Evaluation of the birth
certii cates as source of
information on birth defects
Avaliação das declarações
de nascido vivo como fonte
de informação sobre defeitos
congênitos
Ana Lívia GEREMIAS
1Marcia Furquim de ALMEIDA
1Luiz Patricio Ortiz FLORES
21Faculdade de Saúde Pública da Universidade de São Paulo
2Fundação SEADE – Sistema Estadual de Análises de Dados
FAPESP nº 2006/61304-3
Endereço para correspondência: Faculdade de Saúde Pública da Universidade de São Paulo, De-partamento de Epidemiologia. Avenida Dr. Arnaldo, 715 - 01246-904 - São Paulo, SP - Brazil. Tel.: (011) 3061-7724/ 3061-7744
Abstract
Objective: To obtain the prevalence of birth defects in a live birth cohort, linking the live birth information system (SINASC) and the mortality information system (SIM) databa-ses. Methods: Descriptive study to assess linked databases of hospital live births (LB) and neonatal deaths of resident mothers that occurred in the city of São Paulo, be-tween January 1st, 2006 and June 30th, 2006. Results: According to the SINASC, the most prevalent birth defects (BD) were: BD and musculoskeletal system deformity (44.7%), nervous system BD (10.0%) and chromoso-mal anochromoso-malies (8.6%). There was 80.0% of recovery of circulatory system BD, 73.3% of respiratory system BD and 62.5% of digesti-ve system BD in the linked database. Linked data set identifi ed BD in 640 live births; the SINASC accounted for 55.2% of notifi cations and the SIM for 44.8%. The prevalence rate of BD based on SINASC data was 75.4%00 LB. This rate showed an increase of 14.3% when obtained from the linked dataset (86.2%00 LB). Conclusion: Linkage of the live birth (SINASC) and mortality systems (SIM) provides a more real BD profi le. BDs notifi ed by the SINASC were more visible at birth, while the SIM notifi ed more fatal BD, showing the importance of utilizing both data sources.
Resumo
Objetivo: Estimar a prevalência de defeitos congênitos (DC) em uma coorte de nasci-dos vivos (NV) vinculando-se os bancos de dados do Sistema de Informação de Mor-talidade (SIM) e do Sistema de Informação sobre Nascidos Vivos (SINASC). Métodos: Estudo descritivopara avaliar as declarações de nascido vivo como fonte de informação sobre DC. A população de estudo é uma coorte de NV hospitalares do 1º semestre de 2006 de mães residentes e ocorridos no Município de São Paulo no período de 01/01/2006 a 30/06/2006, obtida por meio da vinculação dos bancos de dados das declarações de nascido vivo e óbitos neo-natais provenientes da coorte. Resultados: Os DC mais prevalentes segundo o SINASC foram: malformações congênitas (MC) e deformidades do aparelho osteomuscular (44,7%), MC do sistema nervoso (10,0%) e anomalias cromossômicas (8,6%). Após a vinculação, houve uma recuperação de 80,0% de indivíduos portadores de DC do aparelho circulatório, 73,3% de DC do apa-relho respiratório e 62,5% de DC do apaapa-relho digestivo. O SINASC fez 55,2% das notifi ca-ções de DC e o SIM notifi cou 44,8%, mos-trando-se importante para a recuperação de informações de DC. Segundo o SINASC, a taxa de prevalência de DC na coorte foi de 75,4%00 NV; com os dados vinculados com o SIM, essa taxa passou para 86,2%00 NV.
Conclusões: A complementação de dados obtida pela vinculação SIM/SINASC fornece um perfi l mais real da prevalência de DC do que aquele registrado pelo SINASC, que identifi ca os DC mais visíveis, enquanto o SIM identifi ca os mais letais, mostrando a importância do uso conjunto das duas fontes de dados.
Palavras-chave: Defeitos congênitos.
Linkage. Declaração de Nascido Vivo. De-claração de Óbito. Sistema de informação. Prevalência.
