A
HOSPITAL
STUDY OF ILLEGAL ABORTION IN
BOLIVIA1
Pa&i& E. Baidey,,2 Lois Llano Saavedra,3 Lzh Kzm?iner,4 Michael WeZsh, 5 and Barbara Janowitzd
IN
TRODUCTION
Illegal abortions are associated with high rates of maternal morbidity and mortality, and treatment of women hospitalized for illegal abortions draws upon scarce medical resources. Hence, in countries where induced abortions are il- legal their adverse consequences consti- tute a serious public health problem.
Abortion is only permitted in Bolivia when a woman’s physical health is threatened by pregnancy or when she has been the victim of rape or incest; oth- erwise it is illegal (1). However, such ille- gal abortions are commonplace. Indeed, in the 1970s the Bolivian Ministry of Public Health estimated that the treat- ment of complications arising from ille- gal abortions accounted for more than
60% of the country’s obstetric and gyne-
cologic expenses (2). In this same vein, a 1983 publication that reported maternal mortality as being 48 deaths per 10,000
live births stated that 27% of these
’ Support for the project reported here was provided by Familv Health International under a coooerative aeree- ment &h the U.S. Agency for Interna~onal Deviop- ment (DPE-0537-A-00-4047-00). This article wili also be published in Spanish in the BoLetetin de k Oj;,i,a Sanitati Panamericana, vol. 104. 1988.
* Senior Research Analyst in the Division of Program Evaluation. Family Health International, Research Xi- angle Park, North Carolina 27709. USA.
deaths were related to induced abortion complications (3).
Bolivia’s population as of 1986
was estimated at about 6.4 million in- habitants. The off&l population policy has been to promote growth by encour- aging immigration and maintaining cur- rent levels of fertility. Direct measures have been taken to maintain these fertil- ity levels by closing family planning clin- ics (4). No government support is pro- vided for family planning services, making the private sector the primary source of contraception. A 1983 contra- ceptive prevalence survey found that
24 % of the married women 15-49 years of age were using contraceptive methods; of these, 14% were using rhythm and other traditional methods, while 10%
were using modern clinical methods.
3 Family Counseling Center (Centro de O&ntaci&z Fa- $ m&a), Ia Paz, Bolivia.
4 Physician, Family Counseling Center, La Paz. 5 Senior Program Coordinator for Iatin America, Family
Health International.
2 . 6 Associate Director for the Division of Program EvaIua- 2
tion, Family Health International. .g u a
Pharmacies and private medical clinics were the most commonly reported sources of contraceptive services (,), As of 1984, the nation’s crude birth rate was estimated at 40 births per 1,000 popula- tion per year, and women who had fin- ished child-bearing had an average of six children (5).
A lack of data on abortion and its medical sequelae led members of the Bolivian Society of Gynecologists and Obstetricians to conduct a study of women hospitalized for complications of abortion. The study’s immediate aims were to determine these hospitalized women’s sociodemographic characteris- tics, the proportion of abortions that were illegally induced, the patients’ symptoms, the complications involved, the medical treatment provided and hos- pital resources used, the patients’ patterns of contraceptive use before hospitalization, and their subsequent contraceptive plans. Ultimately, the pur- pose was to provide policymakers with data that would help them design family planning components for maternal health care programs, so as to reduce the rates of unwanted pregnancy and illegal abortion.
M
ATERIALSAND
METHODS
2
: J
From 1 July 1983 through 30une 1984, data were collected on all z
2
women admitted to a sample of Bolivian hospitals for treatment of complications .j$
9, associated with pregnancy wastage. Q
3
These included the 11 major hospitals in the country’s five largest cities (Cocha-
5
bamba, La Paz, Oruro, Santa Cruz, and
n, Sucre). In each city a Ministry of Health (MOH) and a Social Security (SS) hospital were chosen; and in the case of La Paz
28 two private hospitals were also chosen.
Hospitals within the country’s three main geographic regions (the high plains, valleys, and tropical and subtrop- ical plains) were included in this sample.
Physicians from each partici- pating center were trained to complete questionnaires that included informa- tion about the patient’s sociodemo- graphic characteristics, obstetric and contraceptive history, condition at admis- sion, medical treatment during hospital- ization, and reproductive and contracep- tive plans.
At admission, the attending medical personnel classified each case of abortion as definitely or probably spon- taneous, or (alternatively) definitely or probably induced. This classification was based upon information reported by the patient and the attending physician. If the patient said the abortion was in- duced, it was coded as such. If she said it was spontaneous, but there was clinical evidence to the contrary (such as cervical lacerations), it was coded as induced-ei- ther by the physician or at Family Health International.’
