activities because of lack of information about real needs.