INTRODUCTION
Birth defects (BD) include all structural defects present at birth, which can be clas-sifi ed as primary defects, secondary defects and malformations.1 BDs can be defi ned
as functional or structural anomalies in fetus development, resulting from a factor originated before birth, whether genetic, environmental or unknown, present at birth or possibly manifesting itself years later, as certain chronic degenerative diseases. They can manifest as isolated forms (when the newborn (NB) shows only one defect, in-volving isolated body systems) or associated (when multiple defects coexist, involving many organs).2, 3
Causes associated with BD are still un-certain. It is estimated that between 15% and 25% are due to genetic alterations, between 8% and 12% due to environmental factors, and between 20% and 25% due to both. However, the majority (between 40% and 60%) have an unknown origin.2, 3, 4, 5, 6
Birth defects are an important cause of child mortality in several countries, morbi-dity in childhood and long-term incapaci-tation in developed countries. In addition, they signifi cantly contribute to embryonic and fetal death, they are among the causes that lead to loss of potential years of life, and they are also responsible for three quarters of the population’s physical handicaps.7,8,9
As the child mortality rate from infec-tious, parasitic and respiratory diseases decreased, there was an increase in BD’s relative participation in child deaths. This is because, as other causes of death are con-trolled, BDs begin to play a proportionately more important role. However, progress in health care and basic sanitation has led to a reduction in infectious and malnourish-ment diseases, and, for this reason, BDs now have a greater infl uence on perinatal mortality.2, 5, 10, 11,12
child mortality in this country. Among these BDs, cardiovascular and nervous system de-fects stand out, only falling below perinatal diseases.7, 8,19
BDs are the main cause of death in the fi rst year of life and the fi fth cause of loss of potential years of life in the United States.7
The proportion of deaths due to BD showed an increase from 14% to 22% between 1968 and 1995.8
Brazil does not have a specifi c informa-tion system on populainforma-tion-based BDs to monitor their prevalence. Until the 1990’s, the only information available on BD fre-quency and distribution in the population came from mortality information system. The introduction of the variable “presence of birth defect” in the Live Birth Certifi cate (fi eld 34) occurred in 1999.8 Therefore, the
SINASC (Live Birth Information System) can be an important instrument to monitor the BD population and, for this reason, “efforts must be made to guarantee better informa-tion gathering”.14
Database linkage technique, by enabling the identifi cation of the same individual in two or more databases, allows for the re-trieval of information and, as a result, for an estimate closer to the real BD prevalence in live births to be obtained. The information available in SINASC will be complemented with SIM (Mortality Information System) information, by employing this technique. The most visible BDs are probably recorded in the Live Birth Certifi cate (BC), whereas in the Death Certifi cate (DC) are the most severe BDs. In this study, both the BDs recorded as underlying cause and those recorded as associated cause of death were considered.
METHODOLOGY
A descriptive study was performed in the city of São Paulo, between January 1st
2006 and June 30th, 2006. The study
popu-lation was a hospital live birth cohort from mothers who live in the city of São Paulo, and the neonatal deaths were originated from this cohort.
Linked database information on live birth (BC) and neonatal death certifi cates (DC) for the state of São Paulo was provided by the SEADE (State Data Analysis System) Foundation Vital Statistics System, corres-ponding to 316,109 live births , where 3,004 neonatal deaths occurred.
Live newborns whose mothers did not live in the city of São Paulo (N= 226,594) were excluded from this study, resulting in 89,515 resident live newborns. Of these, non-hospital births (N= 589) and births of residents that did not occur in the city of São Paulo (N= 4,080) were also excluded, resulting in a cohort of 84,846 live birth certifi cates. . The database provided was linked through the deterministic method and came from the research study “Assess-ment of quality of information on perinatal mortality in the city of São Paulo”.
The variable recorded in Field 34 of the live birth certifi cate – “birth defect and/or chromosomal anomaly detected: yes and no” was used. The SEADE Foundation codi-fi es the birth defects recorded in the BCs and the causes of death in the DCs in accordance with the ICD-10 (International Classifi cation of Diseases, 10th revision). BCs and DCs that
showed Q00 to Q99 codes, corresponding to birth defects, were selected.