Even so, the final result was ahnost certainly an underestimate of the true number of induced abortions. For even when abortion is legal, many women do not wish to admit that they have terminated a pregnancy (61. It is
therefore likely that there were some cases of induced abortion that showed no overt clinical evidence and that were said by the women involved to be spontane- ous. If induced abortions (particularly these without complications) were underreported as a result, then the com- plication rate among induced cases was probably overestimated.
Rx
WETS
Characteristics of the Patient
Population
During the year-long study period a total of 4,37 1 women were ad- mitted to the participating hospitals with complications associated with pregnancy loss. Of these women, 28 % were from La Paz, the city with the largest population, 2 5 % were from Cochabamba, 18 % from Santa Cruz, 16% from Oruro, and 13% from Sucre. Nine hundred and ninety- two (23%) of the abortions involved were classified as illegally induced, and 3,379 (77 % ) were classified as spontane- ous (Table 1). The share of abortions clas- sified as induced, by city, ranged from 42 % in Oruro to 15 % in La Paz.
The percentage of abortions classified as induced (see the third col- umn of Table 1) was negatively associated with age, ranging from 39% among women 17 years of age or younger to 18% among women over 29. The per- centage of induced abortions was much higher among women not currently in any union than among those who were in
a consensual union or married. The per- centage of induced abortions was also higher among the study subjects who had been pregnant for the first time (31% induced) than it was among those who had experienced at least one pre- vious pregnancy (22 % induced). The pa- tients’ level of education was not associ- ated with the proportion of abortions induced, nor was their previous abortion experience.
Regarding previous abortions, a relatively small share (16.5 % ) of the women hospitalized for an earlier abor- tion were classified as currently having an induced abortion, while a larger share (39.1%) of the women who had not been hospitalized for an earlier abortion were classified this way (see Table 1). These data are difficult to interpret, be- cause previous abortions were not identi- fied as spontaneous or induced. It is evi- dent, however, that nearly half of all the women studied had experienced a pre- vious abortion, and that three-quarters of those with known prior abortions had also been hospitalized.
Patient Complications,
‘Ikatment, Length of Hospital
Stay, and Mortality
Table 2 indicates that women classified as having a spontaneous abor- tion were admitted with far fewer com- z plications and generally received less 5 treatment than those classified as having 5 an induced abortion. Women with in- R duced abortions were more likely to have 5 a fever exceeding 38°C infection, trau- 2 matic lesions (such as cervical or vaginal . lesions), and excessive blood loss than s were women with spontaneous abor- ; tions. They were also more likely to re- 3 ceive antibiotics and blood transfusions % t3 (but not anesthesia, IV fluid, or oxy-
tocins) than those with spontaneous abortions.
Q
TABLE 1. Percentage distribution of the patients admitted for treatment following abortion according to their age, education, marital status, number of liking children, occurmnce of previous pregnancy, and previous abortion experience. The table also shows the percentage of patients in each gmup who were claMed as having in- duced abortfons.
Abortions Patients classified No. W) inducz (%) Patient age:
14-17years 18-19 tt 20-29 // 230 fl Unknown Education:
Non& Primary
2 secondary Other Unknown
Marital status:
Never in union Consensual union Married
Divorced, separated, or widowed !/umber of living children:
0
1 2 3 4 r5
First pregnancy: Yes No
Previous abortion: b Yes
Hospitalized Not hospitalized No
Total
114 (2.6) (38.6) 244 (5.6) (30.3) 2,349 (53.7) (24.2) 1,658 (37.9) (18.3)
6 (0.1) -a 418 (9.6) (23.9) 1,693 (38.7) (23.0) 2,254 (51.6) (22.2)
4 (0.1) -a 2 (0.1) -a 447
571 3,229 124
(10.2) (13.1) (2
(46.3) (23.6) (18.0) (54.8) 697 (15.9)
897 (20.5) 896 (20.5) 678 (15.5) 502 (11.5) 701 (16.0)
(25.8) (19.5) (21.4) I;;.;{ (24:0) 494 (11.3) (31.3) 3,877 (88.7) (21.6) 1,775 (45.8)
1,334 (34.4) 441 (11.4) 2,102 (54.2)
(22.3) (16.5) ~YIij (22.7) 4,371 (100.0)
<
CL a Less than 25 cases.
ry
-4 b Includes only the 3,877 women wilh prior pregnancies. R
TAME 2. Condiin and tmafment of the study patients with induced and spon- bayous abortions, showing the compliions existing at admission, types of treatment received during hospitalization, number of days hospitalized, and case- fatalll rate.