For the cohort survivors, BCs were the only source of information. For the cohort neonatal deaths, the following were used: a) BC (presence of BD in fi eld 34) and b) DC – underlying causes and associated causes of death that were coded as BD.
The fi rst stage was to assess how fi eld 34 in the BC was fi lled in. The proportion of BCs with no record of BD was obtained. BD prevalence rates were calculated for neonatal deaths and survivors, according to information recorded in the SINASC.
The database was made available on Microsoft’s® Windows Access and the analy-ses were performed using the Epi-Info® 2000 statistical package, version 3.4.1, from July 2007, and the Open Source Epidemiolo-gic Statistics for Public Health, version 2.2.1 (http://www.openepi.com).
196 from October 10th, 1996 (National
He-alth Council – Human Research Regulating Norms and Directives), this project was approved by the COEP (Research and Ethics Committee) of the São Paulo University School of Public Health.
RESULTS
A total of 73,944 (87.2%) live births, from the cohort of the 1st semester of 2006 for the
city of São Paulo, had fi eld 34 of the BC fi lled in (yes and no), while 10,902 (12.8%) ignored this fi eld or left it blank (not fi lled in).
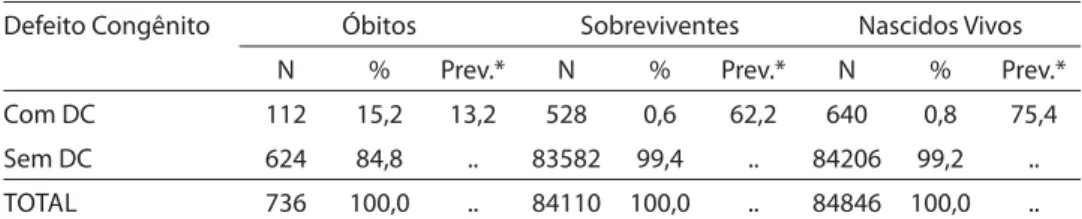
A total of 640 LBs (0.8%) had a BD re-corded in the BC, according to the SINASC. Of these, 112 (15.2%) died and 528 (0.6%) survived. The BD prevalence rate in the cohort was 75.4/10,000 LBs. The prevalence rates among survivors and neonatal deaths were 62.2/10,000 and 13.2/10,000 LBs, res-pectively (Table 1).
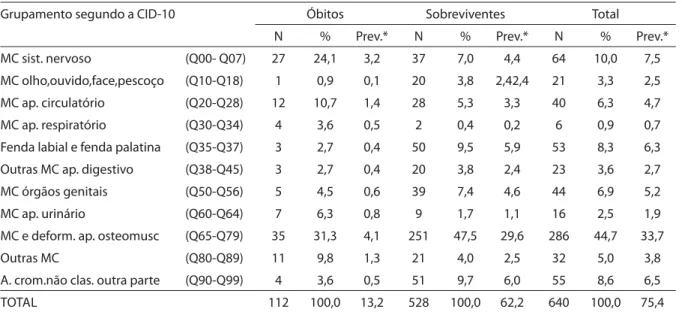
Of all the BDs recorded in BCs, the most prevalent were the following: BD and mus-culoskeletal system defects (44.7%), as well as in deaths and survivors, followed by ner-vous system BDs (10.0% as in neonatal deaths) and chromosomal anomalies not classifi ed elsewhere (8.6%) (Table 2). The most prevalent BDs among neonatal deaths were as follows: BD and musculoskeletal system defects (31.3%), followed by nervous system BDs (24.1%) and circulatory system BDs (10.7%). Among survivors, the most prevalent BDs were also BD and muscu-loskeletal system defects (47.5%), followed by chromosomal anomalies not classifi ed
elsewhere (9.7%) and cleft lip and cleft pa-late (9.5%). Of all the 640 BD records in the
SINASC, only one newborn showed three BDs: Q391 Q435 Q530; the codes Q391 and Q435 belong to the “other digestive system birth defects” group, while Q530 belongs to the “reproductive system BDs”, according to the ICD-10.