% of patients with % of all abortions classified as: patients Spontaneous Induced (n = 4,371) (n = 3,379) (n = 992)
Compkations:
Fever Infection
Eaxsslve blood loss Lesions
Treatment at hospital: General anesthesia Blood transfusion IV fluid
Antibiotics Oxytocins
No. of days hospitalzcxf: 0
1
2 3 r4
Case fatality ratea
8.6 12.0 34.0 4.8
95.4 6i:i
66.5 71.1
0.6 0.3 1.8 38.9 41 .I 31.2 35.4 37.2 29.3 15.7 13.8 22.0 9.4 7.6 15.7 1.6/1,000 0.3/1,000 6/l ,000
3.1 5.7 32.0 0.0
96.3 92.1 6.2 11.9 64.6 65.5 60.9 85.8 70.6 72.8 27.7 33.2 40.8 21.2
a Number of deaths divided by number of cases.
Hospital stays (perhaps the best overall indication of resource use) were significantly longer for women with induced abortions. More than a third of those with induced abortions spent three or more days in a hospital, as com- pared to 21% of those with spontaneous abortions.
Due to abortion-related com- plications, 20 women, 16 of whom had reported induced abortions, received a total hysterectomy. Of these 20, 15 were less than 30 years of age and five had no living children. Besides the high per- sonal cost to these women, the use of
hospital resources was considerable, with each woman spending an average of 17 days in a hospital.
Seven women died during their hospitalization, one as a conse- quence of an incomplete spontaneous abortion. The case-fatality rate among the 992 patients classified as having in- duced abortions was six per thousand, as compared to 0.3 per thousand among women classified as having spontaneous abortions.
Among the patients who died from complications associated with in- duced abortion, one woman 29 years of age was diagnosed as having an ectopic pregnancy as well as a perforated uterus. A hysterectomy was performed, but she died within 24 hours. Another patient was a 35year-old mother of two living children who arrived at the hospital in a state of septic shock. Her abortion had been induced by a medically untrained person, and she had been suffering
symptoms for 15 days before seeking treatment. She died within three hours of arrival, before any surgical interven- tion. A third patient, this one 23 years of age with one child, came to the hospital with peritonitis plus cervical and uterine perforations. Several surgical procedures were performed during a hospital stay that lasted 50 days.
Procedures Used to Induce
Abortion
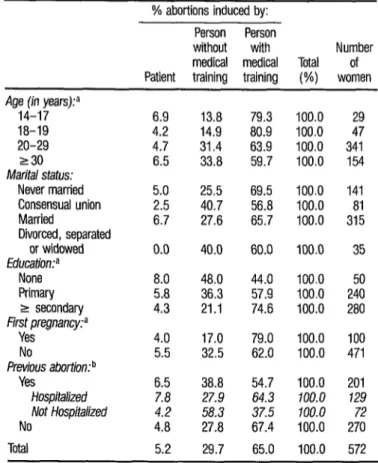
Table 3 provides information about the abortion practitioners used by
TABLE 3. Abortion practitioners cited by 572 of the study women with induced abortions-by age group, marital status, education, pregnancy history, and abor- tion history of the study women.
% abortions induced by: Person Person
without with Number medical medical Total of Patient training training (%) women Age (in years)?
14-17 18-19 20-29 230
Marital status:
Never married Consensual union Married
Divorced, separated or widowed
EducdW
None Primary 2 secondary
First pregnancy? Yes
No
Previous abortion: b Yes
Hospitalized Not Hospitalized No
Total
6.9 13.8 4.2 14.9 4.7 31.4 6.5 33.8 5.0 25.5 2.5 40.7 6.7 27.6
0.0 40.0 8.0 48.0 5.8 36.3 4.3 21.1 4.0 17.0 5.5 32.5 6.5 38.8 7.8 27.9 4.2 58.3 4.8 27.8 5.2 29.7
the patients classified as having induced abortions. In all, 420 (42 % ) of these pa- tients either declined to give information concerning the practitioner or did not ac- knowledge to attending medical person- nel that they had had an induced abor- tion. All of these 420 were excluded from Table 3.
Of the remaining 572, 65% reported that their abortion had been initiated by a person with some medical uaining; only 5 % had self-induced abor- tions. Women under 20 were the most likely to seek medically trained person- nel; and the higher the woman’s educa- tion, the more likely she was to have the abortion induced by a person with medi- cal training. Also, 79% of the women who were pregnant for the first time chose someone with medical training, as compared to only 62 % of the parous women. In addition, 67 % of the parous women with no history of abortion chose a person with medical training, as com-
pared to 55 % of those who reported a previous abortion. Regarding these latter women with previous abortions, 64 % of those who were previously hospitalized appeared to have chosen an abortion practitioner with medical training, as compared to only 38 % of the women with prior abortions who were not hospi- talized.
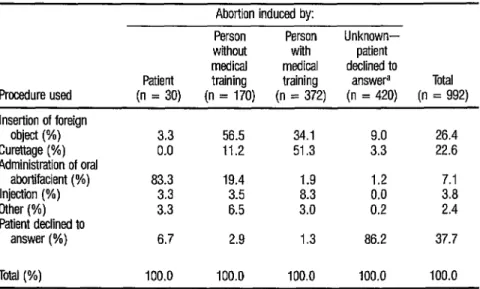
Able 4 provides information about procedures used to initiate rhe in- duced abortions. The method most com-
monly cited was insertion of a foreign ob- ject into the vagina (26%), followed by curettage (23%) and administration of an oral abortifacient (7%). However, many of the patients (38%) declined to specify the method used.
The method of induction var- ied considerably with the type of practi-
TABLE 4. Procedures used to induce abortion in the 992 study women classified as having induced abtins-by the type of abortion practitfoner involved.
Abortion induced by:
Procedure used
Person Person Unknown- without with patient medical medical declined to
Patient training training answera Total (n = 30) (n = 170) (n = 372) (n = 420) (n = 992) Insertion of foreign
object (%) Curettage (%) Administration of oral
abortifacient (%) Injection ( W) Other (%) Patient declined to
answer (%)
3.3 56.5 34.1 9.0 26.4 0.0 11.2 51.3 3.3 22.6 83.3 19.4 1.9 1.2 7.1
3.3
3.3 2 38:: 0.0 0.2 3.8 2.4 6.7 2.9 1.3 86.2 37.7 Total (%) 100.0 100.0 100.0 100.0 100.0
tioner. Among practitioners with some medical background, more than half used curettage, while another third used insertion of a foreign object. Only 11%
of the practitioners without medical training used curettage; over half used insertion of a foreign object. When a woman initiated her own abortion she most frequently took an oral aborti- facient .
Table 5 shows how complica- tions and the number of days hospital- ized varied with the method of induc- tion. More than half of the 992 abortions
classified as induced involved at least one diagnosable complication, and more than a quarter had three or four.
Insertion of a foreign object was associated with a greater number of complications than curettage. Overall, 37 % of the women whose abortions were induced by insertion of a foreign object had three or more complications as com- pared with 28% of those induced by cu-
TABLE 5. Numbers of complications, types of complications, and days of hospitalization experienced by patients whose abortions were induced, by induction method.
Method used to induce abortion:
Unknown- Insertion patient of foreign Oral declined to
object Curettage abortifacient Injection Other specify Total (n = 262) (n = 224) (n = 70) (n = 38) (n = 24) (n = 374) (n = 992)
% of patients with indicated number of complications (%):
0
1
.-I
3’
4 Total
% of patients with indicated compkations at admission (%): co
3 Y Fever Infection
-; Bleedinga CL Lesions 2 % of patients with .g indicated number d of days hospitalized:
3 0 1
$ :
a,
r40.4 2.2 0.0 0.0 16.7 2.1 35.9 50.9 91.4 89.5 50.0 5:.; 53.6 26.3 18.3 4.3 2.6 20.8 11:5 16.3 23.3 17.9 4.3 7.9 8.3 24.6 20.3 14.1 10.7 0.0 0.0 4.2 3.7 7.7 100.0 100.0 100.0 100.0 100.0 100.0 100.0
37.0 25.9 7.1 7.9 12.5 29.0 27.7 40.5 42.9 4.3 10.5 12.5 31.3 33.2 98.5 93.3 100.0 100.0 79.2 96.8 96.4 38.9 22.9 1.4 0.0 29.2 13.2 21.2
3.8 1.8 0.0 0.0 0.0 1.1 1.8 27.1 30.8 35.7 18.4 25.0 35.0 31.2 26.0 23.2 41.4 36.8 37.5 31.8 29.3 26.3 21.4 18.6 36.8 25.0 18.2 22.0 16.8 22.8 4.3 7.9 12.5 13.9 15.7 100.0 100.0 100.0 100.0 100.0 100.0 100.0
rettage. This difference is statistically sig- nificant (p < 0.01). To be more specific, significantly more patients had fever, bleeding, or lesions if a solid object was inserted into the uterus than if curettage was employed; however, no significant difference was observed between the two groups with regard to infection.