Of all the 736 cohort neonatal deaths had 183 BDs recorded in the SIM, representing 24.9% of all deaths, and it represented the second most important cause of death in the cohort studied. Of all the 183 BD deaths recorded in the cohort, 144 (78.7%) were the underlying cause of death and 39 (21.3%) were an associated cause of death. Among the 144 BDs recorded as the underlying cause of death, there was a higher frequency of deaths with BDs classifi ed as: circulatory system BDs (32.6%), respiratory system BDs (18.8%), nervous system BDs (15.3%) and BD and musculoskeletal system defects (8.3%). The order of causes of death from BDs, recorded as associated causes, was different from those observed in the group of BDs as underlying cause. Among the 39 records of death from BDs as associated cause of de-ath, the most frequent were the following: nervous system BD (30.8%), circulatory system BD (25.6%) and respiratory system BD and other BDs (18% each). Of all the BDs recorded as associated causes of death, eight showed two types of BDs and one newborn showed three types of BD. All newborns with recorded BD as associated cause of death also had a record of BD as the underlying cause of death (39 NBs).
Table 1 – Number of neonatal deaths, survivors and live births with birth defects, according to
SINASC data. City of São Paulo, 1st semester of 2006.
Defeito Congênito Óbitos Sobreviventes Nascidos Vivos
N % Prev.* N % Prev.* N % Prev.*
Com DC 112 15,2 13,2 528 0,6 62,2 640 0,8 75,4
Sem DC 624 84,8 .. 83582 99,4 .. 84206 99,2 ..
TOTAL 736 100,0 .. 84110 100,0 .. 84846 100,0 ..
Source: Fundação SEADE – Sistema Estadual de Análises de Dados (SEADE Foundation – State Data
Analysis System).
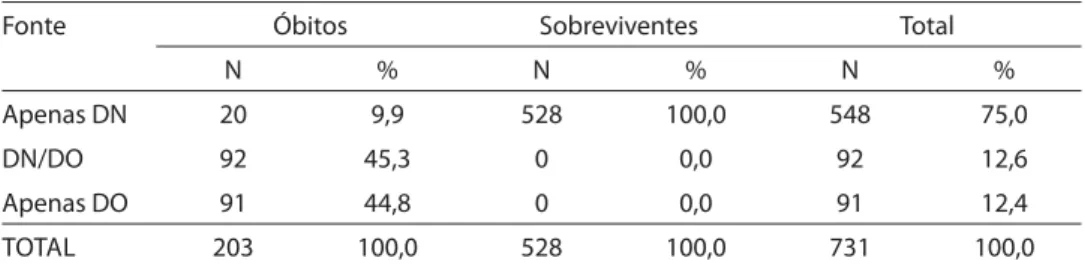
The use of SIM and SINASC data enabled the identifi cation of a total of 731 newborns with BDs, of which 548 (75%) were only re-corded in the BC, 92 (12.6%) in the BC and DC, and 91 (12.4%) in the DC exclusively. As regards all the newborns with BDs in the cohort, which were 640 initially, 91 NBs were added with this procedure, and there were 731 newborns with BDs. The correction obtained by using the linkage technique was 14.3% (91/640) (Table 3).
A total of 55.2% of BD notifi cations were recorded by the SINASC, while 44.8% were recorded by the SIM, i.e. the SIM was found to be a very important information system to retrieve BD data in the cohort.
According to the SINASC, the BD preva-lence rate of the hospital live birth cohort in the 1st semester of 2006, in the city of São
Paulo, was 75.4/10,000 LBs. The prevalence rate, with data corrected by the SIM, was 86.2/10,000 LBs, that is, data retrieval with
SIM increased BD prevalence in the cohort by 14.3% (Table 4).
Of all the 92 deaths with information on BDs in the BC and DC, 41 belonged to the same group, according to the ICD-10, and 51 belonged to different groups, as shown
on Table 5. The following BDs, belonging to the same group, according to the ICD-10, were recorded in the two most prevalent sources of information: nervous system BDs (46.3%), circulatory system and mus-culoskeletal system BDs (17.1% each), and other BDs (7.3%).