Because insertion of a foreign object was associated with a greater num- ber of complications and higher propor- tions of most symptoms, one would have expected longer hospital stays for these women. However, hospitalization was not consistently longer for the women whose abortions were induced with solid objects.
Women whose abortions were initiated by oral abortifacients or injec- tions generally had only one complica- tion, and this was usually bleeding. Not surprisingly, these women were the least likely to stay four or more nights.
Previous Contraceptive Practices
and Reproductive Plans
As Table 6 shows, the rate of contraceptive use among the study popu- lation during the month before concep- tion was low. Twenty-three percent of all the women hospitalized for treatment following abortion reported using some method, but only 7% were using mod- ern clinical methods (oral or injectable contraceptives, IUDs, or barrier meth-
ods), while 13 % were using the rhythm method.
The rate of contraceptive practice was higher among those with in- duced abortions than among those with spontaneous abortions (40% versus 19 % were using some form of contraception). Regarding use of modern clinical meth- ods, 17% of those with induced abor- tions had been using such methods, as compared to 4 % of those with spontane- ous abortions. In general, the rates of
both contraceptive and modern method use for the women with induced abor- tions were similar to the rates found for urban Bolivia by the 1983 contraceptive prevalence survey-which found 39% of the women surveyed to be using contra- ceptive methods and 17% to be using modern clinical methods.
All study women not using contraception during the month before conception were asked why they had not been using a method. The reasons they gave, which are listed in Table 7, may be classified into the following four catego- ries: (1) reasons related to desire for preg- nancy, (2) failure to recognize a need, (3) lack of knowledge and/or accessibility of methods, and (4) personal reasons. Re- gardless of the type of abortion subse- quently involved, the highest percentage of study women cited reasons related to knowledge or accessibility of methods. The percentage lacking knowledge might actually be higher than that shown, since women who cited other rea- sons may also have lacked knowledge. For women with spontaneous abortions, the second most important reason was that they desired the pregnancy. As might be expected, only 2% of the women with induced abortions gave this reason. However, many (27 % ) of the
women with induced abortions said they did not recognize a need for contracep- tion, either because they did not think it was necessary or because of infrequent sexual activity.
Table 7 does not convey a complete picture regarding women who did not want their pregnancies. Of the women with spontaneous abortions, 37% said they did not want the preg-
TABLE 6. Percentages of women practicing contraception among the 4,371 study subjects (classified by type of abortion) during the month of conception and among 2,166 contraceptive prevalence survey
(CPS) subjects, showing the types of contraceptive methods used.
Contraceptive practice during month of conception
% of patients with % of urban % of abortions classified as: women surveyed
total Spontaneous Induced by 1983 CPSa (n = 4,371) (n = 3,379) (n = 992) (n = 2,166) Used a method:
Periodic abstinence Sferiization IUD.9
Hormonalsb
Barrier methods, spermicides Withdrawal, lactation, other
Didn’t use a method
23.4 73.1 3.2
7.6 1.9 3.6 76.6
Total 100.0
18.6
12.8 -
1.2 1.2 1.2 2.7
81.4 100.0
39.8 38.6 14.2 19.5 - 4.4 10.3 6.3 2.7 5.4 4.2 1.3 8.3 1.7 60.2 61.4 100.0 100.0 a Unpublished preliminary results for currently or previously married women 15-49 years of age.
b Oral contracepttves. injectables.
TABLE 7. Reasons given for not using contraception by the 3,347 study women who were not using contraception during the month before conception-by type of abortion.