Of all the BDs belonging to distinct groups, there was a higher frequency of newborns with BDs and musculoskeletal system defects in the SINASC (N=18). Among these newborns, 8 (44.4%) had respiratory system BDs, 5 (27.8%) had other BDs and 3 (16.7%) had other digestive system BDs recorded in the SIM. A total of seven NBs with urinary system BD in the
SINASC had respiratory system BDs in the death certifi cate (SIM).
Of all the seven NBs with records of nervous system BDs at birth, 4 (57.0%) had other BDs, 2 (28.6%) had urinary system BDs and 1 (14.3%) had BD and musculoskeletal system defects in the SIM.
These data show a newborn who had one type of BD at birth, but died from ano-ther type of BD. Thus, it is more diffi cult to identify multiple BDs with information from
SINASC. However, when this is linked to SIM
Table 2 – Number, percentage and prevalence rate* of birth defects recorded in the SINASC for deaths, survivors and live
births of the cohort. City of São Paulo, 1st semester of 2006.
Grupamento segundo a CID-10 Óbitos Sobreviventes Total
N % Prev.* N % Prev.* N % Prev.*
MC sist. nervoso (Q00- Q07) 27 24,1 3,2 37 7,0 4,4 64 10,0 7,5
MC olho,ouvido,face,pescoço (Q10-Q18) 1 0,9 0,1 20 3,8 2,42,4 21 3,3 2,5
MC ap. circulatório (Q20-Q28) 12 10,7 1,4 28 5,3 3,3 40 6,3 4,7
MC ap. respiratório (Q30-Q34) 4 3,6 0,5 2 0,4 0,2 6 0,9 0,7
Fenda labial e fenda palatina (Q35-Q37) 3 2,7 0,4 50 9,5 5,9 53 8,3 6,3
Outras MC ap. digestivo (Q38-Q45) 3 2,7 0,4 20 3,8 2,4 23 3,6 2,7
MC órgãos genitais (Q50-Q56) 5 4,5 0,6 39 7,4 4,6 44 6,9 5,2
MC ap. urinário (Q60-Q64) 7 6,3 0,8 9 1,7 1,1 16 2,5 1,9
MC e deform. ap. osteomusc (Q65-Q79) 35 31,3 4,1 251 47,5 29,6 286 44,7 33,7
Outras MC (Q80-Q89) 11 9,8 1,3 21 4,0 2,5 32 5,0 3,8
A. crom.não clas. outra parte (Q90-Q99) 4 3,6 0,5 51 9,7 6,0 55 8,6 6,5
TOTAL 112 100,0 13,2 528 100,0 62,2 640 100,0 75,4
Source: Fundação SEADE – Sistema Estadual de Análises de Dados (SEADE Foundation – State Data Analysis System).
data, it is possible to identify individuals with multiple BDs.
Using SIM data, the BDs found to be more important were the respiratory sys-tem BDs (N=20); other BDs came in second (N=11); circulatory system BDs came in third (N=5); followed by BDs and musculoskeletal system defects (N=4); urinary system BDs (N=4) and chromosomal anomalies not classifi ed elsewhere (N=2).
The most prevalent BDs recorded in the SINASC were as follows: BDs and mus-culoskeletal system defects (85.4%) and nervous system BDs (84.4%). Cleft lip and
cleft palate (N=3, 100.0%) and reproductive system BDs (N=5, 100.0%) were recorded in the SINASC exclusively.
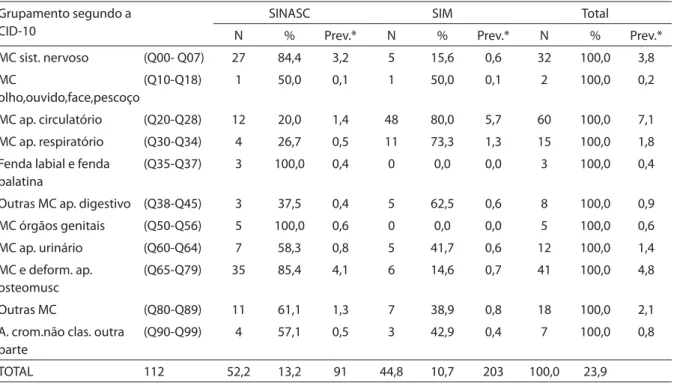
After linkage, there was an 80% retrieval of newborns with circulatory system BDs, 73.3% of those with respiratory system BDs and 62.5% with other digestive system defects.