Reasons given
% of patients with % of abortions classified as: total Spontaneous Induced (n = 3,347) (n = 2,750) (n = 597) Pregnancy desired
Recognition of need:
Didn’t think use necessary Little sexual activity
Knowledge/accessibility:
Didn’t know about contraception Methods not available/tw wstly
Personal reasons:
Fear of side-effects Objections of partner; famih
or religion
Other
29.1 34.9 2.3
14.2 11.4 26.8
9.5 7.8 17.4 4.7 3.6 9.4 42.7 41 .I 49.9 41.1 39.6 47.7 7.6 1.5 2.2
11.7 10.6 16.9 7.9 7.5 9.9
3.8 3.1 7.0
1.8 1.4 3.4
cc
2 Unknown 0.5 0.5 0.7.j$ Total 100.0 100.0 100.0 9)
a 23 2 3 R
nancy, and 20% were uncertain whether they wanted it or not. In contrast, 90 % of those with induced abortions said they did not want the pregnancy, and only 7% were uncertain. Overall, half of the total study population not using contra- ception said the pregnancy was not de- sired, while 17 % were uncertain.
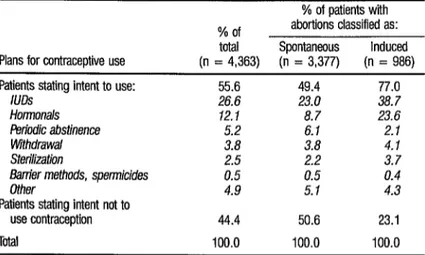
Regarding the stated intent of study subjects to use or not use contra- ception following their abortions, the percentage saying they intended to use a method in the future was higher than the percentage saying they had used a method during the month before con- ception (T&ble 8). Nearly half the women hospitalized for complications associated with spontaneous abortions said they in- tended to use a method, and 34 % said they intended to use a modern clinical method. More emphatically, over three- fourths of the women hospitalized for complications of induced abortion said
they intended to use some contraceptive method, and 66% said they intended to use a modern clinical method.8 While the percentage of women intending to use modern clinical methods was much higher than the percentage reporting use of those methods before pregnancy, the percentage intending to use traditional methods (particularly the rhythm method) was considerably lower than the percentage reporting use of those meth- ods before pregnancy. This was especially true for the group of patients with in- duced abortions.
Women who said they did not intend to use any contraceptive method after their abortion were asked why not. As Table 9 indicates, the reason given most frequently by women with sponta- neous abortions was that they wanted to get pregnant again. (The next most fre- quent reason among this group was lack
8 Defined as use of hormonals, IUDs, condoms, spermi- tides, or sterilization. The category “other” was com- prised largely of women who wished to consult further with a physician before deciding which method to use.
TABLE 8. Statad intentions of 4,363 study subjjcts to use or not use contraceptfve methods following aborlfon, by type of abortion. Information was missing for eight of the 4,371 study subjacts.
Plans for contraceptive use Patients stating intent to use:
/LIDS HOrmonalS
Periodic abstinence Withdrawal Steriiization
f?anier methods, spermicides Other
Patients stating intent not to use contraception Total
% of patients with % of abortions classified as: total Spontaneous Induced (n = 4,363) (n = 3,377) (n = 986) 55.6 49.4 77.0 26.6 23.0 38.7 12.1 8.7 23.6 5.2 6.1 2.7 3.8 3.8 4.1 2.5 2.2 3.7 0.5 0.5 0.4
TABLE 9. Reasons given for intending not to use contraception by the 1,939 study subjects who said atter their abortions that they intended to use no contraception in the future.
% of patients with Reasons given for intending % of abortioos classified as: not to use contraception - total Spontaneous Induced in the future (n = 1,939) (n = 1,711) (n = 228) Pregnancy desired
Intends to discontinue sexual relations
No knowledge of contraception Personal reasons
Fear of side-effects Objections of partnec fan@
or re/igion
Unknown Total
52.4 57.9 11.4 9.1 6.0 32.5 28.2 27.6 32.9 6.7 7.1 21.5 4.7 4.6 5.7 4.0 2.5 75.8 1.1 1.1 1.3 0.4 0.4 0.4 100.0 100.0 100.0
of knowledge.) For women with induced abortions, the two most commonly cited reasons were lack of knowledge about contraception and intent to discontinue sexual relations. However, 21.5 % cited personal reasons, especially objections of their partner, family, or religion to con- traceptive use.