Table 6 shows the prevalence rate, accor-ding to the ICD-10 group, for both sources of information individually and after data linkage. A change in the order of BDs in the cohort live births can be observed. According to SINASC data, BDs and
muscu-Table 3 – Number and percentage of birth defects, according to information system (SINASC and
SIM). City of São Paulo, 1st semester of 2006.
Fonte Óbitos Sobreviventes Total
N % N % N %
Apenas DN 20 9,9 528 100,0 548 75,0
DN/DO 92 45,3 0 0,0 92 12,6
Apenas DO 91 44,8 0 0,0 91 12,4
TOTAL 203 100,0 528 100,0 731 100,0
Source: Fundação SEADE – Sistema Estadual de Análises de Dados (SEADE Foundation – State Data
Analysis System).
Table 4 – Number and percentage of birth defects for neonatal deaths, survivors and total
number of live births, according to source of information. City of São Paulo, 1st semester of 2006.
Fonte Óbitos Sobreviventes Total
N % Prev.* N % Prev.* N % Prev.*
SINASC 112 15,2 13,2 528 0,6 62,2 640 0,8 75,4
SIM/SINASC 203 27,6 23,9 0 0,0 0 731 .. 86,2
Source: Fundação SEADE – Sistema Estadual de Análises de Dados (SEADE Foundation – State Data
Analysis System).
Note: *: Prevalence rate per 10,000 LBs.
Table 5 – Presence of birth defects in neonatal deaths recorded in the SINASC and SIM,
according to ICD-10 groups. City of São Paulo, 1st semester of 2006.
DC presente no SINASC e no SIM N %
Pertencentes ao mesmo grupamento 41 44,6
Pertencentes a grupamento diferente 51 55,4
TOTAL 92 100,0
Source: Fundação SEADE – Sistema Estadual de Análises de Dados (SEADE Foundation – State Data
loskeletal system defects occupied the fi rst place, nervous system BDs came in second, and circulatory system BDs came in third. After data linkage, circulatory system BDs occupied the fi rst place, with a high preva-lence rate correction (407%). Respiratory system BDs showed a 160% increase in their prevalence rate; other BDs also showed high prevalence rate correction (61.5%); even the BDs which occupied the fi rst place in the
SINASC showed a correction of about 18.8%. These data reveal the importance of the joint use of the two sources of information.
DISCUSSION
Quality of information on BDs in the
SINASC can be considered reasonable,15
as lack of recorded information was 12.8% (ignored or left blank)16, indicating that it is
possible to use SINASC data to assess BDs. In fi ve years, there was an improvement in quality of such recorded information in the
SINASC, in the city of São Paulo. A study
performed in the south area of the city of São Paulo showed that lack of information in fi eld 34 (sum of those ignored and left blank) was 30.0% in 2001.14 Then, in 2006,
lack of information was 7.9%17 in this same
location. Thus, in fi ve years, there was great data improvement. The frequency of BDs in the live birth cohort was 0.8%, according to the SINASC. Results from this study are in agreement with the predominance of musculoskeletal system defects, followed by the central nervous system, as found in the cities of Rio de Janeiro, Vitória and Vale do Paraíba Paulista, in Brazil, and in the city of Caracas, in Venezuela. These results are similar to those found in the United States and in Europe.3,13,18 The prevalence of BDs
in the city of São Paulo is comparable to that of the city of Rio de Janeiro, according to SINASC data.13
The higher frequency of recorded BDs belongs to the groups that are clinically perceptible at birth, whether because they are visible or because they show conditions
Table 6 – Number, percentage and birth defect prevalence rate*, according to ICD-10 groups and information on cohort
neonatal deaths in the SINASC and SIM. City of São Paulo, 1st semester of 2006.
Grupamento segundo a CID-10
SINASC SIM Total
N % Prev.* N % Prev.* N % Prev.*
MC sist. nervoso (Q00- Q07) 27 84,4 3,2 5 15,6 0,6 32 100,0 3,8
MC
olho,ouvido,face,pescoço
(Q10-Q18) 1 50,0 0,1 1 50,0 0,1 2 100,0 0,2
MC ap. circulatório (Q20-Q28) 12 20,0 1,4 48 80,0 5,7 60 100,0 7,1
MC ap. respiratório (Q30-Q34) 4 26,7 0,5 11 73,3 1,3 15 100,0 1,8
Fenda labial e fenda palatina
(Q35-Q37) 3 100,0 0,4 0 0,0 0,0 3 100,0 0,4
Outras MC ap. digestivo (Q38-Q45) 3 37,5 0,4 5 62,5 0,6 8 100,0 0,9
MC órgãos genitais (Q50-Q56) 5 100,0 0,6 0 0,0 0,0 5 100,0 0,6
MC ap. urinário (Q60-Q64) 7 58,3 0,8 5 41,7 0,6 12 100,0 1,4
MC e deform. ap. osteomusc
(Q65-Q79) 35 85,4 4,1 6 14,6 0,7 41 100,0 4,8
Outras MC (Q80-Q89) 11 61,1 1,3 7 38,9 0,8 18 100,0 2,1
A. crom.não clas. outra parte
(Q90-Q99) 4 57,1 0,5 3 42,9 0,4 7 100,0 0,8
TOTAL 112 52,2 13,2 91 44,8 10,7 203 100,0 23,9
Source: Fundação SEADE – Sistema Estadual de Análises de Dados (SEADE Foundation – State Data Analysis System).
incompatible with life (anencephalic new-borns: N=15). This, in its turn, indicates that the type of BD present infl uences its diagnosis and recording in the SINASC
and, as a result, will have an effect on its prevalence.
Information on BDs in the SIM focuses on indicating the underlying cause of death (78.7%), which shows there has not been a change in the pattern of mortality from BDs for a long time, similarly to what was recor-ded in the state of São Paulo, in 1989.20 In
the city of Londrina, state of Paraná, deaths from BDs occurred, in a decreasing order of importance, due to: multiple defects, heart diseases, diaphragmatic hernia, polycystic kidneys and hydrocephaly.21
It is more diffi cult to identify multiple BDs when the information is based on
SINASC data (0.1%oo LBs). However, after linkage with SIM data, those individuals with multiple BDs are more clearly identi-fi ed (1.1%oo LBs).
Results showed that more apparent BDs are more frequently recorded in the SINASC,
whereas the BDs present in the SIM are usu-ally those less visible externusu-ally and those that cause physiological problems incom-patible with life, i.e. those that lead to death. In addition, only by adding these deaths through database linkage can these BDs be obtained. This result shows the importance of using linked data from these two informa-tion systems, which provides a more realistic BD prevalence, differently from working with a single information system.
CONCLUSIONS
The SINASC can be used as data source to monitor birth defects in the city of São Paulo. Despite the improvement in data recording observed, it is still necessary to develop actions to help these be recorded in birth certifi cates. The linked SIM and SI-NASC databases are found to be an effi cient mechanism to retrieve data, providing cor-rection measures for BD prevalence in the population, identifi cation of multiple BDs and a different BD distribution pattern.
Referências
1. Dicionário digital de termos médicos 2006. Disponível em http:/www.pdamed.com.br/diciomed/pdamed. [Acessado em 26 de julho de 2006.]
2. Horovitz DDG, Llerena Junior JC, Mattos RA. Atenção aos defeitos congênitos no Brasil: panorama atual. Cad Saúde Pública 2005; 21(4): 1055-64.
3. Maciel ELN, Gonçalves EP, Alvarenga VA, Polone CT, Ramos MC. Perfi l epidemiológico das malformações congênitas no município de Vitória-ES. Cad Saúde Coletiva 2006; 14 (3): 507-18.