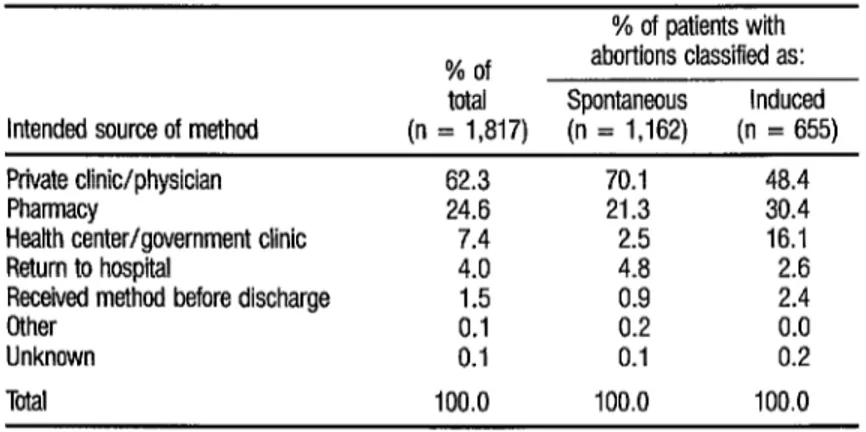
Those who said they intended to use a modern clinical method were asked where they intended to obtain their contraception. As indicated by the figures in Table 10, nearly 80% of the women in the induced group and over
90% of those in the spontaneous group 3
2 said they would obtain their contracep- tion in the private sector. i
2 (\1 -4 -8 u a a 2
38
D
ISCUSSION
The foregoing results cannot be applied generally to all Bolivian women experiencing abortions, since the study sample included only those women who sought medical attention and were admitted to certain hospitals. Women who suffered only minor complications or none at all would have been less likely to seek hospital care. In addition, some women, especially in rural areas, had limited access to hospitals. Nevertheless, because of the difficulties involved in ob- taining data on abortions outside of hos- pital settings, the data obtained provide important information about abortion despite their limitations,
Clearly, the physical and psy- chological costs of abortion to some women and their families were very high. Seven women died; and 20, some of whom were young and unmarried, had hysterectomies.
TABLE 10. Intended sources of modern conbxqtive methods, as reported by study women who said after their abortions that they planned to use such methods:
% of patients with % of abortions classified as: total Spontaneous Induced Intended source of method (n = 1,817) (n = 1,162) (n = 655) Private clinic/physician 62.3 70.1 48.4 Pharmacy 24.6 21.3 30.4 Health center/government clinic 7.4 2.5 16.1 Return to hospital 4.0 4.8 2.6 Received method before discharge 1.5 0.9 2.4 Other 0.1 0.2
Unknown 0.1 0.1 i:; Total 100.0 100.0 100.0 a Defined as homonals, IUDs. condoms, spmicides, or sterilization.
hospital beds, and 25% stayed three nights or more. Virtually all received cu- rettage while under general anesthesia, even though vacuum aspiration is the preferred procedure for treating an in- complete abortion (7). Since vacuum as- piration tends to produce less trauma than curettage and can be used on an outpatient basis, it appears that hospital costs could be reduced by substituting vacuum aspiration for curettage. Also, many of the abortions studied could have been avoided if counseling, sex ed- ucation, and family planning services had been available.
Overall, a considerable pro- portion of the women studied said they had not wanted their pregnancies. As was to have been expected, higher pro- portions of women with induced (as compared to spontaneous) abortions said their pregnancies were not wanted and had been using conuaceptives during the month before conception. It thus ap- pears that among the women with in- duced abortions, in many cases the con- traceptive methods used were not effective or were not being used correctly. Also, it appears that the level of contra- ceptive use was too low to limit pregnan-
cies to those desired. Indeed, even among the women with abortions classi- fied as spontaneous, the level of contra- ceptive use was low. That is, over half said they had not wanted the pregnancy or had not been sure they wanted it. By these criteria, the women in both groups (with induced and spontaneous abor- tions) who reported that their pregnan- cies had been unwanted (as well as some of these who reported not being certain) were in need of effective contraceptive methods.
The paucity of sex education provided in the schools and at home is g reflected in the large percentage of study g women who cited lack of knowledge as a reason for not using contraception dur- 5 ing the month before conception. This 5 information problem was also found R among the women who said they were 3 not planning to practice contraception 2 . G P
s z.
after discharge, nearly a third of whom said they lacked knowledge of contra- ception.
The extent to which patients hospitalized with complications from abortions are counseled on family plan- ning probably varies with the institution, the clinical staff attending them, and the patients themselves. However, it appears that postabortion counseling, as well as prior sex education, would offer an im- portant way of helping these women help themselves.
Although a high percentage of the study women said they intended to use some contraceptive method after discharge, the actual level of contracep- tive use will probably be lower. One rea- son for this could be a lack of available services, especially since no family plan- ning services are provided by the public sector. In this vein, there would appear good reason for health care providers and program planners to respond to the high demand for modern clinical methods. More than half of the study patients in- tending to use a method said they wanted to use an oral contraceptive or IUD. Since the insertion of an IUD re- quires medical training, if there were no legal hindrances hospital personnel could offer interested women insertion before discharge. Studies have shown that postabortal IUD insertion does not significantly increase the rate of subse- quent complications (8).
Also, sterilization is one of the most popular contraceptive methods in much of Latin America. However, even when female sterilization is well- known, obstacles often exist within the delivery system (9). In this study, more than 1,800 women said they wanted no more children. Although there is no spe- cific legislation in Bolivia that mentions sterilization, any medical procedure that affects the normal functioning of the re- productive organs is prohibited. Perhaps
as a result, the prevalence of sterilization is much lower in Bolivia than in other Latin American countries. Physicians may be reluctant to recommend and per- form sterilization, and women may not perceive it as an option.
In countries where highly qualified personnel and financial re- sources are limited, it has been found that family planning services are a cost- effective component of integrated mater- nal health care (10). This finding is sup- ported in a negative sense by the study reported here, which identified a group of Bolivian women whose needs were not being met-needs that were expressed by the risks and costs entailed in the ter- mination of unwanted pregnancy.
S
UMMARY
The extent to which deliber- ate pregnancy wastage (induced abor- tion) is practiced in Latin America is dif- ficult to determine because of its illegal status. Until now, no estimates have been available for Bolivia. However, over a twelve-month period, beginning in July 1983, data were collected at 11 hos-
pitals in five Bolivian cities on 4,37 1
Of the illegally induced cases, 65 % were induced by medically trained practitioners, most of whom employed curettage; the other 35%, induced by people without medical training or by the women themselves, were initiated most commonly by inserting a foreign object in the vagina. In general, the more educated women were more apt to seek out medically trained practitioners. Also, women whose abortions were in- duced by curettage were less likely to ex- perience fever and lesions but had longer average hospital stays.
Sixty-two percent of the women studied said they had not been using contraception during the month before conception; 48 % of these nonus- ers cited lack of knowledge as their rea- son for nonuse. After medical treatment, 77 % said they planned to use contracep- tion, the IUD being the most commonly cited method.
Seven of the hospitalized women studied lost their lives and 20 re- ceived total hysterectomies as a result of abortion-related complications. Of the latter, I5 were less than 30 years old and five had no living children. In addition, substantial scarce medical resources were needed to treat abortion-related prob- lems, as suggested by the fact that over a third of the women with induced abor- tions were hospitalized for three or more days. Overall, the results of this study in- dicate a clear need to improve the deliv- ery of family planning services in Bolivia.
Ft.E
FERENCES
1 Tietze, C. Induced Abortion, A Wodd Re- view, 198.3 ct;Fh ed.). The Population Coun- cil, New York, 1983.
2 Population Reports. Heahh: The Famdy Plan ning Factos Series J, No. 14. Baltimore, 1977. 3 Murillo, A. de la G., and J. de1 Castillo. Mor- talidad matema. Rev&a de l’a Sociedad de GinecoLogiia y Obstetricia (1): 1, 1983. 4
5
6
7
8
9
10
Population Division of the United Nations Department of International Economic and Social Affairs and the United Nations Fund for Population Activities. Popdation Policy Com- pendium (Bohti). New York, 1979. Consultora Boliviana de ReproducciBn Hu- mana. Encuesta de Prevalencia de Medicamen- tos: Informe Preliminar. La Paz, 1984. Szabady, E., A. Klinger, and G. Acsadi. The Hungarian Fertility and Family Planning Study of 1965-66: Preventive Medicine and Family Plannin
1
. In: International Planned Parenthood Fe eration. Proceedings of the
Fifth Conference of the Europe and Near East ~.q&on. of the ZPPF in Copenhagen. London, Kleimnan, R. L. (ed.). Abortion: C~asszj%a- tion and Techniques. IPPF Central Medical Committee, London, 1974.
Goldsmith, A., R. Goldberg, H. Eytaguirre, S. Lucero, and L. Lizana. IUD Insertion in the Immediate Postabortal Period. In: Goldsmith, A., and R. Snowden (eds.). Famdy Planning Research Conference: A Mdtidiscibhnarv Ab- proacb. Excerpta Medica, Amst&dam: The Netherlands, 1972, pp. 59-67.
Janowitz, B., J. Nufiez, D. L. Covington, and C. Colven. Wh women don’t get sterilized: A follow-up o Y women in Honduras. St& Fam PIann 16(2), 1985.