4. Canadian Perinatal Surveillance System. Congenital anomalies in Canada: a perinatal health report. Health Canada, Santé Canada, 2002. Disponível em http:// www.phac_aspc.gc.ca/publicat/cac_acc02/pdf/ cac2002_e.pdf. [Acessado em 13 de janeiro de 2007].
5. Patel ZM, Adhia RA. Birth defects surveillance study. Indian J Pediatr 2005, 72 (S1): 489-91.
6. Castro MLS, Cunha CJ, Moreira PB, Fernández RR, Garcias GL et al. Frequência das malformações múltiplas em recém-nascidos na cidade de Pelotas, Rio Grande do Sul, Brasil, e fatores sociodemográfi cos associados. Cad Saúde Pública 2006; 22(5): 1009-15.
7. Amorim MMR, Vilela PC, Santos ARVD, Lima ALMV, Melo EFP, Bernardes HF et al. Impacto das malformações congênitas na mortalidade perinatal e neonatal em uma maternidade-escola do Recife. Rev Bras Saúde Mater Infant 2006; 6(S1): 519-25.
8. Guerra FAR. Avaliação das informações sobre defeitos congênitos no município do Rio de Janeiro através do SINASC [tese de doutorado]. Rio de Janeiro: Ministério da Saúde, Fundação Oswaldo Cruz, Instituto Fernandes Figueira; 2006.
9. Moratilla NA, García AMG, Benavides FG. El conjunto mínimo básico de datos al alta hospitalaria como fuente de información para el estudio de las anomalías congénitas. Rev Esp Salud Publica 1999; 73 (1): 61-9.
10. Ortiz LP, Camargo ABM. Mortalidade infantil no Estado em 2003. Fundação SEADE, Resenha de Estatísticas Vitais do Estado de São Paulo 2004; 10 , ano 5, jul. 2004, 1-7. [http://www.seade.gov.br/produtos/spdemog/PDF/ julho_2004.pdf].
12. Menezes AMB, Victora CG, Barros FC, Albernaz E, Menezes FS, Jannke HA, et al. Mortalidade infantil em duas coortes de base populacional no Sul do Brasil: tendências e diferenciais. Cad Saúde Pública 1996; 12(S1): 79-86.
13. Guerra FAR, Llerena Junior JC, Gama SGN, Cunha CB, Theme Filha MM. Defeitos congênitos no município do Rio de Janeiro, Brasil: uma avaliação através do SINASC (2000-2004). Cad Saúde Pública 2008; 24(1): 140-9.
14. Almeida MF, Alencar GP, França Junior I, Novaes HMD, Siqueira AAF, Schoeps D, et al. Validade das informações das declarações de nascidos vivos com base em estudo de caso-controle. Cad Saúde Pública 2006; 22 (3): 643-52.
15. Mello Jorge MHP, Gotlieb SLD, Soboll MLMS, Almeida MF, Latorre MRDO. Avaliação do sistema de informação sobre nascidos vivos e o uso de seus dados em
epidemiologia e estatísticas de saúde. Rev Saúde Pública 1993; 27: 1-46.
16. Piper JM, MitchellI Junior EF, Snowden M, Hall C, Adams M, Taylor P. Validation of 1989 Tennessee birth certifi cates using maternal and newborn hospital records. Am J Epidemiol 1993; 137: 758-68.
17. Fundação SEADE – Movimento do Registro Civil – Tabulação de Microdados. Disponível em http://www. seade.gov.br. [Acessado em 02 de março de 2009].
18. Pinto CO, Nascimento LFC. Estudo de prevalência de defeitos congênitos no Vale do Paraíba Paulista. Rev Paul Pediatr 2007; 25(3): 233-39.
19. Saúde Brasil 2004. Uma análise da situação de saúde. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Brasília/DF, maio de 2004.
20. Tanaka ACA, Siqueira AAF, Bafi le APN. Situação de saúde materna e perinatal no Estado de São Paulo, Brasil. Rev Saúde Pública 1989; 23(1): 67-75.